

Abstract
Introduction
Pit and fissures of permanent dentition are considered to be highly vulnerable to the adhesion of cariogenic microorganisms and consequently result in caries formation. The main problem associated with sealant failure will be microleakage. Therefore, sealants can be considered to be an effective preventive procedure for dental caries, only if it strongly bonds to the tooth, and protect the pit and fissures from the oral bacterial environment.
Aim and objective
To compare and assess the microleakage of two different pit and fissure sealants on permanent molars.
Materials and methods
A total of 20 extracted third molars were randomly divided into two groups where group I is conventional sealant and group II is hydrophilic sealant. Occlusal surfaces of permanent molars were treated with 37% orthophosphoric acid before sealant placement. Tooth samples were subjected to 0.1% rhodamine dye immersion, thermocycling, and tooth samples were sectioned and evaluated under a confocal laser microscope for dye penetration. A non-parametric test (Mann–Whitney U) was performed to compare the mean microleakage score difference between the groups.
Results
Group II (hydrophilic sealant) showed a minimum level of the microleakage score when compared to group I (conventional sealant) and was found to be statistically significant using the Mann-Whitney U test with a p value <0.05.
Conclusion
The less the microleakage, the better will be the retention of the sealant for a longer duration and cariostatic action.
How to cite this article
Prabakar J, Indiran MA, Kumar P, et al. Microleakage Assessment of Two Different Pit and Fissure Sealants: A Comparative Confocal Laser Scanning Microscopy Study. Int J Clin Pediatr Dent 2020;13(S-1):S29–S33.
Keywords: Confocal laser microscope, Microleakage, Pit and fissure sealant
Introduction
Pit and fissure caries is a pathogenic microbial disease results from an ecological change in bacterial biofilm composition when exposed for a longer period to fermentable carbohydrates, leading to a disturbance in the balance between demineralization and remineralization.1 Deep pits and fissures on the occlusal surfaces are particularly more prone to dental caries2 and contribute to about 56–70% of dental caries among 5–17-year-old school children.3,4
A panel of experts convened by the American Dental Association (ADA), Council on Scientific Affairs (CSA), and American Academy of Pediatric Dentistry reported that pit and fissure sealants are more effective in interrupting and prevent the progression of pit-and-fissure occlusal caries lesions of primary and permanent molars in children and adolescents on comparison with fluoride varnish application and non-use of sealants.5
In recent years, there is a wide spectrum of resin-based sealant materials were available in dental merchandise. To maximize the effectiveness of resin-based sealants, dental manufacturers have incorporated filler particles, fluoride, fluorescence into the sealant material. One such newer brand of sealant is UltraSeal XT Hydro sealant which is 53% highly filled resin with thixotropic (ideal viscosity) and advanced adhesive technology allows it to flow into pit and fissures and bond effectively without a drying agent to the tooth. Therefore, the higher bond strength results in reduced microleakage and increased marginal retention.6
Sealants can be either clear, color-changing on curing or tinted. The main advantage of colored sealants is that it permits the operator for more precise placement of the sealant. Clinpro 3M ESPE is one such colored sealant that changes its color on polymerization.7 Resin-based sealants are the ones that effectively adheres to the enamel due to acid etching. Hence, the anti-caries or preventive effect of these resin sealants depends on the formation of the tight marginal seal which ultimately prevents microleakage.8
Microleakage by definition refers to the transit of microorganisms and fluids across the gap separating the teeth and the sealant.8 Microleakage is a prime reason for sealant failure.9
Newer brands and make of pit and fissure sealants continue to be developed, despite the lack of scientifically based information addressing the microleakage properties of these materials. Hence, laboratory-based in vitro analysis plays a pivotal role in yielding adequate guidance toward the use of new products in a short duration.
In the present study, UltraSeal XT is compared with conventional Clinpro 3M ESPE sealant. Although many in vitro studies have investigated the microleakage properties of Clinpro 3M ESPE sealant with different sealant material,10,11 no comparative studies have been performed comparing the microleakage property of these two pit and fissure sealants. Hence, the present study was designed to compare and assess the microleakage of conventional and hydrophilic sealant on permanent molars.
Materials and Methods
An experimental randomized in vitro study was carried out on a sample of 20 third molar teeth extracted for orthodontic or surgical reasons. The sample size was estimated based on the study done by Al-Jobair11 using G*Power 3.1.2 software with a power of 0.95 and p ≤ 0.05 and sample size derived was 10 teeth per group and the total sample size will be 20. Teeth with intact occlusal surfaces were included and those teeth with a developmental defect and with caries were excluded from the study. Before the start of the study, ethical clearance was obtained from the institutional ethics committee, Saveetha University (STP/SDMDS13PHD43). All the molars were randomly allocated to two groups of 10 molars each using computer-generated randomization with 5 blocks of two letters (A, B). Group I is a conventional sealant and group II will be a hydrophilic sealant (Table 1).
Table 1.
Tested materials
| Material | Group I Clinpro | Group II UltraSeal XT Hydro |
|---|---|---|
| Type | Unfilled resin based | 53% Highly filled resin based |
| Principal ingredient | Triethylene glycol dimethacrylate, Bis-GMA, tetrabutylammonium tetrafluoroborate, dichloride methylsilane, silica, dye | Triethylene glycol dimethacrylate, diurethane dimethacrylate (DUDMA), aluminum oxide, methacrylic acid, titanium dioxide, sodium monofluorophosphate |
| Manufacturer | 3M ESPE | Ultradent |
The teeth were soaked in 5% sodium hypochlorite. The remaining periodontal tissue and calculus were removed. All the teeth were then microscopically examined for caries and other possible cracks or defects. The specimens that were not fulfilling the inclusion criteria were rejected while those fulfilling were stored in 10% formalin solution until further use.
Acid etching of the selected teeth was carried out using 37% orthophosphoric acid for a duration of 30 seconds followed by rinsing with water and then dried using a three-way syringe to attain a white frosty appearance of enamel for Clinpro 3M ESPE sealant (group I). With UltraSeal XT Hydro (group II), the tooth should be dried gently and left moderately wet with a shiny semblance. The hydrophilic sealant was then applied and cured for 30 seconds. After the placement of sealants, molars were immersed inverted in 0.1% rhodamine B isothiocyanate, Sigma-Aldrich dye for 24 hours at 37°C (Fig. 1). All the teeth were then exposed to a thermocycling procedure for a dwelling period of 30 seconds, temperature ranges between 5°C and 55°C. Molars were sliced longitudinally and the tooth sections were evaluated for microleakage using confocal laser scanning microscopy and were scored by an examiner who was blinded to the study. Ovrebo and Raadal12 guidelines were used to assess the microleakage (Fig. 2) and the interpretation of the scores are as follows:
Figs 1A to E.
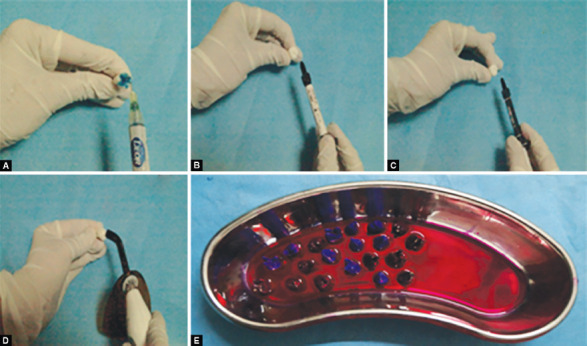
(A to D) Placement of group I and group II sealants; (E) Immersion of tooth samples in 0.1% rhodamine B isothiocyanate dye
Figs 2A and B.
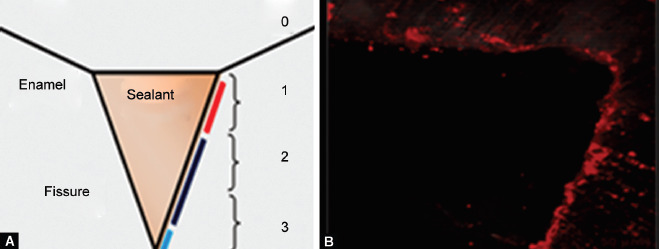
(A) Schematic illustration for dye penetration scoring; (B) Confocal laser microscope image depicts the dye penetration
0 = No dye penetration.
1 = Dye penetration restricted to the outer half of the sealant.
2 = Dye penetration to the inner half of the sealant.
3 = Dye penetration into an underlying fissure.
Data were transferred to a Microsoft Excel spreadsheet and subjected to analysis using SPSS software (IBM SPSS Statistics, Version 20.0, Armonk, NY, USA: IBM Corp). Descriptive statistics were used for data summarization and presentation. Shapiro–Wilks test was used to test the normality of the data set. A non-parametric test (Mann–Whitney U) was used to compare the mean microleakage score difference between the groups. The level of statistical significance was set at a value of p < 0.05.
Results
Table 2 shows the mean microleakage scores of group I sealant which ranges from 0 to 3 while group II sealant shows a range from 0 to 2. The median value of group I and group II sealants were 1.5 and 0.50, respectively. The mean microleakage scores of dye penetration were found to be less for group II sealant (0.60 ± 0.69) than group I sealant (1.5 ± 1.08). Mann–Whitney U test exhibited a statistically significant difference in mean microleakage score between group I and group II which in turn signifies group II sealant found to be superior to the group I sealant (Table 3). Figure 3 depicts the microleakage scores of group I and group II. Out of 10 samples examined, the majority of the samples (five samples) showed a microleakage score of 0 with respect to group II sealant.
Table 2.
Mean microleakage scores of group I and group II
| Descriptive statistics | Group I | Group II |
|---|---|---|
| Number of samples | 10 | 10 |
| Mean microleakage scores | 1.50 | 0.60 |
| Standard deviation | 1.08 | 0.69 |
| Median | 1.0 | 0.00 |
| Minimum | 0.00 | 0.00 |
| Maximum | 3.00 | 2.00 |
Table 3.
Mean difference in microleakage score between group I and group II
| Groups | N | Mean rank | Mann–Whitney U score | Significance |
|---|---|---|---|---|
| I | 10 | 12.95 | 25.50 | p < 0.05* |
| II | 10 | 8.05 |
Mann–Whitney test (p < 0.05)
Fig. 3.
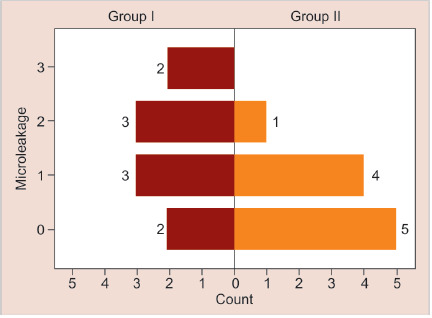
Frequency distribution of microleakage scores of group I and group II sealants
Discussion
The occlusal surfaces of posterior teeth, particularly the pits and fissures have been accepted for their high caries sensitivity for so many years.13 The high caries susceptibility of these surfaces is mainly due to the complex morphology of the occlusal pits and fissures.14 This is especially true for erupting teeth that are in the maturation process15 and their anatomic features cause problems in access for cleansing and further deficient maturation of the enamel adds to caries susceptibility.16
Pits and fissures on the occlusal surfaces differ in size and shape, but are normally slender and curvy, and therefore regarded as a perfect site for food debris and bacterial retention. On average, the diameter of the toothbrush bristle will be around 0.2 mm, all these factors contribute to inaccessibility for mechanical means of food and bacterial debridement.17,18 Cueto and Buonocore19 conducted the first clinical trial on the retention of sealants in 1967. They reported that there was an 86.3% of caries reduction 1 year after sealant application.20 Therefore, sealants were considered to be an outstanding add-on to oral health care preventive strategies for dental caries.21
Microleakage of resin-based filling materials can be evaluated by in vitro tests. A resin-based filling material will be considered to be ideal only when it provides nominal microleakage.22 Adequate marginal adaptation is mandatory for the longevity of the sealant because microorganisms’ diffusion below the sealants commence dental caries.23
The key factor influencing the success of a sealant is its marginal seal to the enamel and microleakage.24 The minimal microleakage property of a sealant is an important factor since a carious process can be initiated and sustained under the sealant.25
The dye penetration method is a more precise technique when compared with other bacterial penetration methods because the diameter of the dye particle is less than those of bacteria and they are similar in size to the bacterial endotoxins.26 In the present study, in vitro microleakage evaluation was performed by measuring the penetration of rhodamine dye between the sealant and tooth structure following the scoring criteria described by Ovrebo and Raadal.12
To mimic the temperature encountered intraorally, the tooth specimens were subjected to a thermocycling procedure. Thermocycling is a technique used frequently that aims at thermally stressing the sealant and tooth interface to high temperatures compatible with intraoral temperature.27
The percentage distribution of microleakage score of group I (Clinpro) sealant was found to be 20% for score 0 and 1 and 30% for score 2 and 3. The mean microleakage score for group I (Clinpro) sealant was found to be 1.5 ± 1.08 higher than group II (UltraSeal XT Hydro) which was 0.60 ± 0.69. Similar results were reported by Borsatto et al.,28 high level of microleakage was observed in Clinpro sealant than its counterpart glass ionomer. The author reported that the glass ionomer provided better marginal sealing than the resin-based Clinpro sealant under saliva contamination. Another in vitro study conducted by Al-Jobair29 observed less microleakage in Fuji Triage cement than Clinpro sealant under wet conditions.
In contrast, a dry condition in the Clinpro™ group showed significantly lower microleakage when compared to the dry condition in the Fuji Triage group in a study done by Al-Jobair.29 This result was consistent with the result of Ganesh and Shobha24 and Rirattanapong et al.30 which showed that resin-based sealant reported better sealing ability (in dry condition) than the Fuji VII GIC Sealant.
However, it was in disagreement with the result of Ashwin and Arathi,25 which revealed no difference in microleakage score between the Fuji Triage and the resin-based pit and fissure sealant.
Nonetheless, the findings of the present research disclosed that the mean microleakage score of group II (UltraSeal XT Hydro) was found to be less compared to group I (Clinpro) sealant. A possible explanation for such behavior could be attributed to three main reasons.
First, the thixotropic nature of group II (UltraSeal XT Hydro) chases moisture deep into the pits and fissures on a microscopic level.6
Second, the adhesive technology of group II (UltraSeal XT Hydro) creates higher bond strength. Hence, higher bond strength results in reduced microleakage and increased retention.6
Third, the wet or moisture contaminations adversely affected the marginal sealing when resin-based sealant (Cinpro™) was used. Most of the porosities normally present are plugged with moisture when the enamel is wet. This causes the lack of resin penetration, which results in tags of insufficient number and length to give adequate retention of the resin to enamel and subsequently, had a high level of microleakage.31
Limitations in the present study could be attributed to the unavailability of a cutting tool for tooth sectioning to provide more tooth slices per tooth for an explicit microleakage evaluation. Depending on the environment, sealants may behave differently due to various factors such as fissure type, tooth preparation, etching, and contamination of prepared surfaces of fissures.
Conclusion
Within the limitations of the present study, we concluded that UltraSeal XT Hydro (group II) showed a minimum level of microleakage than Clinpro sealant (group I). Hence, microleakage is a significant problem and important parameter when it comes to pit and fissure sealant durability and clinical effectiveness since a carious process can be initiated and sustained under the sealant. Therefore, the less the microleakage, the better will be the retention of the sealant for a longer duration and cariostatic action of the sealant.
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.Young DA, Nový BB, Zeller GG, et al. American Dental Association Council on Scientific Affairs. The American Dental Association Caries Classification System for clinical practice: a report of the American Dental Association Council on Scientific Affairs. JADA. 2015;146(2):79–86. doi: 10.1016/j.adaj.2014.11.018. [DOI] [PubMed] [Google Scholar]
- 2.Morales E, Martínez A, Hernández J, et al. Evaluation of marginal seal and microleakage of a sealant modified with silver nanoparticles in primary molars: In vitro study,. Int J Dental SC. 2014;16:107–113. [Google Scholar]
- 3.Kaste LM, Selwitz RH, Oldakowski RJ, et al. Coronal caries in the primary and permanent dentition of children and adolescents 1-17 years of age: United States, 1988-1991. J Dent Res. 1996;75(2_suppl):631–641. doi: 10.1177/002203459607502S03. DOI: [DOI] [PubMed] [Google Scholar]
- 4.Meneghim MC, Saliba NA, Pereira AC. Importance of the first permanent molars in the determination of DMFT index. J Brasileiro de Odontopediatria - Odontologia do Bebê. 1999;2(5):37–41. [Google Scholar]
- 5.Wright JT, Crall JJ, Fontana M, et al. Evidence-based clinical practice guideline for the use of pit-and fissure sealants - report of the American Dental Association and the American Academy of pediatric. JADA. 2016;147(8):672–682. doi: 10.1016/j.adaj.2016.06.001. DOI: [DOI] [PubMed] [Google Scholar]
- 6.Ultradent Products, Inc. Product guide for ultraseal XT hydro. 2013 [Google Scholar]
- 7.Strassler HE, Grebosky M, Porter J, et al. Success with pit and fissure sealants. Dent Today. 2005;24:126, 130. [PubMed] [Google Scholar]
- 8.Markovic D, Petrovic B, Peric T, et al. Microleakage, adaptation ability and clinical efficacy of two fluoride releasing fissure sealants. Vojnosanit Pregl. 2012;69(4):320–325. doi: 10.2298/VSP1204320M. DOI: [DOI] [PubMed] [Google Scholar]
- 9.Alani AH, Toh CG. Detection of microleakage around dental restorations: a review. Oper Dent. 1997;22(4):173–185. [PubMed] [Google Scholar]
- 10.Kane B, Karren J, Garcia-Godoy C, et al. Sealant adaptation and penetration into occlusal fissures. Am J Dent. 2009;22(2):89–91. [PubMed] [Google Scholar]
- 11.Al-Jobair A. Scanning electron microscope analysis of sealant penetration and adaptationin contaminated fissures. J Indian Soc Pedod Prev Dent. 2013;31(3):169–174. doi: 10.4103/0970-4388.117970. DOI: [DOI] [PubMed] [Google Scholar]
- 12.Ovrebo RC, Raadal M. Microleakage in fissures sealed with resin or glass ionomer cement. Scand J Dent Res. 1990;98:66–69. doi: 10.1111/j.1600-0722.1990.tb00941.x. [DOI] [PubMed] [Google Scholar]
- 13.Hicks J, Flaitz CM. Pediatric dentistry infancy through adolescence. 4th ed., New Delhi: Saunders an imprint of Elsevier; 2005. Pit and fissure sealants and conservative adhesive restoration: Scientific and clinical rationale. In: Pinkham JR, Cassamassimo PS, McTigue DJ, et al., ed. pp. 520–576. [Google Scholar]
- 14.Borsatto MC, Giuntini JL, Contente MMMG, et al. Self-etch bonding agent beneath sealant: bond strength for laser-irradiated enamel. Eur J Dent. 2013;7(03):289–295. doi: 10.4103/1305-7456.115412. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dhillon JK, Pathak A. Comparative evaluation of shear bond strength of three pit and fissure sealants using conventional etch or self-etching primer. J Indian Soc Pedod Prev Dent. 2012;30(4):288–292. doi: 10.4103/0970-4388.108922. DOI: [DOI] [PubMed] [Google Scholar]
- 16.Pushpalatha HM, Ravichandra KS, Srikanth K, et al. Comparative evaluation of shear bond strength of different pit and fissure sealants in primary and ermanent teeth - an in-vitro study. J Int Oral Health. 2014;6(2):84–89. [PMC free article] [PubMed] [Google Scholar]
- 17.Feldens EG, Felden CA, De Araujo FB, et al. Invasive pit and fissure in primary molars: a SEM study. J Clin Pediatr Dent. 1994;18:187–190. [PubMed] [Google Scholar]
- 18.Nikiforuk G. Newyork: Karger; 1985. Occlusal sealants. In: Nikiforuk G, ed. Understanding dental caries, etiology and mechanism, basic and clinical aspects. pp. 145–173. [Google Scholar]
- 19.Cueto El, Buonocore MG. Sealing of pits and fissures with an adhesive resin: its use in caries prevention. J Am Dent Assoc. 1967;75(1):121–128. doi: 10.14219/jada.archive.1967.0205. [DOI] [PubMed] [Google Scholar]
- 20.Arrow P, Riordan PJ. Retention and caries preventive effects of a GIC and a resin-based fissure sealant. Community Dent Oral Epidemiol. 1995;23(5):282–285. doi: 10.1111/j.1600-0528.1995.tb00249.x. DOI: [DOI] [PubMed] [Google Scholar]
- 21.Abou El-Yazeed M, Abou-Zeid W, Zaazou M. Effect of different enamel pretreatment techniques for pit and fissure sealing in primary and permanent teeth. Aust J Basic Appl Sci. 1991;7:895–899. [Google Scholar]
- 22.Roberson T, Heymann HO, Swift EJ. 5th ed., Philadelphia: Mosby; 2006. Sturdevant's Art and Science of Operative Dentistry. pp. 185–266. [Google Scholar]
- 23.Pardi V, Sinhoreti MAC, Pereira AC, et al. In vitro evaluation of microleakage of different materials used as pit-and-fissure sealants. Braz Dent J. 2006;17(1):49–52. doi: 10.1590/S0103-64402006000100011. DOI: [DOI] [PubMed] [Google Scholar]
- 24.Mahadevan G, Shobha T. Comparative evaluation of the marginal sealing ability of Fuji VII® and Concise® as pit and fissure sealants. J Contempor Dent Pract. 2007;8(4):10–18. doi: 10.5005/jcdp-8-4-10. DOI: [DOI] [PubMed] [Google Scholar]
- 25.Ashwin R, Arathi R. Comparative evaluation of microleakage between Fuji-VII glass ionomer cement and light-cured unfilled resin: a combined in vivo in vitro study. J Indian SocPedodPrev Dent. 2007;25:86–87. doi: 10.4103/0970-4388.33454. [DOI] [PubMed] [Google Scholar]
- 26.Hansen SR, Montgomery S. Effect of restoration thickness on the sealing ability of TERM. J Endod. 1993;19(9):448–452. doi: 10.1016/S0099-2399(06)80531-5. DOI: [DOI] [PubMed] [Google Scholar]
- 27.Wahab FK, Shaini FJ, Morgano SM. The effect of thermocycling on microleakage of several commercially available composite class V restorations in vitro. J Prosthet Dent. 2003;90(2):168–174. doi: 10.1016/S0022-3913(03)00300-7. DOI: [DOI] [PubMed] [Google Scholar]
- 28.Borsatto MC, Corona SA, Alves AG, et al. Influence of salivary contamination on marginal microleakage of pit and fissure sealants. Am J Dent. 2004;17:365–367. [PubMed] [Google Scholar]
- 29.Al-Jobair A. In vitro evaluation of microleakage in contaminated fissures sealed with GC Fuji triage glass ionomer cement. Dental Sci. 2010;22(1):25–32. [Google Scholar]
- 30.Rirattanapong P, Vongsavan K, Surarit R. Microleakage of two fluoride-releasing sealants when applied following saliva contamination. South East Asian J Trop Med Public Health. 2013;44(5):931–934. [PubMed] [Google Scholar]
- 31.Hormati AA, Fuller JL, Denehy GE. Effects of contamination and mechanical disturbance on the quality of acid-etched enamel. J Am Dent Assoc. 1980;100(1):34–38. doi: 10.14219/jada.archive.1980.0033. DOI: [DOI] [PubMed] [Google Scholar]