

1. INTRODUCTION
The life‐course concept has been widely used during the 20th century to give insights into biomedical as well as wider social issues. However, the biomedical and social science fields have developed concepts in parallel without much cross‐fertilisation. For the developmental origins of health and disease (DOHaD) biomedical scientific discourse, the focus has largely been on pro‐ and retrospective epidemiological cohort studies of risk of non‐communicable diseases (NCDs) and of underlying mechanisms such as epigenetic processes. In parallel, numerous long‐term studies within the social sciences have provided strong evidence on how generations interact and the changing social relations and family structures over the past century. This article explores how the life‐course concepts from these fields can be combined, arguing for a re‐invention of a social medicine approach to family health in communities based on a long‐term, diachronic perspective.
2. THE DOHAD LIFE‐COURSE PERSPECTIVE
The life‐course perspective within DOHaD emerged from the confluence of several lines of biomedical research. Retrospective epidemiological studies of cohorts of individuals characterised from birth led to the perception that prenatal development, measured using the proxy of birthweight, was associated with risk of NCDs such as cardiovascular disease and diabetes many decades later.1 This led to a plethora of studies in experimental animals of many species, and insights drawn from the fields of developmental and evolutionary biology, which revealed that the prenatal processes leading to NCD risk in humans later in the life course were at one end of a spectrum of adaptive processes normally occurring in early life which are not necessarily pathological.2 This contrasted with predominant views that NCD risk was a combination of genetic predisposition and unhealthy adult lifestyle, a controversial proposition which begged a mechanistic explanation for a phenomenon with such a long latency between initiating stimulus and overt response. Possible mechanisms were largely provided by renewed research in the field of epigenetics, initially in animals but more recently in human cohorts, which has revealed how a range of developmental environmental factors can influence gene expression and thus an individual's phenotype and responses to later lifestyle challenges.3
These insights made a life‐course perspective fundamental to current DOHaD concepts for several reasons. First, it became clear that even normative adaptive changes in phenotype arising from epigenetic processes operating during early development could be associated with greater later risk of NCDs if environmental factors such as food and physical activity levels changed across the life course: this is the so‐called Mismatch concept.4 Secondly, in another dogma‐challenging series of discoveries, it became clear that epigenetic changes induced in one generation could be passed through either male or female gamete to the offspring, or even to subsequent generations.5 Consequently, one can visualise the life course as a circle incorporating each stage of life: fetal life, infancy, early childhood, school age, adolescence and fertile age (including the preconception period). Within this circle, positive and negative events at any stage of the life course may have an impact on subsequent stages of the life course of an individual and also have effects on the life course of subsequent generations. Old age is the exception, where the impacts of events are not transmitted to the next generation (Figure 1).6
FIGURE 1.
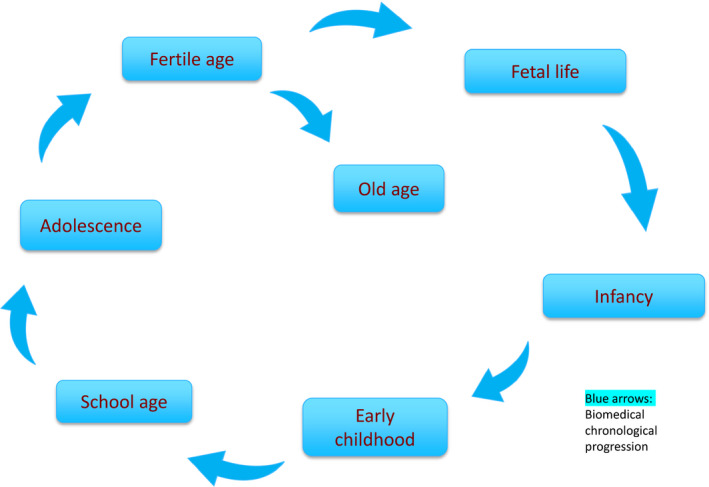
Circular representation of the phases of the biomedical (DOHaD life‐course perspective, illustrating how accumulated risk in each phase chronologically leads to the next and may influence the subsequent generation (modified from Aagaard‐Hansen et al. 2019)
Such models have led to considerations of the most appropriate interventions and timepoints in order to reduce the risk of NCDs in the DOHaD context. Increasingly, the focus of attention has been on early pregnancy and even the preconception period, as epigenetic processes operate in the early embryo to influence development. In addition, as a substantial proportion of pregnancies are unplanned, interventions to promote healthy early development may be necessary before conception.7 Moreover, the paternal transmission of risk makes it important to involve both parents in risk reduction for their child.8
3. THE SOCIAL LIFE‐COURSE PERSPECTIVE
In parallel to the biomedical life‐course discourse described above, there has been a similar growing focus within the social sciences. Most of this research encompassed large‐scale, longitudinal studies conducted in the USA and other high‐income countries and documenting evolving family structures due to changing norms and socio‐demographic trends such as increased divorce rate and longevity. The traditional nuclear family has become less common and multigenerational relationships increasingly important and diverse in structure and function.9 In addition, it has been shown how the ‘life course of individuals is embedded and shaped by the historical times and places they experience over their lifetime’.10 Examples include the Second World War or the COVID‐19 pandemic, which constitute a common reference frame for persons of the same generation.
Not surprisingly, family relationships have profound influence on the family members. The links between family relationships and well‐being differ according to marital, intergenerational and sibling relationships, and gender and ethnicity play a role.11 Canedo‐Garcia et al12 reviewed the impact of interventions within intergenerational social relations, stating that ‘participation in interventions of this type yields benefits in terms of improving older adults’ health and well‐being by facilitating continued intellectual or physical activity in the elderly, and it simultaneously contributes to the encouraging of values and behaviours in children and to the construction of identity among adolescents’.
Figure 2 shows the social perspective superimposed on the biomedical life‐course cycle in terms of the potential social interactions between parents and offspring (one‐generation gap), and grandparents and grandchildren (two‐generation gap). These social relationships may offer unidirectional support or mutually beneficial bidirectional support. As time progresses, they may change from unidirectional to bidirectional (eg when a child grows up and may provide support to the adults), or vice versa (eg as a family member ages and switches from being a resource to mainly needing care and support). Both the biomedical and social life‐course perspectives contain elements of chronological progression where exposures early in life have important bearings on responses to later events. However, in addition intergenerational social interaction bridges generations and thereby shortcuts the chronology (running counter to the chronological direction).
FIGURE 2.
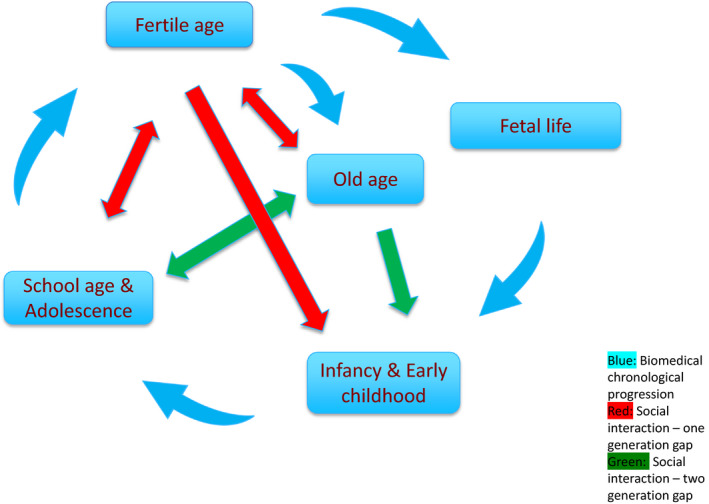
Circular representation of main phases of a combined bio‐social life course. The blue arrows illustrate how each phase chronologically leads to the next, and may influence the following generation. The red and green arrows indicate one‐generation (parental) and two‐generation (grand‐parental) social interactions respectively. The arrowheads (either uni‐ or bidirectional) signify the main directions of potential support
4. TOWARDS A BIO‐SOCIAL LIFE‐COURSE PERSPECTIVE
Combining the biomedical and the social life‐course perspectives into a bio‐social paradigm leads to new insights. It does not change the biomedical rationale that the preconception period and promoting healthy development during the first 1000 days from conception to age two years are critical for a healthy later trajectory. But including the strong social science evidence base expands the well‐known notion that family and social networks are important to a more comprehensive understanding of how these inter‐relationships develop over time and constitute important supportive structures.
Figure 3 visualises the bio‐social life‐course perspective, using a notion of ‘bio‐social capital’ to indicate the combination of phenotypic fitness and health (induced, eg by early epigenetic processes) with social resources (the sum of neuro‐cognitive and emotional skills, educational achievements, social networks and care including close family, relatives and friends, economic resources and environmental factors). This is a refinement on previous life‐course models, which used the concepts of a critical period for induction of an at‐risk phenotype, an accumulation of risk or a chain of risk.13
FIGURE 3.
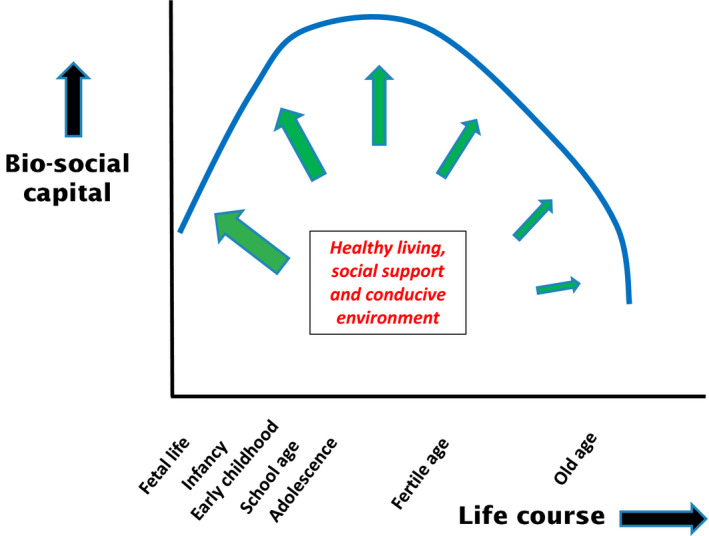
Illustration of the bio‐social life course in terms of chronological age and ‘bio‐social capital’ comprising a combination of phenotypic fitness or resilience and social resources. The blue curve shows how the bio‐social capital life course increases in early years and declines again in old age. It may be sustained or improved by levels of healthy living, social or medical support and conducive environment, as indicated by the green arrows which are drawn thicker earlier in the life course in order to indicate a larger scope for change
Rudolf Virchow (1821–1902) is among many other things credited as the founder of social medicine which, in broad terms, focuses on the interaction between patterns of diseases and risk factors on the one hand and socio‐demographic and economic factors (currently called social determinants) on the other. The bio‐social life‐course perspective fits within this discourse. However, it also adds an essential point. At its core, the life‐course perspective draws attention to the very long‐term causal relationships and mechanisms spanning decades and sometime generations. Whereas traditional epidemiological and social sciences often apply a short‐term focus, the bio‐social life course entails a long‐term view—a shift from synchronic to diachronic social medicine. These terms have been adapted from linguistics: the former denotes the combination of events occurring simultaneously at a point in time, whereas the latter refers to events occurring sequentially over time.
Such thinking has profound implications for public health research. The long and intricate causality chains of intertwined biomedical and social mechanisms can only be explored through long‐term, large‐scale cohort studies measuring both biological and socio‐demographic variables. Hence, notwithstanding the relevance of short‐term trials, only long‐term studies can fully capture the distant outcomes of a given intervention and the intricate bio‐social contextual factors. As mentioned above, most social life‐course research has been conducted in high‐income countries. It is essential that similar research be carried out in low–middle‐income settings, where differing cultures, religions, kinship structures, healthcare systems and stages of demographic transition provide alternative conditions.
Though daily clinical practice will probably remain the same, there are also practical implications of the bio‐social life‐course perspective. Thus, there is now clear evidence confirming previous intuitions that appropriate and adequate interventions early in life not only have immediate benefits but also profound long‐term implications and that such support for ‘nurturing care’14 should integrate biomedical and social elements.
5. CONCLUSIONS
In recent decades, the life‐course perspective has led to important insights within DOHaD biomedical as well as social sciences, although little cross‐fertilisation has occurred. A combined bio‐social life‐course perspective to bring together these two large, but hitherto distinct, bodies of evidence transforms social medicine from a synchronic to a diachronic discipline, suggesting new interventions to reduce common chronic diseases and shifting emphasis from treatment to prevention. We contend that this paradigm shift should guide research as well as practice to look beyond immediate proximal outcomes and consider distal outcomes affecting future lives and generations.
CONFLICT OF INTEREST
None declared.
AUTHOR CONTRIBUTION
Both authors have contributed to all phases of the paper from conceptualisation to writing and approve the final version.
FUNDING INFORMATION
MAH is supported by The British Health Foundation and the EU Horizon 2020 LifeCycle programme.
REFERENCES
- 1.Barker DJP. Fetal origins of coronary heart disease. BMJ. 1995;311:171‐174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hanson MA, Gluckman PD. Early developmental conditioning of later health and disease: physiology or pathophysiology? Physiol Rev. 2014;94:1027‐1076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Godfrey KM, Lillycrop KA, Burdge GC, Gluckman PD, Hanson MA. Epigenetic mechanisms and the mismatch concept of the developmental origins of health and disease. Pediatr Res. 2007;61(7):5‐10. [DOI] [PubMed] [Google Scholar]
- 4.Gluckman P, Hanson M. Mismatch. The Lifestyle Diseases Timebomb. Oxford: Oxford University Press; 2008. [Google Scholar]
- 5.Hanson MA, Skinner MK. Developmental origins of epigenetic transgenerational inheritance. Environ Epigenet. 2016;2(1):1‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aagaard‐Hansen J, Norris SA, Maindal HT, Hanson M, Fall C. What are the public health implications of the life‐course perspective? Global Health Action. 2019;12(1):1603491. 10.1080/16549716.2019.160391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Barker M, Dombrowski SU, Colbourn T, et al. Intervention strategies to improve nutrition and health behaviours before conception. Lancet. 2018;391(10132):1853‐1864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fleming TP. The remarkable legacy of a father’s diet on the health of his offspring. Proc Natl Acad Sci. 2018;115(40):9827‐9829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bengtson VL. Beyond the Nuclear Family: the Increasing Importance of Multigenerational Bonds. The Burgess Award Lecture. J Marriage Fam. 2001;63:1‐16. [Google Scholar]
- 10.Elder GH Jr, Johnson MK, Crosnoe R. The Emergence and Development of Life‐course Theory. In: Mortimer JT, Shanahan MJ, eds. Handbook of the LIFE‐COURSE. Springer Science Business Media, LLC; 2006:3‐22. [Google Scholar]
- 11.Thomas PA, Liu H, Umberson D. Family relationships and well‐being. Innovation in Aging. 2017;1(3):1‐11. 10.1093/geroni//igx025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Canedo‐Garcia A, Garcia‐Sánchez J‐N, Pacheco‐Sanz K‐I. A Systematic review of the effectiveness of intergenerational programs. Front Psychol. 2017;1:1882. 10.3389/fpsyg.2017.01882 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ben‐Shlomo Y, Kuh D. A life‐course approach to chronic disease epidemiology: conceptual models, empirical challenges and interdisciplinary perspectives. Int J Epidemiol. 2002;31(2):285‐293. [PubMed] [Google Scholar]
- 14.Britto PR, Lye SJ, Proulx K, et al. Nurturing care: promoting early childhood development. Lancet. 2017;389(10064):91‐102. [DOI] [PubMed] [Google Scholar]