

Abstract
Background
Speech development requires intact and adequately functioning oral anatomy and cognitive ‘speech processing’ skills. There is evidence that speech input processing skills are associated with speech output problems in children not born with a cleft. Children born with cleft palate ± lip (CP±L) are at high risk of developing disordered speech output. Less is known about their speech input processing skills and whether they are associated with cleft‐related speech sound disorder (SSD).
Aims
(1) To collate and evaluate studies reporting evidence regarding the speech input processing skills of children born with cleft palate in comparison with data from typically developing children or other comparison groups; and (2) to identify any available evidence regarding relationships between speech input processing skills and speech output in children born with CP±L.
Methods & Procedures
Potentially relevant studies published up to November 2019 were identified from the following databases: Medline via Ovid, Embase via Ovid, Cinahl via Ebscohost, PsycInfo via Ebscohost, BNI via ProQuest, AMED via Ovid, Cochrane Library and Scopus. Inclusion criteria were: peer‐reviewed articles published in scientific journals, any design, published in English, participants born with a CP±L aged up to age 18 years who completed speech input processing assessments compared with normative data and/or a control or other comparison group. Critical Appraisal Skills Programme (CASP) checklists were used to quality appraise included studies.
Outcomes & Results
Six studies were retained in the final review. There is some evidence that children born with CP±L perform less well than non‐cleft controls on some speech input processing tasks and that specific input processing skills may be related to errors in the children's speech. Heterogeneity in relation to study groups and assessments used, as well as small sample sizes, limits generalization of findings.
Conclusion & Implications
There is limited evidence regarding the speech input processing skills of children born with CP±L. There are indications that children born with CP+/L may have difficulty in some aspects of speech input processing in comparison with children not born with a cleft, and that difficulties with some speech input processing tasks may be specific to errors in children's speech output. Further research is required to develop our understanding of these skills in this population and any associations with speech output.
What this paper adds
What is already known on the subject
Few studies have been published that examine aspects of speech input processing in children born with CP±L. Theoretical models of speech processing, and published studies, propose that speech input processing skills are associated with SSD in children who were not born with a cleft. However, it is less clear whether there is any association between speech input processing and cleft‐related SSD.
What this paper adds to existing knowledge
This review systematically collates and evaluates the published, peer‐reviewed evidence regarding speech input processing skills in children born with CP±L. The collated evidence indicates that some speech input processing skills differ between children with and without CP±L. There is some evidence, from a single study, that speech input processing of specific cleft speech characteristics (CSCs) may be associated with the presence of these CSCs in the speech output of some children born with CP±L.
What are the potential or actual clinical implications of this work?
While the evidence is currently limited, increasing our knowledge of speech input processing skills in children born with CP±L contributes to our clinical understanding of the nature of cleft‐related SSD. The current evidence suggests that speech and language therapists should consider speech input processing skills when assessing children with cleft‐related SSD to support intervention planning. Considering these skills in relation to literacy development in these children may also be important.
Keywords: cleft palate, speech, processing
INTRODUCTION
Speech development requires intact and adequately functioning anatomical structures (McLeod and Baker 2017). It also requires intact cognitive skills, which enable identification and understanding of the organization and structure of the sound system being learnt and the planning of subsequent output (Chapman and Willadsen 2011, Wren et al. 2016). These cognitive skills that underlie the anatomical structures and functions involved in speech output can be referred to as speech processing skills (Brosseau‐Lapré and Rvachew 2017, Stackhouse and Wells 1997).
Speech input processing
To achieve intelligible speech, children develop speech input processing skills involving the recognition and processing of sounds and words or non‐words from auditory input, enabling the creation of stored representations of sounds and words (Hearnshaw et al. 2019). Specific speech input processing skills include identifying sounds and segments of sounds in words or non‐words, identifying differences between sounds and words, and identifying when a word has been produced incorrectly with reference to a stored representation of the word (Baker et al. 2001, McLeod and Baker 2017, Stackhouse 2001, Stackhouse and Wells 1997). These skills can be assessed using identification or discrimination tasks requiring forced/binary (e.g., same/different) choices between words or non‐words, mispronunciation detection, and lexical or phonetic judgement tasks and sound indication tasks (Rvachew 2006, Stackhouse et al. 2007, Hearnshaw et al. 2019). A child's ability to perceive or recognize their own speech production errors has also been highlighted as an important speech input processing skill (Lof and Synan 1997). These types of task are commonly referred to as speech perception tasks, with most falling under one or more of the eight criteria for clinically useful speech perception assessment proposed by Locke (1980a) and summarized concisely by Hearnshaw et al. (2019).
Speech input processing also involves the awareness of the internal structure of stored representations of words (Stackhouse and Wells 1997). Tasks that may be referred to as testing phonological awareness skills (e.g., alliteration and rhyme awareness tasks) (Burt 1999, Carroll et al. 2003) can be used to assess this aspect of speech input processing. Phonological awareness skills are also important pre‐literacy skills related to reading development (Collett et al. 2010, Anderson et al. 2016).
Relationships between speech input processing and speech output
Theories and models of speech processing such as those proposed by Lieberman and Mattingly (1985), Stackhouse and Wells (1993), Dodd and McCormack (1995), Hewlett et al. (1998), Rvachew and Berhardt (2010), Shriberg et al. (2012) and Walker and Hickock (2016) describe varying approaches to integrated systems of speech input processing and speech output with some including additional contributing factors such as visual and cultural information (Dodd and McCormack 1995), environmental and personality influences (Rvachew and Bernhardt 2010), memory (Hewlett et al. 1998, Shriberg et al. 2012), sex and age (Shriberg et al. 2012). All models and theories agree there is a relationship between speech input processing and speech output but the exact nature of the relationship is not yet fully understood, particularly in terms of clinical application (Brosseau‐Lapré and Rvachew 2017, Hearnshaw et al. 2019).
In a recent systematic review and meta‐analysis of the existing evidence for relationships between speech perception and speech sound disorder (SSD) with no known structural or cognitive cause, Hearnshaw et al. (2019) concluded that children with SSD have difficulties with speech perception, particularly in lexical and/or phonetic judgement tasks in comparison with typically developing peers. However, they also highlighted that it was important to further understand the methodological variation between studies, particularly in relation to the characteristics of participants including the nature of their SSDs, the speech input processing tasks used/specific skills tested and the level of detail regarding these factors provided by authors. Future studies were recommended, with more homogenous groups of participants with SSD try to understand relationships between speech input processing and speech output across different subcategories of SSD (e.g., phonological, articulation, or children's specific speech error types).
The existing evidence for relationships between phonological awareness tasks that examine speech input processing skills (with no speech output required in response) and different types of speech error patterns in the non‐cleft population is mixed (Brosseau‐Lapré and Roepke 2019, Preston and Edwards 2010, Rvachew 2006, Rvachew et al. 2007). Preston and Edwards (2010) found evidence of an association between speech input processing tasks including rhyme and onset matching (also known as rhyme and alliteration awareness), onset segmentation and sound blending, and atypical sound errors in children with no known conditions which could impact on speech. The same association was not observed between these speech input processing skills and typical sound errors or sound distortions in this study (Preston and Edwards 2010). Rvachew et al. (2007) found no statistical evidence that the severity of a child's SSD predicted speech input processing skills (combined score from rhyme and onset matching and onset segmentation tasks) although they did report seeing a trend towards this. Brosseau‐Lapré and Roepke (2019) also did not observe a correlation between speech input processing tasks (matching sounds at the beginning and end of words), similar to those used by Preston and Edwards (2010), and speech output error type. Nijland (2009) found that two small groups of children with different SSD presentations performed less well than children without SSD on a rhyme awareness task. However, on an auditory discrimination of non‐words task, the group with features of childhood apraxia of speech performed less well than the children with no SSD, but the group with phonological disorder type SSD performed similarly to the group with no SSD (Nijland 2009).
Rvachew et al. (2007) also found that children who achieved age‐appropriate speech output skills at the end of kindergarten (mean age = 69.78 months) also achieved age‐appropriate speech input processing skills (combined score from rhyme and onset matching and onset segmentation tasks). Rvachew et al. postulated that children with good speech input processing skills at pre‐school stage may respond better to speech and language therapy (SLT) intervention or that effective SLT intervention in the early years may account for relatively good phonological awareness skills at the end of kindergarten.
Cleft palate, with or without cleft lip (CP±L), and speech
Children born with CP±L have an overt impairment to the anatomy required for speech output. The speech difficulties experienced by children born with CP±L can be broadly divided into two categories:
Speech features directly related to inadequate velopharyngeal/palatal structure and/or function involve the uncontrolled leaking of air into the nose during speech. These are features that the speaker has no control over and are collectively described as evidence of velopharyngeal dysfunction or insufficiency (VPD/VPI) which usually require surgery to resolve. In severe cases, this can have a direct impact upon specific consonant sounds that can be described as ‘passive’ cleft speech characteristics (CSCs) (Harding and Grunwell 1998).
Speech features that are learnt patterns of articulation which may be related to VPD/VPI or other physiological factors such as hearing, but are thought to be a cognitive adaptation/response to anatomical or physiological factors requiring behavioural changes via SLT to resolve. These features may be described as ‘active’ CSCs (Harding and Grunwell 1998).
Prevalence of speech disorder in children with CP±L
Children born with CP±L are at high risk of developing cleft‐related SSD. Studies reporting speech outcomes for sample sizes ranging from 217 to 1110 five‐year‐old children with repaired CP±L in the UK have consistently found that many present with disordered speech (Britton et al. 2014, Sell et al. 2001, Sell et al. 2015). The largest of these studies, Britton et al. (2014) found 40% of 5‐year‐olds with repaired CP±L presented with serious cleft‐related errors of articulation. A summary of published speech outcomes from a number of different countries revealed that ‘good speech’ could be expected in 60–70% of 4–5‐year‐olds and 70–80% of 6–8‐year‐olds with CP ± L (Lohmander 2011). This suggests a minimum of 20% of children born with CP±L continue to have problems with their speech beyond age 8. This contrasts with data from a UK population cohort study which indicated that 3.6% of children from the general population could be expected to present with a persisting speech disorder at 8 years of age (Wren et al. 2016).
Factors associated with speech outcome in children born with CP±L
Studies have begun to explore factors that may be associated with poorer speech outcomes in children born with CP±L. There is evidence that cleft type is associated with speech outcomes in children born with CP±L with children born with bilateral cleft lip and palate (BCLP) having poorer outcomes (Choa et al. 2014). A history of conductive hearing loss has also been found to be associated with poorer speech outcomes and reduced speech intelligibility in 5‐year‐old children born with unilateral cleft lip and palate (UCLP) (Hall et al. 2017, Sell et al. 2017). Residual anatomical structure and function problems post primary palate repair (e.g., VPD/VPI or palatal fistulae) may also impact on speech output and outcomes (Baylis et al. 2008, Harding and Grunwell 1996, Lohmander and Persson 2008, Hardwicke et al. 2014, Sell et al. 2017). Despite the evidence that socio‐economic status is associated with SSD in the general population (Eadie et al. 2015, Wren et al. 2016), measures of deprivation have not been found to be associated with cleft‐related speech outcomes in children born with CP±L in the UK (Choa et al. 2014, Sell et al. 2017). Sex has also not been found to be a factor associated with cleft specific speech outcomes (Choa et al. 2014, Sell et al. 2017). Aspects of language development have been associated with speech output and speech processing in groups of children born with a cleft (Morris and Ozanne 2003, Anderson et al. 2016). There has also been a suggestion that children born with UCLP may experience more challenges in relation to hyperactivity than their peers who were not born with UCLP (Waylen et al. 2017). However, these difficulties have not been associated with speech intelligibility (Waylen et al. 2017) while children with SSD, not related to being born with CP±L, have been found to do less well on sustained auditory attention tasks than children without SSD (Murphy et al. 2014). A history of speech and language therapy (SLT) intervention has been associated with improved speech outcomes for children born with UCLP (Sell et al. 2017). However, there is no robust evidence for the most effective approach to SLT intervention for children born with CP±L (Bessell et al. 2013).
While children born with CP±L have an anatomical difference affecting the structure and function of their oral anatomy, as with all children, their speech systems also require intact speech processing. They may also present with non‐cleft‐related SSD, which may or may not present in addition to CSCs and speech input processing weaknesses.
Relationship between speech input processing and speech output in children with CP±L
Significant attention has been paid in the literature to the speech output of groups of children with CP±L, with phonological and articulation output features being described and discussed in detail (Chapman 1993, Harding and Grunwell 1996, Persson et al. 2006, Lohmander 2011, Sell et al. 2015, Klintö et al. 2016, Willadsen et al. 2017, 2019). While some of the factors described above have been associated with speech outcomes in children born with CP±L, we still have relatively limited understanding of the factors influencing the development and persistence of cleft‐related SSD. It is therefore possible that weaknesses in an aspect of speech input processing could be related to cleft‐related SSD for some children.
Sound and word production errors made by a child in the presence of an anatomical difference, could be perceived and stored by them as the internal representation for those sounds/words. Alternatively, weak speech input processing skills may lead to the child maintaining speech sound errors, even once the peripheral anatomical difference is resolved, due to being unable to detect their own errors or having difficulty updating incorrect stored phonological representations (Stackhouse et al. 2007). Therefore, when considering why cleft‐related SSD in some children might persist, one hypothesis is that children with persisting CSCs have speech input processing difficulties in addition to their known output difficulties.
In comparison with the literature examining relationships between speech input processing and SSD in children who were not born with a cleft, there has been very little work to date examining relationships between speech input processing and cleft‐related SSD and no systematic review of the existing evidence has been undertaken.
A need was therefore identified to collate and review the current evidence regarding the speech input processing skills of children born with CP±L in order to further develop our understanding of the speech development and disorders experienced by this population. This would inform clinicians regarding the current evidence relating to speech input processing and its relationship with speech output in children born with CP±L. In addition, there is evidence that children born with a cleft have difficulties with reading acquisition (Collett et al. 2010, Conrad et al. 2014). Given the evidence for relationships between SSD and speech input processing skills in children not born with a cleft, including phonological awareness skills that are linked to early literacy development, it is important to consider the evidence for similar relationships in children born with CP±L.
Aims of the study
The aim of this systematic review was to identify, collate and evaluate peer‐reviewed studies reporting evidence regarding the speech input processing skills of children born with CP±L, in comparison with data from typically developing controls (including comparison with test norms) or other comparison groups, and to identify any evidence regarding relationships between speech input processing skills and speech output in children born with CP±L.
METHODS
The systematic review was guided by the principles outlined in the Cochrane Collaboration methodology (Higgins and Green 2011), as far as they could be applied to the study methodologies in this review. The systematic review was registered with PROSPERO,1 an international register of prospective systematic reviews.
Search strategy
In order to define the research question and identify search terms, a PECO (Booth and Fry‐Smith 2003) was developed as follows:
Population: Children born with cleft palate aged up to 18 years.
Exposure: Speech input processing skills.
Comparison: Speech input processing skills of typically developing controls or a comparison group from another clinical population.
Outcome: Speech input processing skills of children born with CP±L.
A comprehensive list of search terms was constructed to maximize the chances of finding all literature reporting findings regarding speech input processing in children born with CP±L. As well as terms specifically related to input processing. These included terms relating to speech output processing and reading/literacy development given the association between these skills as reported in the literature (Rvachew 2006). This allowed inclusion of studies where input processing skills were involved in the data collection and analysis but where the primary research question may have focused on other issues. Grey literature (e.g., PhD theses) was excluded from this review because it has not been through a peer‐review process although OpenGrey, ClinicalTrials.gov, and the World Health Organization International Clinical Trials Registry Platform were searched to ensure nothing relevant was missed.
The cleft search string was taken from Bessell et al. (2013) aiming for consistency in literature searching in cleft speech related systematic reviews. The speech input processing string was designed in consultation with a medical librarian, with a review of literature, and author knowledge. See table A1 in appendix A for the search terms as used in the Medline search.
Published, peer‐reviewed studies were identified through a literature search using Medline via Ovid (1946–November 2019), Embase via Ovid (1974–November 2019), Cinahl via Ebscohost (1981–November 2019), PsycInfo via Ebscohost (1887–November 2019), BNI via ProQuest (1985–November 2019), AMED via Ovid (1985–November 2019), Cochrane Library (1996–November 2019), and Scopus (1850–November 2019). The electronic databases were searched by title, abstract, and subject heading fields.
Inclusion criteria
Studies included were peer‐reviewed articles published in scientific journals, of any design, published in English and which involved children born with non‐syndromic CP±L aged up to age 18 years who completed speech input processing assessment tasks/tests using standardized assessments with normative data and/or in comparison with a non‐cleft, typically developing control or other comparison group. For the purposes of this review, a speech input processing task was defined as:
A task which requires the child to internally process, manipulate, segment, identify, differentiate or make judgements between individual sounds, segments of sounds or whole words either within or between words or non‐words. The task stimuli may be either pictures or spoken words (but not written/orthographic). The task must not be reliant on specific speech output other than binary responses such as yes/no, same/different, right/wrong.
The aim was to isolate evidence for speech input processing skills only and not to include tasks where both input and output processing was required to complete the task. This avoids results, where a spoken response was required, being potentially confounded by output difficulties (Preston and Edwards 2010, Sutherland and Gillon 2007).
Exclusion criteria
Studies were excluded if they were not published in English, did not include any participants with non‐syndromic CP±L, only included adult participants or if no speech input processing assessment meeting the inclusion criteria were completed. Studies were also excluded if it was not possible to determine whether assessment tasks used met the inclusion criteria and if a speech input processing assessment was used but it was not possible to extrapolate data from the assessment for participants with CP±L in the results section of the paper.
Screening procedures
Once duplicates were removed, 11,342 titles were screened by LS. Two authors (LS and SH) subsequently screened 431 abstracts retained following title screening. Abstract screening was conducted individually and then those to be retained for full‐text screening were agreed by consensus. LS and SH subsequently undertook full‐text screening (n = 90), first individually and then agreed on the final full‐texts to be included via consensus. The reference lists of these articles were hand‐searched. The final number of full texts that met the inclusion criteria was six.
Quality appraisal
Quality was assessed using the Critical Appraisal Skills Programme (CASP) Cohort Study or Case‐control appraisal tools, as appropriate for the retained study methodology.2 All identified manuscripts were checked for quality against the appraisal tools independently by LS and SH followed by consensus. Due to heterogeneity in outcome measures, meta‐analysis of quantitative data was not appropriate. Therefore, a narrative synthesis of included studies was performed focusing on population characteristics, assessment tasks utilized and outcomes.
RESULTS
Figure 1 shows the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta‐Analyses)3 flowchart and summary of papers retrieved at each stage of the review.
FIGURE 1.
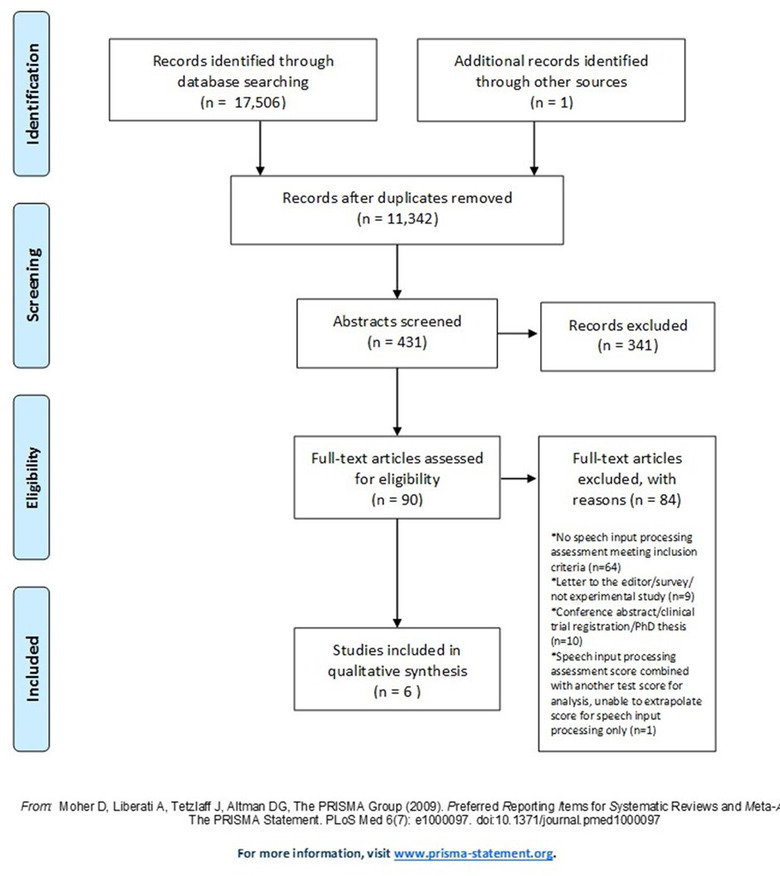
PRISMA 2009 flow diagram [Color figure can be viewed at wileyonlinelibrary.com]
The characteristics of each of the included papers are presented in table 1. These include the aims, study design, sample size including the number of participants with a cleft diagnosis, input processing tasks used, inclusion and exclusion criteria, potential confounders considered and the quality appraisal score. Table 2 details the characteristics of the study participants: sex, age, cleft diagnosis(es) and other demographic features reported/considered including hearing, middle ear function, family socio‐economic status, speech and language therapy, secondary speech surgery and languages spoken.
TABLE 1.
Data extracted from included papers: Study characteristics, aims, design, sample size, speech input processing measures, inclusion/exclusion criteria and results relevant to this review
| Reference | Aim(s) of the study | Study design | Sample size | Input processing measure(s) | Inclusion criteria | Exclusion criteria/potential confounders considered | Results relevant to this review |
|---|---|---|---|---|---|---|---|
| Anderson et al. (2016) | To test if: (1) children with poorer PA skills will have impaired middle ear function; (2) children with poorer PA skills will have poorer speech production skills; and (3) a significant relationship between VP function and PA will be conditional to a significant relationship between PA and speech production and middle ear function | Retrospective cohort | 30 | PIPA (Dodd et al. 2000) Subtests Rhyme Awareness and Alliteration Awareness | 5;0–6;0 years of age, Australian English only language, repaired CL/P, no history of central nervous system involvement, no sensorineural hearing loss, a complete data set in the database | Other diagnosed syndromes or medical conditions present | Rhyme awareness for cohort (SS between 7 and 13 within normal limits): mean SS = 7.43 (SD = 3.014, range = 3–13) Alliteration Awareness for cohort (SS between 7 and 13 within normal limits): mean SS = 9.23 (SD = 3.081, range = 4–15) |
| Baylis et al. (2008) | To examine the influence of speech sound perception skills, cognitive skills and implicit phonological learning ability on the articulation skills of children with VCFS and those with cleft palate or VPD | Case/control | 13 (8 VCFS, 5 CP/VPD) | Minimal pair discrimination task with initial or final phoneme contrasts | VCFS group: confirmed diagnosis by genetic testing. CP/VPD group: non‐syndromic repaired cleft palate, submucous CP/VPD. All English first language | Children with clefts involving the lip and alveolus. CP/VPD group: no known learning disabilities, no other congenital anomalies or syndromes, no known behavioural or psychiatric conditions, no known language impairments, no oronasal fistulae at the time of the study | All three participants with CP/SMCP scored 98% on speech perception task compared with a group mean score of 91% for the group with VCFS |
| Collett et al. (2010) | To test the hypothesis that children with orofacial clefts would score lower than controls on measures of reading and closely related skills | Case/control | 42 (cleft group), 43 (control group): ‘sound matching’ task only administered with 23 cases and 24 controls | Sound matching subtest of the CTOPP (Wagner et al. 1999) | 5–7 years of age, enrolled in kindergarten through second grade, English first language | Known genetic or neurodevelopmental syndrome, visual or auditory impairments that would preclude participation, previously diagnosed learning disability, history of traumatic brain injury, out of home residential placement. Controls also excluded if any history of craniofacial anomaly | Sound matching task: children with clefts: mean SS = 10.9 (SD = 1.7, 95% CI = 8.7–10.5); children without clefts: mean SS = 10.6 (SD = 2.1, 95% CI = 9.7–11.5). Adjusted mean difference = 0.1 (95% CI = –1.1 to 1.3), p = 0.909 |
| Finnegan (1974) | To compare speech sound discrimination skills of boys with and without a cleft palate. To determine if there is a difference in speech sound discrimination between boys with cleft palate with and without a history of middle ear pathology. To ascertain whether there is a difference in speech sound discrimination skills between boys with cleft palate with and without velopharyngeal incompetence | Case/control | 16 (cleft group), 16 (non‐cleft group) | Speech Sound Discrimination Task 68‐F (Rudegeair and Kamil 1969) | Monolingual American English speakers controlled for regional dialect, normal intelligence, no significant deviation in oro‐pharyngeal structures other than surgical repair of the cleft, air conduction hearing threshold average < 2b dB in the better ear for frequencies 500, 1000 and 2000 Hz | Any history of abnormal middle ear pathology in the non‐cleft group | Total mean number of errors on discrimination task higher for cleft group (mean for cleft group = 3.347 (SD = 2.56), mean for non‐cleft group = 1.343 (SD = 1.06). Statistical evidence for effect of group on performance (p ≤ 0.01). Non‐cleft group better at discriminating between affricate and nasal manner classes (p < 0.05 and < 0.01 respectively). Non‐cleft group made no errors with /b/ versus /p/ contrasts, but for cleft group this contrast accounted for a quarter of their errors on voiced/voiceless contrasts. Both groups found voicing contrasts easier to discriminate than place of articulation |
| Lemos and Feniman (2010) | To verify the performance of children with cleft lip and palate in the SAAAT | Case/control | 30 (cleft group), 25 (non‐cleft group) | SAAAT | Non‐cleft group: no cleft lip and palate or associated syndrome, no diagnosis of ADHD or use of medication associated with ADHD, peripheral hearing within normal limits, right‐handed, no diagnosis of any syndrome. Cleft group: CL/P, scheduled visit to the hospital in a 9‐month period, age 7 years at the time of the visit, additional inclusion criteria as per the non‐cleft group | None in addition to needing to meet the inclusion criteria | Evidence of a difference in performance between cleft and non‐cleft groups on ‘decreased vigilance’ domain of SAAAT, with the cleft group performing less well (p = 0.008). No statistical evidence for differences between groups in other domains of the test (inattention, impulsiveness, total number of errors) |
| Whitehill et al. (2003) | To determine whether children with CP and posterior articulation placement error patterns also demonstrated difficulty in the perception of anterior versus posterior place of articulation in comparison with control groups | Case control | 10 (CP plus posterior articulation), 10 (CP with no posterior articulation) and 10 (non‐cleft controls) | Perception of place of articulation (t to k) along an acoustic continuum from synthetic stimuli | Children born with CP presenting with or without posterior placement of alveolar targets. No identified syndrome. Surgical palate closure between 12 and 18 months of age. No palatal fistula at time of testing. Normally developing children matched in age to the children with CP and with no history of speech, language, hearing or learning problems from parent report | As per inclusion criteria. | On an acoustic continuum, children with no CP and children with CP but no posterior speech errors identified 90% of stimuli on one side of identified phonemic boundary as /kh/ and 95% of stimuli on the other side as /th/. All children in these groups able to categorize stimuli into two clear groups. Children with CP and posterior speech errors identified 51–65% of all stimuli along the continuum as /kh/. No children in this group able to identify the stimuli appropriately |
Note: ADHD, attention deficit hyperactivity disorder; CP, cleft palate; CL/P, cleft lip and/or palate; CTOPP, Comprehensive Test of Phonological Processing; PA, phonological awareness; PIPA, Primary Inventory of Phonological Awareness; SAAAT, Sustained Auditory Attention Ability Test; VCFS, velocardiofacial syndrome; VP, velopharyngeal; VPD, velopharyngeal dysfunction; SS, standard/scaled scores; SD, standard deviation; CI, confidence interval; and SMCP, submucous cleft palate.
TABLE 2.
Data extracted from included papers: Characteristics of the study participants, age sex, CLEFT diagnosis, control/comparison group information, speech output measure used and additional information
| Reference (country) | Age of participants | Sex of participants | Cleft diagnosis(es) | Control group/comparison description | Speech output measure used | Additional information |
|---|---|---|---|---|---|---|
| Anderson et al. (2016) (Australia) | 5;0–6;0 years (mean = 5;02 years, SD = 3.39) | Male = 19 (63.3%), female = 11 (36.7%) | Unrepaired SMCP = 3 (10%), soft palate cleft only = 3 (10%), cleft of hard and soft palate = 10 (33.3%), UCLP = 10 (33.3%), BCLP = 2 (6.7%), CLA = 1 (3.3%), cleft soft palate only with PRS = 1 (3.3%) | Standardized assessment with normative data | Diagnostic Evaluation of Articulation and Phonology (DEAP)—Phonology Assessment (Dodd et al. 2002) or Great Ormond Street Speech Assessment (GOS.SP.ASS) (Sell et al. 1999) or Cleft Audit Protocol for Speech—Augmented (CAPS‐A) (John et al. 2006). Speech output for the study categorized into ‘speech difficulties’ or ‘no speech difficulties’ based on the assessment used | Number with speech difficulties = 24 (80%), number with no speech difficulties = 6 (20%), adequate VP function = 20 (66.7%), inadequate VP function = 10 (33.3%), normal middle ear function in at least one ear = 5 (26.7%), bilateral type B tympanometry = 13 (43.3%), abnormal middle ear function = 12 (30%) |
| Baylis et al. (2008) (United States) | 3;10–8;06 years | Male = 6 (46%), female = 7 (54%) | VCFS group (8 including: +CP (1), submucous cleft palate (SMCP) (4), non‐cleft VPD (3)), CP/VPD group (5 including: non‐syndromic repaired CP (2), SMCP (1) or non‐cleft VPD (2)) | Children with VCFS compared with children with repaired cleft/submucous cleft palate or VPD | Phonetic inventory from 39 single‐word picture naming task targeting all English phonemes in initial, medial and final word positions (59 scored consonants and 13 scored vowels). PCC calculated. 15‐min conversational speech sample. PPC score calculated | VP surgery (5), hypernasal (11), years of speech therapy (range = 0–7), history of OM with effusion (9), hearing screening on day of assessment (all 20–25db), grommets (3), tympanometry within normal limits (8) |
| Collett et al. (2010) (United States) | Children with clefts mean = 81.8 months (SD = 9.0), controls mean = 82.1 months (SD = 7.5) Only 5–6‐year‐olds completed the ‘sound matching’ tasks of interest | Male = 56 (28 (66.7%) clefts, 28 (65.1%) controls), female = 29 (14 (33.3%) clefts, 15 (34.9%) controls) | CL only (8), CL+P palate (22), CP only (12). Distribution in the subgroup that completed the ‘sound matching’ task, unknown | Children born with cleft compared with non‐cleft, demographically matched controls and standardized assessment | None used | Mean months of school: cleft = 13.7 (SD = 6.6), control 12.8 (SD = 5.9), mean family SES: cleft = 47.6 (SD = 12.4), control = 50.5 (SD = 11.3), Caucasian: cleft = 29 (69.1), other (13 (31.0), control 35 (83.3) other 7 (16.7), OM: cleft 34 (81), control 28 (65.1) |
| Finnegan (1974) (United States) | Half of each group 7;00–7;11 years (mean = 7;05 years). Half of each group 8;00–8;11 years (mean = 8;07 years) | Male = 32 (16 CP; 16 non cleft) | CP (not specified if CP only or CP±L) | Boys born with CP compared with non‐cleft boys matched for age and meeting all other inclusion criteria | Iowa Pressure Articulation Test (IPAT) (Morris et al. 1961) plus 30‐s language sample. Used to rate nasality and VP function | Mean number of siblings for cleft group = 3.81 and for the non‐cleft group = 2.25. Number in cleft group with history of or current serious OM = 8 |
| Lemos and Feniman (2010) (Brazil) | 7–7;11 years | Male = 29 (12 non‐cleft, 17 cleft), female = 26 (13 non‐cleft, 13 cleft) | 6 post‐foramen and 24 incisive trans‐foramen clefts | Children born with CL/P compared with non‐cleft children meeting all the same inclusion criteria | None used | Non‐cleft group recruited from two schools located in the same town as the hospital the cleft group were recruited from |
| Whitehill et al. (2003) (Hong Kong, China) | Group with CP and posterior articulation placement, mean age = 6;09 (range = 4;06–12;09). Group with CP an no posterior articulation placement, mean age = 6;09 (range = 4;06–12;08). Non‐cleft group, mean age = 6;09 (range = 4;05–12;10) | Male = 22 (73%), female = 8 (27%) | Right unilateral CL/P (6), left unilateral CL/P (8), bilateral CL/P (6) | Comparison between children born with CP with posterior articulation, children born with CP without posterior articulation and non‐cleft controls | Part 1 of the Cantonese Segmental Phonology Test (CSPT) (So 1993), a 31‐item picture‐naming test with each Cantonese phoneme and tone presented at least once. A 36‐item picture‐naming test with each Cantonese syllable initial alveolar phoneme (t, th, s, ts, tsh, l) sampled six times in six different mono‐ and bisyllabic words varying in vowel and final consonant context | All native Cantonese speakers. Previous speech therapy (cleft groups = 20) = 15. History of recurrent OM = 16 |
Note: CL, cleft lip; CLA, cleft lip and alveolous; BCLP, bilateral Cleft lip and palate; CP, cleft palate; CL&P, cleft lip and palate; CL/P, cleft lip and/or palate; OM, otitis media; PRS, Pierre Robin sequence; SD, standard deviation; SMCP, submucosal cleft palate; UCLP, unilateral cleft lip and palate; VCFS, velocardiofacial syndrome; VP, velopharyngeal; VPD, velopharyngeal dysfunction; CP±L, cleft palate with or without cleft lip; PPC, per cent phonemes correct; and PCC, per cent consonant consonants correct.
A total of 245 children participated in the included studies, 81 female and 164 male. Of these, 207 completed speech input processing tasks meeting the inclusion criteria. Sex distribution within the 207 is unknown as this was not specified for the subgroup that completed the relevant task in the study by Collett et al. (2010). However, sex distribution across the five studies in which all participants completed a speech input processing task of interest was 108 male and 52 female. The age range of participants was 3 years 10 months to 12 years 10 months, and 122 had a cleft diagnosis. The remainder were non‐cleft controls with the exception of eight participants in Baylis et al. (2008) who had a diagnosis of velocardiofacial syndrome (VCFS) ± cleft palate, submucous cleft palate (SMCP) or non‐cleft VPD.
All studies excluded children who had genetic syndromes (in addition to any specifically under investigation as part of the study aims) or any known additional developmental, neurological, language or learning impairments.
Quality appraisal
Table 1 shows the total CASP quality appraisal scores. Individual CASP question scores are presented in table B1 in appendix B for the case‐control and the cross‐sectional studies, respectively. All studies reached at least a moderate level of quality.
Description of cleft groups
All the studies included a range of cleft types in their cleft study groups (table 2). Three studies (Finnegan 1974, Lemos and Feniman 2010, Whitehill et al. 2003) included children with CP±L. Finnegan (1974) described the cleft group in their study as having ‘cleft palates’. It is possible therefore that this was a group of children all of whom had a diagnosis of cleft palate only. However, because of this, or the presence/absence of a cleft lip is not specifically described, it is impossible to be certain. The remaining three studies (Anderson et al. 2016, Baylis et al. 2008 Collett et al. 2010) had greater heterogeneity in their cleft groups. They included children with cleft lip or cleft lip and alveolus only (Anderson et al. 2016, Collett et al. 2010), four children with a diagnosis of repaired or unrepaired SMCP (Anderson et al. 2016, Baylis et al. 2008) and two children with non‐cleft velopharyngeal dysfunction (VPD) (Baylis et al. 2008) as well as children with CP±L.
Description of control/comparison groups
Of the six included studies, three (Finnegan 1974, Lemos and Feniman 2010, Whitehill et al. 2003) had a specific aim to compare the speech input processing (speech perception/discrimination) skills of children born with clefts to a non‐cleft control group ± an additional comparison group. Whitehill et al. (2003) included two groups of children born with CP ±L. One group who presented with posterior articulation errors and one who did not have this speech error type, in addition to the non‐cleft control group.
Baylis et al. (2008) did not use a non‐cleft control group. They included a group with CP/SMCP/non‐cleft VPD and a group with VCFS. Although four of the participants in the VCFS group also had a SMCP and one a cleft palate, for the purposes of this review this was considered to be a comparison group.
Two studies explored input processing in the form of phonological awareness tasks (Anderson et al. 2016, Collett et al. 2010) using either a non‐cleft control group (Collett et al. 2010) or test norms as part of their wider analyses/aims (Anderson et al. 2016).
Cleft versus non‐cleft performance on speech input processing tasks
Two studies required participants to discriminate between minimally contrasting pairs of words or non‐words delivered in different ways (Finnegan 1974, Whitehill et al. 2003). Both studies found that children with a cleft performed less well in these tasks than their non‐cleft peers. In Whitehill et al. (2003), this was only the case for the cleft group with posterior articulation errors. The cleft group with no posterior articulation errors performed similarly to their non‐cleft peers. Participants in this study listened to consonant–vowel syllables along a synthetic continuum from /t/ to /k/. The participants who were not born with a cleft and the participants born with CP±L but with no posterior articulation errors both demonstrated a clear pattern of categorization of /t/ versus /k/ on either side of a predetermined boundary, identifying an average of 90% of stimuli on one side of the boundary as /k/ and an average of 95% of stimuli on the other side of the boundary as /t/ (Whitehill et al. 2003). In contrast, the participants with CP±L and posterior articulation errors identified 51–65% of all stimuli as /k/ across the continuum, with no difference in response percentages for this group between the /t/ and /k/ sides of the boundary (p = 0.32) suggesting they were performing at almost chance level (Whitehill et al. 2003). Lemos and Feniman (2010) also found that children in their cleft group performed less well on their input processing task than non‐cleft controls, specifically in relation to ‘decreased vigilance’ (p = 0.008). In this study, decreased vigilance was calculated by identifying how many times the participants identified the word ‘no’ in the first and last presentations of a list of words which were presented to the participants six times. The difference between the number of ‘no’ stimuli identified on the first and last repetitions of the word list defined the decreased vigilance score.
On a task discriminating between minimally contrasting pairs of non‐words, Finnegan (1974) found that the overall mean number of errors on the task was higher in the cleft group with evidence for an effect of group on performance (p = < 0.01). Overall, both groups of children in this study found voicing contrasts (e.g., /t/–/d/) easier to discriminate than place of articulation contrasts (e.g., /d/–/g/). In the cleft group, errors discriminating between voiced and voiceless bilabial plosives (/b/–/p/) accounted for a quarter of the voiced–voiceless discrimination errors whereas the non‐cleft group made no errors with this contrast. When looking across manner classes of sounds, although the cleft group performed less well in terms of percentage of items missed, there was only evidence in relation to ability to discriminate affricates (p < 0.05) and nasals (p < 0.01), with the non‐cleft group better at discriminating within these manner class groups (Finnegan 1974).
Two studies investigated speech input processing in children born with CP±L (and some children born with cleft lip ± alveolus only) with a subset of their phonological awareness tests meeting the speech input processing task inclusion criteria of this review (Anderson et al. 2016, Collett et al. 2010). These tasks were the ‘sound matching’ subtest in Collett et al. (2010) and ‘rhyme awareness’ and ‘alliteration awareness’ subtests in Anderson et al. (2016).
In comparison with test norms, the mean scores for participants in Anderson et al. (2016) on rhyme and alliteration awareness were within normal limits. Similarly, in Collett et al. (2010), the cleft group's mean score on the sound matching task was within the average range of test norms. However, Anderson et al. (2016) also reported that the mean score for rhyme awareness in the cleft group was at the low end of the normal limits range of standard scores on the test.
Cleft versus other comparison group performance on speech input processing tasks
In Baylis et al. (2008), the three participants with CP/SMCP all achieved the same score on the speech perception task (98% correct). This was higher than the mean for the VCFS group (91% correct). It was also higher than the overall mean for the cleft/non‐cleft VPD group (94% correct). These findings were purely descriptive with no statistical analysis of this specific comparison reported in the paper although with only three participants in the cleft group, arguably, statistical analysis would not be appropriate. This was the only data that was possible to extrapolate for the three participants with CP±L in comparison with the participants with VCFS and the children with non‐cleft VPD. Although this study only provides minimal information for speech input processing skills with very small and heterogeneous study groups, a speech input processing task meeting the inclusion criteria was completed. It was therefore possible to extrapolate a small amount of data to compare the performance of participants with CP+/L to those with other clinical diagnoses. As described in the previous section, Whitehill et al. (2003) compared the performance of two groups of children with CP±L. One group presented with posterior articulation errors and the other did not. The results of this comparison are presented in the next section.
Associations between speech input processing and speech output
Only one of the included studies explored associations between the speech input processing skills tested and speech output (Whitehill et al. 2003). Whitehill et al. (2003) found that children born with CP±L who presented with posterior articulation errors, performed less well when identifying anterior versus posterior place of articulation on an acoustic continuum (using synthetic stimuli) than both, children with CP±L and no posterior articulation errors and a non‐cleft control group. The participants in this study were aged 4 years 5 months to 12 years 10 months (mean = 6 years 9 months). Whitehill et al. (2003) also describe that participants in the group of children born with CP±L who did not present with posterior articulation placement did present with other speech production errors.
Although some of the other included studies considered aspects of speech output, they did not examine relationships between speech input processing and speech output specifically. An articulation test was conducted by Finnegan (1974). It was only used to determine a variable for velopharyngeal competence/incompetence and no information for speech sound production was reported. Therefore, there was no information as to the specific nature of any SSD that children may have presented with. Anderson et al. (2016) explored associations between speech output and a total phonological awareness score (combined: syllable segmentation, rhyme awareness, alliteration awareness, phoneme isolation, phoneme segmentation) but not between the input processing only tasks (rhyme and alliteration awareness) and speech output separately. Similarly, in Baylis et al. (2008), although associations between speech input processing and speech output were explored between the two study groups, it was not possible to extrapolate information regarding the participants with CP±L only.
Associations between speech input processing skills and other factors
Although mean group scores across subtests in Anderson et al. (2016) were within the average range for the assessment used, participants’ performance on the rhyme awareness subtest was poorer than their performance on the other subtests (p = 0.38). All the included studies considered hearing and/or middle ear function as part, either of their inclusion/exclusion criteria, or as a covariate in their study. Only Finnegan (1974) and Collett et al. (2010) conducted quantitative analyses specifically exploring associations between the speech input processing task(s) and aspects of hearing/middle ear problems. Finnegan (1974) also considered velopharyngeal function as a covariate as part of the analyses conducted in relation to middle ear pathology.
Through exploratory, descriptive analysis, Finnegan (1974) found that children with CP±L with no history of middle ear pathology and no evidence of velopharyngeal incompetence made fewer errors on the speech discrimination task than children with CP±L with a history of middle ear pathology and/or evidence of velopharyngeal incompetence. Children with both a history of middle ear pathology and evidence of velopharyngeal incompetence made the most errors. At least 80% of the test items were responded to correctly by the children judged as being velopharyngeal competent and at least 68% by the children judged as being velopharyngeal incompetent (Finnegan 1974). Statistical analysis was not undertaken to compare means for these observations due to the small sample size.
In Collett et al. (2010), there was no evidence of a difference between the cleft and non‐cleft groups on the sound matching task when adjusting for age at assessment, grade level, socioeconomic status and amount of shared oral reading per week (p = 0.909) or with additional adjustment for a history of suspected or confirmed hearing problems (p = 0.848). Whitehill et al. (2003) reported, through descriptive analysis, that intragroup variability could not easily be explained by age, cleft type, previous speech therapy or parent reported recurrent otitis media.
DISCUSSION
This review sought to collate and evaluate the existing, peer‐reviewed literature regarding speech input processing skills in children born with CP±L. Six studies meeting the inclusion criteria were retained, demonstrating that this specific area has received relatively little attention in the literature to date, particularly in comparison with Hearnshaw et al.’s (2019) systematic review of speech perception skills in children with non‐cleft‐related SSD, which found 71 papers. Only two studies had the primary aim of comparing speech input processing skills between children born with and without CP±L (Finnegan 1974, Whitehill et al. 2003). The remaining studies had different primary research aims but it was possible to extract information about speech input processing skills from their results data.
Using the categories of speech perception assessment presented by Hearnshaw et al. (2019), there was evidence of differences in performance between children with and without CP±L in: discrimination of minimal and repeated contrast non‐word pairs (Finnegan 1974), categorical perception of a specific minimal pair (Whitehill et al. 2003) and a sound indication task (Lemos and Feniman 2010). No evidence was found for differences between groups on phonological awareness tasks (rhyme and alliteration awareness) meeting the inclusion criteria of a speech input processing task for this review (Anderson et al. 2016, Collett et al. 2010).
Whitehill et al. (2003) found there was only a difference in performance on their speech input processing task, categorical perception of a /t/–/k/ consonant–vowel minimal pair, between their non‐cleft control group and children with CP±L who also presented with posterior speech articulation errors. There was no difference in performance between children with CP±L, who had no posterior articulation errors, and the control group (Whitehill et al. 2003). Although only a single study, this suggests that difficulties with some aspects of speech input processing in children born with CP±L may be specific to the errors they present with in their speech output, particularly given that the group who did not present with posterior errors in their speech output did present with other speech output errors. In addition, although there are many factors that could be associated with why CSCs develop and persist in children born with cleft palate, the findings of Whitehill et al. (2003) lends some preliminary support to the hypothesis that weak speech processing skills may lead to the maintenance of cleft‐related SSD even once the anatomical difference is resolved.
It is notable that 12.5% of errors in the cleft group in discriminating place of articulation were between alveolar and velar consonants /t/ and /k/ in Finnegan (1974). Given the findings in Whitehill et al. (2003), it would be interesting to know whether the children who made these discrimination errors also presented with posterior articulation errors in their speech. This could have implications for the incorporation of these skills into assessment and intervention plans.
Locke (1980a) proposed that speech input processing assessment should centre on the specific speech errors that children produce and Hearnshaw et al. (2019) reported that children with non‐cleft‐related SSD had difficulties with speech input processing of sounds they produced in error in 86% of 30 relevant studies included in their review. Therefore, this aspect of speech input processing appears to warrant further investigation in children born with CP±L.
Although no other study specifically examined relationships between speech input processing and speech output in children with CP±L, the concept was considered by some. Indeed, Finnegan (1974) considered relationships between speech input processing and velopharyngeal function and Anderson et al. (2016) examined the relationship between speech output and a total phonological awareness score which included some subtests requiring speech output. Alternatively, the consideration was between groups which were too heterogeneous to extrapolate information for the very small number of participants with CP±L (Baylis et al. 2008), or theoretical, that is, the authors suggested that it would be useful to explore relationships with speech output in future studies (Collett et al. 2010).
Speech input processing tasks
The tasks in Finnegan (1974), Whitehill et al. (2003) and Baylis et al. (2008) targeted similar skills but were administered in different ways. Both studies that used real word stimuli (Baylis et al. 2008, Whitehill et al. 2003) used pictures for the children to point to, to indicate the word they thought they had heard. In contrast, Finnegan's (1974) non‐word task required the child listen to a target item and then point to which of two speakers they thought they subsequently heard the target word from. All three used recorded auditory stimuli.
Finnegan's (1974) task used a range of word initial and final minimal contrasts and repeated contrasts in consonant–vowel–consonant, non‐word single syllable pairs with place, manner or voicing contrasts. Although this was a non‐word discrimination task, a few of the sound combinations used created real, potentially familiar, words (e.g., /pæt/) and therefore for these combinations, the children could have accessed a lexical route to help them make a judgement (Rees 2001), that is, using their knowledge of a word they recognized, including linked sematic (meaning) related information to inform their judgement which would not be possible with a true non‐word.
Baylis et al. (2008) used a task requiring discrimination between minimally contrasting pairs of single syllables where stimuli were chosen to reflect common speech errors seen in the study population. In contrast to Finnegan (1974), these were real word minimal pairs. Baylis et al.’s (2008) task also included consonant–vowel–consonant, consonant–vowel and vowel–consonant words whereas Finnegan's (1974) task only used consonant–vowel–consonant ‘word/syllable’ combinations. Although the analysis of the nature of error types in Finnegan (1974) is purely descriptive, it is of interest in terms of developing hypotheses as to the cause(s) of these differences and for future study. In contrast, Whitehill et al. (2003) specifically targeted the ability to perceive a repeated single contrast between posterior versus anterior articulation place of articulation on a synthesized acoustic continuum in real word consonant–vowel productions.
Lemos and Feniman (2010) differed from the other studies in that the children were told to listen for the word ‘no’ in a series of single syllable words and make a non‐verbal response when they heard it. The words in the series were maximally contrasting real words and not minimally contrasting as was the case in the other three studies. Although this task was primarily a test of auditory attention, it still met the criteria of an input processing task as defined for this review.
All three of the tasks used in the studies by Collett et al. (2010) and Anderson et al. (2016) used picture stimuli that the children were able to point to for their response. The sound matching task used in Collett et al. (2010) required the participants listen to a sound followed by a word that started or finished with that sound. They were then presented with two to three words and asked to indicate which of the words started or finished with the sound they had heard initially. This task progresses to asking which of three words start or finish with the same sound as a given word. In contrast, the tasks in Anderson et al. (2016) required the child to identify which word from a group of four did not start/end with the same sound.
The detail of the procedures for the tasks in Anderson et al. (2016) and Collett et al. (2010) were not described specifically in the papers themselves, but established by accessing the assessments separately as part of conducting this review. There is a possibility therefore that the tasks were not administered as per the published assessment administration procedure. However, we made the decision to include studies for which we were able to confirm the published test's procedure in the absence of any declaration of deviation from the procedure in the paper.
The differences between the task stimuli and procedures between these papers demonstrates the variety of speech input processing skills that could be assessed and the wide range of possible assessment procedures. It is important to consider the specific skills that speech input processing assessments tasks are actually testing, when comparing evidence regarding speech processing skills and interpreting them clinically (Rees 2001, Stackhouse and Wells 1997). Although tasks may correspond to a level of a theoretical profile or have similar names/aims, when analysed in detail, different tasks may be testing slightly different skills (Stackhouse and Wells 1997). Variability between the assessment tasks used is an important consideration including the level of difficulty of speech input processing assessment tasks used in order to be confident that an appropriate level has been tested for the level of speech production required (Hearnshaw et al. 2019).
Cleft types
Within the cleft groups, there were small sample sizes and considerable heterogeneity with most studies including a range of cleft types in their ‘cleft’ groups. There is evidence that there are differences in the aetiology of different cleft types (Sharp et al. 2017) and that clinical outcomes also vary according to cleft type (Choa et al. 2014). In addition, diagnoses such as SMCP are likely to be made later than those for overt clefts introducing potential confounders in relation to other factors that may be important in relation to speech development (e.g., timing of any surgical or hearing intervention).
In studies of the size included in this review, sample sizes are likely to be too small to conduct subgroup analyses. Therefore, inclusion of a range of cleft types potentially affects the ability to interpret or apply findings clinically. In addition, inclusion of participants with cleft lip ± alveolus only is also problematic because children with no palatal involvement in their cleft are not at the same risk of speech problems as children with clefts involving the palate. Collett et al. (2010) suggested that not including a measure of articulation was a limitation of their study but if they had done so, the issue of including children with cleft lip only in their cleft group could have had implications in relation to this issue unless different cleft types were accounted for in analysis. Achieving an adequate sample size to enable analyses by cleft subtypes is a challenge but highlights the importance of large‐scale research studies and multi‐centre collaboration to achieve this for the benefit of robust and potentially generalizable research evidence and subsequently patient care (Wren et al. 2018).
Speech output measures
There was also considerable variation in the measures used, and subsequent variables produced, where studies had undertaken assessment of speech output and explored associations with aspects of input processing (see table 2 for details). Studies included in this review used single‐word naming tasks, with procedural and target variability between studies depending on the research question (Baylis et al. 2008, Whitehill et al. 2003) and conversational speech tasks (per cent consonants correct) with an implicit priming task assessing phonological learning ability of primed and unprimed words (per cent phonemes correct) (Baylis et al. 2008). Anderson et al. (2016) derived a binary ‘speech difficulties’ or ‘no speech difficulties’ variable using data from either a standardized (single‐word) speech assessment, a CSC specific clinical assessment tool or a CSC audit tool, both of which involve sentence repetition.
The heterogeneity of speech output measures used across studies is a further challenge to being able to compare findings. In addition to the variation described above in relation to the nature of the speech sample assessed, the speech output measure used will also influence exactly what aspect of speech output is being explored in relation to speech input processing. For example, per cent consonants correct versus a standardized developmental speech assessment versus a cleft specific speech assessment all reflect different aspects of speech output. Per cent consonants correct enables a comprehensive measure of consonant production and can be used as a measure across diagnostic groups. However, if reported in isolation, it does not differentiate between types of error (e.g., developmental, atypical or, in the case of the clinical population of interest in this review, CSCs). In contrast, a cleft specific tool such as the Cleft Audit Protocol for Speech—Augmented (CAPS‐A) (John et al. 2006) enables identification and categorization of CSCs but does not provide a measure of developmental, other atypical error patterns or give an overall measure of a child's consonant production. Therefore, careful thought should be given at study design stage regarding which aspect of speech output will be investigated with a specific research question. Any interpretation of findings also needs to consider this issue carefully.
Consideration of hearing and/or middle ear function
As mentioned previously, all the studies had considered hearing/middle ear function in their study design, which is important given the integral role of hearing in speech and speech processing (Stackhouse and Wells 1997). Whitehill et al. (2003) referred to Finnegan (1974) when discussing the potential impact of a history of middle ear problems on speech input processing. In both studies, participants had normal hearing at the time of the study, and both collected retrospective information regarding the children's middle ear history from medical records or parent report. Collett et al. (2010) also used parent reported hearing/middle ear history data and Anderson et al. (2016) derived a variable regarding middle ear function using tympanometry data.
Lemos and Feniman (2010) highlight the challenges of using parent reported hearing/middle ear history data, as did Whitehill et al. (2003). Lemos and Feniman (2010) did not look at associations between hearing and performance on their input processing task but did suggest that differences in performance between children with and without clefts on the input processing task may be associated with a history of middle ear problems in the cleft group.
The variation between the hearing/middle‐ear function variables used in such studies makes comparing hearing/middle ear function related findings difficult. It is important to consider the nature of the variables used and not to overgeneralize any interpretation. Hearing/middle ear function variables may vary in relation to age, developmental stage, frequency, type or degree of problem with or intervention for hearing/middle ear function potentially altering the impact of the hearing/middle ear function variable on the outcome variable (Hall et al. 2017, Whitton and Polley 2011). Establishing and agreeing consistent, robust, meaningful and comparable hearing and/or middle ear function variables for speech and speech processing relating studies is a considerable challenge but important and would benefit from further work.
Clinical implications
This review highlights the variability in the limited current literature exploring speech input processing in children born with CP±L and its relationship with cleft specific SSD. This limited evidence indicates that there may be differences in some speech input processing skills (e.g., discrimination of minimal and repeated contrast non‐word pairs, categorical perception of a specific minimal pair and sound indication task) between children born with and without CP+/L. There was also some evidence that children born with CP±L may only have speech input processing difficulties in comparison with their non‐cleft peers and other children born with CP±L, for specific sounds with which they make errors in their speech output.
Clinicians should consider the possibility that a child born with CP+/L may have problems with speech input processing related to their cleft‐related SSD. Speech and Language Therapy assessment of children born with CP+/L should include elements of speech input processing in order to gain a thorough understanding of the nature of their SSD and include speech input processing in their intervention planning if children present with difficulties.
It is important to give careful consideration to the precise speech input processing skills being assessed and the requirements of the assessment task(s) being used in order to rule in or out specific speech input processing skills as a factor in a child's SSD. Hearnshaw et al. (2019) stated that reliable methods for assessing speech input processing in children with SSD are not yet available. The same challenge applies to children with cleft‐related SSD, particularly in relation to tasks which assess children's speech input processing of sounds they produce in error. CSCs are not all easily reproducible by an adult to accurately mimic a child's output errors for use in a speech input processing task. Until appropriate and reliable assessment tools are developed, clinicians should assess children's input processing of the CSCs they produce with the tools currently available to them, mindful of potential differences between the child's specific production errors and an adult reproduction of these errors when interpreting findings.
Identification of any speech input processing difficulties in children born with CP±L should also prompt consideration of potential difficulties with related areas such as language and literacy (Rvachew 2006), particularly given the emerging evidence that children born with clefts have poorer education outcomes than children not born with a cleft (Wehby et al. 2015, Grewal et al. 2020).
Limitations
This review only included studies published in peer‐reviewed journals introducing some risk of publication bias and the possibility that additional relevant studies in the grey literature (e.g., PhD theses) may not have been included. The implications and recommendations based on the findings of this review should be considered in the context of the very limited evidence available regarding speech input processing skills in children born with CP+/L. The heterogeneity within cleft groups of the studies included should be taken into account in this regard, given the evidence that different cleft subtypes have different aetiologies (Sharp et al. 2017). This impacts on the ability to make clinical interpretations. This may have been minimized if we had only included studies where participants in the cleft group had a diagnosis of CP±L, excluding studies that included participants with cleft lip ± alveolus. However, this would have resulted in fewer than six included papers and would not have highlighted some of the methodological considerations for future work. In addition, the relatively broad definition of a speech input processing task used means that assessment tasks used in included studies were not comparable. However, as so few studies have explored any aspect of speech input processing in children born with CP±L, this review serves as a baseline from which future research can build.
CONCLUSIONS
The current research evidence about the speech input processing skills of children born with CP±L and any associations with speech output is limited. There is therefore a need for further work to develop our understanding of these skills in this population and any relationships between them and the well‐documented cleft‐related speech output problems. This is important in order to provide the best evidence base possible for clinicians.
Methodological considerations highlighted in this review are important in relation to future work. In particular, the nature and diagnosis(es) included in the study group, the nature of the speech input processing and speech output assessment tasks used in relation to the research question and how they are described in the methodology to ensure readers are able to effectively interpret findings. It is also important to give adequate consideration to potential confounding factors in study design and analysis.
Further work to understand relationships between speech input processing, speech output and literacy development in children born with CP±L is indicated. In addition, examination of differences in the relationship between aspects of speech input processing and speech output in children with and without CP+/L presenting with SSD would inform clinicians regarding how to best manage these groups.
DECLARATION OF INTEREST
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
ACKNOWLEDGEMENTS
Lucy Southby, Clinical Doctoral Research Fellow (ICA‐CDRF‐2015‐01‐014), was funded by a Health Education England (HEE)/National Institute of Health Research (NIHR) Clinical Doctoral Research Fellowship for this research project. This publication presents independent research funded by the HEE/NIHR. The views expressed are those of the authors and not necessarily those of the NIHR, HEE, NHS or Department of Health and Social Care.
APPENDIX A.
TABLE A1.
Medline search string
| 1. cleft.tw. |
| 2. cleft lip.tw. |
| 3. cleft palate.tw. |
| 4. Cleft Lip/ |
| 5. (cleft lip and palate).tw. |
| 6. orofacial cleft.tw. |
| 7. cleft palate/ |
| 8. hare lip*.tw. |
| 9. harelip*.tw. |
| 10. palatoschisis.tw. |
| 11. facial cleft*.tw. |
| 12. oral cleft*.tw. |
| 13. craniofacial cleft*.tw. |
| 14. velopharyngeal insufficiency/ |
| 15. velopharyngeal insufficiency.tw. |
| 16. or/1–15 |
| 17. process*.tw. |
| 18. phonological.tw. |
| 19. awareness.tw. |
| 20. phonological awareness.tw. |
| 21. phonological processing.tw. |
| 22. psycholinguistic.tw. |
| 23. perception.tw. |
| 24. reading.tw. |
| 25. literacy.tw. |
| 26. spelling.tw. |
| 27. working memory.tw. |
| 28. psycholinguistic processing.tw. |
| 29. psycholinguistics.tw. |
| 30. speech perception.tw. |
| 31. verbal working memory.tw. |
| 32. auditory discrimination.tw. |
| 33. sound discrimination.tw. |
| 34. word discrimination.tw. |
| 35. or/17‐34 |
| 36. 16 and 35 |
| 37. limit 36 to english language |
APPENDIX B.
TABLE B1.
CASP quality appraisal scores
| (a) CASP quality appraisal of case‐control studies; questionsa and results (2 = yes, 1 = can't tell, 0 = no) for included papers, maximum score = 18 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Q1 Did the study address a clearly focused issue? | Q2 Did the authors use an appropriate method to answer their question? | Q3 Were the cases recruited in an acceptable way? | Q4 Were the controls selected in an acceptable way? | Q5 Was the exposure accurately measured to minimize bias? | Q6(b) Have the authors taken account of the potential confounding factors in the design and/or in their analysis? | Q9 Do you believe the results? | Q10 Can the results be applied to the local population? | Q11 Do the results of this study fit with other available evidence? | Total, n (%) |
| Baylis et al. (2008) | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 16 (88.9) |
| Collett et al. (2010) | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 16 (88.9) |
| Finnegan (1974) | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 1 | 1 | 14 (77.8) |
| Lemos and Feniman (2010) | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 16 (88.9) |
| Whitehill et al. (2003) | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 17 (94.4) |
| (b) CASP quality appraisal of cohort studies; questionsb and results (yes = 2, can't tell = 1, no = 0) for included papers, maximum score = 24 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Q1 Did the study address a clearly focused issue? | Q2 Was the cohort recruited in an acceptable way? | Q3 Was the exposure accurately measured to minimize bias? | Q4 Was the outcome accurately measured to minimize bias? | Q5(a) Have the authors identified all important confounding factors? | Q5(b) Have they taken account of the confounding factors in the design and/or analysis? | Q6(a) Was the follow‐up of subjects complete enough? | Q6(b) Was the follow‐up of subjects long enough? | Q9 Do you believe the results? | Q10 Can the results be applied to the local population? | Q11 Do the results of this study fit with other available evidence? | Q12 What are the implications of this study for practice? | Total, n (%) |
| Anderson et al. (2016) | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 20 (83.3) |
Note: aQuestions 6a, 7 and 8 are not included in the results as related to intervention studies specifically: Q6(a): Aside from the experimental intervention, were the groups treated equally?, Q7: How large was the treatment effect? and Q8: How precise was the estimate of the treatment effect?
Note: bQuestions 7 and 8 are not included in results as no numeric score applied to these items (Q7: What are the results of this study? and Q8: How precise are the results?).
Southby, L, Harding, S, Phillips, V, Wren, Y & Joinson, C. Speech input processing in children born with cleft palate: A systematic literature review with narrative synthesis. International Journal of Language & Communication Disorders, 2021;56: 668–693. 10.1111/1460-6984.12633
NOTES
See https://www.crd.york.ac.uk/prospero/ (accessed on 6 May 2020) (CRD42017062498).
See https://casp‐uk.net/casp‐tools‐checklists/ (accessed on 2 February 2021).
See http://www.prisma‐statement.org/ (accessed 23 December 2019).
DATA AVAILABILITY STATEMENT
Data sharing is not applicable—no new data were generated, or the article describes entirely theoretical research.
REFERENCES
- Anderson, L., Scarini, N. & Morris, H. (2016) Phonological awareness skills in children with cleft lip and/or palate. Journal of Clinical Practice in Speech–Language Pathology, 18 (1), 34–40. [Google Scholar]
- Baker, E., Croot, K., McLeod, S. & Paul, R. (2001) Psycholinguistic models of speech development and their application to clinical practice. Journal of Speech, Language, and Hearing Research, 44(3), 685–702. 10.1044/1092-4388(2001/055) [DOI] [PubMed] [Google Scholar]
- Baylis, A.L., Munson, B. & Moller, K.T. (2008) Factors affecting articulation skills in children with velocardiofacial syndrome and children with cleft palate or velopharyngeal dysfunction: A preliminary report. The Cleft Palate–Craniofacial Journal, 45 (2), 193–207. 10.1597/06-012.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bessell, A., Sell, D., Whiting, P., Roulstone, S., Albery, L., Persson, M., et al. (2013) Speech and language therapy interventions for children with cleft palate: A systematic review. The Cleft Palate–Craniofacial Journal, 50 (1), e1–e17. 10.1597/11-202 [DOI] [PubMed] [Google Scholar]
- Booth, A. & Fry‐Smith, A. (2003) Developing the research question. In: Topfer L. and Austin I. (Eds.) Etext on Health Technology Assessment (HTA) Information Resources (National Information Center on Health Services Research and Health Care Technology). Available at: https://www.nlm.nih.gov/archive/20060905/nichsr/ehta/chapter2.html (accessed on 15 July 2019). [Google Scholar]
- Britton, L., Albery, L., Bowden, M., Harding‐Bell, A., Phippen, G. & Sell, D. (2014) A cross‐sectional cohort study of speech in five‐year‐olds with cleft palate ± lip to support development of national audit standards: benchmarking speech standards in the United Kingdom. The Cleft Palate–Craniofacial Journal, 51(4), 431–51. 10.1597/13-121 [DOI] [PubMed] [Google Scholar]
- Brosseau‐Lapré, F. & Rvachew, S. (2017) Underlying manifestations of developmental phonological disorders in French‐speaking pre‐schoolers. Journal of Child Language, 44, 1337–1361. 10.1017/S0305000916000556 [DOI] [PubMed] [Google Scholar]
- Brosseau‐Lapré, F. & Roepke, E. (2019) Speech errors and phonological awareness in children ages 4 and 5 years with and without speech sound disorder. Journal of Speech Language and Hearing Research, 62, 3276–3289. 10.1044/2019_JSLHR-S-17-0461 [DOI] [PubMed] [Google Scholar]
- Burt, A.H.B.D.L. (1999) Phonological awareness skills of 4‐year‐old British children: an assessment and developmental data. International Journal of Language & Communication Disorders, 34(3), 311–335. 10.1080/136828299247432 [DOI] [PubMed] [Google Scholar]
- Carroll, J.M., Snowling, M.J., Stevenson, J. & Hulme, C. (2003) The development of phonological awareness in preschool children. Developmental psychology, 39(5), 913–923. 10.1037/0012-1649.39.5.913 [DOI] [PubMed] [Google Scholar]
- Chapman, K.L. (1993) Phonologic processes in children with cleft palate. Cleft Palate–Craniofacial Journal, 30(1), 64–72. 10.1597/1545-1569_1993_030_0064_ppicwc_2.3.co_2 [DOI] [PubMed] [Google Scholar]
- Chapman, K.L. & Willadsen, E. (2011) The development of speech in children with cleft palate. In: Howard S. and Lohmander A. (Eds.) Cleft Palate Speech: Assessment and Intervention. Chichester: Wiley‐Blackwell, pp. 23–40. [Google Scholar]
- Choa, R.M., Slator, R., Jeremy, A., Robinson, S., Franklin, D., Roberts, A., et al. (2014) Identifying the effect of cleft type, deprivation and ethnicity on speech and dental outcomes in UK cleft patients: A multi‐centred study. Journal of Plastic, Reconstructive & Aesthetic Surgery, 67, 1637–1643. 10.1016/j.bjps.2014.07.018 [DOI] [PubMed] [Google Scholar]
- Collett, B.R., Stott‐Miller, M., Kapp‐Simon, K.A., Cunningham, M.L. & Speltz, M.L. (2010) Reading in children with orofacial clefts versus controls. Journal of Pediatric Psychology, 35, 199–208. 10.1093/jpepsy/jsp047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conrad, A.L., Mccoy, T.E., Devolder, I., Richman, L.C. & Nopoulos, P., (2014) Reading in subjects with an oral cleft: Speech, hearing and neuropsychological skills. Neuropsychology, 28(3), 415. 10.1037/neu0000024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dodd, B. & McCormack, P. (1995) Differential diagnosis of phonological disorders. In: Dodd B. (Ed) Differential diagnosis and treatment of children with speech disorder. London England: Whurr Publishers Ltd, pp. 44–70. [Google Scholar]
- Eadie, P., Morgan, A., Ukoumunne, O.C., Ttofari Eecen, K.Wake, M. & Reilly, S. (2015) Speech sound disorder at 4 years: Prevalence, comorbidities, and predictors in a community cohort of children. Developmental Medicine & Child Neurology, 57(6), 578–584. 10.1111/dmcn.12635. [DOI] [PubMed] [Google Scholar]
- Finnegan, D.E. (1974) Speech sound discrimination skills of seven and eight‐year‐old cleft palate males. The Cleft Palate Journal, 11, 111–121. [PubMed] [Google Scholar]
- Grewal, S.S., Ponduri, S., Leary, S.D., Wren, Y., Thompson, J.M., Ireland, A.J., et al. (2020) Educational attainment of children born with unilateral cleft lip and palate in the United Kingdom. The Cleft Palate–Craniofacial Journal, 1–10. 10.1177/1055665620959989 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall, A., Wills, A., Mahmoud, O., Sell, D., Waylen, A., Grewal, S., et al. (2017) Centre‐level variation in outcomes and treatment for otitis media with effusion and hearing loss and the association of hearing loss with developmental outcomes at ages 5 and 7 years in children with non‐syndromic unilateral cleft lip and palate: the Cleft Care UK study. Part 2. Orthodontics & Craniofacial Research, 20, 8–18. 10.1111/ocr.12184 [DOI] [PubMed] [Google Scholar]
- Harding, A. & Grunwell, P. (1996) Characteristics of cleft palate speech. European Journal of Disorders of Communication, 31(4), 331–357. 10.3109/13682829609031326 [DOI] [PubMed] [Google Scholar]
- Harding, A. & Grunwell, P. (1998) Active versus passive cleft‐type speech characteristics. International Journal of Language & Communication Disorders, 33(3), 329–352. 10.1080/136828298247776 [DOI] [PubMed] [Google Scholar]
- Hardwicke, J.T., Landini, G. & Richard, B.M. (2014) Fistula incidence after primary cleft palate repair: A systematic review of the literature. Plastic and reconstructive surgery, 134(4), 618e–627e. 10.1097/PRS.0000000000000548 [DOI] [PubMed] [Google Scholar]
- Hearnshaw, S., Baker, E. & Munro, N. (2019) Speech perception skills of children with speech sound disorders: A systematic review and meta‐analysis. Journal of Speech, Language, and Hearing Research, 62(10), 3771–3789. 10.1044/2019_JSLHR-S-18-0519 [DOI] [PubMed] [Google Scholar]
- Hewlett, N., Gibbon, F. & Cohen‐Mckenzie, W. (1998) When is a velar an alveolar? Evidence supporting a revised psycholinguistic model of speech production in children. International Journal of Language & Communication Disorders, 33(2), 161–176. 10.1080/136828298247811 [DOI] [PubMed] [Google Scholar]
- Higgins, J.P.T. & Green, S. (Eds.) (2011) Cochrane handbook for systematic reviews of interventions (Version 5.1.0). The Cochrane Collaboration . Retrieved from http://www.cochrane.org/training/cochrane-handbook
- John, A., Sell, D., Sweeney, T., Harding‐Bell, A. & Williams, A., (2006) The cleft audit protocol for speech—augmented: A validated and reliable measure for auditing cleft speech. The Cleft Palate–Craniofacial Journal, 43(3), 272–288. 10.1597/04-141.1 [DOI] [PubMed] [Google Scholar]
- Klintö, K., Salameh, E.K. & Lohmander, A. (2016) Phonology in Swedish‐speaking 5‐year‐olds born with unilateral cleft lip and palate and the relationship with consonant production at 3 years of age. International Journal of Speech–Language Pathology, 18(2), 147–156. 10.3109/17549507.2015.1081287 [DOI] [PubMed] [Google Scholar]
- Lemos, I.C.C. & Feniman, M.R. (2010) Sustained auditory attention ability test (SAAAT) in seven‐year‐old children with cleft lip and palate. Brazilian Journal of Otorhinolaryngology, 76(2), 199–205. 10.1590/S1808-86942010000200009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lieberman, A.M. & Mattingly, I.G. (1985) The motor theory of speech perception revised. Cognition, 21(1), 1–36. 10.1016/0010-0277(85)90021-6 [DOI] [PubMed] [Google Scholar]
- Locke, J.L. (1980) The inference of speech perception in the phonologically disordered child. Part I: A rationale, some criteria, the conventional tests. Journal of Speech and Hearing Disorders, 45(4), 431–444. 10.1044/jshd.4504.431 [DOI] [PubMed] [Google Scholar]
- Lof, G.L. & Synan, S.T. (1997) Is there a speech discrimination/perception link to disordered articulation and phonology? A review of 80 years of literature. Contemporary Issues in Communication Science and Disorders, 24(Spring), 57–71. 10.1044/cicsd_24_S_57 [DOI] [Google Scholar]
- Lohmander, A. (2011) Surgical intervention and speech outcomes in cleft lip and palate. In: Howard S. and Lohmander A. (Eds.) Cleft palate speech: Assessment and intervention. Chichester: John Wiley & Sons, pp. 55–82. [Google Scholar]
- Lohmander, A. & Persson, C. (2008) A longitudinal study of speech production in Swedish children with unilateral cleft lip and palate and two‐stage palatal repair. The Cleft Palate–Craniofacial Journal, 45, 32–41. 10.1597/06-123.1 [DOI] [PubMed] [Google Scholar]
- McLeod, S. & Baker, E. (2017) Children's Speech: An evidence‐based approach to assessment and intervention. Boston: Pearson. [Google Scholar]
- Morris, H. & Ozanne, A. (2003) Phonetic, phonological, and language skills of children with a cleft palate. The Cleft Palate–Craniofacial Journal, 40(5), 460–470. 10.1597/1545-1569_2003_040_0460_ppalso_2.0.co_2 [DOI] [PubMed] [Google Scholar]
- Murphy, C.F., Pagan‐Neves, L.O., Wertzner, H.F. & Schochat, E. (2014) Auditory and visual sustained attention in children with speech sound disorder. PLoS One, 9(3), e93091. 10.1371/journal.pone.0093091 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nijland, L. (2009) Speech perception in children with speech output disorders. Clinical Linguistics and Phonetics, 23(3), 222–239. 10.1080/02699200802399947 [DOI] [PubMed] [Google Scholar]
- Persson, C., Lohmander, A. & Elander, A. (2006) Speech in children with an isolated cleft palate: A longitudinal perspective. The Cleft Palate–Craniofacial Journal, 43(3), 295–309. 10.1597/04-071.1 [DOI] [PubMed] [Google Scholar]
- Preston, J. & Edwards, M.L. (2010) Phonological awareness and types of sound errors in preschoolers with speech sound disorders. Journal of Speech, Language, and Hearing Research, 53(1), 44–60. 10.1044/1092-4388(2009/09-0021) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rees, R. (2001) What do tasks really tap? In: Stackhouse J. and Wells B. (Eds.) Children's speech and literacy difficulties 2: Identification and intervention. London: Whurr, pp. 66–95. [Google Scholar]
- Rvachew, S. (2006) Longitudinal predictors of implicit phonological awareness skills. American Journal of Speech–Language Pathology, 15(2), 165–176. 10.1044/1058-0360(2006/016) [DOI] [PubMed] [Google Scholar]
- Rvachew, S. & Bernhardt, B.M. (2010) Clinical implications of dynamic systems theory for phonological development. American Journal of Speech–Language Pathology, 19(1), 34–50. 10.1044/1058-0360(2009/08-0047). [DOI] [PubMed] [Google Scholar]
- Rvachew, S., Chiang, P.‐Y. & Evans, N. (2007) Characteristics of speech errors produced by children with and without delayed phonological awareness skills. Language, Speech, and Hearing Services in Schools, 38(1), 60–71. 10.1044/0161-1461(2007/006) [DOI] [PubMed] [Google Scholar]
- Shriberg, L.D., Lohmeier, H.L., Strand, E.A. & Jakielski, K.J. (2012) Encoding, memory, and transcoding deficits in childhood apraxia of speech. Clinical linguistics & phonetics, 26(5), 445–482. 10.3109/02699206.2012.655841 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sell, D., Grunwell, P., Mildinhall, S., Murphy, T., Cornish, T.A., Bearn, D., et al. (2001) Cleft lip and palate care in the United Kingdom–the Clinical Standards Advisory Group (CSAG) Study. Part 3: Speech outcomes. Cleft Palate–Craniofacial Journal, 38(1), 30–7. 10.1597/1545-1569_2001_038_0030_clapci_2.0.co_2 [DOI] [PubMed] [Google Scholar]
- Sell, D., Mildinhall, S., Albery, L., Wills, A.K., Sandy, J.R. & Ness, A.R. (2015) The Cleft Care UK study. Part 4: perceptual speech outcomes. Orthodontics & Craniofacial Research, 18 (Suppl. 2), 36–46. 10.1111/ocr.12112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sell, D., Southby, L., Wren, Y., Wills, A., Hall, A., Mahmoud, O., et al. (2017) Centre‐level variation in speech outcome and interventions, and factors associated with poor speech outcomes in 5‐year‐old children with non‐syndromic unilateral cleft lip and palate: the Cleft Care UK study. Part 4. Orthodontics & Craniofacial Research, 20, 27–39. 10.1111/ocr.12186 [DOI] [PubMed] [Google Scholar]
- Sharp, G.C., Ho, K., Davies, A., Stergiakouli, E., Humphries, K., McArdle, W., et al. (2017) Distinct DNA methylation profiles in subtypes of orofacial cleft. Clinical Epigenetics, 9, 63. 10.1186/s13148-017-0362-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stackhouse, J. (2001) Identifying children at risk for literacy problems. In: Stackhouse J. and Wells B. (Eds.) Children's speech and literacy difficulties 2: Identification and intervention. London: Whurr, pp. 1–40. [Google Scholar]
- Stackhouse, J., Vance, M., Pascoe, M. & Wells, B. (2007) Compendium of auditory and speech tasks: Children's speech and literacy difficulties 4. Chichester: Wiley. [Google Scholar]
- Stackhouse, J. & Wells, B. (1993) Psycholinguistic assessment of developmental speech disorders. European Journal Disord Communs, 28(4), 331–348. 10.3109/13682829309041469 [DOI] [PubMed] [Google Scholar]
- Stackhouse, J. & Wells, B. (1997) Children's speech and literacy difficulties: A psycholinguistic framework. London: Whurr. [Google Scholar]
- Sutherland, D. & Gillon, G.T. (2007) Development of phonological representations and phonological awareness in children with speech impairment. International Journal of Language & Communication Disorders, 42, 229–250. 10.1080/13682820600806672 [DOI] [PubMed] [Google Scholar]
- Walker, G.M. & Hickok, G. (2016) Bridging computational approaches to speech production: the semantic–lexical–auditory–motor model (SLAM). Psychonomic bulletin & review, 23(2), 339–352. 10.3758/s13423-015-0903-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waylen, A., Mahmoud, O., Wills, A.K., Sell, D., Sandy, J.R. & Ness, A.R. (2017) Centre‐level variation in behaviour and the predictors of behaviour in 5‐year‐old children with non‐syndromic unilateral cleft lip: the Cleft Care UK study. Part 5. Orthodontics & Craniofacial Research, 20, 40–47. 10.1111/ocr.12187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wheby, G.L., Collett, B.R., Barron, S., Romitti, P. & Ansley, T. (2015) Children with oral clefts are at greater risk for persistent low achievement in school than classmates. Archives of disease in childhood, 100(12), 1148–1154. 10.1136/archdischild-2015-308358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitehill, T.L., Francis, A.L. & Ching, C.K.Y. (2003) Perception of place of articulation by children with cleft palate and posterior placement. Journal of Speech, Language, and Hearing Research, 46, 451–461. 10.1044/1092-4388(2003/037) [DOI] [PubMed] [Google Scholar]
- Whitton, J.P. & Polley, D.B. (2011) Evaluating the perceptual and pathophysiological consequences of auditory deprivation in early postnatal life: A comparison of basic and clinical studies. Journal of the Association for Research in Otolaryngology, 12(5), 535–547. 10.1007/s10162-011-0271-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willadsen, E., Lohmander, A., Persson, C., Boers, M., Kisling‐Møller, M., Havstam, C., et al. (2019) Scandcleft project, trial 1: comparison of speech outcome in relation to timing of hard palate closure in 5‐year‐olds with UCLP. The Cleft Palate–Craniofacial Journal, 56(10), 1276–1286. 10.1177/1055665619854632 [DOI] [PubMed] [Google Scholar]
- Willadsen, E., Lohmander, A., Persson, C., Lundeborg, I., Alaluusua, S., Aukner, R., et al. (2017) Scandcleft randomised trials of primary surgery for unilateral cleft lip and palate: 5. Speech outcomes in 5‐year‐olds‐consonant proficiency and errors. Journal of Plastic Surgery and Hand Surgery, 51(1), 38–51. 10.1080/2000656X.2016.1254647 [DOI] [PubMed] [Google Scholar]
- Wren, Y., Humphries, K., Stock, N.M., Rumsey, N., Lewis, S., Davies, A., et al. (2018) Setting up a cohort study in speech and language therapy: lessons from The UK Cleft Collective Speech and Language (CC‐SL) study. International Journal of Language & Communication Disorders, 53(3), 421–430. 10.1111/1460-6984.12364 [DOI] [PubMed] [Google Scholar]
- Wren, Y., Miller, L.L.Peters, T.J., Emond, A. & Roulstone, S. (2016) Prevalence and predictors of persistent speech sound disorder at eight years old: Findings from a population cohort study. Journal of Speech, Language and Hearing Research, 59(4), 647–673. 10.1044/2015_JSLHR-S-14-028 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable—no new data were generated, or the article describes entirely theoretical research.