

Abstract
Aim
To develop the caring model and utilize and evaluate the effect of the model in the nursing student's learning process in burn wards.
Design
A longitudinal multiphase study.
Methods
In the first phase, "Coming back to existence caring model" was developed, in the second phase, to evaluate the program, 35 students in the first semester and 31 students in the second semester of the 2017–2018 academic year were selected randomly, and their logbooks were analysed.
Results
Components of the nursing process, based on the model, were wound management, care and documentation, early mobilization, discharge planning and patient education. The lowest nursing process utilization in both semesters was in the sexuality domain. The most nursing diagnosis was a risk for infection. In the discharge plan, education about how the patient communicates with others in the second semester was less than other educational content (61/3%). However, empowering students was remarkable.
Keywords: burns, education, nursing, nursing processes, students
1. INTRODUCTION
Clinical education forms the core of nursing education and plays a key role in forming the identity of the nursing profession (Mudaly & Mtshali, 2018). Clinical learning activities provide a real‐life learning experience and the opportunity to transfer knowledge to practical situations (Flood & Robinia, 2014). The application of nursing scientific knowledge in practice is possible in the use of nursing theories and models in care (Bond et al., 2011). Despite this, studies have shown that there are multiple problems such as inconsistency between theoretical lessons and clinical work, the lack of clarity of the goals of clinical education, the lack of realistic evaluations and educational facilities, are obstacles to achieving the goals of this period (Arkan et al., 2018; Fiset et al., 2017). In fact, clinical abilities obtained by students are not in a favourable position, and they have not acquired the skills and abilities required at the end of their education (Bennett & Jan Rodd, 2017).
To perform a clinical decision‐making process, it is necessary to examine and identify the problem, evaluate the existing solutions, and ultimately select the best option; this process is carried out at the clinic through the nursing process, and in fact, a nursing process is a tool for helping the nurse to make appropriate clinical decision‐making and critical thinking (Guerrero, 2019). The nursing process model involves assessing, planning, implementing and evaluating patient situations, with the ultimate goal of preventing or resolving problematic situations (Benedet et al., 2018).
The burn is one of the main and common health problems that face the victims with significant challenges in their lives (Elsherbiny et al., 2011). A nurse, who cares for a patient with a burn, injuries requires a high level of knowledge about post‐burn physiological changes as well as accurate examination skills to determine minor changes in the patient's condition (Knighton, 2020). Current worldwide reports indicate insufficient knowledge of first aid and initial management for burns amongst nurses (AL‐Sudani & Ali, 2017; Kut et al., 2005). Reviews of the literature conducted in Iran indicate that the nursing process in Iran is not practically implemented or is performed incompletely (Rajabpoor et al., 2018; Moghadas & Sedaghati Kesbakhi, 2020; Ghafouri Fard et al., 2012; Zamanzadeh et al., 2015). Successful internship programs (AL‐Mahmood et al., ; Neto et al., 2018) and using a grounded comprehensive holistic care model (Lotfi, 2014) have an effective role in the implementation of the nursing process.
There are many models in nursing, such as the Roy adaptation model, which, while being holistic and paying attention to the four basic dimensions in human beings, has paid less attention to spiritual health (Meleis, 2011). Or in the biological, psychological and social care model of maladaptation, all nursing steps are described; however, the focus is generally on the process of adapting to malnutrition, and its use to returning patients to the community is not clear (Zamanzadeh et al., 2014). Fisher's model of spiritual health and well‐being, despite paying attention to spiritual health, does not have instructions for clinical use (Fisher, 2013). Furthermore, a review of the literature showed that although the issue of burns has been considered by researchers in various dimensions, attention is often paid to their physical and beauty problems than to the process of bringing them back to the community (Fauerbach et al., 2007; Willebrand et al., 2002; Zamanzadeh et al., 2014). "Coming back to existence caring model" can cover the deficiencies of previous models (Lotfi, 2014), and a nursing plan based on it can be useful in improving the skills of nursing students in the implementation of the nursing process and improve understanding of patients' conditions and their easier return to the community.
Therefore, due to the lake of a study on the process of returning these patients to the community, the lack of evidence on a model‐based approach to care, standardization in burn nursing care and incomplete implementation of the nursing process in Iran, a nursing plan was developed based on the model and implemented, and 35 Students' logbooks in the first semester and 31 students' logbooks in the second semester of the 2017–2018 academic year were selected randomly and analysed.
2. METHODS
2.1. Study design and participants
The study comprised two phases that started in September 2014, and it is still ongoing.
In the first phase, the nursing plan was developed according to the “Coming back to existence caring model.” This model is comprehensive nursing care consistent with the available substitution and needs of Iranian society. To investigate how patients with burns return to the community, the qualitative study was designed using grounded theory. After analysis of 23 interviews with 16 participants, four themes were extracted as follows: A) matrix of self (context), including factors affecting the returning process, B) self‐disruption (main concerns), C) locating (strategies), including the solutions adopted by individuals in the returning process, and D) Balance (outcome). Returning to life outcomes were physical integration, connecting to the lifestream, and return to existence (Zamanzadeh et al., 2014). Since burn disturbances affect all aspects of patients' existence, and balance is achieved through complex mental processes of locating and matrix context, the proposed model for helping patients need to be holistic, considering all their physical, mental, spiritual and value dimensions in the form of their matrix. The present model is called the “Coming back to existence caring model.” Its ultimate goal is to improve the level of inner satisfaction of the individual in all dimensions, and ultimately, to accept oneself as a transcendent human being. The model is presented in two general sections, structure and main stages. The structure of the model includes the ideas and beliefs, goals, knowledge, and skills required. We have used the model steps in this study, which include four basic steps based on the nursing process to achieve the model goal (Figure 1).
FIGURE 1.
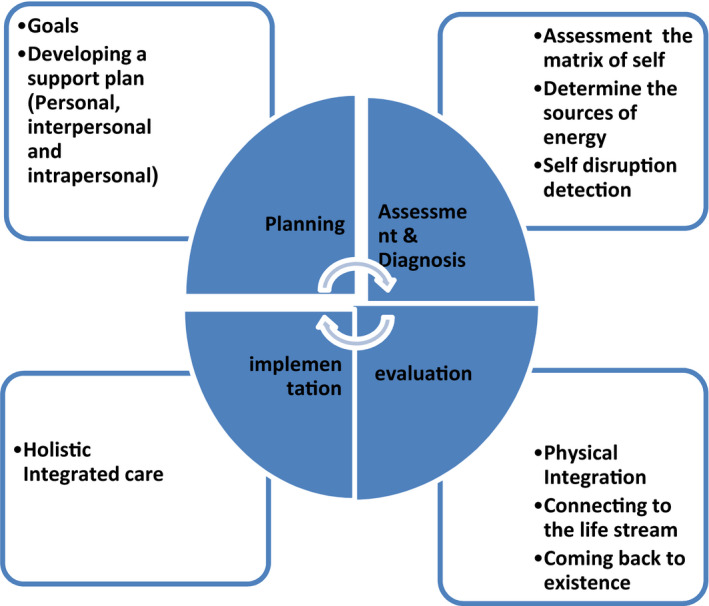
Nursing process according to “Coming back to existence caring model”
In the nursing process, the first action of the nurse, after obtaining general information in different areas of patients’ matrix (background), is to assess their condition and examine the main consequences of burns using various methods such as observation and interview in different dimensions, and afterwards, to identify the type of rupture (physical, mental, interactive and equilibrium) using the collected information, and locating that, including the positive (such as commitment) and negative (such as passive) strategies used by the individual to protect themselves to determine nursing diagnoses and planning. The goal of planning is to achieve balance. After performing the appropriate interventions, the evaluation of the level of balance is performed with regard to achieving physical integrity, connecting to the lifestream, and returning to oneself.
In the following, according to the curriculum of BS in nursing and medical–surgical course content (adults / elderly 3) training, logbook related to the nursing process in burn patients was designed by the research team. Afterwards, the logbook ran for two years in nursing students' training in burn wards in pilot form, and the logbook, the educational content, the registration section of the care program and its educational processes were modified and finalized in each semester on the basis of feedback received from students and Nursing Instructors. Nursing Care and completion of the logbook of each patient was done by senior students under the supervision of a Nursing Instructor during the internship program of elderly/adults 3 in the burn wards at the Sina Hospital of Tabriz.
In the second phase, to test the program and to evaluate the effect of the model in the learning process, 35 Students' logbooks in the first semester and 31 Students' logbooks in the second semester of the 2017–2018 academic year were selected randomly and analysed. All educational logbooks were selected, and their details were analysed.
2.2. Statistical analysis
In the second phase, data were analysed using the Statistical Package for Social Sciences (SPSS) 16.0. Categorical variables were described as relative frequency (%) and compared with the chi‐square or Fisher exacts tests. The results were considered statistically significant if p < .05.
2.3. Ethics
Ethical approval for the study was received by the Ethics Committee in Research Affairs, Tabriz University of Medical Sciences; NO: TBZMED.REC.1394. 462.
3. RESULTS
In the first phase, the nursing care plan was designed according to the “Coming back to existence caring model” and applied in the burn wards to empower nursing students to apply the Nursing Process. The components include wound management in terms of colour and texture, signs of infection, healing, care, and documentation, early mobilization, discharge planning, and patient education about how burns affect limb function, the healing process and returning to pre‐burn conditions, potential problems and complications after discharge, taking medication at home, nutrition, wound caring, communication with others, movement, and physical limitations, and setting time of referral for follow‐up after discharge. After designing the model in the form of a logbook, it was delivered to each student by the instructor, who is one of the researchers, and completed by them.
In the second phase, total records including Steps of the nursing process registered in the logbooks by the students were analysed.
Table 1 illustrates the patients’ socio‐demographic characteristics and burn‐related health status assessment registered in the logbooks. In the second semester, students' performance in assessing the nutritional status of patients improved, and in the first semester, the rate of registered specialized treatment received by patients was higher (p ≤ .05).
TABLE 1.
Socio‐demographic characteristics and burn‐related health status assessment Registered in the logbooks
| first semester(n = 35) | Second semester(n = 31) | * p | |||
|---|---|---|---|---|---|
| A) Personal‐ social characteristics | 35(100) | 31(100) | – | ||
| Burn percentage | 35(100) | 31(100) | – | ||
| Burn depth | 35(100) | 31(100) | – | ||
| Burn site | 35(100) | 31(100) | – | ||
|
Type of the specialized treatment received during hospitalization |
20(57/1) | 19(61/3) | .000 | ||
|
B) Health status related to burn |
Skin function | Burn wound healing | 34(97/1) | 30(96/8) | .5 |
| The stage of wound healing | 35(100) | 31(100) | – | ||
| Skin and mucosal changes | 34(97/1) | 28(90/3) | .335 | ||
| Perception of health | 33(94/3) | 31(100) | .494 | ||
| Nutrition status | 27(77/1) | 31(100) | .005 | ||
| Elimination and exchange status | 34(97/1) | 31(100) | 1.0 | ||
| Activity and mobility | 35(100) | 31(100) | – | ||
| Sleep and rest | 35(100) | 30(96/8) | – | ||
| Perceptional and Cognitive status | 34(97/1) | 31(100) | .530 | ||
| Self‐perception status/ self‐concept | 22(62/9) | 23(71/2) | .324 | ||
| Relationship‐ role status | 28(80) | 29(93/5) | .156 | ||
| sexual status | 18(51/4) | 18(58/1) | .589 | ||
| Stress tolerance/ coping status | 31(88/6) | 30(96/8) | .36 | ||
| Beliefs‐ values status | 16(45/7) | 14(45/2) | .58 | ||
Categorical variables expressed as n (%).
Chi‐Square or Fisher exacts tests Test
According to the above table, the type of specialized treatment received during hospitalization and nutrition status assessment showed a significant difference in the two semesters (p ≤ .05). The lowest domains assessed were the patient's sexual status, beliefs and values in both semesters. After the patient's assessment, a nursing diagnosis was made about the patient's health status. After a comprehensive patient assessment, the students obtained relevant nursing diagnoses, which are shown in detail in the table below (Table 2).
TABLE 2.
Nursing diagnosis registered in the logbooks
| Second semester(n = 31) | first semester (n = 35) | Nursing diagnosis | |
|---|---|---|---|
| percentage | Percentage | ||
| 24(77/4) | 31(88/6) | Risk for infection | Skin function |
| 26(83/9) | 18(51/4) | Perception/ cognition deficient knowledge | |
| 15(48/4) | 9(25/7) | Nutrition less than body requirements | Nutrition status |
| 9(29) | 11(31/4) | Constipation | Elimination and exchange status |
| 7(22/6) | 12(34/3) | Fatigue | Activity and mobility |
| 16(51/6) | 10(28/6) | physical function disorder | |
| 18(58) | 20(57/2) | Sleep pattern disorder | Sleep and rest |
| 8(28/8) | 8(22/9) | Feeling lonely | Self‐perception / self‐concept |
| 12(38/7) | 6(17/1) | Impairment of parent's role | Relationship‐ role |
| 3(9/7) | 5(14/3) | sexual dysfunction | sexuality |
| 16(51/6) | 20(57/1) | Stress | Coping/Stress tolerance |
| 19(61/3) | 13(37/1) | Anxiety | |
| 9(29) | 11(31/4) | preparing for hope | Beliefs‐ values |
According to the above table, the most frequent diagnosis in the domain of skin function in both semesters was a risk for infection (88.6% and 77.4%, respectively). And in the domain of Perception/ cognition in both semesters was deficient knowledge (51/4% and 83/9%, respectively). The lowest nursing diagnosis in both semesters was in the sexuality domain.
After all, nursing diagnoses were related to the consequences of burn injury that each student recorded from his or her patient (Table 3).
TABLE 3.
Registration of nursing diagnosis related to burn consequences
|
Second semester n (%) |
first semester n (%) |
Nursing diagnosis |
|---|---|---|
| 25(80/6) | 29(82/9) | physical disability |
| 16(51/6) | 9(25/7) | Mental disorder |
| 8(25/8) | 6(17/1) | Social disorder |
| 0(0) | 2(5/7) | lack of Excellence |
| 0(0) | 5(14/3) | Non registered |
In the table above, in both semesters, the largest number of nursing diagnoses related to burn injury consequences was physical disability (82/9% and 80/6%, respectively), and the lowest nursing diagnosis was the lack of Excellence (5/7% and 0%, respectively). Furthermore, most students (85.7%) in the first semester and all students in the second semester were able to fulfil this section.
According to the nursing diagnosis, a care plan was performed and registered. Afterwards, interventions were evaluated to investigate the client's progress towards the achievement of goals or desired outcomes. In the analysis conducted in the first semester, 97.1% of the students had a care program, and 77.1% evaluated the interventions, and in the second semester, all of the students completed the care program and evaluated the interventions.
Early mobilization nursing process on the first day to the third day indicated that in the first semester, the patient ability assessment and related nursing diagnosis, implementation, and evaluation reduced from 97.1% on the first day to 85.7% on the second day and 62.9% on the third day. In the second semester, nursing process performance reduced from 100% on the first and second days to 74.2% on the third day.
After the doctor registered in the record that the patient could be discharged, the education sheet was completed, and after education, the related pamphlets were delivered to the patients.
Table 4(discharge planning by students in two semesters) is provided here:
TABLE 4.
Discharge planning by students in two semesters
|
Frequency (percentage) of students who have taught their patients |
Educational content | ||
|---|---|---|---|
| * p | Second semester | First semester | |
| .948 | 25(80/6) | 28(80) | Education about how burns affect limb function |
| .287 | 25(80/6) | 32(91/4) | the healing process and return to pre‐burn conditions |
| .408 | 27(87/1) | 33(94/3) | potential problems and complications after discharge |
| .134 | 25(80/6) | 33(94/3) | How to take medication at home |
| .659 | 28(90/3) | 33(94/3) | Nutrition |
| 28(90/3) | 32(91/4) | Mobility | |
| .240 | 26(83/9) | 33(94/3) | Wound caring |
| .876 | 19(61/3) | 23(65/7) | Communication with others |
| .596 | 21(67/7) | 26(83/9) | Movement and physical limitations |
| .514 | 21(67/7) | 21(67/7) | setting and time of referral for follow‐up after discharge |
Categorical variables expressed as n (%).
Chi‐Square or Fisher exacts tests Test
The table above indicates that although the number of content educated by students was higher in the first semester than the second semester, it is not statistically significant (p ≥ .05).
4. DISCUSSION
In the present study, the nursing care plan was designed according to the “Coming back to existence caring model” in Iran, in order to help patients to achieve an active and spiritual life. This model was tested in burn wards in nursing students' education in September 2014. Training based on this model empowered students in assessing the patient, nursing diagnoses related to burns, implementation, and evaluation of care, and training the patient during the discharge. It is expected that the description of this model will mediate the improvement of patient satisfaction, and the quality of nursing care. They help nurses to organize nursing care daily and allow them to offer higher quality care (Kaya et al., 2010). A review indicated that very little information was found indicating a theory‐based approach to care; a study that investigated the Development and Implementation of an Innovative Burn Nursing Handbook for Quality Improvement and showed that utilizing innovative educational tools such as a handbook improved education and overall fundamental burn knowledge of practicing nursing staff significantly (Olszewski et al., 2016). Works by (AL‐Sudani & Ali, 2017) showed that nurses could significantly improve their knowledge from 8.7%–100% right after attending a training course (AL‐Sudani et al., 2017). Another study proved that participating in training courses is an independent factor affecting knowledge level and emphasized the importance of healthcare providers’ attendance to regular training courses (Lam et al., 2018). Research studies concerning knowledge about the proper care of burn patients—conducted in Australia, the Netherlands, England and Brazil with health professionals, including nurses—have shown gaps in theoretical knowledge and its attendant technical‐assistance practices. Current worldwide reports indicate insufficient knowledge of first aid and initial management for burns among nurses (Alomar et al., 2016; AL‐Sudani et al., 2017; Kut et al., 2005). In a Canadian retrospective study aimed at investigating factors associated with the implementation of nursing diagnoses, the results showed that nurses tend to document nursing diagnoses at institutions that have formal educational programs and computer‐generated care plans (Higuchi et al., 1999). A study in Brazil showed that a smaller number of recordings were done in the steps relative to nursing diagnosis and evolution (Reppetto & Souza, 2005). A study in the same hospital showed that nurses' awareness of nursing diagnoses was very poor (Khajehgoodari et al., 2020). Studies on nursing documentation in Iran have focused more on the quality of nursing documentation. These studies have reported that the quality of nursing documentation was unsuitable and did not contain necessary information (Rajabpoor et al., 2018; Moghadas & Sedaghati Kesbakhi, 2020; Ghafouri Fard et al., 2012; Tab rizi et al., 2016; Zamanzadeh et al., 2015). Results of this study showed that the top prevalent nursing diagnoses were the risk for infection, which is consistent with the results of Khajehgoodari's study and case study by Vinicius Lino Souza Neto and colleagues (Khajehgoodari et al.; Neto et al., 2018). The results indicate the student's unfavourable status in the utilization of the nursing process in the sexuality domain. The reasons for this are the students' low experience in assessing the patient in the sexual domain during the education period, and the importance of examining this dimension in the clinic is insignificant. The findings of the present study can be included in the in‐service educational programs of clinical staff and training programs of nursing students to be useful in preventing or solving their problems by informing them about the problems of burn victims. According to the proposed model and the importance of the nursing process in providing comprehensive care, the findings of this study can be used in planning and implementing programs to continuously monitor the client's condition in the hospital, home and community to help him achieve the highest balance level which means gaining inner satisfaction and enjoying a meaningful life. Finally, the concepts extracted from the theory and model presented can be used as a conceptual framework for other research in this field. It is suggested that the implementation of the nursing process in the clinic be pursued more seriously in the educational curriculum of nursing students.
5. CONCLUSION
Due to the lack of standardization in burn nursing care, it is appropriate to integrate this model and practice or develop similar models in other burns wards. It seems that using a grounded comprehensive holistic care model has an effective role in the implementation of the nursing process, particularly in specialized care, such as burns. Therefore, designing a similar Holistic Nursing Care Model for burn patients in Iran is essential in order to help them to achieve an active and spiritual life. Improving Nursing Students' ability to implement Nursing Process in Burn Wards leads to quality of care and increases the patient survival and the quality of life.
CONFLICT OF INTEREST
There is no conflict of interest in the study.
ACKNOWLEDGEMENTS
We express our appreciation to all educators and students who participated in this study. We thank all the staff of the burn ward of sina teaching hospital in Tabriz for cooperating in this project. Special thank to departy of education of Tabriz nursing and medewifary faculty for supporting.
Lotfi M, Zamanzadeh V, Khodayari‐Zarnaq R, Mobasseri K. Nursing process from theory to practice: Evidence from the implementation of "Coming back to existence caring model" in burn wards. Nurs Open. 2021;8:2794–2800. 10.1002/nop2.856
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- Alomar, M., Al Rouqi, F., & Eldali, A. (2016). Knowledge, attitude, and belief regarding burn first aid among caregivers attending pediatric emergency medicine departments. Burns, 42(4), 938–943. 10.1016/j.burns.2016.03.019. [DOI] [PubMed] [Google Scholar]
- AL‐Sudani, A., & Ali, E. (2017). Evaluation of an Educational Program on Nurses’ Practices for children with Burns Injuries attending Burns Specialist Hospital in Baghdad City. Journal of Nursing and Health Science, 6(4), 57–63. 10.9790/1959-0604015763. [DOI] [Google Scholar]
- Arkan, B., Ordin, Y., & Yılmaz, D. (2018). Undergraduate nursing students' experience related to their clinical learning environment and factors affecting to their clinical learning process. Nurse Education in Practice, 29, 127–132. 10.1016/j.nepr.2017.12.005. [DOI] [PubMed] [Google Scholar]
- Benedet, S. A., Padilha, M. I., Gelbke, F. L., & Bellaguarda, M. L. D. R. (2018). The model professionalism in the implementation of the Nursing Process (1979–2004). Revista Brasileira De Enfermagem, 71(4), 1907–1914. 10.1590/0034-7167-2017-0226. [DOI] [PubMed] [Google Scholar]
- Bennett, L. L., & Jan Rodd, M. (2017). The gap between nursing education and clinical skills. ABNF Journal, 28(4), 96–102. [Google Scholar]
- Bond, A. E., Eshah, N. F., Bani‐Khaled, M., Hamad, A. O., Habashneh, S., Kataua’, H., & Maabreh, R. (2011). Who uses nursing theory? A univariate descriptive analysis of five years’ research articles. Scandinavian Journal of Caring Sciences, 25(2), 404–409. 10.1111/j.1471-6712.2010.00835.x. [DOI] [PubMed] [Google Scholar]
- Elsherbiny, O. E. E., Salem, M. A., El‐Sabbagh, A. H., Elhadidy, M. R., & Eldeen, S. M. A. (2011). Quality of life of adult patients with severe burns. Burns, 37(5), 776–789. 10.1016/j.burns.2010.12.017. [DOI] [PubMed] [Google Scholar]
- Fauerbach, J. A., Bresnick, M. G., & Smith, M. T. (2007). Coping with Burn Injury: Research Summary and a New Model of~the~Influence of Coping on Psychological Complications. In Martz E., Livneh H. (Eds.), Coping with Chronic Illness and Disability. Boston, MA: Springer. 10.1007/978-0-387-48670-3_9. [DOI] [Google Scholar]
- Fiset, V. J., Graham, I. D., & Davies, B. L. (2017). Evidence‐based practice in clinical nursing education: A scoping review. Journal of Nursing Education, 56(9), 534–541. 10.3928/01484834-20170817-04. [DOI] [PubMed] [Google Scholar]
- Fisher, J. (2013). You can’t beat relating with God for spiritual well‐being: Comparing a generic version with the original spiritual well‐being questionnaire called SHALOM. Religions, 4(3), 325–335. 10.3390/rel4030325. [DOI] [Google Scholar]
- Flood, L. S., & Robinia, K. (2014). Bridging the gap: Strategies to integrate classroom and clinical learning. Nurse Education in Practice, 14(4), 329–332. 10.1016/j.nepr.2014.02.002. [DOI] [PubMed] [Google Scholar]
- Ghafouri Fard, M., Haririan, H., Aghajanloo, A., Akbari, M., & Shirvani, Y. (2012). Obstacles of nursing process application from perspective of the nursing instructor and nursing students in Zanjan faculty of nursing and midwifery. Journal of Medical Education Development, 5(8), 69–77. [Google Scholar]
- Guerrero, J. G. (2019). Practice rationale care model: The art and science of clinical reasoning, decision making and judgment in the nursing process. Open Journal of Nursing, 9(2), 79–88. 10.4236/ojn.2019.92008. [DOI] [Google Scholar]
- Higuchi, K. A. S., Dulberg, C., & Duff, V. (1999). Factors associated with nursing diagnosis utilization in Canada. International Journal of Nursing Terminologies and Classifications, 10(4), 137–147. 10.1111/j.1744-618X.1999.tb00044.x. [DOI] [PubMed] [Google Scholar]
- Kaya, N., Babadağ, K., Kaçar, G. Y., & Uygur, E. (2010). Hemşirelerin hemşirelik model/kuramlarını, hemşirelik sürecini ve sınıflama sistemlerini bilme ve uygulama durumları. Maltepe Üniversitesi Hemşirelik Bilim Ve Sanatı Dergisi, 3(3), 24–33. [Google Scholar]
- Khajehgoodari, M., Lotfi, M., Zamanzadeh, V., Valizadeh, L., & Khalilzad, P. (2020). Nursing diagnosis identification by nurses in burn wards: A descriptive cross‐sectional study. Nursing Open, 7(4), 980–987. 10.1002/nop2.470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knighton, J. (2020). Nursing Management of the Burn Patient. Handbook of Burns , Vol. 1 (pp. 347–384). Cham: Springer. 10.1007/978-3-030-18940-2_27. [DOI] [Google Scholar]
- Kut, A., Tokalak, I., Başaran, Ö., Moray, G., & Haberal, M. A. (2005). Knowledge, attitudes, and behavior of occupational physicians related to burn cases: A cross‐sectional survey in Turkey. Burns, 31(7), 850–854. 10.1016/j.burns.2005.04.009. [DOI] [PubMed] [Google Scholar]
- Lam, N., Huong, H., & Tuan, C. (2018). Nurse knowledge of emergency management for burn and mass burn injuries. Annals of Burns and Fire Disasters, 31(3), 246. [PMC free article] [PubMed] [Google Scholar]
- Lotfi, M. (2014). The process of returning burn patients to community and designing a model. (phd thesis in nursing). Faculty of nursing and midwifey. Tabriz University of Medical Sciences. [Google Scholar]
- Meleis, A. I. (2011). Theoretical nursing: Development and progress. Lippincott Williams & Wilkins. [Google Scholar]
- Mudaly, P. D., & Mtshali, N. G. (2018). Academic monitoring and support of undergraduate nursing education programme: A middle‐range theory. Curationis, 41(1), 1–11. 10.4102/curationis.v41i1.1881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moghadas, T., & Sedaghati Kesbakhi, M. (2020). Factors Influencing Implementation of Nursing Process by Nursing Students: A Qualitative Study. Journal of Medical Education, 19(4), 1–4. 10.5812/jme.110810. [DOI] [Google Scholar]
- Neto, V. L. S., da Silva Costa, R. T., de Lucena, E. A., da Silva, S. C., Pereira, V. M., & da Silva, R. A. R. (2018). Implementação do processo de enfermagem no paciente queimado: Um estudo de caso [Implementing the nursing process for a burn patient: A case study][Implementación del proceso de enfermería a paciente quemado: Un estudio de caso]. Revista Enfermagem UERJ, 26, 30962. [Google Scholar]
- Olszewski, A., Yanes, A., Stafford, J., Greenhalgh, D. G., Palmieri, T. L., Sen, S., & Tran, N. (2016). Development and implementation of an innovative burn nursing handbook for quality improvement. Journal of Burn Care & Research, 37(1), 20–24. 10.1097/BCR.0000000000000299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rajabpoor, M., Zarifnejad, G. H., Mohsenizadeh, S. M., Mazloum, S. R., Pourghaznein, T., Mashmoul, A., & Mohammad, A. (2018). Barriers to the implementation of nursing process from the viewpoint of faculty members, nursing managers, nurses, and nursing students. Journal of Holistic Nursing and Midwifery, 28(2).137–142. 10.29252/hnmj.28.2.137. [DOI] [Google Scholar]
- Reppetto, M. Â., & Souza, M. F. D. (2005). Avaliação da realização e do registro da sistematização da assistência de enfermagem (SAE) em um hospital universitário. Revista Brasileira De Enfermagem, 58(3), 325–329. 10.1590/S0034-71672005000300014. [DOI] [PubMed] [Google Scholar]
- Tabrizi, F. J., Rahmani, A., Jafarabadi, M. A., Jasemi, M., & Allahbakhshian, A. (2016). Unmet supportive care needs of Iranian cancer patients and its related factors. Journal of Caring Sciences, 5(4), 307–316. 10.15171/jcs.2016.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willebrand, M., Andersson, G., Kildal, M., & Ekselius, L. (2002). Exploration of coping patterns in burned adults: Cluster analysis of the coping with burns questionnaire (CBQ). Burns, 28(6), 549–554. 10.1016/S0305-4179(02)00064-5. [DOI] [PubMed] [Google Scholar]
- Zamanzadeh, V., Valizadeh, L., Lotfi, M., & Salehi, F. (2014). Burn survivors' experience of core outcomes during return to life: A qualitative study. Journal of Caring Sciences, 3(4), 227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zamanzadeh, V., Valizadeh, L., Tabrizi, F. J., Behshid, M., & Lotfi, M. (2015). Challenges associated with the implementation of the nursing process: A systematic review. Iranian Journal of Nursing and Midwifery Research, 20(4), 411. 10.4103/1735-9066.161002. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.