

Abstract
Aim
This study aimed to determine effectiveness of peanut ball on the duration of the stages of labour and frequency of caesarean section.
Design
A systematic review and meta‐analysis.
Method
A comprehensive electronic search was carried out with no time limit until December 2020. Collected data were analysed using software RevMan‐ version 5.3. Heterogeneity was assessed using I 2, T 2, and 2. GRADE approach was used to assess the certainty of evidence.
Results
The meta‐analysis on six clinical trials with 645 participants showed no statistically significant difference between the two groups in caesarean surgery rate (RR = 0.82) and length of the first (MD = −15.64).
Conclusions
Therefore, further clinical trials with stronger evidence should be carried out to assess the effectiveness of peanut ball on caesarean surgery rate and length of first and second stages of labour.
Keywords: caesarean section, labour, labour ball, peanut ball, systematic review
1. INTRODUCTION
Labour pain is unique, complex and multifactorial (Chao et al., 2007) with pain management being a key factor in gynaecological care and the main goal of delivery care (Qu & Zhou, 2007). Nevertheless, women who are not too afraid of labour can easily tolerate the pain. In this regard, personal experience, the expectation of family support and relationship with caregivers also affect women's perception of labour pain (Hodnett, 2002). Patients' preferences about labour are associated with both labour duration and pain relief (Favilli et al., 2018). Meanwhile, childbirth education classes focus on pain management during delivery, either through pharmaceutical or non‐pharmaceutical interventions (Brown et al., 2001).
Pharmaceutical approaches only relieve the physical sensation of pain while non‐pharmacological methods mainly help prevent pain through emotional, mental and spiritual interventions (Simkin & Bolding, 2004). Intravenous and intramuscular analgesic injection and local anaesthetic nerve block have different side effects and risk factors and are often used in hospitals (Lee & Ernst, 2004). However, various non‐pharmacological interventions for pain relief not only relieve the physical sensation of pain but also offer psychological intervention to inhibit feelings of pain (Brown et al., 2001; Simkin & Bolding, 2004). Non‐pharmacological interventions solely regard pain as a side effect of a normal delivery process (Tournaire & Theau‐Yonneau, 2007). These interventions include relaxation, breathing techniques, positioning, massage, hydrotherapy, hot and cold water therapy, music therapy, acupuncture, aromatherapy, electrical nerve stimulation and birth ball. These methods can be either used in combination or in a sequential manner for enhancing the overall effectiveness (Zwelling et al., 2006).
On average, 61% of pregnant women with singleton gestations are more likely to receive epidural anaesthesia in the United States (Osterman & Martin, 2011). According to the American College of Obstetrics and Gynecology, epidural anaesthesia is the most effective method of pain relief and the first analgesic of choice for women during vaginal delivery (American College of Obstetricians and Gynecologists Committee on Obstetric Practice, 2006). Women who receive epidural anaesthesia feel less pain and have more satisfaction than women who do not receive this method (de Orange et al., 2012). Although epidural anaesthesia significantly reduces labour pain, it is expected to slow the progress of labour and increase the rate of vacuum (Obstetricians & Practice, 2006). Women under epidural analgesia are less mobile during labour, with mobile women experiencing a shorter labour length than women in recumbent positions. Mobility and upright position reduce the length of labour without negative maternal and neonatal outcomes (Lawrence et al., 2013). Indeed, positioning techniques reduce the risk of complications in women under epidural analgesia (Clutter & Grant, 2015).
The prolonged first stage of labour is associated with maternal complications including chorioamnionitis and postpartum haemorrhage (Cheng et al., 2010) as well as neonatal complications including NICU admission (Cheng et al., 2009). Thus, effective interventions can safely reduce the length of labour without any maternal and neonatal complications. The active control of maternal position during labour helps the mother to cope with labour pain and supports progress labour (Zwelling, 2010).
The peanut ball is a proper alternative for the traditional birth ball. The former is a curved and an egg‐shaped ball located between the knees at either the lateral or supine position, which helps widen pelvic opening (Roth et al., 2016). These positions form a C‐shape curve in the spine. Theoretically, it imitates the position of the birth ball with the same benefits of rotating and moving down the baby. The difference is that use of peanut balls is comfortable without constant support to hold the right position during labour in women under epidural analgesia (Mercier & Kwan, 2018).
Regarding the benefits, the peanut ball is an inexpensive and non‐invasive method made of durable plastic, which allows sterilization and repeated use. It is most likely a cost‐effective method in women who receive epidural anaesthesia. The peanut ball shortens the labour length and reduces the rate of caesarean delivery (Tussey & Botsios, 2011; Tussey et al., 2015), which no side effects have been reported (Zhang et al., 2010).
The identification of evidence‐based techniques can contribute to reducing the length of labour and increasing vaginal delivery. Maternal and neonatal health depends on uncomplicated vaginal delivery. Thus, peanut ball can be used to shorten the labour length and increase vaginal delivery in case the positive effects of this method are confirmed.
2. OBJECTIVES
This systematic review and meta‐analysis aimed to evaluate and collate the findings of already published articles examining the effectiveness of peanut ball during labour on the length of labour stages and rate of caesarean section. The primary outcomes included the length of first stage of labour and the rate of caesarean section while the secondary outcome was the length of the second stage of labour.
3. METHODS
3.1. Inclusion and exclusion criteria
All published individual randomized controlled clinical trials (RCTs) and quasi‐RCTs in English and Persian databases were reviewed. All studies that had compared the effectiveness of peanut ball with the routine or non‐pharmacological care on the length of labour and rate of caesarean section in pregnant women with or without epidural analgesia were included. Letters to the editor, qualitative, and observational studies and those papers on women with multiple pregnancies were excluded from the study.
3.2. Data source and identification of studies
We searched multiple databases including English databases (Cochrane Library, Medline, Web of Science, Embase, Scopus, ProQuest) and Persian databases (Magiran, SID, and Barakat) using the related keywords from the inception of the databases until December 2020. For example, the search strategy for Scopus was as follows: ((ALL (pregnan* OR labor* OR labour* OR midwi* OR cesarean OR deliver*)) OR (ALL (patient W/5 position*))) AND ((TITLE‐ABS‐KEY (peanut AND ball*)) OR (ALL (peanut W/6 ball*))). Also, the search strategy for PubMed was as follows: (Peanut ball*) AND ((((((("Pregnancy"[Mesh]) OR "Labor, Obstetric"[Mesh]) OR ("Patient Positioning/instrumentation"[Mesh] OR "Patient Positioning/methods"[Mesh])) OR "Midwifery/instrumentation"[Mesh]) OR "Cesarean Section"[Mesh]) OR "Delivery, Obstetric"[Mesh]) OR (((((((pregnan*) OR (labor*)) OR (labour*)) OR (Patient Position*)) OR (Midwi*)) OR (Cesarean)) OR (deliver*))). The references of included studies were also searched to find further articles.
3.3. Data extraction
Two authors (PA; RD) checked the titles and abstracts of the studies independently to evaluate the eligibility criteria. In case of insufficient information in the titles and abstracts of studies, the full text was reviewed to decide whether the paper was related to the study. If the two authors disagreed on an article, they discussed the issue. If they did not reach a consensus, a third person (MM) was consulted to decide on the matter. The study design, research setting, number of participants in study groups, intervention details, comparison group and results were independently extracted by the authors (Table 1).
TABLE 1.
Characteristics of included studies
| Study (Year) | Country | Study design | Final sample size | Intervention details | Comparison group | Results |
|---|---|---|---|---|---|---|
| Payton, 2015 | Louisville, Kentucky (s a state located in the east south‐central region of the United States) | Quasi‐RCT |
I:200 C:200 |
Use of the Peanut Ball | Not Use of the Peanut Ball | The duration of the second stage of labour was significantly longer in the intervention group (75.63 min) when compared with the control group (57.84 min). |
| Mercier & Kwan, 2018 | Philadelphia USA | RCT |
I:43 C:43 |
Use of the Peanut Ball | Not Use of the Peanut Ball | “There was no statistically significant difference in rates of cervical dilation (0.98 cm/hr vs. 0.79 cm/hr, (p =.27) or length of labour (315 min vs. 387 min, (p =.14) between the groups. There was no difference in the rates of caesarean delivery (33% vs. 35%, p =.8) or occiput posterior presentation. (28% vs. 9%, p =.09)” |
| Tussey et al., 2015 | South western United States | RCT |
I:107 C:94 |
Use of the Peanut Ball | Not Use of the Peanut Ball | Women who used the peanut ball (n = 107) versus those who did not (n = 91) demonstrated shorter first stage of labour by 29 min (p =.053) and second‐stage labour by 11 min (p <.001). The intervention was associated with a significantly lower incidence of caesarean surgery (OR = 0.41, p =.04) |
| Roth et al., 2016 | California | RCT |
I:78 C:71 |
Use of the Peanut Ball | Not Use of the Peanut Ball | In women having use of a peanut ball reduced first stage of labour duration for primiparous patients significantly more than multiparous patients, p =.018. There was no significant difference in the reduction of length of first stage labour for multiparous women, p =.057 with the use of the peanut ball. |
| D'Angelo, 2015 | Winston‐Salem, North Carolina, United States | RCT |
I:39 C:42 |
Use of the Peanut Ball | Not Use of the Peanut Ball | The duration of first stage of labour was longer in the control group (441 min) when compared with the peanut ball group (387 min). The incidence of caesarean surgery was equal in both groups. |
| Evans, 2014 | Cincinnati, Ohio, United States | RCT |
I: 91 C: 100 |
Use of the Peanut Ball | Receiving standard care for positioning during labour using pillows and wedge | The duration of first stage of labour was longer in the control group (322.7 min) when compared with the peanut ball group (331.3 min). The incidence of caesarean delivery was higher in the control group than the intervention group. |
Abbreviations: C, Control; I, Intervention; RCT, Randomized Controlled Trial.
3.4. Assessment of risk of bias in included studies
The two authors (PA; RD) independently assessed the risk of bias in all the studies using the criteria listed in the Cochrane Handbook. The risk of bias per item was categorized as low risk, high risk and unclear. If the authors disagreed on an issue, they discussed it. If their ideas did not converge, they consulted a third person (MM) to decide on the matter.
3.5. Statistical method
The collected data were analysed using RevMan‐ software version 5.3 and STATA version 14.2 (Stata crop, College Station, TX, USA). They were categorized into three categories of the rate of caesarean section as well as the length of the first and second stages of labour. The rate of caesarean section was reported as dichotomous in all collected studies. The average length of the first and second stages of labour was reported as continuous. The length of the first phase of labour was reported in terms of minute based on mean ± standard deviation by groups in all studies except one (Tarsilla, 2016). The length of the second stage of delivery was reported as minute by groups in two studies (Mercier & Kwan, 2018; Tussey et al., 2015). Accordingly, the meta‐analysis results for caesarean section were reported as risk ratio (RR) and 95% confidence interval, while meta‐analysis results for the first and second stages of labour were reported as mean difference and 95% confidence interval. Heterogeneity was assessed using I 2, T 2 and χ 2. The Grades of Recommendation, Assessment, Development and Evaluation Working Group (GRADE) approach was used to assess the certainty of evidence. The GRADE approach recommended by Cochran to examine the quality of evidence (Langendam et al., 2013; Tarsilla, 2016) (Table 2). Also, sensitivity analysis was conducted by excluding the Payton's study (2015) due to high risk of selection bias. Since the number of studies in the meta‐analysis did not exceed 10, graphical or statistical methods were not used to assess publication bias (Tarsilla, 2016).
TABLE 2.
Use of the peanut ball versus no use of the peanut ball
| No. of studies | Design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Use of the peanut ball | Not using the peanut ball | Pooled effect relative (95% CI) | Final judgement |
|---|---|---|---|---|---|---|---|---|---|---|
| Caesarean section delivery | ||||||||||
| 5 | Randomized Controlled Trials (RCTs) | No serious | No seriousa | No serious indirectness | Serious imprecisionb | No serious | 64/322 | 81/323 | 0.82 (0.62, 1.08) |
⨁⨁⨁O Moderate |
| First stage of labour | ||||||||||
| 6 | 5 RCTs and 1 quasi‐RCT | No serious | Very serious inconsistency | No serious indirectness | Very serious imprecisionb | No serious | 372.1/507 | 355.6/489 | −15.64 (−64.91, 33.62) |
⨁OOO Very low |
I2 is higher than 40%.
Not met optimal information size/CI is very wide.
4. RESULTS
4.1. Selection and characteristics of included studies
In total, 89 articles were found through the databases. Of these, 48 articles were eliminated for duplication. Forty‐one articles with title, abstract or full‐text review were screened. Two studies were selected from the website clinicaltrials.gov since they had been completed, and the results were available (D'Angelo, 2015; Evans, 2014). Nine articles were found through searching for references of the papers. From them, one paper was chosen. Finally, six articles were included in the meta‐analysis. One article (Evans, 2014) was not available through the author was contacted (Figure 1).
FIGURE 1.
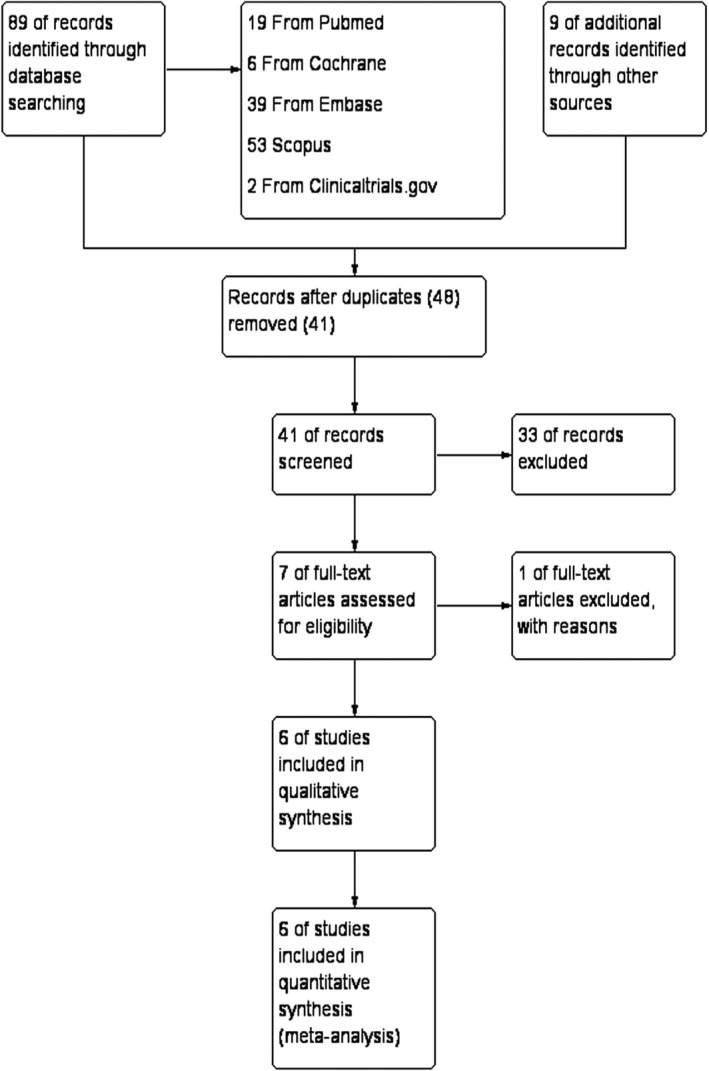
Study flow diagram
Six trials were carried out in parallel. The participants were divided into two groups (use of peanut ball and routine care without its usage). The sample size varied from 86 in Mercier et al.’s study (Mercier & Kwan, 2018) to 400 in Payton's study (2015). The participants consisted of nulliparous and multiparous women in labour under epidural analgesia. The intervention was the use of a peanut ball in women who received epidural anaesthesia. The control group received routine care without the peanut ball. In all studies except one (Hickey & Savage, 2019), the length of the first phase of labour is expressed in minutes based on the mean (standard deviation) by groups and in two studies (Mercier & Kwan, 2018; Tussey et al., 2015) The length of the first and second stages of labour was reported in minutes by groups. All included studies reported frequent caesarean sections.
4.2. Risk of bias of included studies
The bias about different areas was found as follows: random sequence generation was low risk in five studies (D'Angelo, 2015; Evans, 2014; Roth et al., 2016; Tussey et al., 2015; Mercier, & Kwan, 2018, 2015), and high risk in one study (Payton, 2015); allocation concealment was high risk in one study (Payton, 2015), unclear in two studies (D'Angelo, 2015; Evans, 2014) and low risk in three studies (Mercier & Kwan, 2018; Roth et al., 2016; Tussey et al., 2015); blinding participants and staff was high risk in all studies (Evans, 2014; Roth et al., 2016; Tussey et al., 2015; Mercier, & Kwan, 2018, 2015; Payton, 2015, 2015; D'Angelo, 2015, 2015); blinding assessor of outcome was high risk in all studies (Evans, 2014; Roth et al., 2016; Tussey et al., 2015; Mercier, & Kwan, 2018, 2015; & Payton, 2015, 2015; & D'Angelo, 2015, 2015); incomplete outcome data were low risk in five studies (D'Angelo, 2015; Evans, 2014; Mercier & Kwan, 2018; Payton, 2015; Tussey et al., 2015) and high risk in one study (Roth et al., 2016); and selective reporting was low risk in four studies (Mercier & Kwan, 2018; Payton, 2015; Roth et al., 2016; Tussey et al., 2015) and unclear in two studies (D'Angelo, 2015; Evans, 2014) (Figures 2 and 3). There is no published article for two studies (D'Angelo, 2015; Evans, 2014), and judgements about the risk of bias for these studies were made based on Clinicaltrials.gov.
FIGURE 2.
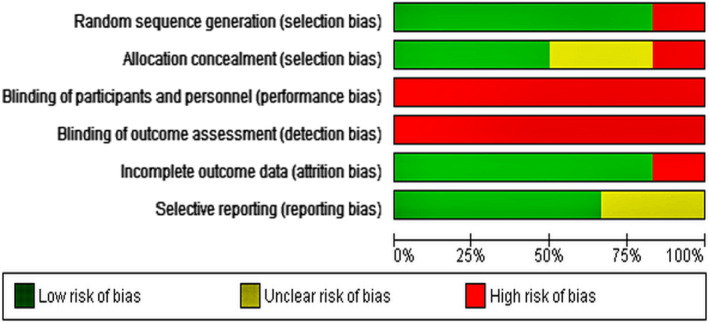
Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies
FIGURE 3.
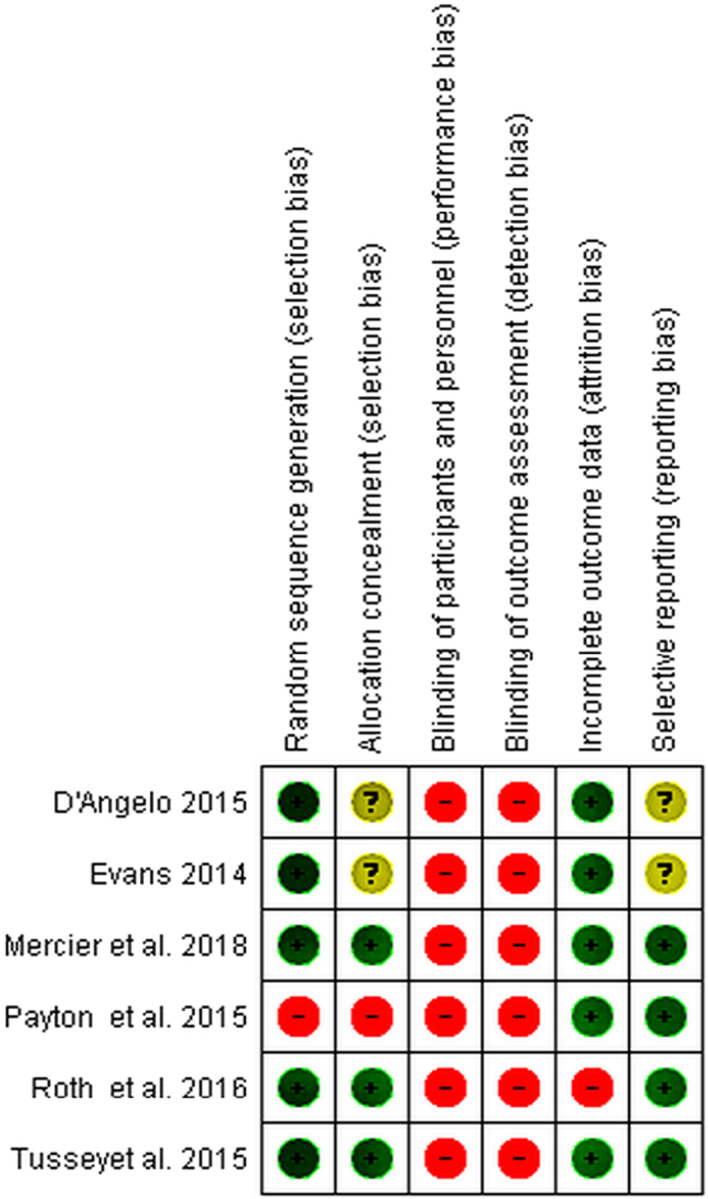
Risk of bias summary: review authors’ judgements about each risk of bias item for each included study
4.3. Rate of caesarean section
The overall result of meta‐analysis on 645 participants showed that although the rate of caesarean section in the peanut ball group was 0.82 times that of the control group, no statistically significant difference was found between them (RR = 0.82; 95% CI: 0.62 to 1.08; p =.15). There was a low heterogeneity across the studies (I 2 = 14%; Chi2 = 4.64; p =.33) (Figure 4).
FIGURE 4.
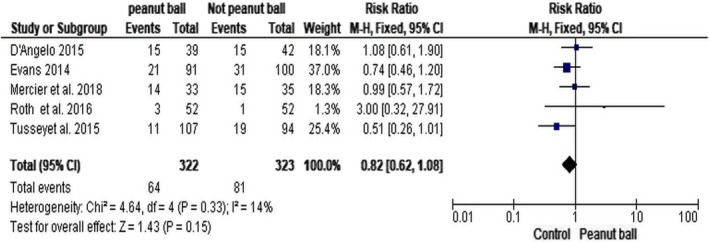
Peanut ball group versus control group; Outcome: Caesarean section delivery
4.4. The length of the first stage of labour
The overall result of meta‐analysis on 996 participants revealed that although the use of peanut balls reduced the length of the first stage of labour, no statistically significant difference was found between the intervention and control groups (MD = −15.64; 95% CI: −64.91 to 33.62; p =.53). Because of the high heterogeneity (I 2 = 71%; Tau2 = 2,521.14; Chi2 = 17.01; p =.004), random effects was used instead of fixed effects (Figure 5). Based on the results of ssensitivity analysis by excluding the Payton's study (2015), no statistically significant difference was also found between the intervention and control groups (MD = −30.42; 95% CI: −86.56 to 25.72; p =.29).
FIGURE 5.
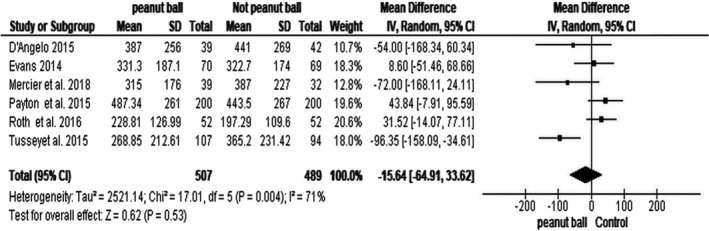
Peanut ball group versus control group; Outcome: First Stage of Labour
4.5. The length of the second stage of labour
In two of the included studies (Payton, 2015; Tussey et al., 2015), the length of the second stage was examined. In the Payton's study (2015), the length of the second stage was longer in the peanut ball group than in the control group; however, in the Tussey et al.’s study (2015), the length of the second stage of labour was shorter in the peanut ball group than in the control group.
5. DISCUSSION
This was the first meta‐analysis on the effectiveness of peanut ball on the rate of caesarean section and length of the first and second stages of labour in women under epidural analgesia. The results revealed that the rate of caesarean section in the peanut ball group was lower than in the control group, but the difference was not statistically significant. The difference in the length of stages of labour was not significant between the peanut ball group and the control group.
Since the primary cause of the caesarean section is its repetition (Spong et al., 2012), maternal morbidity, placental abnormalities and the bleeding increase as the rate of caesarean delivery rises (Marshall et al., 2011). A woman experiencing a caesarean section in the first delivery would be more likely (>90%) to undergo caesarean surgery in the second delivery (Kacica et al., 2017). Women undergoing caesarean section are at the risk of delayed skin‐to‐skin care and lactogenesis as well as an increase in the use of formula milk. Caesarean section is also associated with several adverse outcomes including abdominal adhesions, chronic pelvic pain, placental implantation disorders, surgical injuries and placental abruption in subsequent pregnancies (Marshall et al., 2011). Since vaginal delivery is safer and has fewer side effects than caesarean delivery, it is essential to give some recommendations to mothers to reduce the rate of caesarean section in the first delivery (Caughey et al., 2014).
The peanut ball is an inexpensive and non‐invasive intervention made of durable plastic which allows repeated use and sterilization. It shortens the length of labour and reduces the rate of caesarean section in women who receive epidural anaesthesia (Tussey et al., 2015). The use of these balls can also improve maternal and neonatal outcomes (Clutter & Grant, 2015). Epidural analgesia results in pelvic floor relaxation which supports rotation of the foetal head and mitigates the desire to push due to a diminution of the bearing down reflex and reduced uterine activity (Mayberry et al., 1999). One study reported that epidural analgesia was associated with an increased rate of occiput posterior and high‐risk delivery (Lieberman & O'Donoghue, 2002). Tussey et al. reported shortened first and second stages of labour and a significant decline in the rate of caesarean section in the peanut ball group. In their study, pharmacological interventions (labour induction and assisted delivery using forceps and vacuum) were less common in the peanut ball group but the difference was not statistically significant (Tussey et al., 2015).
The results of a qualitative study recommended the use of peanut balls. In that study, 118 women were satisfied with peanut balls and reported a positive experience of childbirth including comfort, facilitated progress of labour and proper labour positioning. Psychologically, three‐quarters (71%) of the women had used peanut balls and experienced favourable childbirth and recommended peanut ball. This positive experience may also have other psychological benefits both during and after the delivery (Tussey et al., 2015). Hospitals can use these balls to reduce the costs of prolonged labour. However, further studies are required to recommend these balls in clinical practice.
Although the obstetric complications or epidural analgesia can influence the rate of caesarean section and length of labour stages, in all included studies, low‐risk women without obstetric complications had been assessed where epidural analgesia had also been used in all included studies.
5.1. Limitation
Studies on the effectiveness of the peanut ball on maternal outcomes were limited. Nevertheless, one study was ongoing and in the sampling phase. Heterogeneity was high in two of the meta‐analyses. The certainty of evidence was very poor according to the GRADE guidelines. Thus, the effectiveness of the interventions and the results of the present study should be reported with caution.
6. CONCLUSIONS
The results of the meta‐analysis suggested that the use of peanut ball in women under labour had no statistically significant effect on the rate of caesarean section or the length of the first and second stages of labour. Further clinical trials with a stronger study are required.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
AUTHOR CONTRIBUTIONS
MM, PA, SMAC and RD: Study design. PA and RD: Literature research. MM, SMAC and PA: Data analysis. MM, PA, SMAC and RD: Writing the manuscript. All authors were responsible for the manuscript drafting and have read and approved the final version.
ETHICAL APPROVAL
Not applicable.
PATIENT CONSENT
Not applicable.
ACKNOWLEDGEMENTS
No acknowledgements.
Ahmadpour P, Mohammad‐Alizadeh‐Charandabi S, Doosti R, Mirghafourvand M. Use of the peanut ball during labour: A systematic review and meta‐analysis. Nurs Open. 2021;8:2345–2353. 10.1002/nop2.844
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- American College of Obstetricians and Gynecologists Committee on Obstetric Practice (2006). ACOG committee opinion no. 339: analgesia & cesarean delivery rates. Obstet Gynecol, 107, 1487–1488. 10.1097/00006250-200606000-00060 [DOI] [PubMed] [Google Scholar]
- Brown, S. T., Douglas, C., & Flood, L. P. (2001). Women's evaluation of intrapartum nonpharmacological pain relief methods used during labor. The Journal of Perinatal Education, 10, 1. 10.1624/105812401X88273 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caughey, A. B., Cahill, A. G., Guise, J. M., & Rouse, D. J. (2014). American College of Obstetricians and Gynecologists. Safe prevention of the primary cesarean delivery. American Journal of Obstetrics and Gynecology, 210(3), 179–193. [DOI] [PubMed] [Google Scholar]
- Chao, A. S., Chao, A., Wang, T. H., Chang, Y. C., Peng, H. H., Chang, S. D., Chao, A., Chang, C. J., Lai, C. H., & Wong, A. M. (2007). Pain relief by applying transcutaneous electrical nerve stimulation. (TENS). On acupuncture points during the first stage of labor: A randomized double‐blind placebo‐controlled trial. Pain, 127, 214–220. 10.1016/j.pain.2006.08.016 [DOI] [PubMed] [Google Scholar]
- Cheng, Y. W., Delaney, S. S., Hopkins, L. M., & Caughey, A. B. (2009). The association between the length of first stage of labor, mode of delivery, and perinatal outcomes in women undergoing induction of labor. American Journal of Obstetrics & Gynecology, 201, 477. e1–477. e7. 10.1016/j.ajog.2009.05.024 [DOI] [PubMed] [Google Scholar]
- Cheng, Y. W., Shaffer, B. L., Bryant, A. S., & Caughey, A. B. (2010). Length of the first stage of labor and associated perinatal outcomes in nulliparous women. Obstetrics & Gynecology, 116, 1127–1135. 10.1097/AOG.0b013e3181f5eaf0 [DOI] [PubMed] [Google Scholar]
- Clutter, L. B., & Grant, C. (2015). Peanut Balls, improving options for women laboring with an epidural. Australian Midwifery News, 15, 36. [Google Scholar]
- D'Angelo, R. (2015). Do peanut shaped birthing balls reduce the length of labor in patients with epidural analgesia. Retrieved from https://clinicaltrials.gov/ct2/show/NCT02539563 [Google Scholar]
- de Orange, F. A., Passini‐Jr, R., Melo, A. S., Katz, L., Coutinho, I. C., & Amorim, M. M. (2012). Combined spinal‐epidural anesthesia and non‐pharmacological methods of pain relief during normal childbirth and maternal satisfaction: A randomized clinical trial. Revista da Associação Médica Brasileira, 58, 112–117. [PubMed] [Google Scholar]
- Evans, S. (2014). Use of peanut labor ball following epidural anesthesia. (2017). Retrieved from https://clinicaltrials.gov/ct2/show/NCT02190591 [Google Scholar]
- Favilli, A., Laganà, A. S., Indraccolo, U., Righi, A., Triolo, O., D’Apolito, M., & Gerli, S. (2018). What women want? Results from a prospective multicenter study on women’s preference about pain management during labour. European Journal of Obstetrics & Gynecology and Reproductive Biology, 95, 589–595. 10.1016/j.ejogrb.2018.06.038 [DOI] [PubMed] [Google Scholar]
- Hickey, L., & Savage, J. (2019). Effect of peanut ball and position changes in women laboring with an epidural. Nursing for Women's Health, 23, 245–252. 10.1016/j.nwh.2019.04.004 [DOI] [PubMed] [Google Scholar]
- Hodnett, E. D. (2002). Pain and women's satisfaction with the experience of childbirth: A systematic review. American Journal of Obstetrics and Gynecology, 186, S160–S172. 10.1016/S0002-9378(02).70189-0 [DOI] [PubMed] [Google Scholar]
- Kacica, M. A., Glantz, J. C., Xiong, K., Shields, E. P., & Cherouny, P. H. (2017). A statewide quality improvement initiative to reduce non‐medically indicated scheduled deliveries. Maternal and Child Health Journal, 21, 932–941. 10.1007/s10995-016-2196-5 [DOI] [PubMed] [Google Scholar]
- Langendam, M. W., Akl, E. A., Dahm, P., Glasziou, P., Guyatt, G., & Schünemann, H. J. (2013). Assessing and presenting summaries of evidence in Cochrane Reviews. Systematic Reviews, 2(1), 1–9. 10.1186/2046-4053-2-81 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lawrence, A., Lewis, L., Hofmeyr, G. J., Dowswell, T., & Styles, C. (2013). Maternal positions and mobility during first stage labour. Cochrane Database of Systematic Reviews, (8). 10.1590/S1516-31802011000500015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, H., & Ernst, E. (2004). Acupuncture for labor pain management: A systematic review. American Journal of Obstetrics and Gynecology, 191, 1573–1579. 10.1016/j.ajog.2004.05.027 [DOI] [PubMed] [Google Scholar]
- Lieberman, E., & O'Donoghue, C. (2002). Unintended effects of epidural analgesia during labor: A systematic review. American Journal of Obstetrics and Gynecology, 186, S31–S68. 10.1067/mob.2002.122522 [DOI] [PubMed] [Google Scholar]
- Marshall, N. E., Fu, R., & Guise, J. M. (2011). Impact of multiple cesarean deliveries on maternal morbidity: A systematic review. American Journal of Obstetrics and Gynecology, 205, 262. e1–262. e8. 10.1016/j.ajog.2011.06.035 [DOI] [PubMed] [Google Scholar]
- Mayberry, L. J., Wood, S. H., Strange, L. B., Flee, L., Heisler, D. R., & Neilsen‐Smith, K. (1999). Managing second‐stage labour. Nursing for Women's Health, 28, 152–159. 10.1111/j.1552-6356.1999.tb01146.x [DOI] [PubMed] [Google Scholar]
- Mercier, R. J., & Kwan, M. (2018). Impact of peanut ball device on the duration of active labor: A randomized control trial. American Journal of Perinatology, 35, 1006–1011. 10.1055/s-0038-1636531 [DOI] [PubMed] [Google Scholar]
- Osterman, M. J., & Martin, J. A. (2011). Epidural and spinal anesthesia use during labor: 27‐state reporting area, 2008. National Vital Statistics Reports, 59, 1–13, 16. [PubMed] [Google Scholar]
- Payton, C. L. (2015). Use of the peanut ball to decrease first and second stages of labor. Graduate Theses, Dissertations, and Capstones. Paper 14. [Google Scholar]
- Qu, F., & Zhou, J. (2007). Electro‐acupuncture in relieving labor pain. Evidence‐Based Complementary and Alternative Medicine, 4, 125–130. 10.1093/ecam/nel053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roth, C., Dent, S. A., Parfitt, S. E., Hering, S. L., & Bay, R. C. (2016). Randomized controlled trial of use of the peanut ball during labor. MCN: The American Journal of Maternal/Child Nursing, 41, 140–146. 10.1097/NMC.0000000000000232 [DOI] [PubMed] [Google Scholar]
- Simkin, P., & Bolding, A. (2004). Update on nonpharmacologic approaches to relieve labor pain and prevent suffering. Journal of Midwifery and Women's Health, 49, 489–504. 10.1016/j.jmwh.2004.07.007 [DOI] [PubMed] [Google Scholar]
- Spong, C. Y., Berghella, V., Wenstrom, K. D., Mercer, B. M., & Saade, G. R. (2012). Preventing the first cesarean delivery: Summary of a joint Eunice Kennedy Shriver national institute of child health and human development, society for maternal‐fetal medicine, and American College of Obstetricians and Gynecologists workshop. Obstetrics and Gynecology, 120, 1181. 10.1097/AOG.0b013e3182704880 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tarsilla, M. (2016). Cochrane handbook for systematic reviews of interventions. Journal of Multidisciplinary. Evaluation, 6(14), 142–148. [Google Scholar]
- Tournaire, M., & Theau‐Yonneau, A. (2007). Complementary and alternative approaches to pain relief during labor. Evidence‐based Complementary and Alternative Medicine, 4, 409–417. 10.1093/ecam/nem012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tussey, C., & Botsios, E. (2011). Use of a labor ball to decrease the length of labor in patients who receive an epidural. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 40, S105–S106. 10.1111/j.1552-6909.2011.01243_25.x [DOI] [Google Scholar]
- Tussey, C. M., Botsios, E., Gerkin, R. D., Kelly, L. A., Gamez, J., & Mensik, J. (2015). Reducing length of labor and cesarean surgery rate using a peanut ball for women laboring with an epidural. The Journal of Perinatal Education, 24, 16. 10.1891/1058-1243.24.1.16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, J., Landy, H. J., Ware Branch, D., Burkman, R., Haberman, S., Gregory, K. D., Hatjis, C. G., Ramirez, M. M., Bailit, J. L., Gonzalez‐Quintero, V. H., Hibbard, J. U., Hoffman, M. K., Kominiarek, M., Learman, L. A., Van Veldhuisen, P., Troendle, J., & Reddy, U. M. (2010). Contemporary patterns of spontaneous labor with normal neonatal outcomes. Obstetricsand Gynecology, 116, 1281. 10.1097/AOG.0b013e3181fdef6e [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zwelling, E. (2010). Overcoming the challenges: Maternal movement and positioning to facilitate labor progress. The American Journal of Maternal/Child Nursing, 35, 72–78. 10.1097/NMC.0b013e3181caeab3 [DOI] [PubMed] [Google Scholar]
- Zwelling, E., Johnson, K., & Allen, J. (2006). How to implement complementary therapies for laboring women. The American Journal of Maternal/Child Nursing, 31, 364–370. 10.1097/00005721-200611000-00006 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.