

Abstract
This paper surveys the data‐driven dose prediction methods investigated for knowledge‐based planning (KBP) in the last decade. These methods were classified into two major categories—traditional KBP methods and deep‐learning (DL) methods—according to their techniques of utilizing previous knowledge. Traditional KBP methods include studies that require geometric or anatomical features to either find the best‐matched case(s) from a repository of prior treatment plans or to build dose prediction models. DL methods include studies that train neural networks to make dose predictions. A comprehensive review of each category is presented, highlighting key features, methods, and their advancements over the years. We separated the cited works according to the framework and cancer site in each category. Finally, we briefly discuss the performance of both traditional KBP methods and DL methods, then discuss future trends of both data‐driven KBP methods to dose prediction.
Keywords: data‐driven methods, deep learning, knowledge‐based planning, machine learning, radiation dose prediction methods, radiotherapy treatment planning
1. INTRODUCTION
Cancer is the second‐leading cause of death in North America with the most common types being the cancer of lung, breast, and prostate.1 Radiation therapy (RT), chemotherapy, surgery or their combination are used to control the disease. Approximately 50% of all cancer patients undergo RT during the course of their illness,2 which makes RT a crucial component of cancer treatments. Technological innovations have driven the transition from conformal RT to intensity‐modulated radiation therapy (IMRT) resulting in significant improvements in the twofold dosimetric goal of preferentially sparing critical organs‐at‐risk (OARs) while improving high dose conformity to the target. Furthermore, algorithmic advancements have also played major roles in enhancing the efficiency of RT treatments. These include the transition from forward treatment planning to inverse treatment planning approaches and extension of static field IMRT to volumetric‐modulated arc therapy (VMAT). However, despite the use of complex inverse optimization algorithms, an inverse planning approach typically demands a large amount of manual effort and considerable skills to generate a high‐quality treatment plan with the desired dose distribution. This process often spans several days between patient simulation and when RT begins.
To improve the treatment planning efficiency, data‐driven treatment planning approaches have been investigated that use knowledge from prior cases to predict the outcome of a new case. For example, this concept was utilized by researchers over a decade ago in the form of knowledge‐based planning (KBP) to predict dose in radiotherapy treatment planning.3 In this review, we group data‐driven KBP methods into two major categories: I) Traditional KBP methods II) Deep learning (DL)‐based KBP methods. Traditional KBP includes methods that utilize various anatomical and geometrical features (distance to target structures, volumes of target, and OAR structures, etc.) to build a mathematical or statistical model that is then used to predict various dosimetry features (i.e., dose–volume metrics, dose–volume histogram (DVH), spatial dose distribution, etc.) for a new case.4 Traditional KBP methods have been widely investigated in the last decade and have also been clinically implemented. The commercial software RapidPlanTM is one example of the KBP module based on a traditional method, which was released in 2014 by Varian Medical Systems (Varian Medical Systems). The traditional KBP methods include atlas‐based, statistical modeling, and machine learning (ML) methods. In general, traditional KBP methods utilize geometric features (i.e., OAR distance to the planning target volume (PTV) and OAR overlap volume histogram (OVH)) either to find the best‐matched prior case(s) from a repository or to build dose prediction models (i.e., ML, statistical model). In this review, ML‐based methods are included in the traditional KBP category as ML follows a similar framework to traditional KBP methods in terms of inputs (handcrafted geometric and anatomical features) and outputs (DVH metrics).
Prior to the investigations of DL for the dose prediction task, DL had been extensively studied for various imaging tasks including image registration, segmentation, etc., in which DL methods have gained considerable momentum, outperforming many of the existing state‐of‐art techniques.5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21 The enhanced performance of DL in imaging and vision tasks can be attributed to the design of a convolutional neural network (CNN), a class of deep neural networks (DNN) with regularized multilayer perceptron.22 In the past few years, researchers have investigated various DL network architectures for KBP. As an example, U‐Net,23 originally designed for image segmentation, has recently been used to predict the radiation dose distribution without the need for the complex dose calculations routinely used for treatment planning.24, 25, 26, 27 In contrast to traditional KBP methods that use handcrafted features, DL methods can automatically learn image features that are tailored to the specific prediction task from the raw data (i.e., CT, contour, dose map, etc.) Therefore, a key difference between traditional and DL‐based KBP is the way in which previous knowledge is utilized.
KBP research is expanding exponentially, and while there are excellent review papers in publication, this current review is needed to address recent advancements in dose prediction methods. Previous review papers are limited to only traditional KBP methods,28, 29 multicriteria optimization methods,30 and multicriteria optimization as well as traditional KBP methods31 for automatic treatment planning. Another review provided a semi‐comprehensive review of 62 publications including both machine learning and DL‐based methods for automatic treatment planning; however, this study is not specific to the dose prediction task and also includes articles on other delivery parameters (i.e., beam orientation, arc lengths, etc.).32 In comparison to previous review papers, this work focuses solely on the dose prediction task and presents a comprehensive review by separating over 120 publications on data‐driven KBP methods published by August 2020 into two categories: the traditional KBP methods and the recently emerging DL‐based methods. For each category, we first present a review of key features and methods (i.e., OVH, distance to target histogram (DTH) in traditional KBP methods, and different neural networks in DL‐based methods). Subsequently, we present the literature on outcomes of KBP methods according to the influence of various clinically applicable parameters (i.e., outliers, data inconsistency, sample size, treatment planning efficiency and site, multi‐modality, and multi‐institutional investigations). Finally, we discuss the advantages and challenges of each KBP method, followed by an assessment of potential future trends in data‐driven dose prediction methods. Therefore, this current review differentiates itself from previous review papers by the large number of articles covered including more recent publications, the summary of key features, and methodological differences between the published methods, and the focus on the dose prediction task.
2. METHODS
2.1. Article search and selection
We queried papers from Elsevier Scopus®, Web of Science, PubMed, Google Scholar, and medical physics category of arXiv.org using logical statements that included the following keywords: knowledge‐based treatment planning, machine learning, deep learning, dose prediction, RapidPlan®, treatment planning automation, artificial neural network, convolutional neural network, and generative adversarial network. Only peer‐reviewed KBP research articles were included in this review. Each research article from the literature search was manually sorted based on the information presented in the abstract, which was followed by a further in‐depth review of the article. This review focuses on external beam therapies (e.g., IMRT, VMAT, Tomotherapy, Proton), while manuscripts on brachytherapy and patient‐specific quality assurance were excluded. Articles on dose prediction tasks were selected for this review. Dose prediction is a broad term that includes the prediction of the entire DVH curve, specific dose metrics (e.g., dose–volume value, mean, max dose), voxel dose, spatial dose distribution (either 2D or 3D), objective weights/constraints based on previous knowledge and the transfer of these metrics to a new case for planning.
3. RESULTS
Figure 1 shows the number of publications per year (Figure 1a) as well as cumulative publications (Figure 1b) for both traditional KBP and DL‐based dose predictions until August 2020. Between 2009 and 2014, there was a gradual increase in the number of publications (Figure 1b) in what appears to be the initial development stage of traditional KBP‐based methods. The cumulative publication curve (Figure 1b) demonstrates an increased rate in the number of traditional KBP‐based articles between 2015 and 2018. Between 2018 and 2020, most studies on traditional KBP methods have been based on a commercial KBP module rather than further development of earlier ML or statistical methods.33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45 This is certainly not because traditional KBP methods have been fully explored, but presumably due to the wider availability of a commercial KBP module in clinical practice and increased interest in exploring DL methods owing to their recent success in achieving state‐of‐the‐art performance in many medical applications. In recent years, a wide array of research on developing new prediction models has transitioned from traditional KBP methods to DL KBP methods.
FIGURE 1.
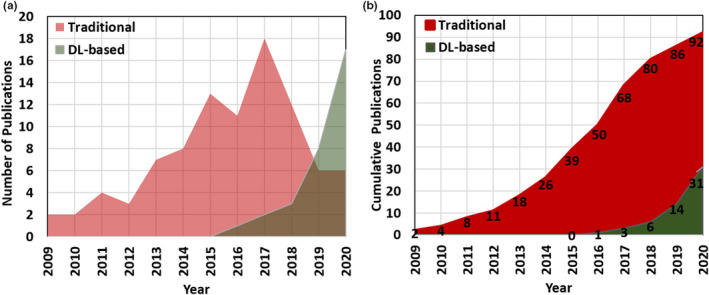
The number of dose prediction publications per year (a) and cumulative number of publications (b) on traditional and DL‐based KBP methods
In the past few years, the number of publications on DL‐based image processing has increased exponentially. More recently, researchers have applied DL methods to dose prediction tasks. In the last 4 years, the number of publications on DL‐based dose predictions has increased from 1 in 2016 to 17 as of August 2020 as shown in Figure 1a. This recent trend shows an increased rate of publications on DL‐based versus traditional KBP methods.
3.1. Knowledge‐based planning
This section includes a review of over 92 articles only on traditional KBP‐based dose prediction methods. We separate these articles based on three dose prediction metrics: I) prediction of the entire DVH (Table 1), II) prediction of one or more dose–volume metrics (Table 2), and III) the voxel‐based dose prediction (Table 3). The articles listed in Table 1 aim to predict the entire DVH for a new patient case and utilize the predicted DVHs to guide the treatment planning. Commercially available software (i.e., RapidPlanTM) estimates DVHs and generates optimization objectives for a new plan as shown in Table 1. Table 2 summarizes the articles that predict one or more dose metrics used to guide treatment planning for a new case. Table 3 lists the publications that predict the voxel‐level dose distributions to either assist in plan optimization or automatically generate a new plan for treatment delivery.
TABLE 1.
Traditional KBP studies aimed to predict dose–volume histograms (DVHs) for providing a starting point for the plan optimization process
| Ref. | Method | Approach/Model | Key features | Purpose |
|---|---|---|---|---|
| 46 | MB | Support Vector Regression | Organ volumes, shape and DTH | To model functional relationship between DVH and patient anatomical shape information. |
| 4 | MB | Fitting using least square min. | OAR distance to PTV | To translate key feature correlation to mathematical relationships between OAR geometry and expected dose. |
| 47 | MB | Stepwise multiple regression | DTH | To build feature models to identify the variation of anatomical features contributing to OAR dose sparing. |
| 48 | MB | Stepwise multiple regression | Target, OARs, overlap volumes and DTH | Extension of Yuan et al. for intra‐treatment‐modality model (IMRT – Tomotherapy) |
| 49 | MB |
Stepwise multiple regression |
Target, OARs, overlap volumes and DTH, fraction of OAR outside treatment field | To build two predictive models (single‐sparing and standard model) to characterize the dependence of parotid dose sparing on patient anatomical features in the summed (primary + boost) plan, rather than two completely separate models. |
| 50 | AB | Direct | Overlapping volume |
To select a reference plan from a library of clinically approved/delivered plans with similar medical conditions and geometry |
| 51 | AB | Direct | PTV shape, volume, three spherical coordinates of PTV with respect to OAR OVH | To develop a knowledge‐driven decision support system to assist clinicians to pick plan parameters and assess radiation dose distribution for a perspective patient |
| 52 | MB | Kernel Density Estimate | Distance to PTV |
To develop an automated treatment planning solution that iteratively
|
| 53 | MB | Ensemble | Anatomical features, DTH | To combine strengths of various linear regression models to build a more robust model |
| 54 | MB | K‐nearest neighbors | Generalized‐DTH | To characterize DVH variance in multiple target plans |
| 33, 34, 35, 36, 37, 38, 39, 40, 42, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78 |
RapidPlanTM Eclipse® treatment planning software: Algorithm is divided into two components: 1) Model configuration and 2) DVH estimation.
|
Abbreviations: AB, atlas‐based (Direct or Indirect method); DTH, distance‐to‐target histogram; MB, model‐based; OVH, overlap volume histogram.
TABLE 2.
Traditional KBP studies aimed to predict one or more dose metrics for providing a starting point for the plan optimization process
| Ref. | Method | Approach/Model | Key features | Purpose |
|---|---|---|---|---|
| 79 | MB | Support vector regression | OAR, DV constraint settings | To create an accurate IMRT plan surface as a decision support tool to aid treatment planners |
| 80 | AB | Direct | Clinical stage, and Gleason score | To update the weights of the difference clinical parameters for a new patient through a group‐based simulated annealing approach |
| 81 | AB | Direct | OVH | To use geometric and dosimetric information retrieved from a database of previous plans to predict clinically achievable dose–volume metric (A retrospective based on a method by 3) |
| 82 | AB | Direct | OVH | To implement the OVH‐based automated planning system to improve quality, efficiency, and consistency for head and neck cancer |
| 83 | AB | Direct | OVH | To predict dose to 35% of rectal volume as a treatment planning quality assurance for prostate cancer patients. |
| 84 | AB | Direct | OVH | To investigate if OVH‐driven IMRT database can guide and automate VMAT planning for head and neck cancer |
| 85 | MB | Linear Regression | OVH | To evaluate OVH metric for the prediction of rectal dose following hydrogel injection |
| 86 | MB | Stepwise multiple regression | OVH | To utilize patients’ anatomic and dosimetric features to predict the pareto front. |
| 87 | MB | Logistic Regression | Distance to the tangent field edge | To predict left anterior descending artery maximum dose. Model to guide the positioning of the tangent field to keep maximum dose <10 Gy |
| 88 | MB | Linear Regression | OAR volumes | To develop a model to predict attainable prescription dose for IMRT of entire hemithoracic pleura |
| 89 | MB | Curve Fitting | Rectum‐target overlap | To predict optimum average rectum dose |
| 90 | MB | Stepwise Regression | Target OAR overlap | To predict mean parotid dose |
| 91 | AB | Direct | OVH’, In field OAR volumes | The minimum DVH value at the percentage volume of the bladder and rectum was used |
Abbreviations: AB, atlas‐based (Direct or Indirect method); DTH, distance‐to‐target histogram; MB, model‐based; OVH, overlap volume histogram.
TABLE 3.
Traditional KBP studies aimed to predict voxel‐level doses for providing a starting point for the plan optimization process
| Ref. | Method | Approach/Model | Key features | Purpose |
|---|---|---|---|---|
| 92 | AB | Direct | BEV projections | To identify similar patient cases by matching 2D BEV projections of structures |
| 93 | AB | Direct | BEV projections | To adapt the best match plan parameters from one institute to optimize the query case of an outside institution |
| 94, 95 | MB | Multivariate analysis Slice weight function |
Distance‐to‐PTV, Slice level |
To determine the relationship between the position of voxels and corresponding doses to predict the sparing of OARs |
| 96 | MB | Active shape model, active optical flow model | PTV locations in relation to spinal cord |
To study the effect of PTV contours on dose distribution at the spinal cord.
|
| 97 | AB | Direct |
Target‐OAR overlap Shell creation surrounding the match target volume |
To adapt the matched case from the database for query case by deforming the match beam fluences, warping the matched primary/boost dose distribution, and distance scaling factor |
| 98 | AB | Direct | Target‐OAR overlap | To transfer the beam settings and multileaf collimator positions of the best match case to the new case |
| 99 | AB | Direct | The PTV and Seminal vesicles (SV) concaveness angle and % distance from SV to the PTV | To transfer treatment parameters of the atlas case to the new case |
| 100 | AB | Indirect | Multi‐scale image appearance features | To use contextual atlas regression forest (cARF) augmented with density estimation over the most informative features to learn an automatic atlas‐selection metric for dose prediction |
| 101 | AB | Indirect | Features based on the spatial dose distribution and features derived from DVHs |
To extend CRF by introducing the conditional random field model (cARF‐CRF) to transform the probabilistic dose distribution into a scalar dose distribution that adheres to desired DVHs. |
| 102 | AB | Indirect | Multi‐scale image appearance features | To converts a predicted per voxel dose distribution into a complete radiotherapy plan through a fully automated pipeline using cARF‐CRF. |
Abbreviations: AB, atlas‐based (Direct or Indirect method); DTH, distance‐to‐target histogram; MB, model‐based; OVH, overlap volume histogram.
Atlas‐based and model‐based methods are the two most common traditional KBP techniques for dose prediction (Tables 1, 2, 3). Briefly, in atlas‐based approaches, physical features (e.g., OVH, beam's eye view projections, tumor location) are first identified to determine the similarity between prior clinical plans and a new patient plan. This is followed by transfer of knowledge (i.e., dose constraints, DVH values, beam geometrical parameters, DVHs of best‐matched cases) to predict achievable DVHs of a new case or to provide a better starting point to a treatment planner for further trial‐and‐error optimization. Within atlas‐based methods, an indirect approach selects matching cases based on the dosimetric parameters predicted through models. In contrast, a direct approach compares the similarity between the old and new patient based on features of the plan (i.e., DVHs), CT images or beam's eye view (BEV) projections of structures, and adopts planning parameters of the best match matching cases. In model‐based approaches, statistical or ML models are trained using prior treatment plans. These methods require careful design and selection of handcrafted features such as PTV‐OAR overlap volume, OVH values, OAR distance‐to‐PTV to predict DVH, one or more dose–volume metric or voxel‐level dose distribution by different regression models as summarized in Tables 1, 2, 3.
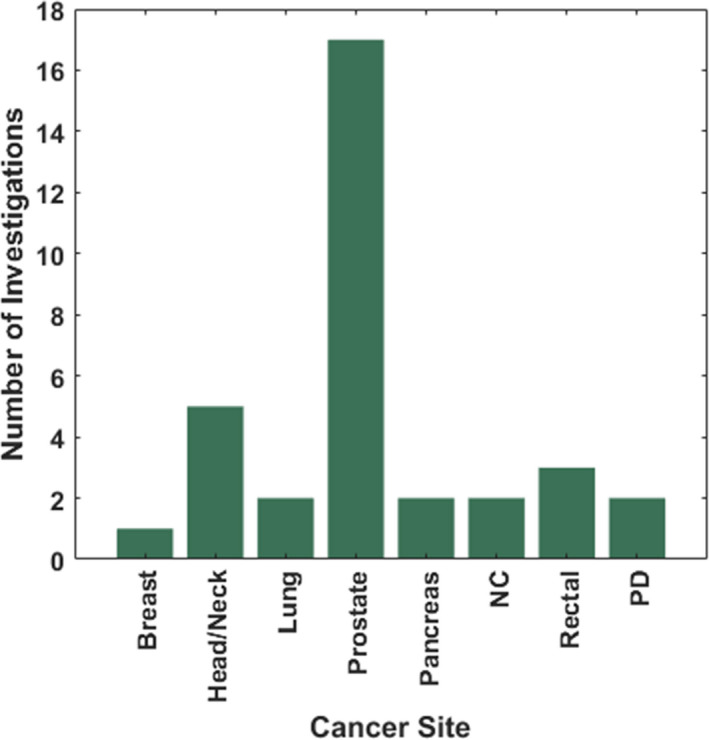
Figure 2 demonstrates the total number of investigations on traditional KBP methods for various treatment sites. Prostate, head and neck, and lung cancers were among the most frequently investigated disease sites, whereas very few studies investigated disease sites in the abdomen, brain, and or the more challenging hemi‐thoracic pleural anatomy.
FIGURE 2.
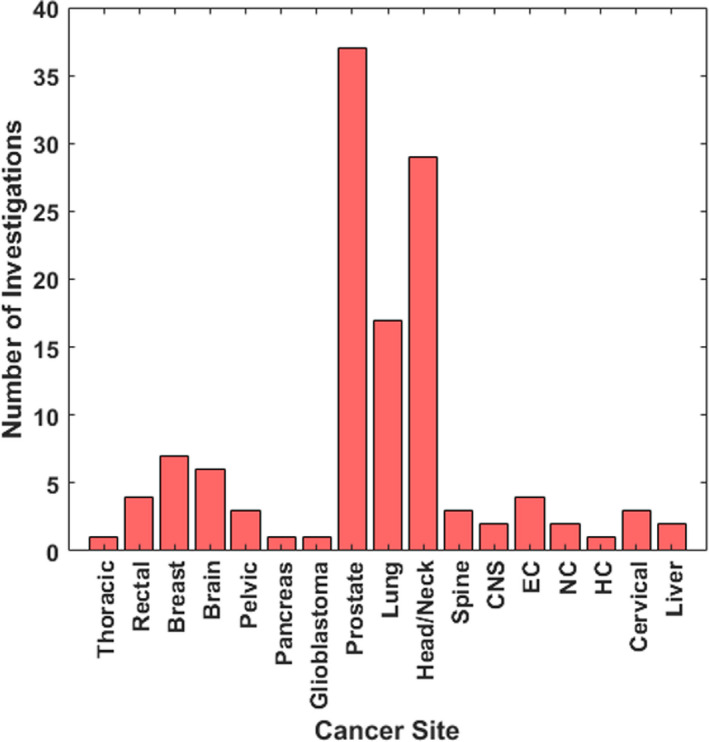
The total number of traditional KBP investigations on dose prediction for various cancer sites. EC, Esophageal cancer; NC, Nasopharyngeal carcinoma; HC, Hepatocellular Cancer
In Section 3.1.1, 3.2.3, we briefly discuss a key concept of traditional KBP methods. Since different geometric and anatomical features play a major role in traditional KBP‐based methods (Tables 1, 2, 3), we present a review of the most common features/metrics and their advancements over the years in Section 3.1.2, 3.2.3. In Section 3.1.3, 3.2.3, we present literature on the outcomes of KBP methods according to the influence of various clinically relevant parameters (i.e., outliers, data inconsistency, sample size, treatment planning efficiency and site, multi‐modality, and multi‐institutional reports).
3.1.1. Dimensionality reduction
The high dimensional input feature space can be redundant, irrelevant, and correlated, which may result in inefficient training, model overfitting, reduced accuracy, and reduced generalizability of the model. Therefore, it is important to utilize the most discriminative features, rather than including all possible features. To address this during the implementation of a KBP‐based dose prediction model, dimensionality reduction methods are often used in KBP studies to decrease the number of variables through feature extraction and feature selection process. Feature extraction begins with an initial set of variables followed by redefinition that makes them more informative. Principal component analysis (PCA) is a widely used technique for reduced‐order modeling. PCA determines the features that vary the most among the data for representation in a smaller number of dimensions.103 For example, in a binary classification problem, the goal is to classify an object , represented by P number of features in a P‐dimensional vectors. If P is very large, then some characteristics are likely more valuable than others for the purpose of classification. The goal of PCA is to reduce the dimensionality of the original correlated dataset into a smaller set of uncorrelated variables.103 The subsequent process of feature selection involves choosing features that are most important for the dose prediction task. In many traditional KBP studies,46, 47, 48, 49, 53, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 86, 104, 105, 106 PCA is commonly used in the process of feature selection.
3.1.2. Various features/metrics
A common theme in the majority of traditional KBP methods is that the geometric relationship of the target with respect to nearby critical structures correlates with achievable plan quality metrics. Various geometric features have been correlated with dose. Commonly reported geometric features include OVH, distance to target histograms (DTH), and OAR distance‐to‐PTV. As an example, the influence of parotid size and proximity to the PTV was first studied by Hunt et al. and found to be predictive of the achievable parotid sparing.107 In addition to 3D geometric features, traditional KBP methods have also incorporated plan features such as mutual information through the beam's eye view projections, and even the number, energy, and angle of the radiation beams (Tables 1, 2, 3). A list of the key features used in traditional KBP studies is tabulated in Tables 1, 2, 3 along with their corresponding references.
OVH‐based methods
The OVH is a feature common to both atlas‐based and model‐based approaches for dose prediction, as summarized in Tables 1 and 2. Wu et al. and Kazhdan et al. introduced the concept of the OVH as a one‐dimensional function measuring the proximity of an OAR to the target.3, 108 The OVH calculation involves the uniform expansion and contraction of the target volume. Target expansion occurs until an OAR is completely overlapped by the target, and contraction is repeated until there is no overlap between the target and the OAR.3 The resulting OVH describes the percentage of the OAR volume that overlaps with a uniformly expanded or contracted target. In general, OVH‐driven models assume that the dose to an OAR is inversely proportional to the distance from the target. Next, we survey how the OVH‐based methods have been evolved over the years to improve dose prediction accuracy.
Several studies have combined historical data with the OVH methods to predict an entire DVH (Table 1) or one or more clinically important dose metrics from a DVH (Table 2). Wu et al. applied the OVH to head/neck IMRT planning as a quality control tool to assist treatment planners with the plan evaluation task.3 This initial approach was further developed in another study that used the OVH to estimate achievable DVH objectives for head/neck plans.81 Using an OVH model 108 and PCA,46, 47 Wang et al. investigated the effect of interorgan dependency and the impact of data inconsistency on dose prediction for head/neck cancer. It was suggested that interorgan dependency be incorporated in the prediction models and that data inconsistency be avoided as much as possible to improve prediction accuracy.69 Larger dosimetric errors were found in the head/neck region (<4 Gy for 83% of cases) as compared to the prostate region (<2 Gy for 96% cases) presumably due to interorgan dependency.69 Moore et al. also used OVH information to predict OAR dose metrics for head/neck and prostate IMRT plans.109 Yuan et al. investigated the OVH to quantify the effects of various anatomical features on interpatient OAR dose sparing using IMRT and found that several important factors are attributable to OAR sparing: the mean distance between an OAR and PTV, overlap volume between an OAR and PTV, volume of an OAR outside the field, and the geometric relationship between multiple OARs.47 When multiple OARs are nearby a target, separate OAR‐specific prediction models were found to be more accurate at predicting voxel doses compared to using a single training model.110
The OVH has been investigated under a wide variety of clinical disease sites with highly variable PTV and OARs geometries. The OVH‐based model 81 has also been studied for pancreatic cancer in which the OARs are larger than the PTV, part of OARs can engulf the PTV, and highly deformable organs can vary the beam configurations among different patients.111 Petit et al. showed that the OVH‐based predicted doses were achieved within 1 and 2 Gy for more than 82% and 94% of the patients, respectively.111 Further, the OVH was investigated in prostate cancer patients who had a synthetic hydrogel spacer injected between the rectum and the prostate. The spacer displaces the rectum from the treatment field for preferential sparing, and correspondingly there is a global shift of the OVH. The OVH was found to be a better feature than the hydrogel volume for predicting rectal sparing.85 Wang et al. used OVH to build a treatment planning QA model from consistently planned pareto‐optimal plans for prostate cancer, improving planning standardization, and preventing validation with possibly suboptimal benchmark plans.112
In earlier OVH‐based IMRT studies, large dose variations were reported at a given OVH distance for a specific fractional volume of an OAR.47, 113 To address the variability of the distance‐to‐dose prediction, Wall et al. studied inherent inter‐planner variations across prior plans and characterized second‐order dosimetric and anatomical factors. Out of all these factors, in‐field bladder and rectal volume showed the strongest correlation (R = 0.86 and R = 0.76) with doses. Therefore, in‐field OAR volume was incorporated into the OVH only metric.91 The generic OVH introduced by Kazhdan et al. relies on a DVH rather than a spatial dose distribution.108 McIntosh and Purdie demonstrated that incorporating spatial information into the model can improve the dose prediction accuracy in comparison to the generic OVH method. The spatial information was found to improve dose prediction accuracy for certain disease sites—whole breast, rectum, and prostate cancer—yet was less important for other sites such as the breast cavity and lung.101
Projection‐based methods
Projection‐based algorithms typically use the perspective of the beam's eye view (BEV) and statistical analysis to assess the similarity between a new case and prior cases. A best‐matched prior case may be identified based on the sum of mutual information values calculated from each BEV perspective across all of the beams in a plan. This method has been used for prostate92 and head/neck cancer.97 Good et al. calculated mutual information to determine the best match for a query case with an additional deformation step to account for any differences in PTV size and shape. More specifically, the PTV projections from a matched case were deformed to the query case's PTV projections at each BEV. This KBP approach resulted in new treatment plans with improved OAR sparing, target dose conformity, and dose homogeneity compared to the original plans.93
DTH‐based methods
The distance‐to‐target histogram (DTH) plots the fractional volume of an OAR within a certain distance of the PTV surface. In addition to volumes of the PTV and OARs, the DTH metric is also used as an input feature in ML approaches to KBP. ML techniques include multivariable nonlinear regression (MVNLR) and support vector regression (SVR).46 It is important to note that DTH is equivalent to OVH 108 when distance is Euclidean. The DTH metric was extended to a generalized distance‐to‐target histogram (gDTH) by Zheng et al. in order to account for the relative shape and spatial arrangement of multiple PTVs in head/neck cancer.54 In comparison to the conventional model, the gDTH model improved DVH prediction accuracy for the brainstem, cord, larynx, mandible, parotid, oral cavity, and pharynx.54 While this gDTH model selects similar plans with respect to an individual OAR, the concept of gDTH was further extended to develop a knowledge‐based tradeoff hyperplane model. The expanded model selects similar plans with respect to all OARs by employing a case similarity metric that is a weighted sum of gDTH Euclidean distances between two cases across all OARs.114 Finally, the DTH has also been utilized with multivariate regression‐based models, which is commercially available as RapidPlanTM in Eclipse® treatment planning software.
3.1.3. Influence of various parameters
Outliers/Data inconsistency
Outlier detection is an important consideration when building a data‐driven dose prediction model that is generalizable to a variety of new cases. Outliers degrade the fit between geometry and dosimetry, which, in turn, can compromise model performance.109 Outliers may be geometric or dosimetric. Geometric outliers include large anatomical variations, such as OAR distance to the PTV. As an example, a model designed for prostate only RT should be built from prior cases only treating the prostate. The inclusion of a case treating both the prostate and pelvic nodes would be a geometric outlier. Several studies investigated the influence of outliers on model performance as shown in Table 4. Dosimetric outliers represent the presence of plans in which OARs are not optimally spared due to the planning technique. In other words, dosimetric outliers are the plans for which the re‐planning can significantly reduce OAR dose without compromising target coverage. Appenzoller et al. described a model to identify outliers from suboptimal plans and showed that excluding outliers in a refined model resulted in a strong correlation between the predicted and achieved doses after re‐planning (r = 0.92 for rectum, r = 0.88 for bladder, and r = 0.84 for parotid glands). In contrast to the negative impact of outliers on the performance of a KBP model, a previous study has shown a better OAR sparing in the presence of a small number of outliers in the KBP model.70 Results of a previous study showed that adding 5 to 10 outliers marginally improved salivary gland and swallowing‐muscle sparing for head/neck RapidPlanTM‐based KBP; however, adding more than 20 outliers showed a moderate degradation of plan quality.70
TABLE 4.
A list of articles with investigations on effects of outliers on plan quality and summary of evaluation metrics used by RapidPlanTM with a threshold in parentheses
| Ref. | Method | Outlier |
|---|---|---|
| 109 | Restricted sum of residual (RSR) | Dosimetric |
| 70 | Regression and residual analysis | Dosimetric |
| 115 | Leverage and studentized residual | Dosimetric, Geometric |
| 116 | Regression analysis scatter plots, cook's distance | Dosimetric, Geometric |
| 53 | Model‐based case filtering | Dosimetric, Geometric |
| RapidPlanTM |
Cook's distance (>10) Studentized residual (>3) Modified Z‐score (>3.5) Areal Difference of Estimate (>3) |
Dosimetric and Geometric |
Outlier detection has been studied for different disease sites and commercial software has metrics for identifying outliers. For pelvic RT, Sheng et al. assessed the effectiveness of outlier identification by studying the impact of both geometric and dosimetric outliers. This study suggested a greater impact of dosimetric outliers with a negative impact on both bladder and rectum model compared to geometric outliers with negative impact only on bladder model.115 Wang et al. studied the effects of data inconsistency with respect to planning prioritizations through a) mixed training dataset with a consistent validation dataset b) a consistent training dataset with a mixed validation dataset c) both a mixed training and validation dataset d) both consistent training and validation dataset and found that data inconsistency led to a large increase in prediction error with errord < errorc < errora < errorb.69 While outlying suboptimal plans may be removed from the training cohort,4 an alternative that maintains the training set size is to re‐plan those cases. This approach has been tested for prostate and head/neck cancer116 and lung cancer.36 Clinically available RapidPlanTM provides different statistical evaluation metrics for identifying the outliers as shown in Table 4.
Diversities within traditional KBP methods
In KBP, the knowledge from prior cases can be used in different combinations (e.g., creating VMAT KBP model by prior knowledge of IMRT plans for a given treatment site). Here, we present a review of studies that investigated the applicability of traditional KBP methods with respect to variations in external parameters and their combinations (e.g., cross‐modality, multi‐institution, sample size). Studies of this nature were performed on both platforms: retrospectively on a commercial KBP module (e.g., RapidPlanTM in Eclipse®) and in‐house built KBP models. Wu et al. 2013 used the DVH objectives derived from previous IMRT plans as an optimization parameter for VMAT treatment planning in head/neck cancer, resulting in a similar dosimetric quality compared to IMRT plans.84 Wu et al. demonstrated that the supine VMAT model for rectal plans can optimize IMRT plans of prone patients, yielding superior OAR sparing and quality consistency than conventional treatment planning method.117 The prediction models trained on Helical Tomotherapy for prostate cancer were utilized to predict constraints for optimizing new RapidArcTM plans. The result was similar/increased bladder and rectum doses compared to the expert plan. Delaney et al. demonstrated that using a model‐based only on photon beam characteristics could make the DVH predictions for proton therapy. This predictor could be used as a patient selection tool for proton therapy.42 McIntosh et al. studied contextual atlas random forest (cARF) algorithm with and without OAR region of interest features and found that the algorithm can pick better atlases without ROI features. However, the dose distribution could not be accurately mapped from those atlases onto a new patient.102
KBP models have successfully navigated some plan differences but not others. Huang et al. demonstrated that the RapidPlanTM model for one energy (10 MV) can generate dose–volume objectives for plans with 6 and 10 MV photon beam energy; however, a RapidPlanTM model for flattened beams cannot optimize un‐flattened beams prior to adjusting the target objectives.40 A RapidPlanTM module can generate high‐quality treatment plans compared to manually optimized plans for prostate cancer.71 For esophageal cancers, the RapidPlan created from plans optimized using RayStation produced comparable lung doses.38
KBP models have been investigated for standardizing plan quality across institutions. For patients enrolled in Radiation Therapy Oncology Group (RTOG) 0617, Kavanaugh et al. showed the feasibility of a single‐institution RapidPlanTM model as a quality control tool for multi‐institutional clinical trials to improve overall plan quality and provide decision support to determine the need for clinical trade‐offs between target coverage and OAR sparing.36 For prostate cancer, Schubert et al. have demonstrated the possibility of sharing models among different institutes in a cooperative framework.63 For prostate cancer RapidPlanTM among five different institutions, Ueda et al. suggested that it is critical to ensure similarity of the registered DVH curves in the models to the institution's plan design before sharing the models. Good et al. applied the prostate model trained with a dataset from their institute to generate plans for patient datasets outside of their institution with the potential of homogenizing plan quality by transferring planning expertise from more to less experienced institutions.93 Good et al. achieved superior or equivalent to the original plan in 95% of 55 test patients.93 More recently, a disease site‐specific multi‐institutional, NRG‐HN001 clinical trial‐based RapidPlanTM model was built as an offline quality assurance tool for which it improved the sparing of OARs in a large number of reoptimized plans submitted to the NRG‐HN001 clinical trial.35
Sample size
Figure 3 shows an average number of training and test set for each cancer site in traditional KBP methods with a standard deviation over the number of investigations listed on the top x‐axis. The number of training/test sample size was not directly mentioned or required in the methods described in some publications. We have also tabulated the list of retrospective studies performed by RapidPlanTM along with their treatment sites, training, and validation dataset size in Table 5.
FIGURE 3.
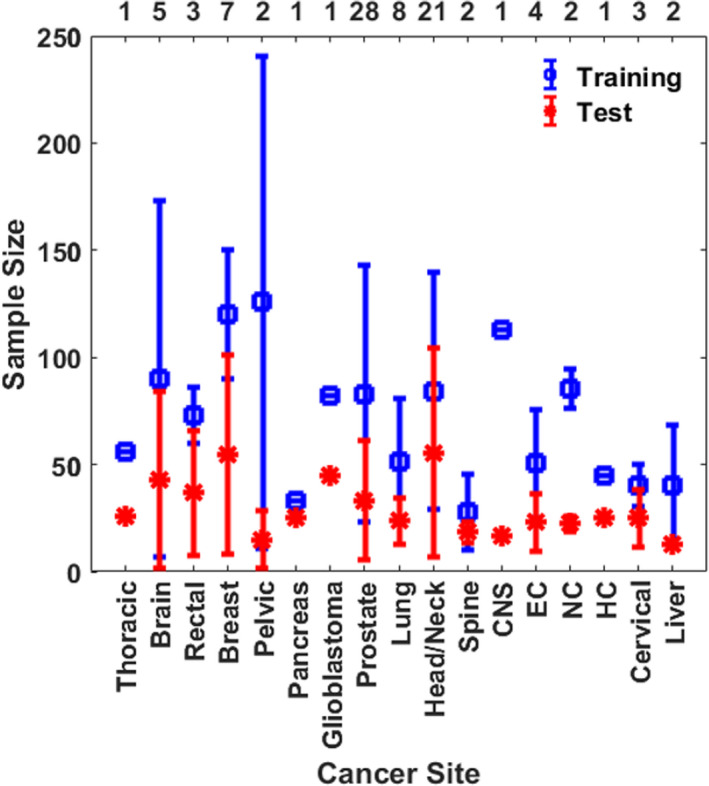
The average number of training and testing datasets in traditional KBP dose prediction methods for each cancer site. The values are averaged over the number of investigations listed on the top x‐axis and the error bars represent standard deviation. CNS, Central Nervous System; NC, Nasopharyngeal Cancer; EC, Esophageal Cancer
TABLE 5.
Summary of published works on KBP using RapidPlan module by Varian treatment planning system
| Ref. |
Training size |
Validation size |
Cancer site | Purpose |
|---|---|---|---|---|
| 34 | 57 | 23 | Lung (VMAT) | To develop an RP‐KBP model for malignant pleural mesothelioma for patients with two intact lungs |
| 35 | 50 | 50 | Head/Neck (IMRT) | To establish a threshold of improvements of treatment plans submitted to the clinical trials for head‐neck cancer (NRG‐HN001) through a multi‐institutional KBP model |
| 36 | 104 | 25 | NSCLC (VMAT) | To evaluate the feasibility of single institution KBP model as a dosimetric quality control for multi‐institutional clinical trials to RTOG 0617 |
| 37 | 30, 60 | 13 | Liver (IMRT) | To study prediction capability of RP general model (Model G with 60 cases) versus RP‐specific model (Model S with 30 cases) and benchmark against clinical plans for liver IMRT |
| 38 | 40 | 24 | Esophageal cancer (VMAT) | To evaluate RP‐KBP for training models with plans optimized with a different treatment planning system (Eclipse and RayStation) |
| 39 | 48 | 25 | Prostate (VMAT) | To demonstrate the effectiveness of RP‐KBP for hypofractionated, multi‐target prostate patients |
| 42 | 30 | 10 |
Head/Neck (VMAT, Proton) |
To investigate whether RP based only on photon beam characteristics can be used to generate DVH‐predictions for proton therapy and whether this could correctly identify patients for proton therapy |
| 55 |
35 (LR) 30 (HR) |
10 HR and 10 LR VMAT |
Prostate (VMAT) | To use KBP models created from helical tomotherapy plans [35 low‐risk (LR) and 30 high‐risk (HR)] for generating plans with different techniques (VMAT) |
| 56 | 79 | 20 | NPC (IMRT) | To investigate the improvements in planning efficiency and quality for patients with NPC IMRT treatments |
| 57 | 82 | 45 | GBM (VMAT) | To create an initial RP‐based KBP model for glioblastoma (GBM) and evaluate the planning efficiency of RP‐based planning against typical manual planning |
| 59 | 70 | 24 | Esophageal (VMAT) | To evaluate the performance of the RP module for esophageal cancer VMAT |
| 60 | 45 | 25 | Liver (VMAT) | To evaluate the performance of RP‐based optimized plan against manually created plans for hepatocellular cancer for clinical acceptability |
| 61 | 38 | 10 | Spine (SBRT) | To determine if RP is effective in improving the quality and efficiency of spine SBRT planning and evaluate the model for outliers |
| 62 |
40 (P) 37 (C) |
10 (P) 10 (C) |
Prostate (IMRT) Cervical (VMAT)) | To determine whether the RP module can efficiently produce IMRT and VMAT plans in the pelvic region in a single optimization and benchmark |
| 63 | 43 | 60 (10, 7, 6, 7,13, 10, 7) | Prostate (VMAT) | To perform the multicentric validation of RP models on seven different centers and compared with corresponding manually optimized plans |
| 65 | 30,30 60 | 15, 15 | Head/Neck (VMAT) | To study whether differences in the composition of plan libraries influenced RP results for two patient groups using three different libraries and benchmark the model versus clinical plans. To evaluate the influence of model size |
| 64 | 90 | 20 | Head/Neck (VMAT) | To evaluate the potential of RP to automate the process for identifying the quality of patient‐specific plans through the correlation between predicted and achieved mean doses to the different OAR structures |
| 66 | 20, 53, 60, 100, 123 | >20 | Prostate (VMAT) | To evaluate the performance of RP‐KBP at multiple radiation therapy departments and check its suitability for sharing the models. |
| 67 | 80 | 70 | Rectal (SIB) | To investigate the performance of RP‐KBP compared to manually optimized clinical plans for rectal SIB cases. |
| 68 | 40 |
11 (Int.) 22 (Ext.) |
Spine SBRT | To investigate whether a validated KBP model for NRG Oncology RTOG 0631 could be used as a retrospective clinical trial quality control tool |
| 70 | 70 | 10 |
Head/Neck (VMAT) |
To study the influence of outliers (Suboptimal plans) on the prediction of RP plans by adding suboptimal plans into a clean model with the increment of five plans. |
| 74 | 83 | 20 | Head/Neck (VMAT) | To assess the stability of RP generated plans for a different beam geometry, different management of bilateral structures, and dose fractionations. Two models were generated: a model separating ipsi‐and‐contralateral parotids and a model associating two parotids to a single structure. |
| 75 | 51 | 30 | Prostate (VMAT) | To investigate whether RP plans created through a single optimization (without any planner intervention during optimization) are clinically acceptable for prostate cancer patients |
| 76 | 51 | 35 | Cervical (IMRT) | To demonstrate an efficient method to train, refine (i.e., according to clinical trial dosimetric objectives), and validate the KBP model for an automated quality control system |
| 71 | 60 | 20 | Prostate (IMRT) | To investigate the role KBP can play in aiding a clinic's transition to a new treatment planning system |
| 78 | 81 | 30 | Pelvic (VMAT) | TO test if RP DVH estimation can be improved interactively through a closed‐loop evaluation process |
| 117 | 81 | 10 | Rectal (VMAT) | To study whether RapidPlan model trained on a technique (VMAT) and orientation can be used for another (30 IMRT plans) |
| 72 | 27, 27 | 25, 25 |
Lung (VMAT) Prostate (VMAT) |
To evaluate the performance of a model‐based optimization process for prostate and lung VMAT plans and evaluate its predictive power compared to manually created plans. |
| 73 | 150 | 70 | Breast (VMAT) | To evaluate the performance of a model‐based optimization process for whole breast VMAT |
Abbreviations: DVH, dose–volume histogram; IMRT, intensity‐modulated radiation therapy; KBP, knowledge‐based planning; NPC, nasopharyngeal carcinoma; NSCLC, non‐small cell lung caner; RP, rapid‐plan; VMAT, volumetric‐modulated arc therapy.
The size of the training set is an important consideration when building a KBP model. For RapidPlanTM, it is indicated that the minimum number of plans required for model creation is 20; however, adding additional plans will usually help create a more robust plan.118 Numerous studies have compared the quality of plans generated by RapidPlanTM by high‐quality plans in training and found that 25–30 plans may produce a clinically acceptable plan for prostate72 and head/neck65 cancer. Zhang et al. showed that approximately 30 plans were sufficient to predict dose–volume levels with less than 3% relative error in both head and neck and whole pelvis/prostate.79 For prostate cancer, Boutilier et al. analyzed the effects of the training set size on the accuracy of four models from three different classes: DVH point prediction, DVH curve prediction, and objective function weights. The authors concluded that the minimum required sample size depends on the specific model and endpoint to be predicted.119
The requirement of sample size also partially depends on the robustness of the model used. Yuan et al. used 64 and 82 cases for prostate and head/neck case, respectively, in support vector regression (SVR) model for DVH predictions.47 Landers et al. demonstrated statistical voxel dose learning (SVDL) to be more robust to patient variability compared to spectral regression and SVR for noncoplanar IMRT and VMAT for head/neck, lung, and prostate cancer by 20 cases for each site in fourfold cross‐validation.110 An atlas‐based dose prediction101 is the more sophisticated method in which each patient in the training set represents 1 atlas. Feature extraction and characterization are typically performed on CT of the patients, which results in probabilistic dose estimates to find the most likely voxel dose from similar atlases. In comparison to artificial neural network (ANN) and SVR methods, large training sample sizes were required for this method (58 for rectal, 77 for lung, 97 for breast cavity, 113 for central nervous system (CNS) brain, 144 for breast, and 144 for prostate cancer).
Treatment planning efficiency
KBP methods may reduce the treatment planning time by minimizing the number of trial‐and‐error steps performed by a person in the treatment planning process. For the commercial KBP module, the total time including data collection, training time, generation of constraints and objectives, and optimization time can depend on the treatment type (i.e., VMAT or IMRT), design (i.e., number of arcs or angles), site (i.e., simple, or complex), and available GPU. For glioblastoma disease site, structure selection and generation of constraints and objectives took 2 minutes for both an IMRT and a 2‐arc VMAT plan, whereas the optimization and dose calculation step took 5 minutes for an IMRT plan and 11 minutes for a 2‐arc VMAT plan. Moreover, it took a planner about 4 hours to create a plan without any KBP module assistance.57 For nasopharyngeal cancer, Change et al. demonstrated that using RapidPlanTM module reduced the average planning time substantially—(295 minutes vs. 64 minutes)—compared to the average planning time of plans created without using RapidPlanTM module. For malignant pleural mesothelioma, the time taken with RapidPlan was 20 minutes compared to 4 hours for manually created plans by an experienced treatment planner.34 The time taken to generate objectives and optimize a plan is reported to be ranging from 15 to 120 s and 300 to 1620 s, respectively.42, 55, 56, 57, 72, 73, 74 The planning time when used auto‐planning by pinnacle (APP) has also been reported to be 135 min for a single arc VMAT plan for esophageal cancer.120 The protocol‐based APP‐based plans have been shown to reduce the manual time spend per treatment plan due to their large clinical acceptance rate.120, 121, 122, 123, 124 In general, the use of KBP resulted in improved treatment planning efficiency when compared with manually created plans.
3.1.4. Summary
Overall, the review of traditional KBP dose prediction publications thus far suggests an improved efficiency compared to manual optimization, sufficient flexibility of traditional KBP methods in terms of their applicability (i.e., multimodality in EBRT), the need of these models for dynamic sites (i.e., pancreas), the requirement of an automated approach for accounting for outliers to further enhance the treatment planning efficiency,70 and the potential of building site‐specific universal RapidPlanTM models for multi‐institution adaptation.
3.2. Deep learning
DL offers numerous advantages across the different multidisciplinary steps of radiotherapy treatment planning. In contrast to traditional KBP methods, DL methods can learn features directly from the raw dataset. Because DL methods are good at discovering intricate structures in high‐dimensional data, DL methods are able to solve a wide range of scientific problems.125 Neural networks underpin DL methods in learning various tasks. A multilayer perceptron has fully connected networks in which each neuron in one layer is connected to all the neurons in the next layer. Multilayer perceptron is now succeeded by CNN, a class of DNN with regularized multilayer perceptron.126 A CNN is by far the most widely used DNN for the dose prediction task as can be seen in Table 6. The main components of a typical CNN are convolutional layers, max‐pooling layers, batch normalization, dropout layers, a sigmoid or softmax layer. These components of CNN will be summarized below. Additionally, other neural network designs will also be described briefly for conceptual understanding prior to reviewing works on the dose prediction task.
TABLE 6.
A list of publications on DL‐based dose prediction for various treatment sites
| Ref. | Architecture | Input | Output |
|---|---|---|---|
| 127 | ANN | Number of fields, PTV volume, PTV to OAR distance, azimuthal and elevation angles | 3D |
| 128 | ANN |
Distance to PTV, Distance to OARs PTV volume |
3D |
| 129 | ANN | 16 different geometrical features | 3D |
| 27 |
Modified U‐net |
PTV + OAR + Prescription | 2D |
| 25 | ResNet‐50 | CT + OAR + PTV images + dose distribution image | 2D |
| 26 | 3D‐FCN | 3D CT + OAR + Prescription | 3D |
| 130 | U‐Res‐Net | 3D CT + OAR | 3D |
| 131 | GAN | Contoured CT images + dose distribution | 2D |
| 132 | HD U‐Net | OAR + PTV + Beam information with approximated dose | 3D |
| 133 |
CNN ‐ Res‐Net 101 |
Contoured images + coarse dose map, with out of field labels | 2D |
| 134 | U‐Net | PET and CT image patches | 3D |
| 135 | HD U‐Net | OAR + PTV | 3D |
| 136 | U – Net |
CT only, CT + ISO, CT + Contours, CT + ISO + Contours |
2D |
| 137 | Modified 3D U‐Net | DVHs + Contours | Pareto Dose Distributions |
| 138 | U‐Net |
PTV + Body + OAR, PTV + Body + OAR + Dose information from selected beam angles |
Pareto Dose Distributions |
| 139 | 3D U‐Net DRN | CT + FMCV | 3D |
| 140 | Modified U‐Net | Density map + 3D CT +Activity map | 2D |
| 141 | U‐Net | PTV + OAR contours | 3D |
| 142 | GAN |
CT + RT Doses, PTV + OAR |
2D |
| 143 | ResNet−50 | CT + OAR +PTV + body contours | 3D |
| 144 | U‐Net | Low‐resolution dose + CT | 2D |
| 145 | HD U‐Net | CT + RT dose distribution | 3D |
| 146 | GAN | CT + PTV + OAR | 2D |
| 24 | Attention gated GAN | CT + PTV + OAR | 3D |
| 147 | GAN | PTV + OAR + Body | Pareto Dose Distribution |
| 148 | 3D GAN | Contoured CT images | 3D |
| 149 | 3D U‐Net + Residual Network | CT + OAR + PTV contours + Beam + Dose | 3D |
| 150 | 3D U‐Net | OAR + PTV contours | 2D |
| 151 | Dense‐Res hybrid Network | Beam + structural information | Static field fluence prediction |
| 152 | Virtual Treatment Planner Network | DVH | TPPs adjustment action |
Abbreviations: DRL, deep reinforcement learning; DVH, dose–volume histograms; FMCV, fluence map converted volume; GAN, generative adversarial network; HD, hierarchically dense; OAR, organ at risk; PTV, planning target volume; TPP, treatment planning parameter.
The convolutional layer consists of a set of convolutional kernels where each kernel acts as a filter. First, the image receptive fields are processed through a series of convolutional kernels that aid in extracting features. Kernels use a specific set of weights to convolve with corresponding elements of the receptive field. The weight sharing ability of convolutional operation allows the extraction of different sets of features within an image by sliding kernel with the same set of weights on the image. This makes CNN more efficient than the fully connected networks. This operation can be grouped based on the type and size of filters, direction of convolution, and type of padding.125
From the result of the convolution operation, the feature motifs can occur at different locations in the image. The goal is to preserve its approximate position relative to others rather than the exact location. The pooling or down‐sampling sums up similar information in the neighborhood of the receptive fields and outputs the dominant response within this local region, helping to extract the combination of features that are invariant to translational shifts.153 Commonly reported pooling formulations used in CNN are max, average, L2, spatial pyramid pooling, and overlapping.154, 155
A nonlinear operation, also known as an activation function, helps in the learning of sophisticated patterns by serving as a decision function. Different activation functions reported in the literature are sigmoid, tanh, SWISH, ReLU,125 and its variants including leaky‐ReLU, parametric ReLU (PReLU) have also been used to inculcate the non‐linear combination of features.155, 156, 157, 158, 159 MISH is a more recently proposed activation function, which has shown better performance than ReLU on benchmark datasets.160 ReLU and its variants are generally preferred as activation functions because of their ability to overcome the vanishing gradient problem.161
Batch normalization is applied to address the issue of internal covariance shifts, a change in the distribution of hidden unit values within the feature maps that can reduce the convergence speed. Batch normalization essentially unifies the distribution of feature map values by setting them to zero mean and unit variance, which, in turn, improves the generalization of the network by smoothening the flow of the gradient.162
Finally, overfitting occurs when the model is trained to closely or even exactly fit a set of training data at the expense of degraded model generality as it would fail to learn general underlying patterns within the data.163 Different approaches such as dropouts, data augmentation, and weight regularization have been used for preventing model overfitting. While a typical neural network has all nodes activated during training, a dropout layer omits a combination of certain nodes along with their connections from the neural network each time the gradient is updated, which, in turn, prevents the network from over‐adaptation.164 Other forms of regularization include early stopping criterion, weight regularization, bias adding, data augmentation, and model combination. Briefly, early stopping criterion is the stoppage of the training when a specific performance measure in the form of validation loss or accuracy is reached. L1 and L2 regularization are common examples of weight regularization in which a regularization term, alpha, is added to the loss function. The idea behind the weight regularization is to find the right balance between alpha and the model complexity as it can lead to either underfitting (fails to perform well on both training and unseen dataset) or overfitting (performs extremely well on training but fails to perform well on an unseen hold‐out dataset). Data augmentation method inflates the training dataset size by warping, which preserves their labels, or by oversampling, which creates synthetic instances to increase the training dataset size.165
Loss function, in its simplest form, is the difference between the predicted and the target output. A loss function is presented in the form of an objective function that is to be minimized during the backpropagation step to improve the network performance. Janocha et al. investigated how different choices of loss functions affect deep models and their learning abilities, as well as robustness to various effects.166 While log loss performed well, other losses may also be preferable depending on the application of a given model.166
Backpropagation is a widely used technique in both traditional ML and recently emerging DL methods. Briefly, it systematically allows improvements in weights and biases to further improve the network's prediction in three steps: (1) feed‐forward network with learnable parameters; (2) network's performance is measured with a loss function; (3) the error is backpropagated through the network to alter the learnable parameters. This process is typically achieved through a gradient descent which allows for instantaneous rates of change between the parameter to the neural network's error. Deeper networks with many layers tend to train slowly due to gradient exploding/vanishing. For faster and efficient learning, He et al. proposed to utilize the residual functions instead of directly fitting a desired underlying mapping.167 A densely connected neural network (DenseNet) by Huang et al. connects each layer to every other layer.168 More recently, the attention gate was introduced in CNN in order to suppress irrelevant features and highlight salient features useful for a given task.169
3.2.1. Deep artificial neural network
The simplest form of ANN consists of three layers: an input layer, the hidden layer, and the output layer. Neurons within each layer are nodes which are connected to subsequent nodes via links that correspond to biological axon‐synapse‐dendrite connections, analogous to the neural cell of human. The hidden layer is embedded between an initial input layer and the final output layer. The use of DL in dose prediction was initially utilized in the form of ANN.127 Therefore, ANN‐based studies are included in the DL‐based dose prediction category in Table 6. In these earlier methods, organ volumes including PTV and OARs, number of fields, and distances from OARs to the PTV were used to train ANN, which was then used to correlate dose at a given voxel to several geometric and plan parameters. The earlier ANN‐based methods were, therefore, similar to the traditional KBP methods in terms of framework. Deep ANN, moreover, consists of multiple hidden layers in addition to an input and an output layer, separating itself from the original three‐layer ANNs. In general, the number of layers determines the network's depth, and the number of neurons determines its width. Deep ANNs can learn deeper features by filtering information through multiple hidden layers. Each neuron between its input and output undergoes a linear followed by a non‐linear operation. In DL‐KBP, the ability of deep ANN to teach itself, through multiple hidden layers between input and output layer, provides the flexibility of presenting raw information without having to extract different geometric features.
In layered format, each neuron receives information from the neurons in the previous layer and passes processed information to neurons of the next layer. Alternatively, residual connections can be added to connect neurons in non‐adjacent layers such as ResNet proposed by He et al.170 The ResNet architecture has been presented with different numbers of layers: ResNet (18, 34, 50, 101, 152). Many DNN architectures have been presented for various applications. The fully convolutional neural network (FCN) and fully connected CNN (FCNN) have been applied so far for the dose prediction task (Table 6). Figure 4 shows the flowchart of the CNN and its extended networks.
FIGURE 4.
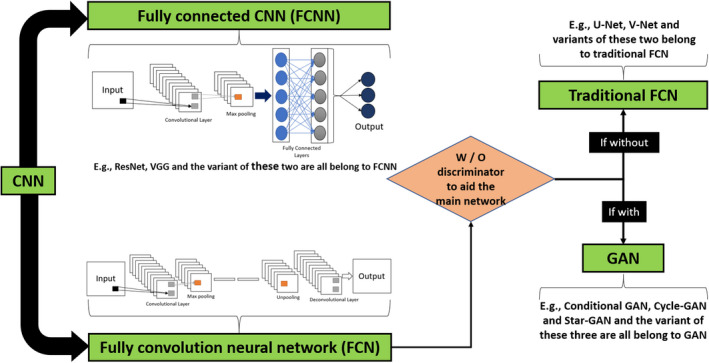
Flow chart of convolutional neural network (CNN) with its extended networks
3.2.2. Convolutional neural network
CNNs, including fully convolutional neural network (FCN) and fully connected CNN (FCNN), have been applied so far for the dose prediction task (Table 6). Figure 4 shows the flowchart of the CNN and its extended networks. Different architectures have been proposed in the literature to enhance the performance of CNN. U‐Net, originally built for the segmentation of neuronal structures in electron microscope stacks,23 is one of the most widely used architectures in CNN. In addition to segmentation, it is also used for image‐to‐image translation tasks that outputs an image that has a one‐to‐one voxel correspondence with the input. U‐Net permits effective feature learning even with a small number of training sample size. Milletary et al. proposed a three‐dimensional variant of U‐Net known as V‐Net.171
3.2.3. Generative adversarial network
Generative adversarial network (GAN) is a widely used supervised learning method in DL.172 Two major components of GAN are generative network and discriminator network that are trained concurrently to compete against each other. The goal of the generative network is to generate artificial data that can approximate a target data distribution from a low‐dimensional latent space, whereas the goal of the discriminator network is to recognize the data presented by the generator and flag it as either real or fake. For the dose prediction task, the artificial data generator is replaced by the predicted dose map, which then goes through the discriminator in order to be identified as a realistic or an unrealistic dose distribution. Both, dose map generator and discriminator, networks get better over the course of training to reach Nash equilibrium, which is the minimax loss of the aggregate training protocol.172 Some of the popular variants of GAN include CycleGAN,173 conditional GAN (cGAN),174 and StarGAN.175 GAN is widely used in medical imaging.13, 16, 17, 176
3.2.4. Reinforcement learning
Reinforcement learning (RL) trains an agent, connected to its environment through perception and action, to make adjustments based on the interaction between the agent and the environment. The agent gets certain indications about the current knowledge of the environment at each step of its interaction. Based on this indication, the agent then chooses an action to generate an output. This action changes the state of the environment, the value of this state transition is communicated to the agent through a reward function. The agent's behavior can learn to do this over time through exploration and exploitation.163
3.2.5. Deep learning in dose prediction
DL‐based dose prediction methods can be categorized according to DL properties such as network architectures (CNN, GAN, etc.), input image types (CT only, CT + OAR + PTV contours, etc.), output types (2D or 3D dose distribution), and sample size (training, testing, etc.). As shown in Figure 1, DL‐based dose prediction methods have gained popularity among the researchers only in the past few years, there are nearly 30 publications on DL‐based dose prediction as of August 2020. These DL‐based dose prediction publications are tabulated in Table 6 along with their network architectures, input, and output characteristics. Figure 5 represents the total number of DL‐based dose prediction investigations per treatment site. This follows a similar trend to that observed for traditional KBP methods with the highest number of investigations being on prostate and head/neck cancer sites. Here, we categorized DL‐based dose prediction publications thus far into three groups based on network architectures: I) CNN – namely U‐Net architecture, II) GAN, and III) RL. We first provide the review of work for each network architecture followed by their applicability on various dose prediction applications and limitations. Subsequently, we discuss the influence of different parameters in DL‐based dose prediction methods.
FIGURE 5.
The total number of DL‐based dose prediction investigations for various cancer sites. NC, Nasopharyngeal Cancer; PD, Personalized Dosimetry
3.2.6. Overview of CNN‐based works
As shown in Table 6, U‐Net has been widely used CNN architectures used for predicting dose distributions. U‐Net is effective in terms of end‐to‐end learning of global and local features because it consists of encoding and decoding paths. The decoding path concatenates the features from both previous layers in the encoding path and features from current layers in the decoding path. Many variants of U‐Net including 3D U‐Net have appeared in the literature for dose prediction purposes (Table 6).
Earlier work in DL‐based dose prediction methods involved predicting doses in a 2D manner.25, 27 Sumida et al. used the U‐net model, initially proposed by Ronneberger et al.23 to make 2D dose prediction. The network was trained to make dose prediction for Acuros XB (AXB) from low‐resolution dose calculated through AAA algorithm and CT.144 Similarly, Nguyen et al. also trained a seven‐level hierarchy with a modified version of the original U‐Net to make dose prediction for a prostate case.27
More recent works were focused on predicting 3D dose distributions using DL methods. To overcome increased computation load in 3D dose prediction, Nguyen et al. proposed Hierarchically Densely U‐Net (HD U‐Net), which not only was able to predict 3D dose distribution, but also outperformed dose predictions made by the standard U‐Net model.135 HD U‐Net combines DenseNet's efficient feature propagation and utilizes U‐Net's ability to infer both local and global features by connecting each layer to every other layer in a feed‐forward fashion, yielding better RAM usage, and better generalization of the model. To further simplify the 3D dose prediction problem and increase prediction accuracy, Xing et al. projected the 2D fluence maps onto the 3D dose distribution using a fast and inexpensive ray‐tracing dose calculation algorithm and trained HD U‐Net to map the ray‐tracing low accuracy dose distribution (does not consider scatter effect) into an accurate dose distribution calculated using collapsed cone convolution/superposition algorithm.145
DL‐based methods have also been expanded to predict pareto optimal dose distributions so that physicians can learn the desired dosimetric trade‐offs in real‐time and learn the viability of different dosimetric goals. Ma et al. constructed the 3D U‐Net architecture to predict individualized dose distribution for different tradeoffs.137 In predicting the pareto dose distribution, the network should be able to map many dose distributions from single anatomy, and in doing so differentiate between the clinical consequences of corresponding predicted dose distributions. To address this clinical tradeoff problem across different dose distributions, Nguyen et al. proposed the differentiable loss function based on the DVH and adversarial loss in addition to traditional voxel‐wise mean square error (MSE) loss to train the network.147 Along the same line of work, Bohara et al. incorporated beam information to predict pareto dose distribution using anatomy beam model proposed by Barragán‐Montero et al.138
U‐Net architecture has also been used for radiopharmaceutical dosimetry.134, 140 The network was trained to predict 3D dose rate maps given the mass density distribution and radioactivity maps. The current clinical standard is the decades‐old Medical Internal Radiation Dose Committee (MIRD) formulism which is limited by somewhat crude analytical equations. The long‐term goal of the U‐Net studies is to create a stable DL‐based dose estimation model that achieves a precision close to that of Monte Carlo simulations.
He et al. proposed the residual network, known as ResNet, to mitigate the difficulty of training DNN caused by gradient vanishing.170 He et al. reformulated the layers as a learning residual function instead of directly fitting a desired underlying mapping. Chen et al. and Fan et al. proposed the DL method based on ResNet with 101 and 50 weight layers, respectively, to predict dose distribution for head/neck cancer IMRT patients.133, 143 Since networks with very deep layers are difficult to train due to vanishing gradient, such networks used shortcut connections to add to the outputs of the stacked layers.170 More recently, Liu et al. proposed ResNet for dose prediction in the nasopharyngeal cancers for Helical Tomotherapy. To achieve multi‐scale feature learning, Liu et al. divided the ResNet into several parts without fully connected layers and respectively combined with input data to achieve pixel‐wise feature abstraction and extraction in the structural image.130
3.2.7. Overview of GAN‐based works
GAN entails a pair of neural networks: a generator and a discriminator. From the treatment planning standpoint, the generator could be represented as the treatment planner who generates the plan, and the discriminative network could be represented by a radiation oncologist who evaluates the generated plan. Both the treatment planner and a radiation oncologist get better at performing their tasks as they become more experienced over time. Only a handful of studies have investigated the performance of GAN for dose prediction task as shown in Table 6.
Mahmood et al. demonstrated the first use of 2D GAN for predicting dose for each 2D slice independently for oropharyngeal cancer. Subsequently, Babier et al. proposed the first 3D GAN for the prediction of full 3D dose distributions, which outperformed the 2D GAN model proposed by Mahmood et al. presumably owing to its ability to learn the 3D features in contrast to 2D features by 2D GAN networks. Recently, Vasant et al. proposed a novel 3D attention‐gated generative adversarial network (DoseGAN) as a superior alternative to the current state of the art dose prediction networks.24 Spatial self‐attention allows networks to emphasize portions of the intermediate convolution layers. Attention gated GAN can potentially offer deeper and more efficient discrimination, while being trained in parallel with the generator network and facilitating the model convergence.24, 177 This addresses the issue of keeping the number of network parameters as low as possible in conventional GAN. Attention‐gated GAN proposed by Vasant et al. outperformed conventional 2D and 3D GAN in all dosimetric criteria including PTV and OARs.24
All four studies 24, 131, 142, 148 on GAN‐based dose predictions constructed a generator and discriminator network using the pix2pix architecture proposed by Iosa et al.178 In these studies, U‐Net is used as a dose map generator that passes a contoured CT image slice through consecutive layers, a bottleneck layer, and subsequent deconvolution layers. U‐net also uses skip connections to easily pass high‐dimensional information between the input (CT image slice or contoured structures) and the output (dose slice).
3.2.8. Overview of RL‐based works
RL is a unique framework that resembles the workflow of treatment planning optimization. RL has been combined with DNN to accomplish human‐level performances for decision‐making tasks.179 In order to implement the RL‐based framework for dose prediction task, in‐house treatment planning system and RL architecture must be synchronized in a single pipeline, which is implemented by only a few research groups.151, 180 Recently, RL was used to train a DNN named virtual treatment planner network, which learns to adjust treatment planning parameters to improve plan quality similar to the treatment planning process.152, 180 The use of the trained network to perform treatment planning improved plan quality score compared to the initial plan. In comparison to U‐Net and GAN, deep RL is one of the least studied networks for dose prediction tasks presumably due to the high action space of the actual treatment planning process.
3.2.9. Overview of learning processes
Three commonly used learning processes include unsupervised learning (USL), semi‐supervised learning (SSL), and supervised learning (SL). In this section, we briefly present a review of SL due to its wide adoption in dose prediction application. SL refers to a technique that utilizes labeled data with input‐output correspondence to train the model. The learning goal during training is defined by the paired input data and output target. While both, traditional KBP and DL‐based KBP, methods largely use the SL framework to train models, each presents a different framework with regards to labeled data with input. For instance, one subcategory of SL is regression analysis, which establishes a relationship among the variables by estimating how one set of variables affect their corresponding response variables (i.e., relationship between the distance of OAR to target and doses to OAR). As can be seen in Tables 1, 2, 3, various regression analyses were performed in traditional KBP methods. DL‐based KBP methods use CNN to learn contour‐to‐dose mappings in a supervised manner with the clinically generated dose map being the learning target. The discriminator in the GAN‐based model learns to discriminate between predicted dose map and real clinical dose map, therefore, belongs to supervised learning. Therefore, the network is trained through adversarial loss and able to predict more realistic dose distributions.177
3.2.10. Influence of various parameters on DL‐based model performance
Input parameters
In terms of the number of input parameters, Williems et al. studied the impact of four different inputs (Table 6) for dose prediction under with and without data normalization of dose distribution. The order of models in terms of performance was CT + isocenter + contours >CT + contours >CT + isocenter >CT only. While the dose distribution normalization had more benefits for CT + contours, it was found to be less necessary for CT +isocenter + contours model. Whereas, normalization produced hot and cold spots for CT + isocenter model.136
While many studies use only CT with anatomical information (i.e., PTV and OAR contours) as inputs to the CNN27, 132, 135 as can be seen in Table 6, Barragán‐Montero et al. included beam geometry information along with anatomical information as inputs. As a result, the model was able to learn from the database that was heterogeneous in terms of beam configurations (i.e., noncoplanar),132 which was the limitation of the network proposed in the earlier studies.27 For rectal cancer IMRT, Zhou et al. showed improvements in the prediction accuracy by including beam configurations as input to the network compared to that of without beam configurations.149 For head/neck cancer, Chen et al. investigated the influence of adding out of field labels into the network training to deal with inability of 2D network to account for radiation beam geometry. It resulted in a better overall performance compared to the network excluding out‐of‐field labels.133 For prostate cancer, Murakami et al. compared the performance of CT‐only‐based GAN with contour‐based GAN in predicting target dose map and found prediction performance of contoured‐based GAN to be superior.
Loss functions
In terms of losses, MSE is one of the most widely used cost functions in DL methods as it has many desirable properties from an optimization standpoint. Owing to its simplicity, well‐behaved gradient, and convexity, majority of previous studies including the ones shown in Table 6 utilized only MSE loss for dose prediction. Nguyen et al. combined domain‐specific loss function based on DVH with adversarial loss and MSE loss for the training of deep neural networks. While this approach outperformed dose predictions compared to the MSE‐based trained model, for the same computational system, it increased the training time to 3.8 days with 100000 iterations compared to 1.5 days for MSE only based network.147
Lee et al. and Chen et al. utilized mean absolute error (MAE) cost function between the ground truth and dose rate map predicted by CNN.133, 134 As compared to MSE, MAE is more robust to outliers but may be less efficient to find the solution, whereas MSE provides a more stable and closed‐form solution. Other loss functions may include Huber loss, smooth mean absolute error, quantile loss, and log cosh loss function. So far, the MSE loss function has been the standard cost function used in DL‐based dose prediction studies.
Sample size
In general, the DL‐based methods require a large number of high‐quality data to be effective. Small datasets in DL can be challenging as it may result in overfitting. Data augmentation,144 dropout layer,164 estimation based on the training and the validation curves,135 synthesizing new data based on physics principles,181 and incorporating regularizations to model parameters 182 have been used in the literature to prevent overfitting. The process of data augmentation, more commonly used in dose prediction approaches, is to expand the dataset by synthesizing additional realistic samples from available samples. It is important to note here, however, that the process of augmentation to be used depends on the suitability of the context. For the purpose of dose prediction, we have presented the average training and testing sample size for each treatment site in Figure 6 for all DL‐based dose prediction methods to date, which provides the readers with an approximate range of training and testing dataset for each cancer site.
FIGURE 6.
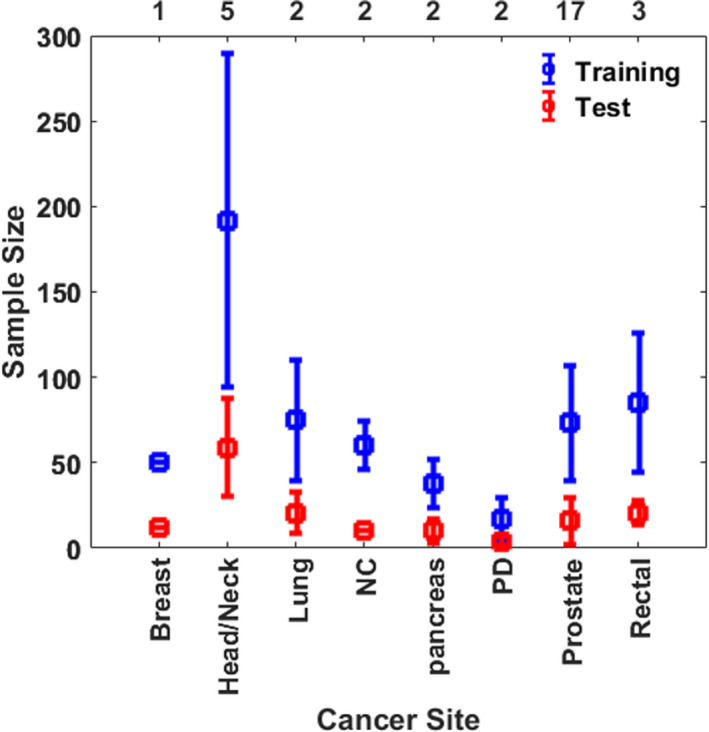
The average training and testing sample size in DL‐based dose prediction methods for each cancer site. The values are averaged over the number of investigations listed on the top x‐axis and the error bars represent standard deviation. NC, Nasopharyngeal Cancer; PD, Personalized Dosimetry
As shown in Table 6, three investigations on prostate cancer have been reported for predicting pareto optimal dose distributions.137, 138, 147 For each patient in the training set, 10, 100, and 500 plans were generated by Ma et al. Nguyen et al. and Bohara et al. respectively, to sample the pareto surface with different tradeoffs. An optimal number of plans per patient in training set is unknown as it may depend on case to case basis. Nonetheless, in the case of predicting pareto optimal plans, it may be ideal to stay within a clinically relevant regime by including only those plans that cover dosimetric trade‐offs presented by a physician.
Kandalan et al. studied the issue of generalizing DL‐based dose prediction models and make use of transfer learning to adapt a DL dose prediction model to different planning styles in the same institutions and planning practices at different institutions. A source model was adapted to four different planning styles only with 14–29 cases.150 A long‐term goal of these studies is to generate a universal model that can easily be transferred to different institutions for a similar task.
4. DISCUSSION
With the goals of improving plan quality and efficiency, researchers have investigated KBP to guide treatment planning for a new patient. In the last decade, there has been a rapid growth in the number of publications in traditional KBP dose prediction. More recently, the number of publications on DL has increased exponentially because of its flexibility and superior performances compared to many state‐of‐the‐art techniques. Over 90 articles have been published on traditional KBP dose prediction methods between 2011 and August 2020, whereas over 17 publications have already been published on DL‐based dose prediction as of August 2020.
In general, most publications demonstrate improvements in comparison to manually optimized clinical plans in terms of both treatment planning quality and efficiency. A large number of manuscripts were published on traditional methods between 2015 and 2018, with the highest number of publications in 2017. This is presumably due to the commercialization of the RapidPlanTM in Eclipse® treatment planning software in 2014, which allowed researchers from different centers to perform retrospective studies for investigating the influence of various parameters on the quality of plans generated through commercial KBP module. In addition to RapidPlanTM, RayStation allows a scripting option that allows user to implement a mathematical dose prediction model as demonstrated in.89 However, the automatic treatment planning module of RayStation has not been largely investigated as it may not be widely available to the users to perform retrospective investigations. An auto planning by Pinnacle (APP) is another commercially available software. It is a protocol‐based method that performs iterative optimization steps to reach a final plan compared to using the machine learning‐based method.122 Nonetheless, we have also tabulated these additional APP‐based clinical studies with their key findings in Table 7.
TABLE 7.
Summary of research papers on automatic plans generated in Pinnacle (APP) with their key findings
| Ref. |
Cancer Site |
Key Findings |
|---|---|---|
| 183 | Esophageal | APP plans were preferred for 31/32 patients and achieved lower mean doses to the lungs. APP plans and manually created plans achieved similar target coverage |
| 124 | Advanced head/neck | In a 10 patients’ study, the human‐driven plans achieved better target homogeneity, whereas the APP consistently achieved better OAR sparing. Overall, an improved tradeoff process between homogeneity and OAR sparing in APP could further enhance its benefits. |
| 184 | Oropharyngeal | The performance of cross‐institutional OVH‐based KBP compared to APP was studied on 25 patients and the plan quality was found to be comparable for both techniques. |
| 185 | Oropharyngeal | APP plans were clinically acceptable and achieved comparable PTV coverage with better OARs sparing |
| 121 | Breast | In a 25 patients’ study, dose homogeneity was found to be significantly better in APP plans compared to manual plans (p < 0.001). |
| 186 | Prostate | In a 23 patients’ study, doses to the PTV and rectum by APP were comparable to manually optimized plans. APP plans achieved lower doses to bladder and femoral heads compared to manual plans (p < 0.05) |
| 187 | Nasopharyngeal | Impact of APP was studied on IMRT and VMAT plans on 10 patients with three dose level target volumes. Better parotid sparing was achieved by APP‐VMAT versus APP‐IMRT (p < 0.01). PTVs coverage was comparable in both techniques. |
| 123 | Head/Neck | APP produced clinically acceptable plans in all 26 cases with better sparing of OARs. APP plans achieved a comparable plan quality score to the previously delivered plans in 94% of the evaluations. |
| 188 | Prostate | In 100 patients’ study, 98 plans met all clinical constraints with significant improvement bladder and rectum sparing in higher dose region (V72 Gy). Proposed automated treatment planning workflow reduced operator time to less than 5 min. |
| 189 | Head/Neck | Script‐based APP plans achieved higher points compared to manually created plans (67.0 vs. 62.3), however, resulted in increased monitor units up to 35.5%. |
| 190 | Whole brain | In a 10 patients’ study, APP‐based 2 coplanar VMAT and 9‐field plans were compared. With comparable dosimetric results, both APP‐based plans achieved clinically acceptable and deliverable plans and eliminated the need of generating pseudo‐structures by the planners. |
| 191 | Breast (Tangential) | Automated planning was found to be applicable in 1661/1708 patients with treatment planning time to be around 5 to 6 minutes on standard commercially available planning system hardware. |
| 192 | Lung SBRT | In a 56 patients’ study, APP plans significantly reduced D2% for the spinal cord, esophagus, heart, aorta, and main stem bronchus and maintained target coverage compared to manually created treatment plans. |
| 193 | Liver SBRT | In a 10 patients’ study, APP plans resulted in comparable to manual plans, but with reduced doses to the spinal cord and planning time. |
| 194 | Prostate | Evaluated the adaptability of APP across clinics with different planning protocols and demonstrated that APP configurations can be shared and implemented across multiple centers. |
| 195 | Partial breast irradiation | In a 23 patients’ study, APP plans were compared with manually created plans. No significant differences in OARs were observed, but APP plans achieved significant improvements in PTV coverage compared to manual plans. |
| 196 | Nasopharyngeal | In a 25 patients’ study, APP and manual plans had similar ratings including PTV coverage and doses to OARs for 19/25 patients. APP plans reduced planning duration time by 17% |
| 197 | Locally advanced Head/Neck | The performance of 1) APP plans 2) RapidArc‐based automatic interactive optimizer 3) RapidPlan 4) RapidPlan with automated setup fields and 5) RayStation multicriteria optimization was studied retrospectively on 16 head/neck cases. All systems generated comparable treatment plans, but APP plans performed the best for parallel organs with minor dose differences. |
Abbreviations: APP, Auto planning by Pinnacle; D2%, Dose received by 2% of the volume; OARs, organs at risk; PTV, planning target volume.
In terms of modality, both (traditional KBP and DL KBP) methods were mostly applied to IMRT, VMAT, and other noncoplanar intensity‐modulated external beam radiation therapy treatments. Only a small number of studies were reported for the purpose of magnetic resonance imaging‐guided therapy (MRgRT).129 The number of traditional KBP and DL‐based publications for on‐table adaptation may increase in the future, owing to recent technical developments such as MR‐Linear Accelerator (MR‐Linac). In terms of treatment sites, prostate, head/neck, and lung were among the most investigated sites in both traditional KBP and DL‐based methods. Other disease sites—complex abdominal or cranial—were studied less often. This trend was anticipated as both KBP techniques require large training sets, and prostate, lung, and head/neck are among the more common and static disease sites treated with external beam radiation therapy. Therefore, the availability of a prior plan is likely to be one of the predictive factors for future model development.
In KBP, three commonly reported dose prediction metrics in the literature are the entire DVH curve (Table 1), one or more dose metrics (Table 2), and voxel‐based dose prediction (Table 3). For DVH only prediction model, DTH of the OARs, volumes of PTV OARs excluding external or body structure, and patient‐specific anatomical information are used as the input to the model, whereas the output is the DVH curve of each OAR (i.e., bladder and rectum). In this case, dose outside of the PTV region may not be accounted for unless body structure is included in the model, which, in turn, would provide information regarding dose conformality or gradient outside the PTV. However, including the body structure in the model has not been a common practice for the DVH‐only prediction model.46 Moreover, the voxel‐based dose prediction model predicts the dose distribution accounting for doses to each voxel within the patient's image set,96, 127 hence provides spatial information including dose gradient outside of the PTV and dose conformality. However, the voxel‐based approach relies heavily on the quality of the plans used to build the model as the inclusion of outliers can compromise the model performance. Even for RapidPlanTM‐based KBP, several studies indicated the need to investigate the proper identification of outlier plans.60, 65, 72 Outlier identification in RapidPlanTM involves statistics and regression plots for each structure, suggesting Cook's Distance >10.0, Studentized Residual >3.0, Areal Difference of Estimate >3, and Modified Z‐score >3.5 as potential outliers.118 To an extent, this also requires removal of outliers in an iterative manner with either stopping the removal once no significant improvement is observed or identification of the outliers followed by the re‐planning of all the outliers so that it can be reused in the training cohort.116 The time required to address the issue of outliers may vary across institutions, as those without standardized contouring and planning techniques may have many dosimetric outliers, which in turn can result in a time‐consuming process of eliminating outliers either through visual inspection or additional statistical analysis. In the literature, there only limited effort toward establishing a systematic process for identifying dosimetric and geometric outliers. To our knowledge, currently, there is no well‐established workflow for outlier identification and mitigation in terms of model creation for both KBP techniques. Therefore, a standardized automated method of outlier identification and model creation could further enhance the treatment planning experience.53
KBP research is growing rapidly. Past work has been surveyed before, though much has changed since then and even old work can be given a new context in light of more recent advancements. In contrast to a previous review that calculated an average number of training and testing dataset used in each year,28 we calculated the average number of training and testing datasets used for each cancer site for traditional KBP and DL KBP in Figures 3 and 6, respectively. Table 5 provides site‐specific training and validation dataset size for the RapidPlanTM KBP module. This could inform readers of a range of training sample size used in the literature for each treatment site. Direct comparison of training sample size between the traditional and DL‐based KBP was not made as DL‐based dose prediction is a relatively new technique with a fewer number of investigations per site compared to traditional KBP methods.
There are key differences between traditional KBP and DL methods for dose prediction. In contrast to DL, an inherent limitation of traditional methods is that it is unable to extract important features and patterns hidden within the raw dataset. Both, similarity measures in atlas‐based methods and input features to model‐based methods require considerable effort to design handcrafted features (i.e., overlap volume histogram, OAR distance to the PTV, projections, etc.) that can be processed either to identify the best‐matched case or into a representation from which patterns within the input can be classified through a classifier. In traditional KBP, PCA has been widely used in the literature for feature selection owing to its simplicity. However, a major limitation of PCA is that it learns a low dimensional representation of data only with a linear projection. Whereas DNNs can be used to address this issue and untangle non‐linear projections. For instance, an autoencoder is a type of neural network that is consisted of encoder, which encodes the input into a low dimensional latent space, and decoder, which restores the original input from the low dimensional latent space.198 DL‐based dose prediction methods use an autoencoder type of neural network as shown in Table 6.
Multiple DL networks have been investigated for dose prediction. The two most widely investigated networks, thus far, included CNN and GAN. From the results so far, it appeared that GANs may be a good choice for dose prediction tasks over conventional CNNs for several reasons. First, GAN has been proven to perform well in lesion detection and data augmentation tasks.148, 199 In addition, GAN does not rely on pure spatial loss, such as mean square error between dose–volumes, which makes it a suitable candidate not only for the dose prediction of conventional radiation therapy but also for SBRT in which dose heterogeneity is prevalent.177 Furthermore, Babier et al. found that GAN models did not require significant parameter tuning and architecture modifications during implementations compared to other conventional methods.148 However, in contrast to CNN, one limitation of conventional GAN is that they are difficult to train and require the number of network parameters to be as low as possible. Future studies are anticipated to account for such shortcomings by proposing the extension of networks such as attention‐gated GAN.24 Finally, Deep RL is one of the least studied networks for generating a treatment plan presumably due to the high action space of the actual treatment planning process. One application of RL in dose prediction would be to adjust treatment planning parameters such as dose–volume objectives, constraints, and corresponding weights to reach the desired treatment plan. However, this would require synchronizing DL framework and inverse optimizer in a single pipeline, which may not be feasible with inverse optimizer of commercial TPS due to its “black box” nature. Therefore, applying RL for generating a treatment plan may require in‐house built TPS 152 that can be presented with DL network architectures in the same pipeline.
4.1. Method comparison of KBP dose predictions
KBP model performance varies as does the geometric and dosimetric complexity of treatment plans for different disease sites. For these reasons, KBP performance is presented here for specific disease sites. For head/neck cancer, the difference between the traditional KBP predicted and actual median doses for the parotids ranged from −17.7% to 15.3%,48 whereas it ranged between – 7.7 and 13.5% for DL‐based dose prediction.133 With the same level of prediction accuracy, DL‐based KBP was able to predict median dose for 80% of parotids compared to 63% by the traditional KBP method.133 Kajikawa et al. made the direct comparison of dose distribution predicted by the DL method with that generated by RapidPlanTM for prostate cancer.141 This dosimetric comparison showed that CNN significantly predicted DVH accurately for D98 in PTV‐2 and V35 V50, V65 in the rectum. Given that features automatically extracted by DL methods can include both geometric/anatomic features and the mutual tradeoffs between the OARs, it gives an edge to DL methods in terms of dose prediction accuracy compared to traditional KBP methods that mainly rely on DVH and geometry‐based expected dose.
For oropharyngeal cancer, Mahmood et al. directly compared the GAN approach for generating predicted dose distribution with several traditional approaches including bagging query 3, 200 and generalized PCA,47 random forest.102 Through the gamma analysis,201 Mahmood et al. demonstrated that GAN plans were the most similar to the clinical plans and achieved 4.0% to 7.6% improvements in the frequency of clinical criteria satisfaction compared to traditional approaches.131
For prostate SBRT, Vasant et al. compared the performance of the proposed attention gated GAN with an earlier approach that used relative distance map information of neighboring input structures.127 In contrast to conventional radiation therapy, SBRT produces hot spots within the target volume. The mean absolute difference in V120 between KBP‐like approach and actual plan was fourfold higher compared to that achieved by the attention gated GAN technique, demonstrating the ability of a DL‐based method to predict cold spots and hotspots that are prevalent in SBRT dose distributions. While both, traditional and DL‐based KBP methods used the data from previously treated patients to make dose prediction for a new patient, DL‐based methods have been shown to outperform several traditional KBP methods as demonstrated by some studies in the literature.131, 141
4.2. Future trends
According to published articles on each KBP method in recent years, a bulk of research on further developments of models has shifted from traditional KBP methods to DL‐based methods. This is presumably due to the recent success of DL in various medical applications as well as its potential in dose prediction task. In terms of traditional KBP methods, future investigations are anticipated to be retrospective in nature by clinically available tools (i.e., RapidPlanTM, APP). Since DL‐based methods appear to be in their initial development stage, their possibilities are expected to be further explored through the development of new DL models and in different areas of dose prediction tasks in treatment planning workflow including adaptive radiotherapy in the near future.
Adaptive radiotherapy (ART) involves adjusting dose distribution based on anatomical changes observed on intra‐procedural imaging such CBCT. The standard approach requires a physician to perform the recontouring of OAR and tumor regions followed by plan re‐optimization, which is difficult to implement with a patient on the table due to time constraints. To date, only one study has been reported to adopt DL methods for the purpose of ART of head/neck cancer.146 The future trend will certainly be toward utilizing DL‐based methods to present dose prediction models of dosimetry changes and radiotherapy response for ART.
Post‐dose prediction, the main component of treatment planning workflow includes ensuring the achievability of the predicted dose plans, which often involves inverse treatment planning through manual intervention. Only a handful of studies extended such KBP in a fully automated pipeline that not only predict the dose distribution but also generates a complete treatment plan with minimum human interaction in traditional 52, 101, 184, 202, 203 and DL‐based methods.131, 148, 151 The accurate deliverability of the predicted plans is crucial and it must account for various mechanical, physical, and algorithmic constraints. It is important to note here that good predictions with the low error may not necessarily lead to the final deliverable plan with the same performance on clinical criteria. For instance, five of the seven prediction methods investigated by Babier et al. resulted in significantly worse clinical criteria satisfaction despite lower error post‐dose predictions.148 We, therefore, believe synchronizing an inverse optimization engine with dose prediction methods hold great potential in improving treatment planning efficacy and efficiency of DL KBP. Alternatively, a DL‐based fluence prediction has also been proposed for real‐time prostate treatment planning.151 This approach follows the conversion of predicted fluence maps to a deliverable treatment plan through delivery parameter generation and dose calculations directly in a treatment planning software. Such approaches do not require an inverse optimization process and involve minimal human intervention. After generating a clinically acceptable plan, a subsequent task in many clinics involves patient‐specific quality assurance (QA) measurements that are performed routinely prior to actual treatment delivery. This QA step is not feasible if adapting a plan for a patient currently on the treatment table. Several ML204 and DL205 approaches have been reported for predicting gamma analysis pass rates for patient‐specific IMRT QA that may prove to be an acceptable surrogate for actual measurements or be an acceptable complement in an overarching QA program. More effort is needed to incorporate such approaches into the treatment planning pipeline to establish a fully automated workflow.
One of the challenges in data‐driven algorithms, including both ML and DL, is that it requires a large set of high‐quality data. Since the quality of data and radiotherapy practices vary from one center to the other, the heterogeneity in previously treated plans becomes a major obstacle in the deployment of data‐driven solutions in the field of radiation oncology. To address this issue, the concept of transfer learning for model adaptation to different learning styles at different centers may be investigated further in the future. A long‐term goal of this area of investigations would be to incorporate data‐driven predictive tools as a part of the clinical pathway. Pooled data from multiple institutions are the likely path forward for creating KBP models for rare disease sites.
Finally, while the emergence of traditional ML and modern DL methods in the form of KBP has had a positive impact in radiotherapy clinics, adopting several practices from computer vision (CV) communities can further contribute to the growth of KBP on a larger scale. Data sharing is one category of CV that focuses on collaborative analysis and publishing on the web.206, 207, 208 Within KBP communities, an exclusive platform may be used to share, combine, and analyze the dataset within the boundaries of HIPAA (Health Insurance Portability and Accountability Act). Through collaborative analysis, individuals from different centers can run KBP models on the dataset from their centers and later merge with other versions of the data available on this platform. Practice of publishing code is another area that the KBP community may adopt from CV as it matures. Availability of codes along with a corresponding paper on web (i.e., paperswithcode.com) aids the reproducibility of research, and provides useful information and details that may not be sufficient to provide in publications (i.e., training strategies, detailed list of hyper‐parameter values, network structure, data augmentation, etc.). Eglen et al. compiled general guidelines from different areas of science for sharing computer codes and programs.209 By advocating for such guidelines, the KBP community may embrace reproducibility, transparency, and reusability of research products.
5. CONCLUSION
In the last decade, a tremendous amount of work has been done to improve treatment plan quality and efficiency through knowledge‐based planning research. We have reviewed over 120 articles covering two major KBP methods for dose prediction: traditional KBP methods and the more recent DL‐based KBP. Many traditional KBP methods are shown to be equivalent or superior to an experienced planner with greater efficiency. Recent developments in DL‐based KBP methods also hold a great potential to further improve the accuracy of the dose prediction task without compromising on efficiency. Both traditional and DL‐based KBP methods need further development for many other disease sites. Given the commercial availability of the traditional KBP module, more retrospectives studies are foreseen in the future. However, new DL‐based KBP methods are actively being introduced and trending in a steep upward direction and its commercialization may be anticipated in near future. There are various areas of future research, several of which have been highlighted in this review, required to achieve an ultimate goal of a fully automated treatment planning system.
CONFLICT OF INTEREST
None.
AUTHOR CONTRIBUTIONS
Shadab Momin: Conceptualization, Methodology, Investigation, Writing ‐ Original Draft, Visualization Yabo Fu: Methodology, Writing ‐ Review and Editing Yang Lei: Methodology, Writing ‐ Review and Editing Justin Roper: Writing ‐ Review and Editing Yang Lei: Writing ‐ Review and Editing Jeffrey D. Bradley: Writing ‐ Review and Editing Walter J. Curran: Writing ‐ Review and Editing, Supervision Tian Liu: Writing ‐ Review and Editing, Supervision Xiaofeng Yang: Conceptualization, Writing ‐ Review and Editing, Supervision, Project administration, Funding acquisition.
ACKNOWLEDGMENTS
This research is supported in part by the National Cancer Institute of the National Institutes of Health under Award Number R01CA215718, the Department of Defense (DoD) Prostate Cancer Research Program (PCRP) Award W81XWH‐17‐1‐0438, and Dunwoody Golf Club Prostate Cancer Research Award, a philanthropic award provided by the Winship Cancer Institute of Emory University.
Momin S, Fu Y, Lei Y, et al. Knowledge‐based radiation treatment planning: A data‐driven method survey. J Appl Clin Med Phys. 2021;22:16–44. 10.1002/acm2.13337
REFERENCES
- 1.Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin. 2018;68:394‐424. [DOI] [PubMed] [Google Scholar]
- 2.Jaffray DA, Gospodarowicz MK. Radiation therapy for cancer. Cancer: Disease Control Priorities. Washington (DC). 2015. [Google Scholar]
- 3.Wu B, Ricchetti F, Sanguineti G, et al. Patient geometry‐driven information retrieval for IMRT treatment plan quality control. Med Phys. 2009;36:5497‐5505. [DOI] [PubMed] [Google Scholar]
- 4.Appenzoller LM, Michalski JM, Thorstad WL, Mutic S, Moore KL. Predicting dose‐volume histograms for organs‐at‐risk in IMRT planning. Med Phys. 2012;39:7446‐7461. [DOI] [PubMed] [Google Scholar]
- 5.Wang T, Lei Y, Tang H, et al. A learning‐based automatic segmentation and quantification method on left ventricle in gated myocardial perfusion SPECT imaging: a feasibility study. J Nucl Cardiol. 2019;3:1‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang T, Manohar N, Lei Y, et al. MRI‐based treatment planning for brain stereotactic radiosurgery: dosimetric validation of a learning‐based pseudo‐CT generation method. Med Dosim. 2019;44:199‐204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wang T, Lei Y, Manohar N, et al. Dosimetric study on learning‐based cone‐beam CT correction in adaptive radiation therapy. Med Dosim. 2019;44:e71‐e79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang T, Ghavidel BB, Beitler JJ, et al. Optimal virtual monoenergetic image in “TwinBeam” dual‐energy CT for organs‐at‐risk delineation based on contrast‐noise‐ratio in head‐and‐neck radiotherapy. J App Clin Med Phys. 2019;20:121‐128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wang B, Lei Y, Tian S, et al. Deeply supervised 3D fully convolutional networks with group dilated convolution for automatic MRI prostate segmentation. Med Phys. 2019;46:1707‐1718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Liu Y, Lei Y, Wang Y, et al. MRI‐based treatment planning for proton radiotherapy: dosimetric validation of a deep learning‐based liver synthetic CT generation method. Phys Med Biol. 2019;64:145015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liu Y, Lei Y, Wang T, et al. MRI‐based treatment planning for liver stereotactic body radiotherapy: validation of a deep learning‐based synthetic CT generation method. Br J Radiol. 2019;92:20190067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lei Y, Harms J, Wang T, et al. MRI‐based synthetic CT generation using semantic random forest with iterative refinement. Phys Med Biol. 2019;64:085001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lei Y, Dong X, Wang T, et al. Whole‐body PET estimation from low count statistics using cycle‐consistent generative adversarial networks. Phys Med Biol. 2019;64:215017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lei Y, Tian S, He X, et al. Ultrasound prostate segmentation based on multidirectional deeply supervised V‐Net. Med Phys. 2019;46:3194‐3206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lei Y, Tang X, Higgins K, et al. Learning‐based CBCT correction using alternating random forest based on auto‐context model. Med Phys. 2019;46:601‐618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lei Y, Harms J, Wang T, et al. MRI‐only based synthetic CT generation using dense cycle consistent generative adversarial networks. Med Phys. 2019;46:3565‐3581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Harms J, Lei Y, Wang T, et al. Paired cycle‐GAN‐based image correction for quantitative cone‐beam computed tomography. Med Phys. 2019;46:3998‐4009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fu Y, Mazur TR, Wu X, et al. A novel MRI segmentation method using CNN‐based correction network for MRI‐guided adaptive radiotherapy. Med Phys. 2018;45:5129‐5137. [DOI] [PubMed] [Google Scholar]
- 19.Dong X, Lei Y, Tian S, et al. Synthetic MRI‐aided multi‐organ segmentation on male pelvic CT using cycle consistent deep attention network. Radiat Oncol. 2019;141:192‐199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dong X, Lei Y, Wang T, et al. Automatic multiorgan segmentation in thorax CT images using U‐net‐GAN. Med Phys. 2019;46:2157‐2168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fu Y, Lei Y, Wang T, et al. Pelvic multi‐organ segmentation on cone‐beam CT for prostate adaptive radiotherapy. Med Phys. 2020;47:3415‐3422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Schmidhuber J. Deep learning in neural networks: an overview. Neur Netw. 2015;61:85‐117. [DOI] [PubMed] [Google Scholar]
- 23.Ronneberger O, Fischer P, Brox T. U‐net: Convolutional networks for biomedical image segmentation. International Conference on Medical image computing and computer‐assisted intervention. Springer; 2015:234‐241. [Google Scholar]
- 24.Vasant K, Chan JW, Tianqi W, et al. DoseGAN: a generative adversarial network for synthetic dose prediction using attention‐gated discrimination and generation. Sci Rep. 2020;10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fan J, Wang J, Chen Z, Hu C, Zhang Z, Hu W. Automatic treatment planning based on three‐dimensional dose distribution predicted from deep learning technique. Med Phys. 2019;46:370‐381. [DOI] [PubMed] [Google Scholar]
- 26.Kearney V, Chan JW, Haaf S, Descovich M, Solberg TD. DoseNet: a volumetric dose prediction algorithm using 3D fully‐convolutional neural networks. Phys Med Biol. 2018;63:235022. [DOI] [PubMed] [Google Scholar]
- 27.Nguyen D, Long T, Jia X, et al. A feasibility study for predicting optimal radiation therapy dose distributions of prostate cancer patients from patient anatomy using deep learning. Sci Rep. 2017;9:1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ge Y, Wu QJ. Knowledge‐based planning for intensity‐modulated radiation therapy: a review of data‐driven approaches. Med Phys. 2019;46:2760‐2775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Moore KL. Automated radiotherapy treatment planning. Semin Radiat Oncol: Elsevier. 2019;209‐218. [DOI] [PubMed] [Google Scholar]
- 30.Breedveld S, Craft D, Van Haveren R, Heijmen B. Multi‐criteria optimization and decision‐making in radiotherapy. Eur Jour Op Res. 2019;277:1‐19. [Google Scholar]
- 31.Hussein M, Heijmen BJ, Verellen D, Nisbet A. Automation in intensity modulated radiotherapy treatment planning—a review of recent innovations. Br J Radiol. 2018;91:20180270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wang M, Zhang Q, Lam S, Cai J, Yang R. A review on application of deep learning algorithms in external beam radiotherapy automated treatment planning. Front Oncol. 2020;10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cornell M, Kaderka R, Hild SJ, et al. Noninferiority study of automated knowledge‐based planning versus human‐driven optimization across multiple disease sites. Int J Radiat Oncol Biol Phys. 2020;106:430‐439. [DOI] [PubMed] [Google Scholar]
- 34.Dumane VA, Tam J, Lo Y‐C, Rosenzweig KE. RapidPlan for knowledge‐based planning of malignant pleural mesothelioma. Pract Radiat Oncol. 2021;11(2):e219‐e228. [DOI] [PubMed] [Google Scholar]
- 35.Giaddui T, Geng H, Chen Q, et al. Offline quality assurance for intensity‐modulated radiotherapy treatment plans for NRG‐HN001 head and neck clinical trial using knowledge‐based planning. Adv Radiat Oncol. 2020;5(6):1342‐1349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kavanaugh JA, Holler S, DeWees TA, et al. Multi‐institutional validation of a knowledge‐based planning model for patients enrolled in RTOG 0617: implications for plan quality controls in cooperative group trials. Pract Radiat Oncol. 2019;9:e218‐e227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Yu G, Li Y, Feng Z, et al. Knowledge‐based IMRT planning for individual liver cancer patients using a novel specific model. Radiat Oncol. 2018;13:52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ueda Y, Miyazaki M, Sumida I, et al. Knowledge‐based planning for oesophageal cancers using a model trained with plans from a different treatment planning system. Acta Oncol. 2020;59:274‐283. [DOI] [PubMed] [Google Scholar]
- 39.Chatterjee A, Serban M, Faria S, Souhami L, Cury F, Seuntjens J. Novel knowledge‐based treatment planning model for hypofractionated radiotherapy of prostate cancer patients. Phys Med. 2020;69:36‐43. [DOI] [PubMed] [Google Scholar]
- 40.Huang Y, Li S, Yue H, et al. Impact of nominal photon energies on normal tissue sparing in knowledge‐based radiotherapy treatment planning for rectal cancer patients. PLoS One. 2019;14:e0213271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Scaggion A, Fusella M, Roggio A, et al. Reducing inter‐and intra‐planner variability in radiotherapy plan output with a commercial knowledge‐based planning solution. Phys Med. 2018;53:86‐93. [DOI] [PubMed] [Google Scholar]
- 42.Delaney AR, Dahele M, Tol JP, Kuijper IT, Slotman BJ, Verbakel WF. Using a knowledge‐based planning solution to select patients for proton therapy. Radiother Oncol. 2017;124:263‐270. [DOI] [PubMed] [Google Scholar]
- 43.Kamima T, Ueda Y, Fukunaga J‐I, et al. Multi‐institutional evaluation of knowledge‐based planning performance of volumetric modulated arc therapy (VMAT) for head and neck cancer. Phys Med. 2019;64:174‐181. [DOI] [PubMed] [Google Scholar]
- 44.Shepherd M, Bromley R, Stevens M, et al. Developing knowledge‐based planning for gynaecological and rectal cancers: a clinical validation of RapidPlan™. J Med Rad Sci. 2020;67:217‐224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Smith A, Granatowicz A, Stoltenberg C, et al. Can the student outperform the master? A plan comparison between pinnacle auto‐planning and eclipse knowledge‐based rapidplan following a prostate‐bed plan competition. Tech Can Res Treat. 2019;18:153303381985176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Zhu X, Ge Y, Li T, Thongphiew D, Yin FF, Wu QJ. A planning quality evaluation tool for prostate adaptive IMRT based on machine learning. Med Phys. 2011;38:719‐726. [DOI] [PubMed] [Google Scholar]
- 47.Yuan L, Ge Y, Lee WR, Yin FF, Kirkpatrick JP, Wu QJ. Quantitative analysis of the factors which affect the interpatient organ‐at‐risk dose sparing variation in IMRT plans. Med Phys. 2012;39:6868‐6878. [DOI] [PubMed] [Google Scholar]
- 48.Lian J, Yuan L, Ge Y, et al. Modeling the dosimetry of organ‐at‐risk in head and neck IMRT planning: an intertechnique and interinstitutional study. Med Phys. 2013;40:121704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Yuan L, Wu QJ, Yin FF, Jiang Y, Yoo D, Ge Y. Incorporating single‐side sparing in models for predicting parotid dose sparing in head and neck IMRT. Med Phys. 2014;41:021728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Zarepisheh M, Long T, Li N, et al. A DVH‐guided IMRT optimization algorithm for automatic treatment planning and adaptive radiotherapy replanning. Med Phys. 2014;41:061711. [DOI] [PubMed] [Google Scholar]
- 51.Deshpande RR, DeMarco J, Sayre JW, Liu BJ. Knowledge‐driven decision support for assessing dose distributions in radiation therapy of head and neck cancer. Int J Comp Ass Radiol. 2016;11:2071‐2083. [DOI] [PubMed] [Google Scholar]
- 52.Fan J, Wang J, Zhang Z, Hu W. Iterative dataset optimization in automated planning: Implementation for breast and rectal cancer radiotherapy. Med Phys. 2017;44:2515‐2531. [DOI] [PubMed] [Google Scholar]
- 53.Zhang J, Wu QJ, Xie T, Sheng Y, Yin F‐F, Ge Y. An ensemble approach to knowledge‐based intensity‐modulated radiation therapy planning. Front Oncol. 2018;8:57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Zhang J, Ge Y, Sheng Y, Yin FF, Wu QJ. Modeling of multiple planning target volumes for head and neck treatments in knowledge‐based treatment planning. Med Phys. 2019;46:3812‐3822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Cagni E, Botti A, Micera R, et al. Knowledge‐based treatment planning: an inter‐technique and inter‐system feasibility study for prostate cancer. Phys Med. 2017;36:38‐45. [DOI] [PubMed] [Google Scholar]
- 56.Chang AT, Hung AW, Cheung FW, et al. Comparison of planning quality and efficiency between conventional and knowledge‐based algorithms in nasopharyngeal cancer patients using intensity modulated radiation therapy. Int J Radiat Oncol Biol Phys. 2016;95:981‐990. [DOI] [PubMed] [Google Scholar]
- 57.Chatterjee A, Serban M, Abdulkarim B, et al. Performance of knowledge‐based radiation therapy planning for the glioblastoma disease site. Int J Radiat Oncol Biol Phys. 2017;99:1021‐1028. [DOI] [PubMed] [Google Scholar]
- 58.Chin Snyder K, Kim J, Reding A, et al. Development and evaluation of a clinical model for lung cancer patients using stereotactic body radiotherapy (SBRT) within a knowledge‐based algorithm for treatment planning. J App Clin Med Phys. 2016;17:263‐275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Fogliata A, Nicolini G, Clivio A, et al. A broad scope knowledge based model for optimization of VMAT in esophageal cancer: validation and assessment of plan quality among different treatment centers. Radiother Oncol. 2015;10:220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Fogliata A, Wang P‐M, Belosi F, et al. Assessment of a model based optimization engine for volumetric modulated arc therapy for patients with advanced hepatocellular cancer. Radiat Oncol. 2014;9:236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Foy JJ, Marsh R, Ten Haken RK, et al. An analysis of knowledge‐based planning for stereotactic body radiation therapy of the spine. Pract Radiat Oncol. 2017;7:e355‐e360. [DOI] [PubMed] [Google Scholar]
- 62.Hussein M, South CP, Barry MA, et al. Clinical validation and benchmarking of knowledge‐based IMRT and VMAT treatment planning in pelvic anatomy. Radiother Oncol. 2016;120:473‐479. [DOI] [PubMed] [Google Scholar]
- 63.Schubert C, Waletzko O, Weiss C, et al. Intercenter validation of a knowledge based model for automated planning of volumetric modulated arc therapy for prostate cancer. The experience of the German RapidPlan Consortium. PLoS One. 2017;12(5):e0178034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Tol JP, Dahele M, Delaney AR, Slotman BJ, Verbakel WF. Can knowledge‐based DVH predictions be used for automated, individualized quality assurance of radiotherapy treatment plans? Radiat Oncol. 2015;10:1‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Tol JP, Delaney AR, Dahele M, Slotman BJ, Verbakel WF. Evaluation of a knowledge‐based planning solution for head and neck cancer. Int J Radiat Oncol Biol Phys. 2015;91:612‐620. [DOI] [PubMed] [Google Scholar]
- 66.Ueda Y, Fukunaga J‐I, Kamima T, Adachi Y, Nakamatsu K, Monzen H. Evaluation of multiple institutions’ models for knowledge‐based planning of volumetric modulated arc therapy (VMAT) for prostate cancer. Radiat Oncol. 2018;13:46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Wu H, Jiang F, Yue H, Li S, Zhang Y. A dosimetric evaluation of knowledge‐based VMAT planning with simultaneous integrated boosting for rectal cancer patients. J App Clin Med Phys. 2016;17:78‐85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Younge KC, Marsh RB, Owen D, et al. Improving quality and consistency in NRG Oncology Radiation Therapy Oncology Group 0631 for spine radiosurgery via knowledge‐based planning. Int J Radiat Oncol Biol Phys. 2018;100:1067‐1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Wang Y, Heijmen BJ, Petit SF. Knowledge‐based dose prediction models for head and neck cancer are strongly affected by interorgan dependency and dataset inconsistency. Med Phys. 2019;46:934‐943. [DOI] [PubMed] [Google Scholar]
- 70.Delaney AR, Tol JP, Dahele M, Cuijpers J, Slotman BJ, Verbakel WF. Effect of dosimetric outliers on the performance of a commercial knowledge‐based planning solution. Int J Radiat Oncol Biol Phys. 2016;94:469‐477. [DOI] [PubMed] [Google Scholar]
- 71.Masi K, Archer P, Jackson W, et al. Knowledge‐based treatment planning and its potential role in the transition between treatment planning systems. Med Dosim. 2018;43:251‐257. [DOI] [PubMed] [Google Scholar]
- 72.Fogliata A, Belosi F, Clivio A, et al. On the pre‐clinical validation of a commercial model‐based optimisation engine: application to volumetric modulated arc therapy for patients with lung or prostate cancer. Radiother Oncol. 2014;113:385‐391. [DOI] [PubMed] [Google Scholar]
- 73.Fogliata A, Nicolini G, Bourgier C, et al. Performance of a knowledge‐based model for optimization of volumetric modulated arc therapy plans for single and bilateral breast irradiation. PLoS One. 2015;10:e0145137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Fogliata A, Reggiori G, Stravato A, et al. RapidPlan head and neck model: the objectives and possible clinical benefit. Radiat Oncol. 2017;12:73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kubo K, Monzen H, Ishii K, et al. Dosimetric comparison of RapidPlan and manually optimized plans in volumetric modulated arc therapy for prostate cancer. Phys Med. 2017;44:199‐204. [DOI] [PubMed] [Google Scholar]
- 76.Li N, Carmona R, Sirak I, et al. Highly efficient training, refinement, and validation of a knowledge‐based planning quality‐control system for radiation therapy clinical trials. Int J Radiat Oncol Biol Phys. 2017;97:164‐172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Tran A, Woods K, Nguyen D, et al. Predicting liver SBRT eligibility and plan quality for VMAT and 4π plans. Radiat Oncol. 2017;12:1‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Wang M, Li S, Huang Y, et al. An interactive plan and model evolution method for knowledge‐based pelvic VMAT planning. J App Clin Med Phys. 2018;19:491‐498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Zhang HH, Meyer RR, Shi L, D'Souza WD. The minimum knowledge base for predicting organ‐at‐risk dose–volume levels and plan‐related complications in IMRT planning. Phys Med Biol. 2010;55(7):1935‐1947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Mishra N, Petrovic S, Sundar S. A self‐adaptive case‐based reasoning system for dose planning in prostate cancer radiotherapy. Med Phys. 2011;38:6528‐6538. [DOI] [PubMed] [Google Scholar]
- 81.Wu B, Ricchetti F, Sanguineti G, et al. Data‐driven approach to generating achievable dose–volume histogram objectives in intensity‐modulated radiotherapy planning. Int J Radiat Oncol Biol Phys. 2011;79:1241‐1247. [DOI] [PubMed] [Google Scholar]
- 82.Wu B, McNutt T, Zahurak M, et al. Fully automated simultaneous integrated boosted–intensity modulated radiation therapy treatment planning is feasible for head‐and‐neck cancer: a prospective clinical study. Int J Radiat Oncol Biol Phys. 2012;84:e647‐e653. [DOI] [PubMed] [Google Scholar]
- 83.Wang Y, Zolnay A, Incrocci L, et al. A quality control model that uses PTV‐rectal distances to predict the lowest achievable rectum dose, improves IMRT planning for patients with prostate cancer. Radiother Oncol. 2013;107:352‐357. [DOI] [PubMed] [Google Scholar]
- 84.Wu B, Pang D, Simari P, Taylor R, Sanguineti G, McNutt T. Using overlap volume histogram and IMRT plan data to guide and automate VMAT planning: a head‐and‐neck case study. Med Phys. 2013;40:021714. [DOI] [PubMed] [Google Scholar]
- 85.Yang Y, Ford EC, Wu B, et al. An overlap‐volume‐histogram based method for rectal dose prediction and automated treatment planning in the external beam prostate radiotherapy following hydrogel injection. Med Phys. 2013;40:011709. [DOI] [PubMed] [Google Scholar]
- 86.Wang J, Jin X, Zhao K, et al. Patient feature based dosimetric Pareto front prediction in esophageal cancer radiotherapy. Med Phys. 2015;42:1005‐1011. [DOI] [PubMed] [Google Scholar]
- 87.Cooper BT, Li X, Shin SM, et al. Preplanning prediction of the left anterior descending artery maximum dose based on patient, dosimetric, and treatment planning parameters. Adv Radiat Oncol. 2016;1:373‐381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Kuo L, Yorke ED, Dumane VA, et al. Geometric dose prediction model for hemithoracic intensity‐modulated radiation therapy in mesothelioma patients with two intact lungs. J App Clin Med Phys. 2016;17:371‐379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Powis R, Bird A, Brennan M, et al. Clinical implementation of a knowledge based planning tool for prostate VMAT. Radiat Oncol. 2017;12:1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Millunchick CH, Zhen H, Redler G, Liao Y, Turian JV. A model for predicting the dose to the parotid glands based on their relative overlapping with planning target volumes during helical radiotherapy. J App Clin Med Phys. 2018;19:48‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Wall PD, Carver RL, Fontenot JD. An improved distance‐to‐dose correlation for predicting bladder and rectum dose‐volumes in knowledge‐based VMAT planning for prostate cancer. Phys Med Biol. 2018;63:015035. [DOI] [PubMed] [Google Scholar]
- 92.Chanyavanich V, Das SK, Lee WR, Lo JY. Knowledge‐based IMRT treatment planning for prostate cancer. Med Phys. 2011;38:2515‐2522. [DOI] [PubMed] [Google Scholar]
- 93.Good D, Lo J, Lee WR, Wu QJ, Yin F‐F, Das SK. A knowledge‐based approach to improving and homogenizing intensity modulated radiation therapy planning quality among treatment centers: an example application to prostate cancer planning. Int J Radiat Oncol Biol Phys. 2013;87:176‐181. [DOI] [PubMed] [Google Scholar]
- 94.Nwankwo O, Sihono DSK, Schneider F, Wenz F. A global quality assurance system for personalized radiation therapy treatment planning for the prostate (or other sites). Phys Med Biol. 2014;59:5575. [DOI] [PubMed] [Google Scholar]
- 95.Nwankwo O, Mekdash H, Sihono DSK, Wenz F, Glatting G. Knowledge‐based radiation therapy (KBRT) treatment planning versus planning by experts: validation of a KBRT algorithm for prostate cancer treatment planning. Radiat Oncol. 2015;10:111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Liu J, Wu QJ, Kirkpatrick JP, Yin F‐F, Yuan L, Ge Y. From active shape model to active optical flow model: a shape‐based approach to predicting voxel‐level dose distributions in spine SBRT. Phys Med Biol. 2015;60:N83. [DOI] [PubMed] [Google Scholar]
- 97.Schmidt M, Lo JY, Grzetic S, Lutzky C, Brizel DM, Das SK. Semiautomated head‐and‐neck IMRT planning using dose warping and scaling to robustly adapt plans in a knowledge database containing potentially suboptimal plans. Med Phys. 2015;42:4428‐4434. [DOI] [PubMed] [Google Scholar]
- 98.Schreibmann E, Fox T, Curran W, Shu HK, Crocker I. Automated population‐based planning for whole brain radiation therapy. J App Clin Med Phys. 2015;16:76‐86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Sheng Y, Li T, Zhang Y, et al. Atlas‐guided prostate intensity modulated radiation therapy (IMRT) planning. Phys Med Biol. 2015;60:7277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.McIntosh C, Purdie TG. Contextual atlas regression forests: multiple‐atlas‐based automated dose prediction in radiation therapy. IEEE Trans Med Imag. 2015;35:1000‐1012. [DOI] [PubMed] [Google Scholar]
- 101.McIntosh C, Purdie TG. Voxel‐based dose prediction with multi‐patient atlas selection for automated radiotherapy treatment planning. Phys Med Biol. 2016;62:415. [DOI] [PubMed] [Google Scholar]
- 102.McIntosh C, Welch M, McNiven A, Jaffray DA, Purdie TG. Fully automated treatment planning for head and neck radiotherapy using a voxel‐based dose prediction and dose mimicking method. Phys Med Biol. 2017;62:5926. [DOI] [PubMed] [Google Scholar]
- 103.Owen J‐A. Principal component analysis: data reduction and simplification. Mc Schol Res Journ. 2014;1:2. [Google Scholar]
- 104.Faught AM, Olsen L, Schubert L, et al. Functional‐guided radiotherapy using knowledge‐based planning. Radiother Oncol. 2018;129:494‐498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Li N, Noticewala SS, Williamson CW, et al. Feasibility of atlas‐based active bone marrow sparing intensity modulated radiation therapy for cervical cancer. Radiother Oncol. 2017;123:325‐330. [DOI] [PubMed] [Google Scholar]
- 106.Wang J, Hu W, Yang Z, et al. Is it possible for knowledge‐based planning to improve intensity modulated radiation therapy plan quality for planners with different planning experiences in left‐sided breast cancer patients? Radiat Oncol. 2017;12:85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Hunt MA, Jackson A, Narayana A, Lee N. Geometric factors influencing dosimetric sparing of the parotid glands using IMRT. Int J Radiat Oncol Biol Phys. 2006;66:296‐304. [DOI] [PubMed] [Google Scholar]
- 108.Kazhdan M, Simari P, McNutt T, et al. A shape relationship descriptor for radiation therapy planning. International Conference on Medical Image Computing and Computer‐Assisted Intervention. Springer; 2009:100‐108. [DOI] [PubMed] [Google Scholar]
- 109.Moore KL, Brame RS, Low DA, Mutic S. Experience‐based quality control of clinical intensity‐modulated radiotherapy planning. Int J Radiat Oncol Biol Phys. 2011;81:545‐551. [DOI] [PubMed] [Google Scholar]
- 110.Landers A, Neph R, Scalzo F, Ruan D, Sheng K. Performance comparison of knowledge‐based dose prediction techniques based on limited patient data. Tech Can Res Treat. 2018;17:1533033818811150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Petit SF, Wu B, Kazhdan M, et al. Increased organ sparing using shape‐based treatment plan optimization for intensity modulated radiation therapy of pancreatic adenocarcinoma. Radiother Oncol. 2012;102:38‐44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Wang Y, Breedveld S, Heijmen B, Petit SF. Evaluation of plan quality assurance models for prostate cancer patients based on fully automatically generated Pareto‐optimal treatment plans. Phys Med Biol. 2016;61:4268. [DOI] [PubMed] [Google Scholar]
- 113.Wu B, Pang D, Lei S, et al. Improved robotic stereotactic body radiation therapy plan quality and planning efficacy for organ‐confined prostate cancer utilizing overlap‐volume histogram‐driven planning methodology. Radiother Oncol. 2014;112:221‐226. [DOI] [PubMed] [Google Scholar]
- 114.Zhang J, Ge Y, Sheng Y, et al. Knowledge‐based tradeoff hyperplanes for head and neck treatment planning. Int J Radiat Oncol Biol Phys. 2020;106(5):1095‐1103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Sheng Y, Ge Y, Yuan L, Li T, Yin FF, Wu QJ. Outlier identification in radiation therapy knowledge‐based planning: a study of pelvic cases. Med Phys. 2017;44:5617‐5626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Alpuche Aviles JE, Cordero Marcos MI, Sasaki D, Sutherland K, Kane B, Kuusela E. Creation of knowledge‐based planning models intended for large scale distribution: minimizing the effect of outlier plans. J App Clin Med Phys. 2018;19:215‐226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Wu H, Jiang F, Yue H, Zhang H, Wang K, Zhang Y. Applying a RapidPlan model trained on a technique and orientation to another: a feasibility and dosimetric evaluation. Radiat Oncol. 2016;11:108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.VMS . Eclipse Photon and Electron 13.6 Instruction of Use. Palo Alto, CA: Varian Medical Systems, Inc. 2015. [Google Scholar]
- 119.Boutilier JJ, Craig T, Sharpe MB, Chan TC. Sample size requirements for knowledge‐based treatment planning. Med Phys. 2016;43:1212‐1221. [DOI] [PubMed] [Google Scholar]
- 120.Hansen CR, Bertelsen A, Hazell I, et al. Automatic treatment planning improves the clinical quality of head and neck cancer treatment plans. J Clin Trans Rad Oncol. 2016;1:2‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Liu F‐Y, Dong Z‐W, Yang H‐B, Shi H‐Y. Evaluation of the clinical application of Auto‐Planning module for IMRT plans of left breast cancer. Rad Phys Chem. 2020;166:108500. [Google Scholar]
- 122.Janssen TM, Kusters M, Wang Y, et al. Independent knowledge‐based treatment planning QA to audit Pinnacle autoplanning. Radiother Oncol. 2019;133:198‐204. [DOI] [PubMed] [Google Scholar]
- 123.Hazell I, Bzdusek K, Kumar P, et al. Automatic planning of head and neck treatment plans. J App Clin Med Phys. 2016;17:272‐282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Gintz D, Latifi K, Caudell J, et al. Initial evaluation of automated treatment planning software. J App Clin Med Phys. 2016;17:331‐346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.LeCun Y, Bengio Y, Hinton G. Deep learning. Nat. 2015;521:436‐444. [DOI] [PubMed] [Google Scholar]
- 126.LeCun Y, Bengio Y. Convolutional networks for images, speech, and time series. Han Br Neur Net. 1995;3361:1995. [Google Scholar]
- 127.Shiraishi S, Moore KL. Knowledge‐based prediction of three‐dimensional dose distributions for external beam radiotherapy. Med Phys. 2016;43:378‐387. [DOI] [PubMed] [Google Scholar]
- 128.Campbell WG, Miften M, Olsen L, et al. Neural network dose models for knowledge‐based planning in pancreatic SBRT. Med Phys. 2017;44:6148‐6158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Thomas MA, Fu Y, Yang D. Development and evaluation of machine learning models for voxel dose predictions in online adaptive magnetic resonance guided radiation therapy. J App Clin Med Phys. 2020;21(7):60‐69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Liu Z, Fan J, Li M, et al. A deep learning method for prediction of three‐dimensional dose distribution of helical tomotherapy. Med Phys. 2019;46:1972‐1983. [DOI] [PubMed] [Google Scholar]
- 131.Mahmood R, Babier A, McNiven A, Diamant A, Chan TC. Automated treatment planning in radiation therapy using generative adversarial networks. In Machine Learning for Healthcare Conference. 2018:484‐499.
- 132.Barragán‐Montero AM, Nguyen D, Lu W, et al. Three‐dimensional dose prediction for lung IMRT patients with deep neural networks: robust learning from heterogeneous beam configurations. Med Phys. 2019;46:3679‐3691. [DOI] [PubMed] [Google Scholar]
- 133.Chen X, Men K, Li Y, Yi J, Dai J. A feasibility study on an automated method to generate patient‐specific dose distributions for radiotherapy using deep learning. Med Phys. 2019;46:56‐64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Lee MS, Hwang D, Kim JH, Lee JS. Deep‐dose: a voxel dose estimation method using deep convolutional neural network for personalized internal dosimetry. Sci Rep. 2019;9:1‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Nguyen D, Jia X, Sher D, et al. 3D radiotherapy dose prediction on head and neck cancer patients with a hierarchically densely connected U‐net deep learning architecture. Phys Med Biol. 2019;64:065020. [DOI] [PubMed] [Google Scholar]
- 136.Willems S, Crijns W, Sterpin E, Haustermans K, Maes F. Feasibility of CT‐Only 3D Dose Prediction for VMAT Prostate Plans Using Deep Learning. Cham: Springer International Publishing; 2019:10‐17. [Google Scholar]
- 137.Ma J, Bai T, Nguyen D, et al. Individualized 3D dose distribution prediction using deep learning. Workshop on Artificial Intelligence in Radiation Therapy. Springer; 2019:110‐118. [Google Scholar]
- 138.Bohara G, Sadeghnejad Barkousaraie A, Jiang S, Nguyen D. Using deep learning to predict beam‐tunable pareto optimal dose distribution for intensity modulated radiation therapy. Med Phys. 2020;47(9):3898‐3912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Fan J, Xing L, Dong P, Wang J, Hu W, Yang Y. Data‐driven dose calculation algorithm based on deep learning. arXiv preprint arXiv:2006.15485. 2020. [DOI] [PMC free article] [PubMed]
- 140.Götz TI, Schmidkonz C, Chen S, Al‐Baddai S, Kuwert T, Lang E. A deep learning approach to radiation dose estimation. Phys Med Biol. 2020;65:035007. [DOI] [PubMed] [Google Scholar]
- 141.Kajikawa T, Kadoya N, Ito K, et al. A convolutional neural network approach for IMRT dose distribution prediction in prostate cancer patients. J Radiat Res. 2019;60:685‐693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Murakami Y, Magome T, Matsumoto K, Sato T, Yoshioka Y, Oguchi M. Fully automated dose prediction using generative adversarial networks in prostate cancer patients. PLoS One. 2020;15:e0232697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Song Y, Hu J, Liu Y, et al. Dose prediction using a deep neural network for accelerated planning of rectal cancer radiotherapy. Radiother Oncol. 2020;149:111‐116. [DOI] [PubMed] [Google Scholar]
- 144.Sumida I, Magome T, Das IJ, et al. A convolution neural network for higher resolution dose prediction in prostate volumetric modulated arc therapy. Phys Med. 2020;72:88‐95. [DOI] [PubMed] [Google Scholar]
- 145.Xing Y, Nguyen D, Lu W, Yang M, Jiang S. A feasibility study on deep learning‐based radiotherapy dose calculation. Med Phys. 2020;47:753‐758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Svecic A, Roberge D, Kadoury S. Prediction of inter‐fractional radiotherapy dose plans with domain translation in spatiotemporal embeddings. Med Imag Anal. 2020;64:101728. [DOI] [PubMed] [Google Scholar]
- 147.Nguyen D, McBeth R, Sadeghnejad Barkousaraie A, et al. Incorporating human and learned domain knowledge into training deep neural networks: A differentiable dose‐volume histogram and adversarial inspired framework for generating Pareto optimal dose distributions in radiation therapy. Med Phys. 2020;47:837‐849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Babier A, Mahmood R, McNiven AL, Diamant A, Chan TC. Knowledge‐based automated planning with three‐dimensional generative adversarial networks. Med Phys. 2020;47:297‐306. [DOI] [PubMed] [Google Scholar]
- 149.Zhou J, Peng Z, Song Y, et al. A method of using deep learning to predict three‐dimensional dose distributions for intensity‐modulated radiotherapy of rectal cancer. J App Clin Med Phys. 2020;21(5):26‐37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Kandalan RN, Nguyen D, Rezaeian NH, et al. Dose prediction with deep learning for prostate cancer radiation therapy: model adaptation to different treatment planning practices. Radiotherapy Oncol. 2020;153:228‐235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Li X, Zhang J, Sheng Y, et al. Automatic IMRT planning via static field fluence prediction (AIP‐SFFP): a deep learning algorithm for real‐time prostate treatment planning. Phys Med Biol. 2020;65(17):175014. [DOI] [PubMed] [Google Scholar]
- 152.Shen C, Nguyen D, Chen L, et al. Operating a treatment planning system using a deep‐reinforcement learning‐based virtual treatment planner for prostate cancer intensity‐modulated radiation therapy treatment planning. Med Phys. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Lee C‐Y, Gallagher PW, Tu Z. Generalizing pooling functions in convolutional neural networks: Mixed, gated, and tree. Artificial Intelligence and Statistics; 2016:464‐472. [Google Scholar]
- 154.He K, Zhang X, Ren S, Sun J. Spatial pyramid pooling in deep convolutional networks for visual recognition. IEEE Trans Pat Anal Mach Intel. 2015;37:1904‐1916. [DOI] [PubMed] [Google Scholar]
- 155.Wang T, Wu DJ, Coates A, Ng AY. End‐to‐end text recognition with convolutional neural networks. Proceedings of the 21st international conference on pattern recognition (ICPR2012). IEEE; 2012:3304‐3308. [Google Scholar]
- 156.Gu J, Wang Z, Kuen J, et al. Recent advances in convolutional neural networks. Pattern Recognit. 2018;77:354‐377. [Google Scholar]
- 157.Ramachandran P, Zoph B, Le QV. Searching for activation functions. arXiv preprint arXiv:1710.05941. 2017.
- 158.Xu B, Wang N, Chen T, Li M. Empirical evaluation of rectified activations in convolutional network. arXiv preprint arXiv:1505.00853. 2015.
- 159.LeCun YA, Bottou L, Orr GB, Müller K‐R. Efficient backprop. Neural networks: Tricks of the trade. Springer; 2012:9‐48. [Google Scholar]
- 160.Mish MD. A self regularized non‐monotonic neural activation function. arXiv preprint arXiv:1908.08681. 2019.
- 161.Nwankpa C, Ijomah W, Gachagan A, Marshall S. Activation functions: comparison of trends in practice and research for deep learning. arXiv preprint arXiv:1811.03378. 2018.
- 162.Szegedy C, Liu W, Jia Y, et al. Going deeper with convolutions. Proceedings of the IEEE conference on computer vision and pattern recognition; 2015:1‐9. [Google Scholar]
- 163.Shen C, Nguyen D, Zhou Z, Jiang SB, Dong B, Jia X. An introduction to deep learning in medical physics: advantages, potential, and challenges. Phys Med Biol. 2020;65:05TR1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Srivastava N, Hinton G, Krizhevsky A, Sutskever I, Salakhutdinov R. Dropout: a simple way to prevent neural networks from overfitting. J Mach Learn Res. 2014;15:1929‐1958. [Google Scholar]
- 165.Shorten C, Khoshgoftaar TM. A survey on image data augmentation for deep learning. J Big Data. 2019;6:1‐48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Janocha K, Czarnecki WM. On loss functions for deep neural networks in classification. arXiv preprint arXiv:1702.05659. 2017.
- 167.He K, Zhang X, Ren S, Sun J. Deep residual learning for image recognition. Proceedings of the IEEE conference on computer vision and pattern recognition. 2016:770; ‐778. [Google Scholar]
- 168.Huang G, Liu Z, Van Der Maaten L, Weinberger KQ. Densely connected convolutional networks. Proceedings of the IEEE conference on computer vision and pattern recognition; 2017:4700‐4708. [Google Scholar]
- 169.Schlemper J, Oktay O, Schaap M, et al. Attention gated networks: Learning to leverage salient regions in medical images. Med Imag Anal. 2019;53:197‐207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170.He K, Zhang X, Ren S, Sun J. Deep residual learning for image recognition. Proceedings of the IEEE conference on computer vision and pattern recognition; 2016:770‐778. [Google Scholar]
- 171.Milletari F, Navab N, Ahmadi S‐A. V‐net: Fully convolutional neural networks for volumetric medical image segmentation. 2016 fourth international conference on 3D vision (3DV). IEEE; 2016:565‐571. [Google Scholar]
- 172.Goodfellow I, Pouget‐Abadie J, Mirza M, et al. Generative adversarial nets. Advances in neural information processing systems; 2014:2672‐2680. [Google Scholar]
- 173.Zhu J‐Y, Park T, Isola P, Efros AA. Unpaired image‐to‐image translation using cycle‐consistent adversarial networks. Proceedings of the IEEE international conference on computer vision; 2017:2223‐2232. [Google Scholar]
- 174.Mirza M, Osindero S. Conditional generative adversarial nets. arXiv preprint arXiv:1411.1784. 2014.
- 175.Choi Y, Choi M, Kim M, Ha J‐W, Kim S, Choo J. Stargan: Unified generative adversarial networks for multi‐domain image‐to‐image translation. Proceedings of the IEEE conference on computer vision and pattern recognition; 2018:8789‐8797. [Google Scholar]
- 176.Jiang J, Hu YC, Tyagi N, et al. Cross‐modality (CT‐MRI) prior augmented deep learning for robust lung tumor segmentation from small MR datasets. Med Phys. 2019;46:4392‐4404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Momin S, Lei Y, Wang T, et al. Radiation dose prediction for pancreatic stereotactic body radiotherapy via convention neural networks. Medical Imaging 2021: Image‐Guided Procedures, Robotic Interventions, and Modeling. International Society for Optics and Photonics; 2021:1159823. [Google Scholar]
- 178.Isola P, Zhu J‐Y, Zhou T, Efros AA. Image‐to‐image translation with conditional adversarial networks. Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition; 2017:1125‐1134. [Google Scholar]
- 179.Mnih V, Kavukcuoglu K, Silver D, et al. Human‐level control through deep reinforcement learning. Nat. 2015;518:529‐533. [DOI] [PubMed] [Google Scholar]
- 180.Shen C, Chen L, Gonzalez Y, Jia X. Improving efficiency of training a virtual treatment planner network via knowledge‐guided deep reinforcement learning for intelligent automatic treatment planning of radiotherapy. Med Phys. 2021;48:1909‐1920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Maier J, Berker Y, Sawall S, Kachelrieß M. Deep scatter estimation (DSE): feasibility of using a deep convolutional neural network for real‐time x‐ray scatter prediction in cone‐beam CT. Medical Imaging 2018: Physics of Medical Imaging. International Society for Optics and Photonics; 2018:105731L. [Google Scholar]
- 182.Venkatesh G, Nurvitadhi E, Marr D. Accelerating deep convolutional networks using low‐precision and sparsity. 2017 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP). IEEE; 2017:2861‐2865. [Google Scholar]
- 183.Hansen CR, Nielsen M, Bertelsen AS, et al. Automatic treatment planning facilitates fast generation of high‐quality treatment plans for esophageal cancer. Acta Oncol. 2017;56:1495‐1500. [DOI] [PubMed] [Google Scholar]
- 184.Wu B, Kusters M, Kunze‐Busch M, et al. Cross‐institutional knowledge‐based planning (KBP) implementation and its performance comparison to Auto‐Planning Engine (APE). Radiother Oncol. 2017;123:57‐62. [DOI] [PubMed] [Google Scholar]
- 185.Kusters J, Bzdusek K, Kumar P, et al. Automated IMRT planning in Pinnacle. Strahlen und Onkol. 2017;193:1031‐1038. [DOI] [PubMed] [Google Scholar]
- 186.Nawa K, Haga A, Nomoto A, et al. Evaluation of a commercial automatic treatment planning system for prostate cancers. Med Dosim. 2017;42:203‐209. [DOI] [PubMed] [Google Scholar]
- 187.Boylan C, Rowbottom C. A bias‐free, automated planning tool for technique comparison in radiotherapy‐application to nasopharyngeal carcinoma treatments. J App Clin Med Phys. 2014;15:213‐225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188.Winkel D, Bol GH, Van Asselen B, et al. Development and clinical introduction of automated radiotherapy treatment planning for prostate cancer. Phys Med Biol. 2016;61:8587. [DOI] [PubMed] [Google Scholar]
- 189.Speer S, Klein A, Kober L, Weiss A, Yohannes I, Bert C. Automation of radiation treatment planning. Strahlen un Onkol. 2017;193:656‐665. [DOI] [PubMed] [Google Scholar]
- 190.Wang S, Zheng D, Zhang C, et al. Automatic planning on hippocampal avoidance whole‐brain radiotherapy. Med Dosim. 2017;42:63‐68. [DOI] [PubMed] [Google Scholar]
- 191.Purdie TG, Dinniwell RE, Fyles A, Sharpe MB. Automation and intensity modulated radiation therapy for individualized high‐quality tangent breast treatment plans. Int J Radiat Oncol Biol Phys. 2014;90:688‐695. [DOI] [PubMed] [Google Scholar]
- 192.Vanderstraeten B, Goddeeris B, Vandecasteele K, Van Eijkeren M, De Wagter C, Lievens Y. Automated instead of manual treatment planning? A plan comparison based on dose‐volume statistics and clinical preference. Int J Radiat Oncol Biol Phys. 2018;102:443‐450. [DOI] [PubMed] [Google Scholar]
- 193.Gallio E, Giglioli FR, Girardi A, et al. Evaluation of a commercial automatic treatment planning system for liver stereotactic body radiation therapy treatments. Phys Med. 2018;46:153‐159. [DOI] [PubMed] [Google Scholar]
- 194.Roach D, Wortel G, Ochoa C, et al. Adapting automated treatment planning configurations across international centres for prostate radiotherapy. Phys Imag Radiat Oncol. 2019;10:7‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 195.Marrazzo L, Meattini I, Arilli C, et al. Auto‐planning for VMAT accelerated partial breast irradiation. Radiot Oncol. 2019;132:85‐92. [DOI] [PubMed] [Google Scholar]
- 196.Bai P, Weng X, Quan K, et al. A knowledge‐based intensity‐modulated radiation therapy treatment planning technique for locally advanced nasopharyngeal carcinoma radiotherapy. Radiat Oncol. 2020;15:1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 197.Krayenbuehl J, Zamburlini M, Ghandour S, et al. Planning comparison of five automated treatment planning solutions for locally advanced head and neck cancer. Radiat Oncol. 2018;13:1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198.Fu Y, Lei Y, Wang T, Curran WJ, Liu T, Yang X. Deep learning in medical image registration: a review. Phys Med Biol. 2020;65(20):20TR01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199.Frid‐Adar M, Diamant I, Klang E, Amitai M, Goldberger J, Greenspan H. GAN‐based synthetic medical image augmentation for increased CNN performance in liver lesion classification. Neurocomp. 2018;321:321‐331. [Google Scholar]
- 200.Babier A, Boutilier JJ, McNiven AL, Chan TC. Knowledge‐based automated planning for oropharyngeal cancer. Med Phys. 2018;45:2875‐2883. [DOI] [PubMed] [Google Scholar]
- 201.Low DA, Harms WB, Mutic S, Purdy JA. A technique for the quantitative evaluation of dose distributions. Med Phys. 1998;25:656‐661. [DOI] [PubMed] [Google Scholar]
- 202.Kaderka R, Mundt RC, Li N, et al. Automated closed‐and open‐loop validation of knowledge‐based planning routines across multiple disease sites. Pract Radiat Oncol. 2019;9:257‐265. [DOI] [PubMed] [Google Scholar]
- 203.Ziemer BP, Sanghvi P, Hattangadi‐Gluth J, Moore KL. Heuristic knowledge‐based planning for single‐isocenter stereotactic radiosurgery to multiple brain metastases. Med Phys. 2017;44:5001‐5009. [DOI] [PubMed] [Google Scholar]
- 204.Lam D, Zhang X, Li H, et al. Predicting gamma passing rates for portal dosimetry‐based IMRT QA using machine learning. Med Phys. 2019;46:4666‐4675. [DOI] [PubMed] [Google Scholar]
- 205.Nyflot MJ, Thammasorn P, Wootton LS, Ford EC, Chaovalitwongse WA. Deep learning for patient‐specific quality assurance: Identifying errors in radiotherapy delivery by radiomic analysis of gamma images with convolutional neural networks. Med Phys. 2019;46:456‐464. [DOI] [PubMed] [Google Scholar]
- 206.Bhardwaj A, Bhattacherjee S, Chavan A, et al. Datahub: collaborative data science & dataset version management at scale. arXiv preprint arXiv:1409.0798. 2014.
- 207.Bhardwaj A, Karger D, Subramanyam H, et al. Collaborative data analytics with DataHub. Proceedings of the VLDB Endowment International Conference on Very Large Data Bases. NIH Public Access; 2015:1916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 208.Halevy AY. Data publishing and sharing using fusion tables. CIDR. 2013.
- 209.Eglen SJ, Marwick B, Halchenko YO, et al. Toward standard practices for sharing computer code and programs in neuroscience. Nat Neurosci. 2017;20:770‐773. [DOI] [PMC free article] [PubMed] [Google Scholar]