

Abstract
Hereditary hearing loss accounts for nearly 60% of deafness in developed countries and about 30% of them are syndromic. Pierre Robin Syndrome is one such condition. The patient with this syndrome usually presnts with triad of micrognathia, glossoptosis and cleft palate. Hearing loss is mostly conductive but there can be sensorineural hearing loss also. Here we present a case of Pierre Robin Syndrome who presented with congenital hearing loss. He also had bilateral serous otitis media. He underwent cochlear implant surgery and was prescribed antihistaminics and steroid spray for middle ear effusion. Therefore, proper clinical evaluation is required.
Keywords: Pierre robin syndrome, Congenital hearing loss, Middle ear effusion, Cochlear implantation
Introduction
Hereditary hearing loss accounts for nearly 60% of deafness in developed countries and 30% of them are syndromic that present with other abnormalities along with deafness. More than 400 syndromes are being reported in various literature which include various degrees of hearing impairment with different phenotypes [1, 2]. Abnormalities include different systems along with syndromic hearing loss. They include craniofacial malformations, dental abnormalities, ocular abnormalities, renal defects, cardiac abnormalities, endocrine dysfunction, neurologic dysfunction, skeletal abnormalities, integumentary abnormalities, metabolic disease, chromosomal abnormalities.
Pierre Robin condition is better defined as “sequence” instead of “syndrome”.
because of the common origin that give rise to main clinical features. There is mandibular hypoplasia which become evident in the first period of gestation and due to which there is anomalous position of the tongue. Therefore, the proper development of the palate is affected. At the time of birth, the newborn presents with micrognathia, glossoptosis and cleft palate. As a result, there are respiratory, feeding and swallowing problems problems in these patients [3].
With an estimated prevalence of about 1/10.000 Pierre Robin sequence is generally sporadic. Familial transmission has been reported in about 10% cases.
Although Robin sequence occur due to a SOX9 gene mutation [4], but can present along with other syndromes in about half of cases (e.g : 22q11.2 deletion syndrome and Stickler) [3]. The brain is normal.
Here we present a case of Pierre Robin sequence who had undergone cochlear implantation surgery for congenital hearing loss.
Case
A four year old male patient presented to ENT department of SMS Medical College, Jaipur with chief complaints of congenital hearing loss and speech delay. Patient had undergone surgery for cleft palate. He also had micrognathia. On otoscopy, patient had bilateral serous otitis media. Audiological assessment was done. On BERA, Vth peak was not tracable even at 100 dB in both ears. OAE showed bilateral non-functional outer hair cells i.e. " refer" type. Tympanometry showed B type with absent stapedial reflexes in both ears. Bone conduction ABR showed no waves even at 100 dB. High resolution computed tomography showed serous otitis media in the right ear (Fig. 1).
Fig. 1.

High resolution computed tomography of temporal bone showing serous otitis media in the right ear (arrow)
The patient was given fluticasone furoate nasal spray and levocetrizine for one month. There was significant improvement in otoscopy findings. Patient was taken up for cochlear implant after hearing aid trial did not show any improvement. Surgery was planned. Anesthetic clearance was taken. Surgery was done by transmastoid facial recess approach. There were granulations in middle ear cleft and edematous middle ear mucosa, which were cleared (Fig. 2). Adrenaline and dexamethasone soaked gelfoam were kept in the middle ear to reduce the edema and help in identifying the landmarks. Cochleostomy done by extended round window approach. Finally, implant was placed in the well and electrodes inserted through cochleostomy site in the scala tympani of cochlea. Flap was repositioned and wound closed in layers.
Fig. 2.
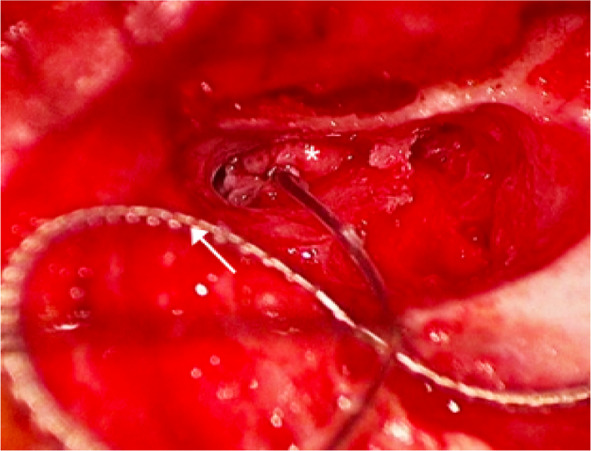
Edematous middle ear mucosa(*) with cochlear implant placed via posterior tympanotomy (arrow)
Post-operatively, the patient was prescribed fluticasone furoate nasal spray for a month.
Discussion
In cases of Pierre Robin triad, hearing loss is typically conductive and bilateral. Patients with Pierre Robin sequence present with middle ear effusion as the most common finding. Therefore the mainstay of treatment remains the use of tympanostomy (ventilation) tubes in these patient. In a study conducted by Handzic et al. [5] the mean hearing loss at speech frequencies was 24.5 dB. Patients with Pierre Robin sequence can also present with sensorineural hearing loss. In a study conducted by Medard et al. [6], about 30% patients of Pierre Robin sequence had congenital permanent sensorineural hearing loss.
Middle ear pathologies are the most common, with conductive hearing loss occurring due to eustachian tube dysfunction secondary to a cleft palate. This can lead to middle ear effusions, chronic otitis media, retraction pockets and cholesteatoma [5, 7]. Middle ear ossicular chain can also be affected and have anomalies like abnormal stapes footplate and ankylosis of the incus and malleus [8]. In our case, there was congested middle ear mucosa present along with granulations. In view of middle ear involvement, evaluation should include bone conduction ABR. Routine air conduction ABR would not be able to truly diagnose sensorineural hearing loss. Decision-making also involves treatment of serous otitis media with medicines or grommet insertion. In patients with extensive disease, subtotal petrosectomy with cul de sac closure of the external auditory canal is a good option. In rare cases, the surgery may need to abandoned.
Inner ear abnormalities such as hypoplastic cochlea, dysplastic vestibule along with anomalous facial nerve have also been reported in various studies [8, 9]. Here in our patient also, the facial nerve was found to be anomalous. Also there was risk of facial nerve injury as the landmarks were not clearly visible due to inflamed middle ear mucosa.
Conlusion
Pierre Robin Sequence is a triad of micrognathia, glossoptosis and cleft palate. Patients can present with both conductive and sensorineural hearing loss. Therefore, proper clinical evaluation is required. In patients with congenital hearing loss, one can also for cochlear implantation surgery as one of the option.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Barlow-Stewart K, Mona Sale (2007) Centre for genetics education. Deafness and hearing loss–genetic aspects. The Australasian genetics Resource Book.
- 2.Berrettini S (2008) Linee guida per la conduzione dello screening audiologico neonatale nella regione Toscana http://www.fimp.org
- 3.Evans KN, Sie KC, Hopper RA, Glass RP, Hing AV, Cunningham ML. Robin sequence: from diagnosis to development of an effective management plan. Pediatr. 2011;127(5):936–948. doi: 10.1542/peds.2010-2615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Breugem CC, Evans KN, Poets CF, Suri S, Picard A, Filip C, et al. Best practices for the diagnosis and evaluation of infants with robin sequence: a clinical consensus report. JAMA Pediatr. 2016;170:894–902. doi: 10.1001/jamapediatrics.2016.0796. [DOI] [PubMed] [Google Scholar]
- 5.Handzić J, Bagatin M, Subotić R, Cuk V. Hearing levels in pierre robin syndrome. Cleft Palate Craniofac J. 1995;32(1):30–36. doi: 10.1597/1545-1569_1995_032_0030_hliprs_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 6.Medard C, François M, Narcy P. Hearing status of robin sequence patients. Ann Otolaryngol Chir Cervicofac. 1999;116(6):317–321. [PubMed] [Google Scholar]
- 7.Sando I, Takahashi H. Otitis media in association with various congenital diseases; preliminary study. Ann Otol Rhinol Laryngol. 1990;99:13–16. doi: 10.1177/00034894900990S605. [DOI] [PubMed] [Google Scholar]
- 8.Gruen PM, Carranza A, Karmody CS, Bachor E. Anomalies of the ear in the pierre robin triad. Ann Otol Rhinol Laryngol. 2005;114(8):605–613. doi: 10.1177/000348940511400805. [DOI] [PubMed] [Google Scholar]
- 9.Igarashi M, Filippone MV, Alford BR. Temporal bone findings in pierre robin`. Laryngoscope. 1976;86:1679–1687. doi: 10.1288/00005537-197611000-00009. [DOI] [PubMed] [Google Scholar]