

Abstract
Anxiogenic settings lead to reduced postural sway while standing, but anxiety-related balance may be influenced by the location of postural threat in the environment. We predicted that the direction of threat would elicit a parallel controlled manifold relative to the standing surface, and an orthogonal uncontrolled manifold during standing. Altogether, 14 healthy participants (8 women, mean age = 27.5 years, SD = 8.2) wore a virtual reality (VR) headset and stood on a matched real-world walkway (2 m × 40 cm × 2 cm) for 30 s at ground level and simulated heights (elevated 15 m) in two positions: (1) parallel to walkway, lateral threat; and (2) perpendicular to walkway, anteroposterior threat. Inertial sensors measured postural sway acceleration (e.g., 95% ellipse, root mean square (RMS) of acceleration), and a wrist-worn monitor measured heart rate coefficient of variation (HR CV). Fully factorial linear-mixed effect regressions (LMER) determined the effects of height and position. HR CV moderately increased from low to high height (p = 0.050, g = 0.397). The Height × Position interaction approached significance for sway area (95% ellipse; β = −0.018, p = 0.062) and was significant for RMS (β = −0.022, p = 0.007). Post-hoc analyses revealed that sagittal plane sway accelerations and RMS increased from low to high elevation in parallel standing, but were limited when facing the threat during perpendicular standing. Postural response to threat varies depending on the direction of threat, suggesting that the control strategies used during standing are sensitive to the direction of threat.
Keywords: Anxiety, Sway, Fear of falling, Heart rate, Motor control, Virtual reality
Introduction
The anxiogenic effects of standing at high elevation are well documented. In addition to increased physiological arousal and levels of worry, anxiety is associated with decreased variability of postural sway, increased power–frequency of center of pressure oscillations, and a posterior trunk lean-away from the direction of threat (Adkin et al. 2000; Carpenter et al. 2001; Brown et al. 2006; Adkin and Carpenter 2018; Wuehr et al. 2019). Published reports on balance control derived from threatening scenarios (i.e., elevated heights) consistently demonstrate that reductions in anteroposterior (A/P) sway tend to be greater than mediolateral (M/L) sway (Adkin and Carpenter 2018). Yet, it remains unclear if this effect is a function of the direction of postural threat, the motor constraints of the task, or biomechanical control of posture based on underlying musculature (Gendre et al. 2016; Adkin and Carpenter 2018).
According to contemporary theories of motor control, the spatial characteristics of the environment and the task goals are important for configuring postural control strategies and subsequent balance control outcomes (Latash et al. 2010). Yet, researchers have traditionally induced anxiety with a postural threat that is imposed by positioning participants at the edge of an elevated platform (Carpenter et al. 1999; Adkin et al. 2000; Cleworth et al. 2012, 2016; Zaback et al. 2016; Martens et al. 2019; Wuehr et al. 2019; Johnson et al. 2019), or asking individuals to walk along a narrow, elevated beam (e.g., Boroomand-Tehrani et al. 2019; Ehgoetz Martens et al. 2015; Peterson et al. 2018), where the threat is presented either perpendicular or parallel relative to the participant. The configurations of postural threat in relation to the participant could affect the goals of a motor task and how balance is controlled. The context of postural threat is known to affect balance control when anxious, illustrated by changes in response to the direction of impending physical balance perturbations, but this effect is typically eliminated with multi-directional perturbations (Adkin and Carpenter 2018; Johnson et al. 2019). It remains unknown if the spatial context of postural threat in relation to an individual represents an important constraint on motor control strategies during standing balance. We present a novel attempt to rectify this gap in the literature.
The Uncontrolled Manifold Theory (UMT) states that the goal and spatial properties of a task determines how individuals manage redundant degrees of freedom (Latash et al. 2010). The UMT has since been expanded upon and integrated into the framework of several modern theories of motor control based on similar tenets, such as Goal Equivalent Manifold (Latash et al. 2010; Cusumano and Dingwell 2013). These theories suggest that during standing, a likely goal is simply to maintain upright posture and prevent a fall, and this is achieved through countless combinations of joint moments and muscle activation patterns that balance the center of mass (COM) in an inverted pendulum configuration (Scholz and Schöner 1999). Such theories of motor control propose that ‘controlled’ movement during quiet standing represents motion within a space where postural control characteristics resist internal and external perturbations (Latash et al. 2010). Orthogonal to this state-space would be ‘uncontrolled’ movement, or the uncontrolled manifold (UCM), a space where the majority of variance in movement configurations occurs and does not disrupt the goal of the task (Latash et al. 2010). Accordingly, the dimensions of the support surface within an environment could act to prevent a fall or support upright posture while standing and should play a role in postural variability (Scholz and Schöner 1999). For example, the presence of a support surface allows for a recovery step in the event that the COM moves beyond the base of support (BOS). In such a case, COM movement along the support surface has lower risk than COM movement perpendicular to the support surface; a recovery step is a feasible option to prevent a fall in the former, but not in the latter. Consequently, fluctuation of the COM aligned with the direction of the support surface may be conceptualized as the UCM.
The principles of modern theories of motor control suggest that the direction of the postural threat shapes anxiety-related postural responses based on the spatial constraints of the environment and overall goals of the balance control task. We extend the tenets of modern theories of motor control, including UMT, to understand if imposing a postural threat may affect a person’s assessment of risk, and as a result, participants may ‘reweight’ their goal of preventing a fall by prioritizing not falling towards the threat (Fig. 1). The influence of anxiety on the control priorities of the task, or its interaction with the direction of the threat, has not yet been observed because when researchers examine the impact of anxiety during standing they typically place participants in one orientation relative to the threat (Adkin and Carpenter 2018), or control for a directional effect with multi-directional postural threats (Johnson et al. 2019). We hypothesize that when facing a postural threat, forward postural fluctuations become highly controlled to avoid perturbation, and a UCM exists orthogonal to that space (Fig. 1c). Similarly, when a threat to posture (i.e., fall risk) is lateral to the individual, the M/L direction of postural accelerations becomes controlled to avoid the threat (i.e., reduction in lateral sway) (Fig. 1b). In the same vein, when the threat is lateral to the participant, postural accelerations in the A/P direction would represent a UCM that is dependent on the direction of postural threat, or where posture can fluctuate without a perceived risk of external perturbation (Fig. 1b). However, to our knowledge, this effect has not yet been directly tested.
Figure 1.

The theoretical framework of the present investigation. Grey shapes represent potential postural sway configuration in situations where no postural threat is present (a.) as compared to the scenarios where a postural threat is presented in the sagittal plane (b.) or the frontal plane (c.). We propose a controlled manifold (red double-arrow) exists in response to the direction of postural threat (red arrows) that could facilitate a potential uncontrolled manifold in the orthogonal direction (green line).
In the present study, we extended the principles of UMT, and similar theories of motor control, and manipulated the constraints of the environment (and the presumptive UCM) through the direction of postural threat to examine if anxiety-induced balance responses are sensitive to spatial properties of the environment. Using immersive virtual reality (VR), we presented a postural threat in different orientations (i.e., direction relative to the participant) while participants stood quietly with feet together at simulated low (ground level) and high elevations (15 m above ground). Participants stood at each height in the middle of a 2-m walkway oriented in two positions: (1) parallel to the walkway (i.e., threat presented laterally); and (2) perpendicular to the walkway (i.e., threat presented anterior/posteriorly) (Fig. 1). Postural acceleration data (95% Ellipse Sway Area and RMS acceleration) were measured to reflect spatial characteristics and the magnitude of fluctuations in postural control, and heart rate (HR) variability indicated anxiety-responses. We have previously demonstrated that self-reported measures of cognitive and somatic anxiety, as well as balance confidence, are sensitive to virtual elevation (Raffegeau et al. 2020), so we expected physiological indices of anxiety (i.e., HR variability) to increase when participants stood at simulated high elevation. In line with the tenets of UMT (Scholz and Schöner 1999; Latash et al. 2010), we predicted that the direction of postural threat would dictate the direction of postural responses. Specifically, standing parallel to the walkway (lateral threat) would result in less postural sway in the M/L direction, or the ‘controlled manifold,’ and a UCM would be exhibited in the orthogonal A/P direction along the walkway (Fig. 1b). Conversely, standing perpendicular to the walkway (facing the threat) would result in restricted acceleration of postural sway in the A/P direction, representing the controlled manifold, and increased fluctuation in the M/L direction due to the presence of the UCM in the orthogonal direction (Fig. 1c).
Methods
Participants
All procedures were approved by the University of Utah Institutional Review Board. Participants provided informed consent before commencing the experiment in accordance with ethical standards of the Declaration of Helsinki. Altogether, 14 healthy young adults (8 women, mean (standard deviation) age = 27.50 (8.16) years, height = 1.72 (0.18) m, mass = 75.44 (17.63) kg) participated. Participants were excluded for any known neurological, orthopedic, or cardiovascular conditions that would affect walking, or require assistance during walking. Participants were excluded if they self-reported discomfort during walking, excessive motion sickness, or vertigo. Participants reported normal or corrected vision and hearing and were able to walk unassisted without discomfort.
Procedures
The experimental procedures were part of a larger study that investigated the feasibility of inducing anxiety during locomotor behavior in VR (Raffegeau et al. 2020). Participants wore their usual corrective eyewear and were fitted with an HTC Vive (version 1.0, Bellevue, WA, USA)1 head-mounted display (HMD) presenting a 0.40 m × 2.2 m virtual path in two immersive environments: (1) ground level (low elevation); and (2) at 15 m above ground (high elevation) to induce anxiety. A real-world path (0.02 m high × 0.40 m wide × 2.20 m long) matched the VR path dimensions and location in the virtual simulation (Fig. 2a, d). The VR program used a custom-rendered environment (Unity Technologies, San Francisco, CA, USA) which was designed to mimic a local outdoor setting (program available upon request, or for open access information see Raffegeau et al. 2020). The location and dimensions of the virtual path were captured using hand controllers that marked the four corners of the actual walkway. Participants wore motion trackers (HTC Vive, version 2.0)1 on both ankles to provide a continuous representation of their feet in the virtual environment that was depicted as a pair of tennis shoes. Foot tracker position and rotation were recorded at 90 Hz using gyroscopes and two lighthouse-based infrared sensors1 to track each object. Postural sway was assessed using inertial sensors (APDM Inc, Portland, OR, USA) containing tri-axial accelerometers, gyroscopes, and magnetometers placed on the lumbar spine and both feet, which sampled at 128 Hz. A wrist-worn heart rate monitor (Polar M430, Kempele, Finland) recorded heart rate at 1 Hz.
Figure 2a-f.

Participant orientation in relation to the walkway in Parallel (left, a-c) versus Perpendicular (right, d-f) conditions. Left: Image of participant standing on real-world path in the Parallel (a.) orientation. View of Parallel foot position in the center of the walkway at ground level (b.) and at high elevation (c.) in the Parallel position. Right: Image of participant standing in Perpendicular (d.) orientation. View of Perpendicular foot position on walkway at ground level (e.) and at high elevation (f.).
Before beginning the experimental tasks, adjustments were made to the inter-pupillary distance of the HMD and participants underwent a familiarization period. First, participants were guided through an adjustment of the inter-pupillary distance of the HMD display so that they could see the center of the VR environment clearly, and the motion trackers were aligned to their feet in the virtual space. Next, during a 2-min familiarization period, participants were encouraged to traverse along the walkway in the low elevation environment (Fig. 2b, e) to gain a sense of where they were in the immersive environment in relation to the matched real-world walkway. The familiarization period was used to ensure the accuracy of the visual walkway representation in the HMD and integrity of the foot tracking. If the participant reported that their feet or the walkway were not shown accurately in the virtual setting due to poor motion tracking, the base stations were adjusted, or plank coordinates and foot trackers were recalibrated until participants reported that the virtual environment matched their perceptions of the walkway and their feet. A research assistant followed participants at all times to ensure safety.
Participants were subsequently given verbal instructions about the protocol and an opportunity to ask questions before beginning the experimental trials. One end of the walkway was designated as the ‘beginning’ where the participant stepped onto the platform and were later positioned for walking trials. For each standing trial, participants were instructed to stand quietly in the middle of the walkway for 30 s with their feet together, arms at their sides, looking straight ahead (Fig. 2). Participants completed the quiet standing task in two orientations: (1) parallel, facing forward so the walkway was parallel in relation to the participant’s anatomical sagittal plane (Fig. 2d-f); and (2) perpendicular, facing the side of the walkway so the path was perpendicular to the participant’s anatomical sagittal plane (Fig. 2d, e). For consistency between manipulations, participants stood at the designated ‘beginning’ of the walkway to be instantaneously (i.e., 100 ms) ‘transported’ 15 m above ground, and with support from a trained research assistant they then walked to the middle of the path and assumed the parallel standing position. Participants were instructed to stand quietly without speaking, and to keep their head up and eyes straight ahead. The trial time and data recording began once they verbally confirmed they were ready to begin. In total, participants completed four tasks in the following order: (1) low elevation, parallel orientation (low-parallel); (2) low elevation, perpendicular orientation (low-perpendicular); (3) high elevation, parallel orientation (high-parallel); and (4) high elevation, perpendicular orientation (high-perpendicular).
Data analysis
Validated measures of postural control (Mancini et al. 2012) were derived from Moveo Mobility Lab software (version 1.0, APDM Inc, Portland, OR, USA). We selected 95% ellipse of postural acceleration sway area (sway area, minor axis, major axis) and the root mean square (RMS: total sway, frontal plane, sagittal) of postural accelerations to represent characteristics of postural control. Postural sway area indicates the total and linear planes in which the majority of postural accelerations occur, representing the range of corrections to stability of the COM in space, where perfect stability would result in accelerations equal to zero in all three planes of motion. The RMS of sway accelerations reflect the magnitude of variability of postural fluctuation, or the extent of COM corrections in space. For ellipse measures, the minor axis was defined as the shortest radius of the best fit 95% confidence interval ellipse to postural sway accelerations, and the major axis was the longest radius of the best fitting 95% ellipse for postural sway. The orientation of the axes was determined by the ellipse rotation angle, which dictates the degrees the major axis is oriented counterclockwise. Therefore, we first report the ellipse rotation angles to better interpret the directions of postural sway along the major and minor axes. For data visualization, raw data at the lumbar sensor were first filtered using a fourth order zero-lag Butterworth filter at 6 Hz, and sensor coordinates were aligned with respect to the gravitational vector (Moe-Nilssen 1998).
Physiological and postural outcomes were compared in a series of linear mixed-effect regression (LMER) models. We compared measures of HR and HR CV across low and high heights to support the efficacy of the height illusion and included fixed effects of Height (Low (reference condition), High) and random-effects to account for the within-participant manipulation. Separate models compared 95% ellipse and RMS measures of postural sway with fixed-effects of Height (Low (reference condition), High) and Position (Parallel (reference condition), Perpendicular), and random-effects to account for the within-participant manipulations. We conducted statistical analyses using R and the lme4 package (Bates et al. 2015; R Core Team 2019). We consider results statistically significant as p < 0.05. To better understand the findings, effect sizes were computed for post hoc comparisons of interest, standardized by the average group standard deviation and corrected for small sample size using Hedge’s g (Hedges 1981; Cumming 2012). We considered corrected effect sizes small at 0.20, medium at 0.50, and large at 0.80 (Cohen 1988). To support our a priori hypotheses, we report the unstandardized beta weight (β) or slope based on fixed factors (i.e., Parallel vs. Perpendicular), for the interaction term (Height × Position), significance level (p), and corrected effect size (Hedge’s g).
Results
Physiological responses
We lost HR recordings for two participants due to technical difficulties, thus 12 participants were included in the analysis of HR and HR CV. The LMER indicated that there was no significant effect of Height on HR (β = 1.558, p = 0.185, g = 0.094), neither was there a statistically significant effect of Height on HR CV (β = 1.010, p = 0.050, g = 0.397). Thus, HR was not reliably influenced by Height (Fig. 3a) and while we cannot rule out a non-zero effect on HR CV with 95% confidence, the data generally suggest that HR CV increased at higher elevations, with a moderately large increase observed in the sample (Fig. 3b).
Figure 3a-b.
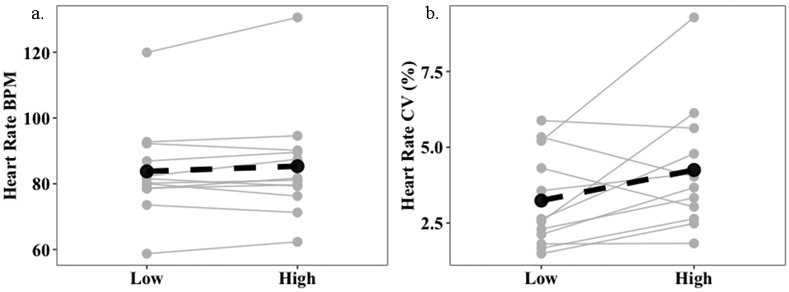
The changes in average heart rate (BPM: beats per minute) (a.) and the heart rate variability (CV: coefficient of variation) (b.) in response to the height illusion. Data points represent mean values for each participant at Low and High elevation (x-axis) in both standing positions. Black points represent mean values and dashed line shows the slope of the change in means from low to high elevation.
Postural control responses
When standing in the Parallel position at high compared to low elevations, participants exhibited a UCM in the ‘safe’ A/P direction. Conversely, participants exhibited a general restriction of sway, or ‘stiffening’, in all directions in the Perpendicular position from low to high heights. We present data from an exemplar participant in Fig. 4.
Figure 4.

A stabilogram representing postural accelerations for one participant. Black circles represent 95% ellipse fit of postural accelerations. The horizontal axis represents the M/L direction and the vertical axis represents the A/P direction. In Low-Parallel, participants demonstrated a larger and wider range of accelerations. In High-Parallel, sway acceleration becomes sharply oriented in the sagittal plane, along the walkway. In Perpendicular condition, participants tended to reduce overall accelerations (reduction in ML sway acceleration shown here), despite the ML direction aligning with the walkway.
95% Ellipse of postural accelerations
The LMER comparing 95% ellipse of overall postural sway acceleration showed that the Position × Height interaction was not statistically significant (β = −0.018, p = 0.062; Fig. 5a). However, it is worth noting that in the sample participants restricted overall postural sway accelerations in the Perpendicular condition at High, as compared to Low, elevations (Mean (SD): Perpendicular-Low = 0.063 (0.03) m2/s4, Perpendicular-High = 0.049 (0.04) m2/s4, g = 0.391) but negligibly increased accelerations in the parallel position from low to high elevation (Mean (SD): Parallel-Low = 0.055 (0.03) m2/s4, Parallel-High = 0.060 (0.04) m2/s4, g = −0.122).
Figure 5a-c.

The 95% ellipse of postural sway area (a.), the minor axis of the ellipse representing motion in the approximate M/L direction (b.), and the major axis of the ellipse representing motion in the approximate A/P direction (c.).
The minor and major axes of the 95% ellipse of postural sway accelerations were oriented in the same manner for all conditions; the major axis of the ellipse was oriented counterclockwise from the M/L axis approximately 90° in each condition. In the Parallel condition, standing at a low elevation oriented the postural acceleration ellipse 85° away from the M/L axis and standing at a high elevation oriented the major axis 91° away from M/L, on average. In the Perpendicular position, standing at a low elevation oriented the long axis of the sway acceleration ellipse 90° away from the M/L axis, and standing at a high elevation oriented the major axis 87° away from M/L, on average. We can therefore approximate that the minor axis of the 95% ellipse represents postural sway acceleration in the frontal plane (Fig. 5b), and the major axis represents sway acceleration in the approximate sagittal plane (Fig. 5c).
For the minor axis, in this case postural sway in the frontal plane, participants in this sample reduced frontal sway accelerations in both positions at high elevations. The LMER comparing differences in the minor axes did not reveal a statistically significant position × height interaction (β = −0.004, p = 0.669) (Fig. 5b). However, at a descriptive level, participants in our sample reduced frontal plane postural sway in both the Perpendicular position (Mean (SD): Perpendicular-Low = 0.097 (0.03) m/s2, Perpendicular-High = 0.079 (0.05) m/s2, g = 0.418) and the Parallel position (Parallel-Low = 0.091 (0.03) m/s2, Parallel-High = 0.076 (0.04) m/s2, g = 0.354) from low to high elevations.
The major axis, representing postural accelerations in the sagittal plane, was largest in the Parallel position at high elevations (Fig. 5c). The LMER comparing the major axis revealed a significant Height × Position interaction (β = −0.057, p = 0.003). Follow-up tests and medium to large effect sizes supported an effect of Height that was specific to the Parallel condition, where participants increased sway within the sagittal plane from low to high heights (β = 0.044, p = 0.060, g = −0.572) on average. The opposite occurred in the Perpendicular position, where participants slightly decreased sagittal sway (β = −0.013, p = 0.366, g = 0.232) from low to high elevation. Note that although the simple effect of Height was not statistically significant in either position, the simple effects of Height were in opposite directions, which led to the significant Height × Position interaction.
RMS of postural accelerations
When we compared RMS sway in the frontal plane from low to high heights, participants in this sample limited RMS sway in the Perpendicular, but not Parallel, position (Fig. 6a). The LMER analyzing RMS sway in the frontal plane did not detect a significant Height × Position interaction (β = −0.006, p = 0.236). Participants moderately reduced frontal RMS sway in the Perpendicular position from low to high elevations (Mean (SD): Perpendicular-Low = 0.043 (0.01) m/s2, Perpendicular-High = 0.034 (0.02) m/s2, g = 0.435), and to a lesser extent in the Parallel position in our sample (Mean (SD): Parallel-Low = 0.040 (0.01) m/s2, Parallel-High = 0.037 (0.02) m/s2, g = 0.140).
Figure 6a-b.

The RMS of postural sway accelerations in the frontal plane (a.), and in the sagittal plane (b.). Asterisk indicates statistically significant differences (p < 0.05) between low and high elevation within conditions.
In the sagittal plane, RMS sway increased substantially from low to high elevation in the Parallel position but was restricted in the Perpendicular condition (Fig. 6b). The LMER analyzing RMS Sway in the sagittal plane revealed a significant Height × Position interaction (β = −0.022, p = 0.003). The interaction showed that in the Parallel position, RMS Sway in the sagittal plane was moderately increased from low to high heights (β = 0.017, p = 0.060, g = −0.542), where sagittal plane RMS sway slightly decreased in the Perpendicular Position upon elevating to high height (β = −0.005, p = 0.388, g = 0.227). The effect of Height was not statistically significant in either condition, but we detected opposing effects from the perpendicular to parallel conditions.
Discussion
We examined the effect of the direction of postural threat on postural control strategies by manipulating the threat in relation to the participant and support surface. We expected that presenting the threat laterally (i.e., parallel orientation) would restrict M/L motion at high elevation, and the presence of the walkway would facilitate a UCM, represented as postural sway and greater variability in the A/P direction. Similarly, we expected that participants would restrict forward motion at high elevation when facing the threat in the perpendicular orientation, and the presence of the walkway in the lateral direction would facilitate a UCM, represented as postural sway and greater variability in the M/L direction.
Our findings partially agreed with our hypotheses. Participants expressed a UCM when positioned parallel to the threat by increasing overall sway acceleration and variability from low to high heights, and aligning fluctuations in postural sway with the walkway (i.e. in the A/P direction) at high elevations. Conversely, the findings were inconclusive when participants faced the threat in the perpendicular orientation. Participants exhibited an overall restriction of sway acceleration and variability at high compared to low heights; but reductions in sway did not align with the direction of threat and were primarily in the ML direction. While the change in A/P sway acceleration and variability between heights was not significant in the perpendicular orientation, the Height × Position interactions supported that the effect of height on A/P sway reliably differed according to the direction of threat. Thus, a UCM in the M/L plane was not expressed in the perpendicular position, but our overall results supported the influence of threat direction on balance control when standing at elevation.
In this study, participants redefined the priorities of balance control when standing at high elevations by taking into account the direction of the postural threat in relation to themselves. The most prominent finding from this study is that participants increased postural accelerations in the sagittal plane when the threat was parallel to the participant, exhibiting a UCM by not strictly controlling fluctuation of the COM in the ‘safe’ direction. Specifically, participants allowed a longer range of sway acceleration in the direction of the support surface (the UCM), exhibiting the largest change in postural control from low to high elevation. The elongation of sway acceleration in the A/P direction may have been caused by prioritizing sway in the frontal plane (i.e., the direction of postural threat), at the expense of controlling A/P postural sway. Participants did not exhibit changes in accelerations in the frontal plane and appeared to avoid postural sway acceleration in the M/L direction that brought them closer to the postural threat. In agreement with our hypotheses and the predictions of modern theories of motor control, at high elevations, participants exhibited a UCM by shifting priorities to avoid motion of the COM in the threatening lateral direction and not attending to postural fluctuation in the orthogonal direction (sagittal plane).
We observed a different pattern in the Perpendicular condition where participants restricted overall postural sway acceleration (i.e., total postural ellipse) from low to high heights. In this position, postural control was not affected by the specific direction of threat, but the results suggest an interaction between the effect of anxiety on the goals of the standing task and the biomechanical constraints of standing posture. The overall restriction of accelerations of the COM at height is consistent with the commonly reported ‘stiffening response,’ where participants restrict COP movement at high elevations (Brown et al. 2006; Adkin et al. 2008). Postural stiffening is considered to be a conservative, preparatory strategy that prevents destabilization from internal or external perturbations, and may be beneficial when task demands are low (Young and Williams 2015). The present findings suggest that a stiffening response is apparent when facing elevated heights, regardless of the spatial characteristics of the environment and allowance for postural fluctuations in the orthogonal plane. However, our data indicate that the observed postural stiffening may be a result of biomechanical coupling between A/P and M/L control. Contemporary models of postural control suggest that independent ankle torque in each limb can simultaneously control A/P and M/L sway through asymmetrical plantarflexion/dorsiflexion torques (Bakshi et al. 2019). We cannot affirm with confidence that individuals exhibited independent ankle or hip torques, but we speculate that combining a stiffening response with neuromechanical delays and intermittent muscle firings results in coupled postural control (Wang and Newell 2012). Therefore, when participants attempted to restrict postural fluctuation in the A/P direction, we observed a simultaneous reduction in M/L postural sway acceleration. When facing the threat, the overall restriction of postural adjustments suggested that coupling between the A/P and M/L planes of postural control at high elevations may be a result of the spatial goals of the standing task (avoiding a threat) combined with the biomechanical constraints of avoiding an anteriorly-oriented threat.
We relied on a wrist-worn consumer-friendly heart rate monitor to provide an index of anxiety-induced physiological arousal based on the VR height illusion. The data revealed a moderate increase in HR CV that was clinically detectable in this sample. Published reports have previously highlighted large physiological responses to anxiety derived from experimental manipulations that physically lift participants 3 m above ground (Tokuno et al. 2018) and use refined laboratory-based measures of physiological arousal such as electrodermal activity (EDA; Phanthanourak et al. 2016). In this study, a physiological response to the height illusion was not reflected in average heart rate, but our findings revealed a moderate increase in heart rate variability from low to high heights, supporting the efficacy of the VR height illusion. The present findings align with a previous study showing that young healthy adults exhibit increased heart rate variability from low to high virtual elevations, but this difference was not detectable in EDA or average beats per minute (Peterson et al. 2018). The majority of researchers reporting large physiological effects of VR height illusions in healthy people observe dynamic movements such as balance recovery from platform translations (Cleworth et al. 2016) or balance beam walking (Boroomand-Tehrani et al. 2019), which involve dynamic sensory processes and may be perceived as more demanding or realistic in VR compared to static standing tasks, perhaps resulting in stronger effects on physiological indices of anxiety. Nevertheless, the medium to large height-related differences in postural sway accelerations in the current study indicated the elevated VR simulation did elicit a behavioral response to threat, and increases to HR CV were detected by an accessible heart rate monitor. However, the present findings may differ in those with stronger height-related anxiety (e.g., individuals with acrophobia; Wuehr et al. 2019).
Limitations
Several limitations are worth considering. First, participants were healthy young adults and demonstrated a relatively stable posture in the M/L plane, so there may have been little room for change in postural control strategy from low to high elevations. The potential for floor/ceiling effects with respect to the task constraints may be perpetuated by a narrow stance width. Standing with the feet together drives postural control to act more like an inverted pendulum and limits small or fast adjustments to M/L sway (Winter 1995), which could have influenced the present findings. We brought back a subset of the original participants (see Supplemental Material) to support that behavioral responses in this study were related to the experimental manipulations rather than the biomechanical constraints of a narrow BOS. When participants’ feet were positioned pelvic-width apart, they generally adopted a similar pattern of increased sagittal plane postural acceleration and variability in parallel orientation and restricted overall sway in the perpendicular position from low to high elevations (see Supplemental Material). However, we did not examine this potential limitation empirically and acknowledge that the current findings may be limited to a narrow stance width. Further research using varied stance widths is warranted to determine if the present findings extend to other stance configurations. Second, we acknowledge the limitations of a fixed order in the study design, such that the Parallel condition was always administered first at each height. We exposed participants first to the low elevation, then high elevation environment, to maximize the anxiety-response at high elevation (Adkin et al. 2000). While this choice does theoretically increase the strength of the Height effect, the condition order is fundamentally confounded with both Height and Position. However, trial times in the current study were shorter in duration than height exposure trial times reported in other similar studies (30 s vs. 120 s; Cleworth et al. 2012), and we observed a significant Height effect during tasks that were completed after the standing tasks (Raffegeau et al. 2020), thus we suggest that any acclimation to height likely did not occur between Parallel and Perpendicular standing trials. For this reason, we focused on the interaction effect between Height and Position to understand the results, and suggest that in the future researchers control for the limitations of a fixed order with repeated trials and randomized condition order. Third, whereas in previous published reports participants were asked to fix gaze using a visual target (i.e. Brown et al. 2006; Adkin et al. 2008) within a range suggested to control for physiological height vertigo effects (Bles et al. 1980; Brandt et al. 1980), we did not provide participants with a fixed target while standing. While visual objects are present in the VR environment at both low and high heights, specific visual targets were not included in this version of the VR program because it was designed to measure dynamic activity (e.g., walking/turning), where visual targets would impede such adaptive walking (Lo et al. 2015; Worden et al. 2016). We were motivated to promote ‘natural’ gaze behavior because participants were transported to the high elevations to prevent sensory conflict/motion sickness during the transition from low to high heights (Lee 2019). Therefore, the success of the height illusion depended on the ability to gather visual information from the virtual environment. However, variations in gaze behavior and visual sampling strategies may have influenced postural responses differently from previous studies, or as a result of changes in the visual feedback inherent to each condition. Additionally, the HTC Vive headset has a field of view of 100° horizontally and 110° vertically, limiting wide ranges in visual gaze behavior, but potentially impeding important peripheral visual feedback of the height illusion, although this limitation was present in both standing positions. A closer examination of the interactions between gaze strategies and task constraints while standing at virtual elevation is a fruitful candidate for future work. Fourth, we did not include any measures of subjective immersion or state anxiety in this study, thus we cannot confirm how participants perceived the postural threat during the standing task. Finally, our results and interpretation are limited to observing 30 s of unperturbed postural responses. We suggest that in the future researchers apply the UMT framework to understand postural responses to the direction of threat by including perturbations, presenting threat directionally, and capturing traditional performance outcomes across repeated trials.
Conclusion
Overall, these novel findings suggest that standing balance in anxiety-inducing settings may be reconfigured in accordance with constraints imposed by the direction of postural threat, supporting the salience of spatial properties of postural threat when identifying controlled characteristics of balance. When participants stood along a walkway with a lateral postural threat, they allowed more postural accelerations in the ‘safe’ direction (A/P) and prevented change in the direction of threat (M/L) consistent with use of an UCM. Conversely, when facing the postural threat, participants were unable to allow similar fluctuations in the M/L direction, even if it was safe, which aligns with a stiffening response interpretation. We speculate the directional-dependence of this response may be based on biomechanical coupling of A/P and M/L sway from independent ankle or hip torques. In the future, theoretically-driven work is needed to better understand how balance control and postural strategies are modified in response to the spatial context (direction) of threat.
Supplementary Material
Acknowledgements
We would like to acknowledge the hard work of the students that made this work possible including Mindie Clark, Nick Kreter, and Ashlee McBride.
Funding
PCF was supported by the Eunice Kennedy Shiver National Institute of Child Health and Human Development of the National Institutes of Health under Award Number K12HD073945. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Health.
Footnotes
Availability of data and material All data are available here: https://github.com/keithlohse/Gait_VR/tree/master/standing_balance.
Code availability All analysis code are available here: https://github.com/keithlohse/Gait_VR/tree/master/standing_balance.
Electronic supplementary material The online version of this article (https://doi.org/10.1007/s00221-020-05917-5) contains supplementary material, which is available to authorized users.
HTC Vive versions were switched to version 2.0 after the first six participants to increase the number of lighthouses (i.e., infrared tracking stations) from two to four and improve tracking quality.
Conflict of interest The authors have no conflict of interest. Material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the author, and are not to be construed as official, or as reflecting true views of the Department of the Army or the Department of Defense. The investigators have adhered to the policies for protection of human subjects as prescribed in AR 70–25.
Ethics approval All procedures in this study were approved by the University of Utah IRB.
Consent to participate All participants provided informed consent in accordance with the Declaration of Helsinki.
References
- Adkin AL, Carpenter MG (2018) New insights on emotional contributions to human postural control. Front Neurol 9:789. 10.3389/fneur.2018.00789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adkin AL, Frank JS, Carpenter MG, Peysar GW (2000) Postural control is scaled to level of postural threat. Gait Posture 12:87–93. 10.1016/S0966-6362(00)00057-6 [DOI] [PubMed] [Google Scholar]
- Adkin AL, Campbell AD, Chua R, Carpenter MG (2008) The influence of postural threat on the cortical response to unpredictable and predictable postural perturbations. Neurosci Lett 435:120–125. 10.1016/j.neulet.2008.02.018 [DOI] [PubMed] [Google Scholar]
- Bakshi A, Dizio P, Lackner JR (2019) Adaptation to coriolis force perturbations of postural sway requires an asymmetric two-leg model. J Neurophysiol 121:2042–2060. 10.1152/jn.00607.2018 [DOI] [PubMed] [Google Scholar]
- Bates D, Mächler M, Zurich E et al. (2015) Fitting linear mixed-effects models using lme4 [Google Scholar]
- Bles W, Kapteyn TS, Brandt T, Arnold F (1980) The mechanism of physiological height vertigo II. Posturography. Acta Otolaryngol 89:534–540. 10.1017/CBO9781107415324.004 [DOI] [PubMed] [Google Scholar]
- Boroomand-Tehrani A, Huntley AHAB-TAH, Jagroop D et al. (2019) The effects of postural threat induced by a virtual environment on performance of a walking balance task. bioRxiv. 10.1101/752139 [DOI] [PubMed] [Google Scholar]
- Brandt T, Arnold F, Bles W, Kapteyn TS (1980) The mechanism of physiological height vertigo I. Theoretical approach and psychophysics. Acta Otolaryngol 89:513–523 [DOI] [PubMed] [Google Scholar]
- Brown LA, Polych MA, Doan JB (2006) The effect of anxiety on the regulation of upright standing among younger and older adults. Gait Posture 24:397–405. 10.1016/j.gaitpost.2005.04.013 [DOI] [PubMed] [Google Scholar]
- Carpenter MG, Frank JS, Silcher CP (1999) Surface height effects on postural control: a hypothesis for a stiffness strategy for stance. J Vestib Res Equilib Orientat 9:277–286 [PubMed] [Google Scholar]
- Carpenter MG, Frank JS, Silcher CP, Peysar GW (2001) The influence of postural threat on the control of upright stance. Exp Brain Res 138:210–218. 10.1007/s002210100681 [DOI] [PubMed] [Google Scholar]
- Cleworth TW, Horslen BC, Carpenter MG (2012) Influence of real and virtual heights on standing balance. Gait Posture 36:172–176. 10.1016/J.GAITPOST.2012.02.010 [DOI] [PubMed] [Google Scholar]
- Cleworth TW, Chua R, Inglis JT, Carpenter MG (2016) Influence of virtual height exposure on postural reactions to support surface translations. Gait Posture 47:96–102. 10.1016/j.gaitpost.2016.04.006 [DOI] [PubMed] [Google Scholar]
- Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates, New York [Google Scholar]
- Cumming G (2012) Cohen’s d. In: Understanding the new statistics: effect sizes, confidence intervals, and meta-analysis. Routledge, pp 281–320 [Google Scholar]
- Cusumano JP, Dingwell JB (2013) Movement variability near goal equivalent manifolds: fluctuations, control, and model-based analysis. Hum Mov Sci 32:899–923. 10.1016/j.humov.2013.07.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ehgoetz Martens KA, Ellard CG, Almeida QJ (2015) Virtually-induced threat in Parkinson’s: dopaminergic interactions between anxiety and sensory–perceptual processing while walking. Neuropsychologia 79:322–331. 10.1016/J.NEUROPSYCHOLOGIA.2015.05.015 [DOI] [PubMed] [Google Scholar]
- Gendre M, Yiou E, Gélat T et al. (2016) Directional specificity of postural threat on anticipatory postural adjustments during lateral leg raising. Exp Brain Res 234:659–671. 10.1007/s00221-015-4471-x [DOI] [PubMed] [Google Scholar]
- Hedges LV (1981) Distribution theory for glass’s estimator of effect size and related estimators. J Educ Stat 6:107–128 [Google Scholar]
- Johnson KJ, Zaback M, Tokuno CD et al. (2019) Repeated exposure to the threat of perturbation induces emotional, cognitive, and postural adaptations in young and older adults. Exp Gerontol 122:109–115. 10.1016/j.exger.2019.04.015 [DOI] [PubMed] [Google Scholar]
- Latash M, Levin M, Scholz J, Schöner G (2010) Motor control theories and their applications. Medicina (B Aires) 46:382. 10.3390/medicina46060054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee GC (2019) Full immersion virtual reality: adverse effects related to static balance. Neurosci Lett. 10.1016/j.snb.2019.127065 [DOI] [PubMed] [Google Scholar]
- Lo OY, van Donkelaar P, Chou LS (2015) Distracting visuospatial attention while approaching an obstacle reduces the toe-obstacle clearance. Exp Brain Res 233:1137–1144. 10.1007/s00221-014-4189-1 [DOI] [PubMed] [Google Scholar]
- Mancini M, Salarian A, Carlson-Kuhta P et al. (2012) ISway: a sensitive, valid and reliable measure of postural control. J Neuroeng Rehabil 9:1. 10.1186/1743-0003-9-59 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martens MA, Antley A, Freeman D et al. (2019) It feels real: physiological responses to a stressful virtual reality environment and its impact on working memory. J Psychopharmacol. 10.1177/0269881119860156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moe-Nilssen R (1998) A new method for evaluating motor control in gait under real-life environmental conditions. Part 1: the instrument. Clin Biomech 13:320–327 [DOI] [PubMed] [Google Scholar]
- Peterson SM, Furuichi E, Ferris DP (2018) Effects of virtual reality high heights exposure during beam-walking on physiological stress and cognitive loading. PLoS One 13:1–18. 10.1371/journal.pone.0200306 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phanthanourak AL, Cleworth TW, Adkin AL et al. (2016) The threat of a support surface translation affects anticipatory postural control. Gait Posture 50:145–150. 10.1016/j.gaitpost.2016.08.031 [DOI] [PubMed] [Google Scholar]
- R Core Team (2019) R: a language and environment for statistical computing [Google Scholar]
- Raffegeau TE, Fawver B, Clark M, Engel BT, Young WR, Williams AM, Lohse KR, Fino PC (2020) The feasibility of using virtual reality to induce mobility-related anxiety during turning. Gait Posture 77:6–13. 10.1016/j.gaitpost.2020.01.006 [DOI] [PubMed] [Google Scholar]
- Scholz JP, Schöner G (1999) The uncontrolled manifold concept: identifying control variables for a functional task. Exp Brain Res 126:289–306. 10.1007/s002210050738 [DOI] [PubMed] [Google Scholar]
- Tokuno CD, Keller M, Carpenter MG et al. (2018) Alterations in the cortical control of standing posture during varying levels of postural threat and task difficulty. J Neurophysiol 120:1010–1016. 10.1152/jn.00709.2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang Z, Newell KM (2012) Asymmetry of foot position and weight distribution channels the inter-leg coordination dynamics of standing. Exp Brain Res 222:333–344. 10.1007/s00221-012-3212-7 [DOI] [PubMed] [Google Scholar]
- Winter DA (1995) Human blance and posture control during standing and walking. Gait Posture 3:193–214. 10.1016/0966-6362(96)82849-9 [DOI] [Google Scholar]
- Worden TA, Mendes M, Singh P, Vallis LA (2016) Measuring the effects of a visual or auditory Stroop task on dual-task costs during obstacle crossing. Gait Posture 50:159–163. 10.1016/j.gaitpost.2016.08.033 [DOI] [PubMed] [Google Scholar]
- Wuehr M, Breitkopf K, Decker J et al. (2019) Fear of heights in virtual reality saturates 20 to 40 m above ground. J Neurol 266:80–87. 10.1007/s00415-019-09370-5 [DOI] [PubMed] [Google Scholar]
- Young WR, Williams AM (2015) How fear of falling can increase fall-risk in older adults: applying psychological theory to practical observations. Gait Posture 41:7–12. 10.1016/j.gaitpost.2014.09.006 [DOI] [PubMed] [Google Scholar]
- Zaback M, Carpenter MG, Adkin AL (2016) Threat-induced changes in attention during tests of static and anticipatory postural control. Gait Posture. 10.1016/j.gaitpost.2015.12.033 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.