

Abstract
Preclinical testing platforms have been instrumental in the research and development of thrombectomy devices. However, there is no single model which fully captures the complexity of cerebrovascular anatomy, physiology, and the dynamic artery-clot-device interaction. This paper provides a critical review of phantoms, in-vivo animal, and human cadaveric models used for thrombectomy testing and provides insights into the strengths and limitations of each platform. Articles published in the last ten years that reported thrombectomy testing platforms were identified. Characteristics of each test platform, such as intracranial anatomy, artery tortuosity, vessel friction, flow conditions, device-vessel interaction, and visualization, were captured and benchmarked against human cerebral vessels involved in large vessel occlusion stroke. Thrombectomy phantoms have been constructed from silicone, direct 3D-printed polymers, and glass. These phantoms represent oversimplified patient-specific cerebrovascular geometry but enable adequate visualization of devices and clots under appropriate flow conditions. They do not realistically mimic the artery-clot interaction. For the animal models, arteries from swine, canines, and rabbits have been reported. These models can reasonably replicate the artery-clot-device interaction and have the unique value of evaluating the safety of thrombectomy devices. However, the vasculature geometries are substantially less complex and flow conditions are different from human cerebral arteries. Cadaveric models are the most accurate vascular representations but with limited access and challenges in reproducibility of testing conditions. Multiple test platforms should be likely used for comprehensive evaluation of thrombectomy devices. Interpretation of the testing results should take into consideration platform-specific limitations.
INTRODUCTION
Thrombectomy has become the standard of care for large vessel occlusion (LVO) stroke since 2015.1 Although large-bore catheter and stent retriever technologies have been refined and clinical experience has steadily accumulated, the limitations of low rates of first-pass efficacy and complete recanalization persist.2,3 Interestingly, many devices currently in clinical use demonstrated recanalization rates in pre-clinical models close to 100%, suggesting that current testing platforms tend to oversimplify thrombectomy conditions and/or underestimate pitfalls. More realistic pre-clinical testing platforms would enable the scientific community to generate new knowledge in thrombectomy mechanics and develop devices more likely to achieve first-pass efficacy. Although various test platforms have been described in the literature to date, a critical comparison is lacking, especially because each research group has generally focused on one subtype neglecting the others. Several reviews have been published on this topic. Mehra et al. provided a review mainly on animal models back in 2011,4 but over 50 articles on different thrombectomy models have been published ever since. In the latest two reviews on thrombectomy models, Herrmann et al. reviewed large animal models,5 and Waqas et al. reviewed 3D printed models,6 neither of which provided a systematic comparison between benchtop phantoms and animal models or included the lately published cadaveric models. In this review, we collected articles published from January 2011 to Oct 2020 and describing in vitro or in vivo models for mechanical thrombectomy testing. To compare against human cerebral vessels, the following characteristics for each type of platforms were summarized: intracranial tortuosity, proximal artery tortuosity, vessel friction, flow conditions, visualization, and artery-device interaction. The recanalization rates and complications such as distal embolization and vasospasm were also compared against clinical results of thrombectomy. Clot analogs used to replicate LVO are also summarized. We provide a critical discussion on the advantages and disadvantages of each test platform so that readers understand the pros and cons of testing devices in any given models. We also include insights and suggestions derived from first-hand experience in the development, optimization and testing of devices involving each model category.7–11
BENCHTOP PHANTOMS
Nineteen articles were included for the benchtop phantoms used for thrombectomy testing (Table 1), including: silicone (13 articles), direct 3D-printed (five articles), and glass (three articles).
Table 1.
Experiment setup and recanalization results for benchtop phantoms.
| Study | Vascular bed | Fluid | Clots | Technique | Recanalization rate | Passes to recanalization | Distal embolization |
|---|---|---|---|---|---|---|---|
| Silicone | |||||||
| Tennuci et al. 201112 | NA | Saline | Ovine blood | DA, SR | DA: 16%; SR: 22% | DA: 1.9, SR: 1.3 | 33% |
| Saleh et al. 201213 | NA | Saline | Ovine blood | SR | 80%–90% | 1.6–2.1 | 37% |
| Chueh et al. 201215 | NA | 40 vt% glycerin |
Bovine blood + barium | DA, SR | DA: 83%, SR: 67%–100% | NA | Present |
| Chueh et al. 201316 | ICA-MCA-ACA | 40 vt% glycerin |
Hard: Bovine blood + barium, Soft: human blood | SR | ~100% | 1.1–1.5 | Present |
| Madjidyar et al. 201517 | CCA-ICA-MCA-ACA | 40% vt glycerin |
Human blood | SR, SR+A | 100% | SR: 4.5, SR+A: 2 | 98% |
| Fargen et al. 201662 | ICA-MCA-ACA | Saline | NA | SR | 27–80% | NA | 40% |
| Van Der Marel et al. 201663 | CoW | Saline | Soft: human blood + barium, Hard: bovine blood + barium | SR | NA | NA | Present |
| Chueh et al. 201764 | ICA-MCA-ACA | Saline | Bovine blood + barium | SR, SR+A | 96% | Mostly single pass | Present |
| Larsen et al. 201865 | NA | Saline | Human blood | SR | NA | NA | 100% |
| Madjidyar et al. 201966 | NA | Saline | Red & white human emboli | DA, SR | ~100% | White emboli: 1, red emboli: 1–1.5 | 42% |
| Arslanian et al. 201967 | CoW | Saline | Hard: Bovine blood + fibrinogen, Soft: bovine blood + barium | DA, SR | NA | NA | Present |
| Johnson et al. 202068 | CoW | Saline | Ovine PRP + ovine bone | DA, SR | NA | NA | NA |
| Reddy et al. 20208 | ICA-MCA-ACA | Saline | Human RBCs + plasma + barium | DA, SR+A | NA | 1.3–1.9 | Present |
| Direct 3D printed | |||||||
| Mokin et al. 201518 | CoW | 40 vt% glycerin |
Swine blood + bovine fibrinogen | DA, SR, SR+A | DA: 100%; SR: 37%–55%; SR+A: 82% | NA | 37% |
| Mokin et al. 201569 | CoW | NA | Swine blood + bovine fibrinogen | SR, SR+A | SR: 36%; SR+A: 91% | NA | 14% |
| Mokin et al. 201670 | CoW | NA | Swine blood + bovine fibrinogen | SR | 45%–91% | NA | 16% |
| Fennell et al. 201871 | CoW | Water | Ovine RBC + plasma | SR | 100% or 8% | 2.2 or 3 | 32% |
| Reddy et al. 20208 | ICA-MCA-ACA | Saline | Elastic: human RBCs + plasma, Fragment-prone: human RBCs + plasma + barium | DA, SR+A | NA | NA | Present |
| Glass | |||||||
| Wenger et al. 201320 | NA | Water | Swine blood | SR | 85% | ~1.5 | 38% |
| Liu et al. 20207, Reddy et al. 20208 | ICA-MCA-ACA | Saline | Elastic: human RBCs + plasma, Fragment-prone: human RBCs + plasma + barium | DA, SR+A | NA | NA | Present |
ACA: anterior commuting artery; CCA: common carotid artery; CoW: circle of Willis; DA: direct aspiration; ICA: internal carotid artery; MCA: middle cerebral artery; PRP: platelets-rich plasma; RBC: red blood cell; SR: stent retriever; SR+A: stent retriever with aspiration.
Silicone phantoms
Silicone is the most frequently used material to build thrombectomy phantoms. In many cases, silicone phantoms were commercial products and the fabrication techniques were proprietary,8,12,13 Chueh et al. described the technique for small-batch fabrication.14 Briefly, patient-specific vasculature was reconstructed from CT and then modified to make a core-shell mold with the core having the same geometry as the reconstructed lumen. The mold was then 3D printed and liquid silicone was infused into the mold. The mold was dissolved after silicone cured, resulting in silicone vessels with the patient-specific lumen geometry.
Most of the reported silicone phantoms (8/13) can accurately replicate the gross geometry of the main intracranial arteries (Table 1). Replicating the proximal arteries such as the common carotid arteries and aortic arch is possible but have been seldomly implemented in research.8,12,13 There are commercially-available solutions such as the Replicator from Mentice that provides transfemoral and transradial access. To reduce the friction, the inner wall of the silicone vessel can be coated by liquid silicone rubber to mimic the lubricity of the endothelial layer and infused with slippery fluid,8,14 resulting in similar navigation difficulty compared to patients.8 The silicone phantoms can be connected to a pump system to deliver accurate (both in flow rate and pressure) flow of blood mimicking fluid, such as 40 vt% glycerin solution with similar rheological properties to blood.15–18 In addition, the silicone vessels are transparent and allow radiation-free observation of clot-device interaction (Fig. 1A).8 However, the synthetic nature of silicone prevents the phantoms from accurately mimicking vessel wall injury, the interaction of the clot to the vascular surface, and the phantoms are significantly stiffer than biological arteries. A large range of recanalization rates (16%−100%) were reported as different blood material and devices were tested. Distal embolization was reported in most (12/13) of the studies.
Figure 1. Optical visualization of thrombectomy of clots in the anterior circulation inside a silicone phantom (A), direct 3D-printed phantom (B), glass phantom (C), and whole human brain model (D).
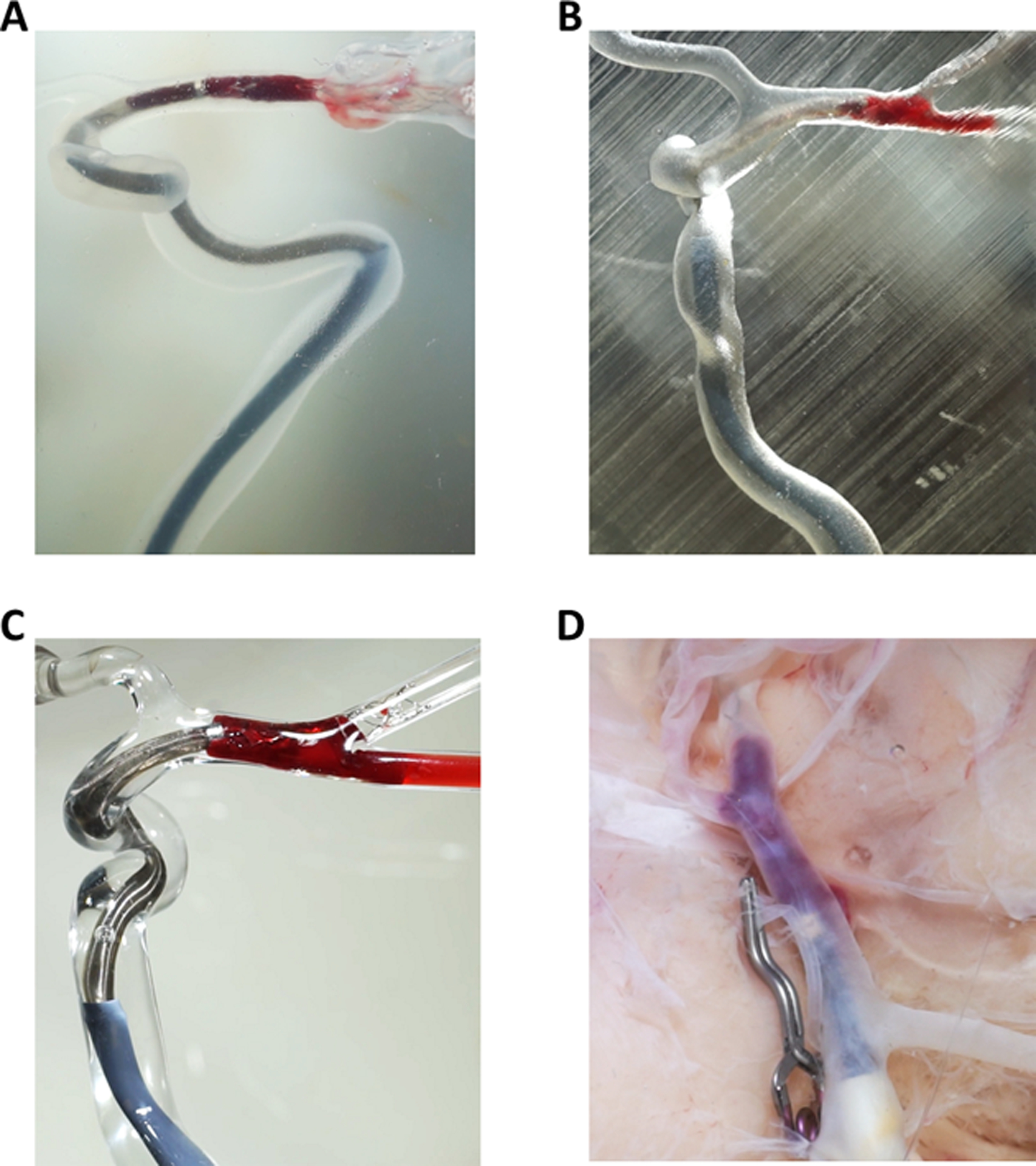
All the test platforms can enable high-definition and radiation-free observation of device-clot interaction and the glass phantom provides the best clarity.
Direct 3D-printed phantoms
Similar to the silicone phantoms, direct 3D-printed phantoms were also fabricated from reconstructed patient-specific anatomy. Two kinds of proprietary polymer have been used: Stratasys Tango Plus®,19 and Formlab Clear Resin® which is rigid and more transparent.8 The 3D-printed phantoms have the least amount of lead time to prepare and cost the least among all the benchtop phantoms.8
The 3D-printed phantoms had per report an accurate representation of the geometry of the main intracranial arteries (Table 2). Replicating the proximal arteries is possible but has not been reported. The friction of the 3D-printed arteries is high, resulting in more difficult navigation than what is seen in patients.8 All of the reported phantoms were connected to a pump system to deliver physiological flow, although glycerin solution to match the blood’s viscosity was only reported in one study (Table 1).18 Optical visualization of the thrombectomy process (Fig. 1B) is possible but not as good as in silicone phantoms.8 The 3D printed arteries are much stiffer than human arteries and cannot be used to study artery-device interaction.8 Similar to the silicone phantom studies, a large range of recanalization rates (8%−100%) was reported and distal embolization was reported in all the studies.
Table 2.
Comparison of thrombectomy test platforms in major thrombectomy related characteristics.
| Silicone | 3D-printed | Glass | Swine | Canine | Rabbit | Human brain | Cadaver | |
|---|---|---|---|---|---|---|---|---|
| Intracranial tortuosity | Similar to human | Similar to human | Simpler than human | Absent | Possible* | Absent | Absent | Identical to human |
| Proximal artery tortuosity | Possible | Possible | Possible | Absent | Absent | Absent | Absent | Identical to human |
| Vessel friction | Similar to human | More friction than human | Less friction than human | Similar to human | Similar to human | Similar to human | NA‡ | NA‡ |
| Flow conditions | Similar to human | Similar to human | Similar to human | NA | Slower than human | Similar to human | Similar to human | NA‡ |
| Visualization of clot-device interaction | Good | Fair | Excellent | Poor | Poor | Poor | Good | Poor |
| Visualization of artery-clot-device interaction | Absent# | Absent# | Absent# | Absent | Absent | Absent | Excellent | Absent |
| Artery-device interaction | ||||||||
| Vessel wall injury | Minimal to absent | Absent | Absent | Underestimate | Underestimate | Underestimate | Good | Limited |
| Vasospasm | Absent | Absent | Absent | Overestimate | Present | NA | Absent | Absent |
For canine middle cerebral artery
Not tested or validated
Absent as the arterial wall in phantoms can’t realistically mimic the mechanical response of human arterial wall
Glass phantoms
Glass phantoms are fabricated by blowing glass tubes for hand-shaping and connection, and were only reported in three studies (Table 1).7,8,20 Due to the fabrication techniques, the glass arteries had a mildly simplified geometry compared to human anatomy, and glass models including the proximal artery tortuosity have not been reported in the literature (Table 2). The lubricity of the glass arteries has not been quantified, although navigation was shown to be easier than patients.8 The glass phantoms can also be connected to a pump system to deliver physiological flow, although only water or saline which were less viscous than blood were used. The glass arteries have the highest optical transparency and clarity, allowing the best visualization of the clot-device interaction (Fig. 1C). However, glass arteries are rigid so it is not possible to evaluated the response to mechanical loading of the devices. A recanalization rate of 85%, which is similar to clinical experience,21 has been reported in glass models (Table 1). Distal embolization was reported in all the studies.
ANIMAL MODELS
Nineteen articles were included for the animal models used for thrombectomy testing (Table 3) including: swine (15 articles), canine (two articles), and rabbit (two articles). The endothelium lining of animal arteries better mimics friction in human artery and the animal blood better resembles the rheologic properties of human blood when compared to the benchtop phantoms. However, visualization for artery-clot-device interaction in the animal models is limited to fluoroscopy.
Table 3.
Experiment setup, recanalization results, and complications for animal models.
| Study | Vascular bed | Clots | Technique | Recanalization rate | Passes to recanalization | Distal embolization | Vasospasm | Acute vessel damage |
|---|---|---|---|---|---|---|---|---|
| Swine | ||||||||
| Mordasini et al. 201122 | IMA, LA | Swine blood + barium | SR | 100% | NA | Absent | 100% | NA |
| Nogueira et al. 201223 | IMA, LA | Regular: swine blood + Barium, white: swine PRP + barium | SR, SR+A | 100% | Mostly 1 | 6% | 100% | Endothelial denudation, acute inflammation and hemorrhage in adventitia, degeneration of IEL |
| Gory et al. 201325,72 | SFA | Swine blood + barium | SR | NA | NA | NA | NA | Endothelial denudation, intimal layer edema, degeneration of IEL, medial edema |
| Yuki et al. 201326 | SCA | Swine blood + barium | SR | 75% | 2 | NA | NA | Acute inflammation |
| Shao et al.201427, Zhu et al. 201628 | LA, SCA, DCA | Swine blood + barium | SR | 94% | Mostly 1 | Absent | 100% | Endothelial denudation, degeneration of IEL |
| Wainwright et al.73 | ITA, VA | NA | SR | NA | NA | Absent | Absent | Endothelial denudation |
| Jiang et al.201629 | CCA | Swine blood + fibrinogen + iopamidol | SR | 100% | 1.3 | Absent | 9% | Absent |
| Srinivasan et al. 201730 | IMA | Swine blood | SR+A | NA | NA | NA | 100% | NA |
| Peschillo et al. 201731 | CCA, SCA | Swine blood | DA, SR | DA: 50%, SR: 100% | NA | 25% | 25% | Endothelial denudation, degeneration of IEL and adventitia |
| Ulm et al. 201834 | CCA | Red: Swine blood + barium, White: swine plasma | SR | 97% | 1.2 | 5% | 100% | Endothelial denudation |
| Jankowitz et al. 201974 | IMA, SCA, renal artery | Swine blood | DA | 93%−100% | NA | NA | Present | Endothelial denudation |
| Sanchez et al. 202075 | LA, cervical artery | Firm: swine plasma + RBCs, Soft: swine blood | SR, SR+A | SR: 77%, SR+A: 100% | SR: 1.9, SR+A: 1.4 | 4% | 62% | NA |
| Simgen et al. 202024 | Auxiliary artery | NA | SR | 100% | NA | NA | Absent | Absent |
| Canine | ||||||||
| Park et al. 201341 | IMA | Canine blood | SR | 100% | 2 | 40% | Absent | Endothelial denudation |
| Brooks et al. 201940 | MCA | Canine blood + fibrinogen | SR | 67% | 1 | NA | 1/6 | NA |
| Rabbit | ||||||||
| Gounis et al. 201344 | CCA | Rabbit blood | SR | 0 | NA | NA | NA | Endothelial denudation |
| Arai et a;. 201645 | CCA | Absent | SR | NA | NA | NA | NA | NA |
APA: ascending pharyngeal artery; CCA: common carotid artery; CoW: circle of Willis; DA: direct aspiration; DCA: deep cervical artery; EC: endothelial cell; ICA: internal carotid artery; IMA: internal maxillary artery; IEL: internal elastic lamina; ITA: internal thoracic artery; LA: lingual artery; MCA: middle cerebral artery; PRP: platelets-rich plasma; RBC: red blood cell; SCA: superficial cervical artery; SFA: superficial femoral artery; SR: stent retriever; SR+A: stent retriever with aspiration; VA: vertebral artery.
Swine model
The swine anterior intracranial circulation is not accessible for catherization due to the presence of the rete mirabile and extracranial arteries are the most used for thrombectomy testing (Table 3). A variety of arteries, although significantly less tortuous than human intracranial arteries, have been used with lumen sizes spanning from the M2 segment of human middle cerebral artery (MCA) to human internal carotid artery (ICA) (Fig. 2). Catheters were delivered via femoral access for most (11/16) of the studies,22–32 while carotid access was also used in another two studies.33,34 Flow velocity was not evaluated in any of these studies but the peak systolic velocity in the swine carotid was reported about 20 cm/s,35 much slower than that of human MCA (95 cm/s).36 In addition, these swine arteries are rather muscular with higher diastolic resistance than human intracranial arteries. Among the studies where histopathologic evaluation of arterial wall response was carried out, the most common (9/12) vessel wall injury was endothelial denudation, and no arterial dissection was reported. Swine arteries were overly susceptible to vasospasm. Among studies (10 articles) where vasospasm was evaluated, over a half (7 articles) have reported vasospasm happening during every recanalization procedure (Table 3). In comparison, clinical vasospasm rate is only 3.9%−23%.37 A large range of recanalization rate (50%−100%) was reported. Among studies where distal embolization was evaluated, over half (6/10) studies reported absence of distal embolization while the clinical incidence rate is about 20%,38 implying an underestimation of the distal embolization event in the swine models.
Figure 2. Lumen diameter of the target vessels in animal models for thrombectomy and comparison to human cerebral arteries involved in large vessel occlusion.
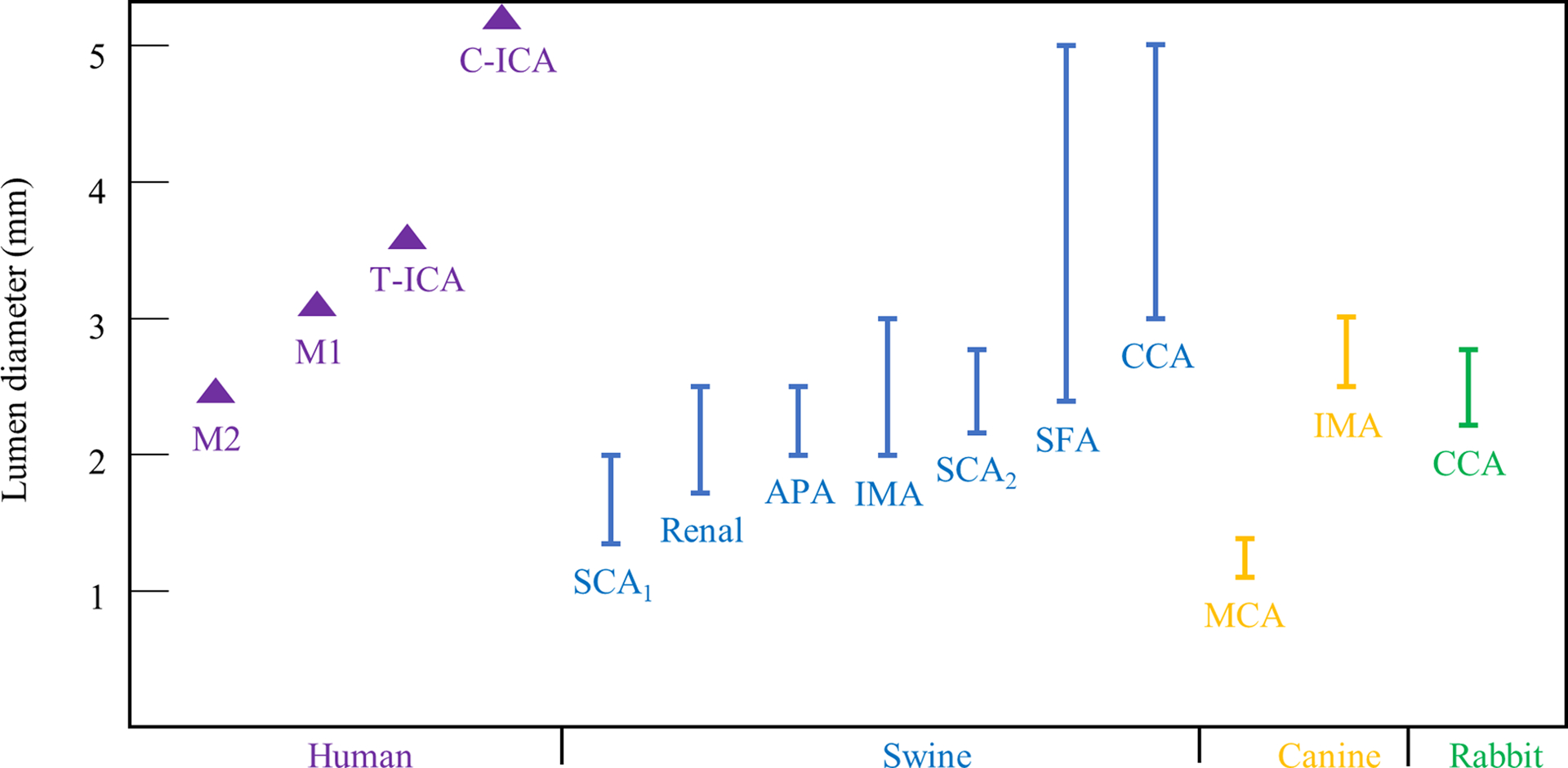
Included arteries: human M2,39 M1,39 D-ICA,39 and P-ICA,39 swine SCA,26,31 renal arteries,33 APA,33 IMA,30 SFA,25,72 and CCA;31 canine MCA,40 IMA,41 and VA;76 rabbit CCA.46 APA: ascending pharyngeal artery, CCA: common carotid artery, C-ICA: cavernous ICA, ICA: internal carotid artery, IMA: internal maxillary artery, MCA: middle cerebral artery, SCA: superficial cervical artery, SFA: superficial femoral artery, T-ICA: terminal ICA, VA: vertebral artery.
Canine model
Canines lack the rete mirabile and therefore catheterization of intracranial arteries is possible. The canine MCA (Table 3) has been used for thrombectomy testing although the lumen diameter (1.2–1.4 mm) is much smaller than human MCA (3.1 mm) (Fig. 2),39,40 limiting the capacity of testing large-bore catheters. In another study, the canine internal maxillary artery (IMA) with comparable lumen diameter (2.4–3.0 mm) to human MCA was used for thrombectomy testing (Fig. 2).41 Flow velocity was not evaluated but the mean velocity was reported to be slower than human MCA (18 cm/s vs 71 cm/s) in another study.42,43 Vessel wall injury was limited to endothelial denudation and rare vasospasm (1/6) was reported for the MCA,40 and no vasospasm was reported for the IMA.41 In addition, the degree of vasospasm was milder than that seen in swine arteries.23 Recanalization rates of 67% and 100%, and distal embolization rates of 0 and 40% were reported for the MCA and the IMA, respectively.
Rabbit model
The rabbit CCA has been used to replicate LVO and catheterization has been done via transfemoral access (Table 3).44,45 The lumen diameter of the rabbit CCA (2.2–2.8 mm) is similar to those of M1(3.1 mm) and M2 (2.4 mm) segments of human MCA(Fig. 2).39,46 Rabbit blood has the closest rheological similarity to human blood,47 but blood flow conditions have not been evaluated in the thrombectomy studies. From another study, the mean blood velocity in the rabbit carotid is slightly less (53 cm/s vs 71 cm/s) than human MCA.43,48 During thrombectomy testing, vessel wall injury was limited to endothelial denudation and vasospasm was not evaluated. Neither successful recanalization nor events of distal embolization were reported.
CADAVERIC MODELS
Whole human brain model
Hybrid test bed consisting of pressurized human brains had been developed and validated for LVO and revascularization with aspiration catheters and stent retrievers.9 In this model, fresh human brains were harvested en-bloc and tested within 24 hours of death to minimize postmortem degradation effect on testing results, and histological analysis of tissues confirmed the tissue integrity. The ICAs and vertebral arteries were cannulated and connected to a hydraulic system. This model reproduced LVO by embolization of representative clot analogs (elastic, fragment-prone, and stiff). Physiological pressure with pulsatile waveforms can be generated consistently, and the optically semi-transparent arterial walls enabled conventional cameras to visualize the artery-clot-device interaction without the need of radiation (Fig. 1D)11. This model is the most accurate to replicate the cerebrovascular anatomy, including perforating arteries and small arterial branches, and to capture the response of the arterial wall to mechanical forces.9 Recanalization rates are similar to the observed in clinic.9 In addition, this model has demonstrated previously suspected but unproven failure mechanisms of current thrombectomy devices, including arterial collapse, arterial traction and avulsion, and residual occlusion in small and perforating arteries in the context of “complete” parent artery revascularization.11 Limitations of the model includes the absence of carotid petrous and cavernous ICA segments and the ex-vivo nature of the tissue that precludes the analysis of biologically active phenomena such as vasospasm.9,11
Whole cadaver model
This model has been used to evaluate the navigation of a device to a target intracranial artery but not to test thrombectomy. In this model, fresh-frozen cadavers were infused with hot water and thrombectomy devices were advanced to the MCAs or basilar arteries via transfemoral access.49
CLOT ANALOGS
Most of the clot analogs were made by whole blood (Tables 1 and 3), which are soft and easy to be removed and could be a reason for the reported high recanalization rates in some studies. In comparison, clots retrieved from patients are known to have a large range of compositions and mechanical properties.7,50 To make clinically representative clot analogs, blood components were separated and mixed with different ratios,51,52 and mechanical properties were validated against a group of clots retrieved from patient with LVO by compression test to evaluate the clot stiffness,53 or tensile test to evaluate the stiffness and strength.52 The tensile test mimics the clot response to the tensional force (applied by pulling of a suction catheter or a stent retriever) during thrombectomy.52
EVALUATION OF RECANALIZATION AND DISTAL EMBOLIZATION
Testing results should be interpretated in the context of using different evaluation methods compared to fluoroscopy in clinic. To evaluate recanalization, studies using benchtop phantoms used the presence of clots or TICI score to evaluate recanalization. Although conventionally accepted, TICI is a scoring system for flow restoration (i.e. anterograde reperfusion angiographically detected by contrast penetration in the hemispheric vasculature), which cannot be accessed in phantoms as they only include proximal cerebral vasculature. Studies using animal models also employed TICI score although the extrapolation to human is limited given the major difference with human cerebral architecture. The whole human brain model, similar to benchtop phantoms, also focused on recanalization in proximal large vessel occlusion, although TICI score evaluation is also possible if post thrombectomy angiography is performed. For the published whole cadaver model, thrombectomy testing was not performed.
Distal embolization could be evaluated by fluoroscopy in animal and cadaveric models by comparing pre and post thrombectomy angiography or by employing radiopaque clots. However, quantification of size and numbers of emboli is significantly more precise in benchtop phantoms as the fluid can be collected and analyzed by a particulate analyzer.54
ADVANTAGES AND DISADVANTAGES OF DIFFERENT PLATFORMS
Multiple platforms should be used in combination to comprehensively evaluate thrombectomy in different aspects (Table 4) to support premarket submissions for new devices. Per the US FDA guideline, bench testing should be conducted to evaluate the devices’ maneuverability, flexibility, durability, and torque strength and animal testing should be conducted to evaluate the devices’ usability, safety, and effectiveness.55
Table 4.
Comparison of thrombectomy test platforms with suggested testing modalities.
| Silicone | 3D-printed | Glass | Swine | Canine | Rabbit | Human brain | Cadaver | |
|---|---|---|---|---|---|---|---|---|
| Navigation | Good | Fair | Fair | Poor | Poor | Poor | Poor | Good |
| Safety | Poor | Poor | Poor | Good | Good | Good | Good | Poor |
| Distal embolization | Good | Good | Good | Poor | Poor | Poor | Good | Poor |
| Action mechanism | Good | Fair | Good | Poor | Poor | Poor | Excellent | Poor |
| Analysis of failure mechanisms | Fair | Fair | Fair | Fair | Fair | Fair | Good | Fair |
| Recanalization rates | Overestimates | Overestimates | Overestimates | Overestimates | Overestimates | Overestimates | Accurate | NA |
Benchtop phantoms are the easiest to use and provide a decent representation of the anatomy for navigation testing. They can also allow direct optical visualization of the recanalization procedure to understand the action mechanism with much finer details than fluoroscopy, although the vessels are significantly stiffer than human cerebral arteries, limiting the fidelity of artery-clot-device interaction. Benchtop phantoms can also replicate physiological flow to study distal embolization. In addition, the benchtop phantoms are much more consistent and replicable compared to other testing platforms. However, benchtop phantoms usually lack small branching arteries and perforators, due to the limitation of the fabrication techniques.8 Therefore, distal occlusions or residual occlusions in small branching arteries cannot be captured.
In comparison, the animal models do not have realistic vascular anatomy or allow detailed observation of device-clot-artery interactions but have the unique value of assessing device safety. However, vessel damage might be underestimated. The human intracranial arteries have a much thinner adventitia, lack an external elastic lamina, and have a much smaller wall to lumen ratio,56 making them rather prone to damage during device maneuver. In addition, human intracranial arteries are surrounded by cerebrospinal fluid and are more easily injured than tested animal arteries with soft tissue surrounded. In addition, distal embolization could also be underestimated in animal models. Many tested animal arteries such as swine carotid, canine MCA, and rabbit CCA have lower flow velocity compared to human MCAs. Such lower flow velocity is associated with lower shear stress on the clot, resulting in an underestimation of distal embolization. In this review, most of the swine models reported absent or minimal embolization events (Table 3) while the clinical incidence rate is over 20%.38 For future animal models, the vascular bed should be selected to match both the lumen size and flow conditions of human cerebral arteries. Finally, the consistency of the testing results will inevitably suffer from animal subject variance.
The whole human brain model is the only model that enables the analysis of artery-clotdevice interaction under physiologic hemodynamic conditions within the unmodified complexity of the cerebral vasculature. However, it cannot accurately represent the challenges in device navigation from a peripheral arterial access to intracranial arteries. In comparison, the whole cadaver model replicates the access-to-target navigation experience with fluoroscopic guidance. However, it is challenging to recreate flow conditions that can mimic both the hemodynamics and friction behavior and there is no published description of thrombectomy procedures.
FUTURE THROMBECTOMY TESTING PLATFORMS
Future thrombectomy testing platforms should focus on optimizing the modelling of recalcitrant occlusions and challenging access. In a recent patient cohort study, of the 17% of the cases where only mTICI0–2a were achieved, top reasons were: persistent or new occlusions (65% cases) and the occlusion could not be reached or passed due to anatomical difficulty (20% cases).57 To model recalcitrant occlusions, there has not been a consensus. Srinivasan et al. have defined recalcitrant occlusion as unsuccessful recanalization after first pass and have recreated such occlusion by lodging large clot burden at bifurcations in a swine model.30
The higher recanalization rates observed in the bench implies oversimplified testing platforms. The thrombectomy devices apply tensional load (by suction or stent pull) to overcome the static friction between the clot and vessel wall and the pressure gradient across the clot to dislodge the clot.7 After clot is dislodged, the restored blood flow applies hemodynamic pressure and shear stress, which, together with the dynamic friction between the clot and vessel wall, can strip clot substance away from the main clot mass, leading to residual occlusion or distal embolization. Therefore, the thrombectomy test platform must accurately replicate hemodynamics and vessel wall friction. While physiological flow has been successfully replicated in the phantoms, the characterization of vessel wall friction is lacking and could be a future research topic. Tubular tissue scaffolds where the inner wall is seeded with endothelial cells have been used to compare the endothelial damage caused by aspiration and stent retriever.58 However, this approach is limited by the technical difficulty of making bifurcated and tortuous scaffolds. In addition, the adhesion forces between the endothelium and substrate has not been quantified and therefore the fidelity of endothelial damage is not validated.
The lack of realistic clot analogs that can accurately replicate the device-clot interactions may be another contributor for the non-realistic biomechanics inside thrombectomy test platforms. Although clot analogs made by mixing different blood components were described, these clot analogs have homogeneous structure while patient clots are known to frequently be heterogeneous,59 which are easier to fragment under the tensional load and hemodynamic forces and prone to cause residual occlusion or distal embolizations.7 In addition, most of the clot analogs used in thrombectomy testing have focused on the fibrin or RBC content while patient clots have more components and much more complex structure which can potentially affect thrombectomy efficacy. In a recent study, patient clots were found to be composed of RBC-rich and platelets-rich region, where dense fibrin/von Willebrand factor structure and neutrophil extracellular traps are presented and can affect the clot mechanical properties.60 However, von Willebrand factor and neutrophil extracellular traps have been overlooked in making clot analogs for thrombectomy testing and future research is warranted. Fabrication of clot analogs with similar mechanical properties and structure to patient clots is needed to improve the platform fidelity.
The inability to reach or pass an occlusion suggests an insufficient optimization of devices in challenging anatomies. Extreme tortuosity can make device delivery more challenging (i.e. stentrievers) and can possibly introduce kinks and bends to aspiration catheters, limiting aspiration forces. Cadaveric models could theoretically enable optimization of device navigability, but the tortuosity varies for each specimen and a large number is likely required to find challenging anatomy. The benchtop phantoms can be a better option as the geometry can be fully customized. By modularizing the vasculature (from femoral arteries and radial arteries to intracranial arteries) and having different representative anatomies for each module, such benchtop phantoms could be used to optimize the navigability of thrombectomy devices with a wide spectrum of anatomical difficulties.
Given the strength and weakness of each testing platform, different platforms should be utilized to achieve a comprehensive and accurate evaluation of thrombectomy devices. Ideally, all these platforms should be harbored in a single center employing a unified clot analog model to interpret and compare results across different models. However, multi-center pre-clinical trials could be potentially carried out to take advantages of the experience and expertise on specific testing platforms from different centers and a unified clot analog model should be used.
In addition to physical models, computational modelling is gaining attention and likely to have an increasing role in medical device development. For example, the INSIST project (IN-Silico trials for treatment of acute Ischemic Stroke) was recently launched for thrombectomy and thrombolysis. The INSIST project is developing a platform where computational simulations of thrombosis and thrombolysis, thrombectomy, perfusion, and brain tissue infarction are carried out on “virtual patients”.61 These “virtual patients” have clinically important characteristics such as clot properties, vessel geometries, and clinical record. However, accurately modelling the complex physiology, anatomy, and arterial response to mechanical loads remain a daunting challenge and the clinical value needs to be validated prospectively.
CONCLUSION
A combination of benchtop phantoms, animal models, and cadaveric models should be used to complement each other to get a comprehensive understanding of the failure modes of thrombectomy devices. The generation of new knowledge in thrombectomy mechanics and the next generation thrombectomy devices will require improved test platforms with more realistic anatomy, friction, flow conditions, and vessel wall response.
Funding Statement
This work was supported by National Institute of Health grant number NS105853.
Footnotes
Competing Interests Statement
LS is a co-founder and stake-owner of Endovascular Engineering, Inc., which develops thrombectomy technologies. YL serves on this company’s Scientific Advisory Board.
Ethics Approval
Ethics approval is not required as this is a review article analyzing publicly available literature data and does not involve animal or patient participants.
Data Sharing
The authors are willing to share any additional unpublished data upon reasonable request to the corresponding author.
REFERENCES
- 1.Palaniswami M, Yan B. Mechanical thrombectomy is now the gold standard for acute ischemic stroke: implications for routine clinical practice. Interv. Neurol 2015;4:18–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zaidat OO, Castonguay AC, Linfante I, Gupta R, Martin CO, Holloway WE, MuellerKronast N, English JD, Dabus G, Malisch TW, et al. First pass effect: A new measure for stroke thrombectomy devices. Stroke. 2018;49:660–666. [DOI] [PubMed] [Google Scholar]
- 3.Kleine JF, Wunderlich S, Zimmer C, Kaesmacher J. Time to redefine success? TICI 3 versus TICI 2b recanalization in middle cerebral artery occlusion treated with thrombectomy. J. Neurointerv. Surg 2017;9:117–121. [DOI] [PubMed] [Google Scholar]
- 4.Mehra M, Henninger N, Hirsch JA, Chueh J, Wakhloo AK, Gounis MJ. Preclinical acute ischemic stroke modeling. J. Neurointerv. Surg 2012;4:307–313. [DOI] [PubMed] [Google Scholar]
- 5.Herrmann AM, Meckel S, Gounis MJ, Kringe L, Motschall E, Mülling C, Boltze J. Large animals in neurointerventional research: A systematic review on models, techniques and their application in endovascular procedures for stroke, aneurysms and vascular malformations. J. Cereb. Blood Flow Metab 2019;39:375–394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Waqas M, Mokin M, Lim J, Vakharia K, Springer ME, Meess KM, Ducharme RW, Ionita CN, Nagesh SVS, Gutierrez LC, et al. Design and Physical Properties of 3-Dimensional Printed Models Used for Neurointervention: A Systematic Review of the Literature. Neurosurgery. 2020;87:445–453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Liu Y, Zheng Y, Reddy AS, Gebrezgiabhier D, Davis E, Cockrum J, Gemmete JJ, Chaudhary N, Griauzde J, Pandey AS, et al. Analysis of human emboli and thrombectomy forces in large vessel occlusion stroke. J. Neurosurg 2020;ahead of print. [DOI] [PubMed] [Google Scholar]
- 8.Reddy A, Liu Y, Cockrum J, Gebrezgiabhier D, Davis E, Zheng Y, Shih AJ, Pandey AS, Savastano LE. Construction of a Comprehensive Endovascular Test Bed for Research and Device Development in Mechanical Thrombectomy in Stroke. J. Neurosurg 2020;ahead of print. [DOI] [PubMed] [Google Scholar]
- 9.Gebrezgiabhier D, Liu Y, Reddy AS, Davis E, Zheng Y, Shih AJ, Pandey AS, Savastano LE. A human brain test bed for research in large vessel occlusion stroke. J. Neurosurg 2020;(In press). [DOI] [PubMed] [Google Scholar]
- 10.Liu Y, Zheng Y, Li ADR, Liu Y, Savastano LE, Shih AJ. Cutting of blood clots – Experiment and smooth particle Galerkin modelling. CIRP Ann. 2019;68:97–100. [Google Scholar]
- 11.Liu Y, Gebrezgiabhier D, Reddy AS, Davis E, Zheng Y, Arturo Larco JL, Shih AJ, Pandey AS, Savastano LE. Failure Modes and Effects Analysis of Mechanical Thrombectomy for Stroke Discovered in Human Brains. J. Neurosurg :(Accepted). [DOI] [PubMed] [Google Scholar]
- 12.Tennuci C, Pearce G, Wong J, Nayak S, Jones T, Lally F, Roffe C. Comparison of the effectiveness of three methods of recanalization in a model of the middle cerebral artery: Thrombus aspiration via a 4F catheter, thrombus aspiration via the gp thromboaspiration device, and mechanical thrombectomy using the solitaire th. Stroke Res. Treat 2011;2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Saleh M, Spence JN, Nayak S, Pearce G, Tennuci C, Roffe C. Safety and efficacy of the Aperio thrombectomy device when compared to the Solitaire AB/FR and the Revive devices in a pulsatile flow system. Am. J. Cardiovasc. Dis 2012;2:301–308. [PMC free article] [PubMed] [Google Scholar]
- 14.Chueh JY, Wakhloo AK, Gounis MJ. Neurovascular modeling: Small-batch manufacturing of silicone vascular replicas. AJNR Am. J. Neuroradiol 2009;30:1159–1164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chueh JY, Wakhloo AK, Gounis MJ. Effectiveness of mechanical endovascular thrombectomy in a model system of cerebrovascular occlusion. Am. J. Neuroradiol 2012;33:1998–2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chueh JY, Kühn AL, Puri AS, Wilson SD, Wakhloo AK, Gounis MJ. Reduction in distal emboli with proximal flow control during mechanical thrombectomy: A quantitative in vitro study. Stroke. 2013;44:1396–1401. [DOI] [PubMed] [Google Scholar]
- 17.Madjidyar J, Hermes J, Freitag-Wolf S, Jansen O. Stent-thrombus interaction and the influence of aspiration on mechanical thrombectomy: evaluation of different stent retrievers in a circulation model. Neuroradiology. 2015;57:791–797. [DOI] [PubMed] [Google Scholar]
- 18.Mokin M, Setlur Nagesh SV., Ionita CN, Levy EI, Siddiqui AH. Comparison of modern stroke thrombectomy approaches using an in vitro cerebrovascular occlusion model. Am. J. Neuroradiol 2015;36:547–551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ionita CN, Mokin M, Varble N, Bednarek DR, Xiang J, Snyder KV., Siddiqui AH, Levy EI, Meng H, Rudin S. Challenges and limitations of patient-specific vascular phantom fabrication using 3D Polyjet printing. In: SPIE. 2014. p. 90380M. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wenger K, Nagl F, Wagner M, Berkefeld J. Improvement of stent retriever design and efficacy of mechanical thrombectomy in a flow model. Cardiovasc. Intervent. Radiol 2013;36:192–197. [DOI] [PubMed] [Google Scholar]
- 21.Yoo AJ, Andersson T. Thrombectomy in Acute Ischemic Stroke : Challenges to Procedural Success. J. Stroke 2017;19:121–130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mordasini P, Frabetti N, Gralla J, Schroth G, Fischer U, Arnold M, Brekenfeld C. In vivo evaluation of the first dedicated combined flow-restoration and mechanical thrombectomy device in a swine model of acute vessel occlusion. Am. J. Neuroradiol 2011;32:294–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Nogueira RG, Levy EI, Gounis M, Siddiqui AH. The Trevo device: Preclinical data of a novel stroke thrombectomy device in two different animal models of arterial thromboocclusive disease. J. Neurointerv. Surg 2012;4:295–300. [DOI] [PubMed] [Google Scholar]
- 24.Simgen A, Kettner M, Webelsiep FJ, Tomori T, Mühl-Benninghaus R, Yilmaz U, Bhogal P, Laschke MW, Menger MD, Reith W, et al. Solitaire Stentectomy Using a Stent-Retriever Technique in a Porcine Model. Clin. Neuroradiol 2020; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gory B, Bresson D, Kessler I, Perrin ML, Guillaudeau A, Durand K, Ponsonnard S, Couquet C, Yardin C, Mounayer C. Histopathologic evaluation of arterial wall response to 5 neurovascular mechanical thrombectomy devices in a swine model. Am. J. Neuroradiol 2013;34:2192–2198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Yuki I, Kan I, Golshan A, Sohn J, Murayama Y, Vinters HV., Viñuela F. A swine model to analyze arterial structural changes induced by mechanical thrombectomy. Am. J. Neuroradiol 2013;34:8–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Shao Q, Zhu L, Li T, Li L, Li D, Zhang J, Ren W, Wu L. New method of thrombus preparation using a fl uid model for evaluation of thrombectomy devices in a swine model. Thromb. Res 2014;134:1087–1092. [DOI] [PubMed] [Google Scholar]
- 28.Zhu L, Shao Q, Li T, Saver JL, Li L, Li D, Zhao W, Jiang W. Evaluation of the JRecan device for thrombus retrieval: Efficacy and safety in a swine model of acute arterial occlusion. J. Neurointerv. Surg 2016;8:526–530. [DOI] [PubMed] [Google Scholar]
- 29.Jiang Y, Li Y, Xu X, Yu Y, Liu W, Liu X. An in vitro porcine model evaluating a novel stent retriever for thrombectomy of the common carotid artery. Catheter. Cardiovasc. Interv 2016;87:457–464. [DOI] [PubMed] [Google Scholar]
- 30.Srinivasan VM, Chen SR, Camstra KM, Chintalapani G, Kan P. Development of a recalcitrant, large clot burden, bifurcation occlusion model for mechanical thrombectomy. Neurosurg. Focus 2017;42:1–6. [DOI] [PubMed] [Google Scholar]
- 31.Peschillo S, Diana F, Berge J, Missori P. A comparison of acute vascular damage caused by ADAPT versus a stent retriever device after thrombectomy in acute ischemic stroke: A histological and ultrastructural study in an animal model. J. Neurointerv. Surg 2017;9:743–749. [DOI] [PubMed] [Google Scholar]
- 32.Sanchez S, Bailey L, Ducore R, Andersson T, Nogueira R, Cognard C, Ribo M, Villanova H, Rios A, Galve I. Preclinical evaluation of the ANCD thrombectomy device: Safety and efficacy in a swine clot model. J. Neurointerv. Surg 2020;1–6. [DOI] [PubMed] [Google Scholar]
- 33.Jahan R Solitaire flow-restoration device for treatment of acute ischemic stroke: Safety and recanalization efficacy study in a swine vessel occlusion model. Am. J. Neuroradiol 2010;31:1938–1943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ulm AJ, Khachatryan T, Grigorian A, Nogueira RG. Preclinical Evaluation of the NeVaTM Stent Retriever: Safety and Efficacy in the Swine Thrombectomy Model. Interv. Neurol 2018;37203:205–217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Johnston ME, Zheng Z, Maldjian JA, Whitlow CT, Morykwas MJ, Jung Y. Cerebral blood flow quantification in swine using pseudo-continuous arterial spin labeling. J. Magn. Reson. Imaging 2013;38:1111–1118. [DOI] [PubMed] [Google Scholar]
- 36.Wang HB, Laskowitz DT, Dodds JA, Xie GQ, Zhang PH, Huang YN, Wang B, Wu YF. Peak systolic velocity measurements with transcranial doppler ultrasound is a predictor of incident stroke among the general population in China. PLoS One. 2016;11:1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Akins PT, Amar AP, Pakbaz RS, Fields JD. Complications of endovascular treatment for acute stroke in the SWIFT trial with Solitaire and Merci devices. Am. J. Neuroradiol 2014;35:524–528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Klinger-gratz PP, Schroth G, Gralla J, Jung S, Weisstanner C, Verma RK, Mordasini P, Kellner-weldon F, Hsieh K, Heldner MR, et al. Protected stent retriever thrombectomy prevents iatrogenic emboli in new vascular territories. Neuroradiology. 2015;57:1045–1054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Rai AT, Hogg JP, Cline B, Hobbs G. Cerebrovascular geometry in the anterior circulation: An analysis of diameter, length and the vessel taper. J. Neurointerv. Surg 2013;5:371–375. [DOI] [PubMed] [Google Scholar]
- 40.Brooks OW, King RM, Nossek E, Marosfoi M, Caroff J, Chueh JY, Puri AS, Gounis MJ. A canine model of mechanical thrombectomy in stroke. J. Neurointerv. Surg 2019;11:1243–1248. [DOI] [PubMed] [Google Scholar]
- 41.Park S, Hwang SM, Song JS, Suh DC, Lee DH. Evaluation of the solitaire system in a canine arterial thromboembolic occlusion model: Is it safe for the endothelium? Interv. Neuroradiol 2013;19:417–424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Fukushima U, Sasaki S, Okano S, Takase K, Hagio M. The Comparison between the Cerebral Blood Flow Directly Measures and Cerebral Blood Flow Velocity in the Middle and Basilar Cerebral Arteries Measured by Transcranial Doppler Ultrasonography. J. Vet. Med. Sci 1999;61:1293–1297. [DOI] [PubMed] [Google Scholar]
- 43.Dahl A, Russell D, Nyberg-Hansen R, Rootwelt K. A comparison of regional cerebral blood flow and middle cerebral artery blood flow velocities: Simultaneous measurements in healthy subjects. J. Cereb. Blood Flow Metab 1992;12:1049–1054. [DOI] [PubMed] [Google Scholar]
- 44.Gounis MJ, Nogueira RG, Mehra M, Chueh J, Wakhloo AK. A thromboembolic model for the efficacy and safety evaluation of combined mechanical and pharmacologic revascularization strategies. J. Neurointerv. Surg 2013;5:i85–i89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Arai D, Ishii A, Chihara H, Ikeda H, Miyamoto S. Histological examination of vascular damage caused by stent retriever thrombectomy devices. J. Neurointerv. Surg 2016;8:992–995. [DOI] [PubMed] [Google Scholar]
- 46.Haider T, Plasenzotti R, Bergmeister H, Mach G, Kleinpeter G, Aguilar-Perez M, Sherif C. New mechanical thrombectomy model in the rabbit: A feasibility study. J. Neurosci. Methods 2016;271:139–142. [DOI] [PubMed] [Google Scholar]
- 47.Windberger U, Bartholovitsch A, Plasenzetti R, Korak KJ, Heinze G. Whole blood viscosity, plasma viscosity and erythrocyte aggregation in nine mammalian species: Reference values and comparison of data. Exp. Physiol 2003;88:431–440. [DOI] [PubMed] [Google Scholar]
- 48.Den Dekker WK, Tempel D, Speelman L, Huizingh J, Ramos A, Gijsen FJ, Wentzel JJ, Cheng C, Duckers HJ. Effect of shear stress alteration on atherosclerotic plaque vulnerability in cholesterol-fed rabbits. Vasc. Med 2014;19:94–102. [DOI] [PubMed] [Google Scholar]
- 49.Fitzgerald S, Ryan D, Thornton J, Nogueira RG. Preclinical evaluation of Millipede 088 intracranial aspiration catheter in cadaver and in vitro thrombectomy models. J. Neurointerv. Surg 2020;1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Fitzgerald S, Dai D, Wang S, Douglas A, Kadirvel R, Layton KF, Thacker IC, Gounis MJ, Chueh JY, Puri AS, et al. Platelet-Rich Emboli in Cerebral Large Vessel Occlusion Are Associated with a Large Artery Atherosclerosis Source. Stroke. 2019;50:1907–1910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Duffy S, Farrell M, Mcardle K, Thornton J, Vale D, Rainsford E, Morris L, Liebeskind DS, Maccarthy E, Gilvarry M. Novel methodology to replicate clot analogs with diverse composition in acute ischemic stroke. J. Neurointerv. Surg 2017;9:486–491. [DOI] [PubMed] [Google Scholar]
- 52.Liu Y, Reddy AS, Cockrum J, Ajulufoh M, Zheng Y, Shih AJ, Pandey AS, Savastano LE. Standardized Fabrication Method of Human-Derived Emboli with Histologic and Mechanical Quantification for Stroke Research. J. Stroke Cerebrovasc. Dis 2020;29:105205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Chueh JY, Wakhloo AK, Hendricks GH, Silva CF, Weaver JP, Gounis MJ. Mechanical characterization of thromboemboli in acute ischemic stroke and laboratory embolus analogs. AJNR Am. J. Neuroradiol 2011;32:1237–1244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Chueh J, Puri AS, Wakhloo AK, Gounis MJ. Risk of distal embolization with stent retriever thrombectomy and ADAPT. J. Neurointerv. Surg 2016;8:197–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.US Food and Drug Administration. Guidance for Industry and FDA Staff: Pre-Clinical and Clinical Studies for Neurothrombectomy Devices. 2007.
- 56.Krings T, Mandell DM, Kiehl TR, Geibprasert S, Tymianski M, Alvarez H, TerBrugge KG, Hans FJ. Intracranial aneurysms: From vessel wall pathology to therapeutic approach. Nat. Rev. Neurol 2011;7:547–559. [DOI] [PubMed] [Google Scholar]
- 57.Heider DM, Simgen A, Wagenpfeil G, Dietrich P, Yilmaz U, Mühl-Benninghaus R, Roumia S, Faßbender K, Reith W, Kettner M. Why we fail: mechanisms and co-factors of unsuccessful thrombectomy in acute ischemic stroke. Neurol. Sci 2020;41:1547–1555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Teng D, Pannell JS, Rennert RC, Li J, Li YS, Wong VW, Chien S, Khalessi AA. Endothelial Trauma from Mechanical Thrombectomy in Acute Stroke: In Vitro Live-Cell Platform with Animal Validation. Stroke. 2015;46:1099–1106. [DOI] [PubMed] [Google Scholar]
- 59.Staessens S, Fitzgerald S, Andersson T, Clarençon F, Denorme F, Gounis MJ, Hacke W, Liebeskind DS, Szikora I, van Es ACGM, et al. Histological stroke clot analysis after thrombectomy: Technical aspects and recommendations. Int. J. Stroke 2020;15:467–476. [DOI] [PubMed] [Google Scholar]
- 60.Staessens S, Denorme F, François O, Desender L, Dewaele T, Vanacker P, Deckmyn H, Vanhoorelbeke K, Andersson T, De Meyer SF. Structural analysis of ischemic stroke thrombi: Histological indications for therapy resistance. Haematologica. 2020;105:498–507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Konduri PR, Marquering HA, van Bavel EE, Hoekstra A, Majoie CBLM. In-Silico Trials for Treatment of Acute Ischemic Stroke. Front. Neurol 2020;11:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Fargen KM, Mocco J, Gobin YP. The lazarus funnel: A blinded prospective randomized in vitro trial of a novel CE-marked thrombectomy assist device. J. Neurointerv. Surg 2016;8:66–68. [DOI] [PubMed] [Google Scholar]
- 63.Van Der Marel K, Chueh JY, Brooks OW, King RM, Marosfoi MG, Langan ET, Carniato SL, Gounis MJ, Nogueira RG, Puri AS. Quantitative assessment of device-clot interaction for stent retriever thrombectomy. J. Neurointerv. Surg 2016;8:1278–1282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Chueh JY, Puri AS, Gounis MJ. An in vitro evaluation of distal emboli following Lazarus Cover-assisted stent retriever thrombectomy. J. Neurointerv. Surg 2017;9:183–187. [DOI] [PubMed] [Google Scholar]
- 65.Larsen N, Oberbeck K, Lima De Miranda R, Trentmann J, Madjidyar J, Quandt E, Jansen O. Comparison of Efficacy, Embolism Rate and Safety of Thrombectomy with Stent Retrievers in an Anterior Circulation Stroke Model. RoFo Fortschritte auf dem Gebiet der Rontgenstrahlen und der Bildgeb. Verfahren 2018;190:1053–1058. [DOI] [PubMed] [Google Scholar]
- 66.Madjidyar J, Pineda Vidal L, Larsen N, Jansen O. Influence of Thrombus Composition on Thrombectomy: ADAPT vs. Balloon Guide Catheter and Stent Retriever in a Flow Model. RöFo - Fortschritte auf dem Gebiet der Röntgenstrahlen und der Bildgeb. Verfahren 2019; [DOI] [PubMed] [Google Scholar]
- 67.Arslanian RA, Marosfoi M, Caroff J, King RM, Raskett C, Puri AS, Gounis MJ, Chueh JY. Complete clot ingestion with cyclical ADAPT increases first-pass recanalization and reduces distal embolization. J. Neurointerv. Surg 2019;11:931–936. [DOI] [PubMed] [Google Scholar]
- 68.Johnson S, McCarthy R, Fahy B, Mereuta OM, Fitzgerald S, Gaudirc J, Remadi JP, Shotar E, Sourour NA, Doyle K, et al. Development of an in vitro model of calcified cerebral emboli in acute ischemic stroke for mechanical thrombectomy evaluation. J. Neurointerv. Surg 2020;1–6. [DOI] [PubMed] [Google Scholar]
- 69.Mokin M, Ionita CN, Nagesh SVS, Rudin S, Levy EI, Siddiqui AH. Primary stentriever versus combined stentriever plus aspiration thrombectomy approaches: In vitro stroke model comparison. J. Neurointerv. Surg 2015;7:453–457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Mokin M, Nagesh SVS, Ionita CN, Mocco J, Siddiqui AH. Stent retriever thrombectomy with the Cover accessory device versus proximal protection with a balloon guide catheter: In vitro stroke model comparison. J. Neurointerv. Surg 2016;8:413–417. [DOI] [PubMed] [Google Scholar]
- 71.Fennell VS, Setlur Nagesh SV, Meess KM, Gutierrez L, James RH, Springer ME, Siddiqui AH. What to do about fibrin rich “tough clots”? Comparing the Solitaire stent retriever with a novel geometric clot extractor in an in vitro stroke model. J. Neurointerv. Surg 2018;10:907–910. [DOI] [PubMed] [Google Scholar]
- 72.Gory B, Bresson D, Rouchaud A, Yardin C, Mounayer C. A novel swine model to evaluate arterial vessel injury after mechanical endovascular thrombectomy. Interv. Neuroradiol 2013;19:147–152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Wainwright JM, Jahan R. Solitaire FR revascularization device 4×40: Safety study and effectiveness in preclinical models. J. Neurointerv. Surg 2016;8:710–713. [DOI] [PubMed] [Google Scholar]
- 74.Jankowitz BT, Gross BA, Mintz E, Jalgaonkar U, Marchesiello D, Girdhar G, Jadhav AP, Jovin TG. Safety and Efficacy Evaluation of Aspiration Thrombectomy With Large Bore Catheters in a Porcine Model. World Neurosurg. 2019;132:e409–e417. [DOI] [PubMed] [Google Scholar]
- 75.Sanchez S, Cortiñas I, Villanova H, Rios A, Galve I, Andersson T, Nogueira R, Jovin T, Ribo M. ANCD thrombectomy device: In vitro evaluation. J. Neurointerv. Surg 2020;12:77–81. [DOI] [PubMed] [Google Scholar]
- 76.Zhang Y, Jin M, Du B, Lin H, Xu C, Jiang W, Jia J. A novel canine model of acute vertebral artery occlusion. PLoS One. 2015;10:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]