

Summary
Childhood obesity is a major problem in Latin America and among US Latinos. Effective public health policies require contextually relevant evidence to guide them, which demands sustained research capacity. The objectives of this study are to determine research productivity in Latin America and in the United States focused on Latino populations and examine domains of research capacity (research infrastructure, training programs, mentoring, funding, and networks). We conducted a scoping review of indexed childhood obesity‐related articles published June 2015–December 2019. We collected data on perceptions of capacity for childhood obesity research among Latin American investigators through an online survey. We identified 612 childhood obesity‐related articles (505 from Latin America, 124 from the United States, and 17 US–Latin America collaborations). Brazil, Mexico, Chile, Colombia, and the United States are the top publishing countries. There are similar numbers of obesity, nutrition, and physical activity articles, but physical activity research capacity lagged in other domains (research training, funding, and networking opportunities). Complementary research areas, including sedentary behavior, systems science, and policy studies, are uncommon in Latin America but more prevalent in the United States, whereas sleep research is nascent across settings. Realizing the promise of an effective cross‐border collaborative childhood obesity prevention agenda will require committed investment in all domains of research capacity and across all relevant topics.
Keywords: capacity building, childhood obesity, Latin America, Latino populations, research infrastructure
1. INTRODUCTION
Childhood obesity is a major unresolved public health problem in Latin America and among US Latinos. It is estimated that 20% to 25% of Latin American children have overweight or obesity,1 while 25.8% of Latino children in the United States have obesity.2
Latin American countries have many commonalities. The region continues to have stark inequalities, with widespread poverty and its associated conditions (undernutrition, sanitation problems, and infectious diseases).3 This, coupled with political instability, and sometimes conflict, crime, and violence, has favored multiple waves of local (e.g., rural–urban), regional (within Latin America) and global (e.g., Latin America to the United States) migrations over the past century.4 At the same time, Latin American countries have undergone several interrelated, rapid transitions (economic, demographic, epidemiological, nutritional, and in physical activity), resulting in the co‐existence of high levels of communicable and non‐communicable diseases.5, 6, 7 This context is important for understanding the drivers of childhood obesity in the region, as well as among US Latinos. Over a third of all US‐based Latinos are foreign‐born,8 that is, they come from places with the contextual background described above. Similarly, contextual factors influencing childhood obesity among US Latino populations include socioeconomic disparities resulting in persistent health inequalities.9
Effective public health programs and policies require contextually relevant evidence and local experts to guide them.10 Achieving sustained research productivity for documenting, understanding, and resolving the childhood obesity epidemic in Latin America and among US Latino populations requires local research capacity in all relevant sub‐fields. Research capacity is defined as “the ability of individuals, institutions and networks to pursue locally relevant research, maintain a career pipeline for scientists and promote a research environment that is conducive to multidisciplinary collaboration.”11, 12 Beyond dietary and physical activity research, sedentary behavior and sleep research (i.e., movement behaviors) have recently emerged as relevant sub‐fields for childhood obesity research.13, 14
In 2017, Parra et al. published a review examining research productivity by Latin American authors between 2010 and May 2015 and found that obesity and nutrition research were more developed than the study of physical activity and sedentary behavior.11 Childhood obesity research in Latin America was found to rely heavily on cross‐sectional studies. An equivalent review focused on US‐based childhood obesity studies of Latinos is not available. However, there are several examples of observational and experimental studies addressing childhood obesity among Latinos in the United States, indicating that the field is at a more advanced stage in the United States.15
Establishing a cohesive regional agenda integrating the 26 countries comprising Latin America, and the United States, given its 56.5 million Latinos,8 can help accelerate childhood obesity prevention efforts across the region. However, fair, effective, and sustainable cross‐national collaborations require a “level playing field” for all involved parties. Existing gaps in research capacity across the region must be documented and addressed to optimize cross‐national collaborative efforts. On the other hand, cross‐national collaborations in and of themselves can become part of the solution, as they can serve as catalysts for capacity building.11, 16, 17
Through this paper, we aim to determine the current status of research productivity across the region and to expand the diagnosis of research capacity for Latin American childhood obesity research to include (1) sleep research as a key sub‐field of relevance to childhood obesity prevention and (2) the examination of additional domains of research capacity beyond the quantification of indexed, peer‐reviewed articles (research infrastructure/human capital, training programs, mentoring, funding, and networking opportunities). We also include a general scope of the status of Latino‐focused childhood obesity research publications in the United States since June 2015. With this work, we seek to identify gaps and highlight opportunities to strengthen childhood obesity research in Latin America and the United States and underline the critical role of contextually targeted capacity‐building efforts for fostering a cross‐national childhood obesity prevention agenda across the region.
2. METHODS
We conducted a scoping review of the childhood obesity‐related peer‐reviewed literature from Latin America, or with focus on US Latino children, published between June 2015 and December 2019. Additionally, we collected data on the perceptions of research capacity for childhood obesity and related sub‐fields research among Latin American investigators, via an online survey.
2.1. Scoping review
2.1.1. Systematic search and abstraction
We followed the PRISMA guidelines for systematic scoping reviews,18 a methodology that aims to provide a general overview of the state of the science of a field of study.19
The search was conducted in April of 2020 using the PubMed and LILACS bibliographic databases. First, we defined search term categories and, within each, multiple variants of each term. Our search term categories included “obesity,” “nutrition,” “physical activity,” “sedentary behavior,” “sleep,” “childhood,” “Latin America,” “United States,” and “Latino populations.” The “Latin America” terms included the names of all Latin American countries (excluding non‐Latin Caribbean countries) and variants (e.g., Argentina and Argentinians). Likewise, the “United States” terms included the names of all the states and territories and their variants (e.g., Texas and Texan*). Next, we implemented the following search algorithm: (1) the title of the article must contain an “obesity” or “nutrition” or “physical activity” or “sedentary behavior” or “sleep” search term or variant; (2) the title of the article must contain a “childhood” term or variant; (3) the title or abstract must contain a “Latin America” term/variant, or, a “United States” term/variant plus a “Latino populations” term/variant. The search was conducted in English, Spanish, and Portuguese and was restricted to articles published after June 2015. This date was selected because the Parra et al. review covered research published through May 2015.11
After running the initial search, duplicates and non‐eligible documents were removed. This included reports, books, book chapters, non‐peer reviewed or indexed articles (i.e., pre‐prints), opinions, editorials, letters to the editor, and theses or dissertations. Next, two reviewers performed a title and abstract scan of the remaining articles for identifying non‐relevant articles for abstraction. This included removal of articles without an explicit focus on an obesity‐related topic (obesity, nutrition, physical activity, sedentary behavior, or sleep). Obesity‐themed articles were defined as those using weight, body mass index (BMI) status or body composition as the outcome or exposure. Nutrition articles were those for which dietary intake, dietary behaviors, or dietary patterns (inclusive of breastfeeding practices) were outcomes or exposures in the analysis. The physical activity and sedentary behavior topics included articles using overall or domain‐specific physical activities and sedentary time, respectively, as outcomes or exposures. Sleep articles included those using measures of sleep duration or sleep quality as outcomes or exposures. In this phase, we also identified articles not including children and adolescents (under 18 years of age) or for which results for these groups were not reported separately from those of other age groups. We also removed articles reporting research that was not conducted in Latin America or the United States. US‐based articles were deemed ineligible if Latino populations were not central to the study. Studies of predominantly Latino samples, conducted in predominantly Latino areas, or contrasting Latino groups to other racial or ethnic groups in the United States as part of their central theme were included for abstraction. Articles focused exclusively on undernutrition or micronutrient deficiencies were excluded.
Data on the following characteristics were abstracted for all eligible articles: author characteristics (country of affiliation of first author, gender of first and senior authors, whether the first and senior authors hold doctorates [PhD, DrSc, DrPH, or MD]), study site (country), research type (health effects, measurement and surveillance, correlates and determinants, interventions, and policy), research topic (obesity, nutrition, physical activity, sedentary behavior, and sleep), and study design/methods (ecological, cross‐sectional, case–control, cohort, experimental, reviews, qualitative, and systems science). Studies could be classified as being about more than one research topic. Five pairs of authors were assigned for this task. Both members of each team abstracted the data for all assigned articles. The coded data from each team were compiled, and an agreement analysis was performed. Kappa agreement statistics were calculated for each pair and ranged from 0.79 to 0.90. All discrepancies were resolved by a third reviewer.
2.1.2. Analysis
We used the data gleaned from the scoping review to derive indicators of research productivity, research infrastructure (human capital), and cross‐national collaborations.
Peer‐reviewed, indexed publications objectively quantify research productivity, a direct result of research capacity. As such, the number of peer‐reviewed, indexed articles on a given topic is a good bibliometric indicator of overall research capacity for a given field.11, 20 Using the scoping review data, we calculated the absolute and per capital (per million inhabitants) number of peer‐reviewed, indexed publications on childhood obesity‐relevant topics between June 2015 and April 2020.
Using the Cartogram Geoprocessing Tool21 in ArcMap v10.6 (ESRI, ArcGIS Desktop, Redlands, CA, USA), we built a series of density equalizing cartograms to contrast population size by country with overall and topic‐specific research productivity across Latin America. We also built heat maps depicting the cross‐tabulation of articles by topic (as previously defined) and research type (health effects, measurement and surveillance, correlates and determinants, interventions, and policy) for the four Latin American countries with most indexed articles on childhood obesity and related topics, which comprised 84.4% of all Latin American articles (Brazil, Mexico, Chile, and Colombia), and the United States. The types of research were ordered according to the stages of Sallis et al.'s behavioral epidemiology framework,22 which poses that any health behavior field (e.g., dietary behaviors, physical activity, sedentary behavior, or sleep) should build evidence in five progressive stages: (1) demonstrating the adverse or beneficial health effects of the behavior, (2) developing measures and surveillance systems for the behavior, (3) identifying the correlates and determinants of the behavior, (4) designing and testing interventions to positively change the behavior, and (5) translating evidence into policies. Although in reality, research rarely occurs in a linear fashion, understanding how research is distributed across these stages is helpful for assessing the level of maturity of a field in a given place or region. Heat maps were developed using Python v3.7, via the Matplotlib and Seaborn 0.10 packages.
Research infrastructure (human capital) is also a critical element of strong research capacity.23 Human capital includes the extent to which skills and knowledge are accessed fully across the labor force, including both women and men. We calculated the following indicators using data from the scoping review: proportion of first and senior authors of indexed peer‐reviewed articles on childhood obesity‐related topics with a doctorate (included PhD, DrSc, DrPH, and MD); proportion of childhood obesity‐related articles in which neither the first nor the senior author reside in the country where the research took place (based on primary affiliations); and proportion of childhood obesity‐related articles in which a woman was either the lead or the senior author.
Finally, given the important role that international collaborations are known to have for the growth of research in a region,17 we used scoping review data to derive two indicators of cross‐national collaborations for childhood obesity research: the proportion of peer‐reviewed articles on childhood obesity‐related topics published between June 2015 and April 2020 (per the scoping review) of studies involving more than one Latin American country (multi‐site Latin American collaborations, i.e., “south–south” collaborations); and the proportion of studies involving collaborations between Latin American countries and the United States (multi‐site Latin American–US collaborations, i.e., north–south collaborations).
2.2. Online survey
2.2.1. Survey development and data collection
We administered an online survey of perceptions of research capacity among Latin American childhood obesity investigators to obtain information on additional research capacity domains. Eligibility criteria for completing the survey included (1) being a self‐identified obesity, nutrition, physical activity, sedentary behavior, and/or sleep investigator, who is (2) a part of active research projects involving children/adolescent populations (<18 years), and (3) resides and works in Latin America.
The survey was developed and pilot tested by the author team and translated to Spanish and Portuguese. Data were collected using the Qualtrics online platform. Dissemination took place via the official listserves, websites, and social media of several prestigious Latin American research societies and networks, including the Latin American Society of Nutrition, the Americas Network for Chronic Disease Surveillance, the Latin American Congress of Physical Activity and Health Research, the Physical Activity Network of the Americas, the Global Observatory for Physical Activity, and multiple country‐level and institutional networks. Survey data were collected during May of 2020. This study was deemed exempt by the Institutional Review Board of Washington University in St. Louis.
2.2.2. Analysis
We derived a series of indicators for each domain of research capacity included in the survey and calculated descriptive statistics (counts and percentages).
Perceived Research Infrastructure (human capital) was examined by calculating the proportion of Latin American childhood obesity researchers with a bachelor, master, or doctoral degree as their terminal level of education; years of research experience among childhood obesity investigators in Latin America; proportion of Latin American childhood obesity researchers reporting expertise on obesity, nutrition, physical activity, sedentary behavior, and sleep research; and proportion of Latin American researchers working in academia, government entities, the private sector, and non‐governmental organizations.
Another important component for building strong local capacity for research is the quantity and quality of advanced training programs for all fields of relevance.16, 24 Data from the online survey were used to build the following indicators: proportion of Latin American childhood obesity researchers reporting that all of their formal training took place in their own country; proportion of Latin American childhood obesity researchers reporting some formal training in another Latin American country beyond their own; proportion of Latin American childhood obesity researchers reporting some formal training in a high‐income country outside of Latin America (includes the United States, Canada, European countries, Australia, and New Zealand); and proportion of Latin American childhood obesity researchers whose current institution host doctoral training programs with focus on nutrition, physical activity and/or sleep. We also calculated the proportion of Latin American childhood obesity researchers perceiving sufficient availability of doctoral programs in nutrition and physical activity in their country, and the proportion of respondents perceiving that their country offers high‐quality doctoral programs in nutrition and physical activity. These last two indicators were derived from a 4‐point Likert scale of agreement, by combining the “strongly agree” and “agree” responses.
There is robust evidence demonstrating the important role of mentoring for academic success and for establishing research capacity in a growing field.25 We included four indicators for gauging the perceived mentoring environment for childhood obesity research in Latin America, derived from 4‐point Likert scale‐based survey items. The proportion of respondents who reported to either strongly agree or agree with the following statements about their institution was calculated: “there are formal mentoring mechanisms/policies in place”; “established researchers spend sufficient time mentoring early career researchers”; “all students and trainees specializing in childhood obesity find experienced mentors in their sub‐area of interest” (sub‐areas can include obesity, nutrition, physical activity, sedentary behavior, sleep, or methodological approaches like systems science, etc.); and “all students and trainees specializing in childhood obesity have the necessary resources and support to become independent investigators.”
Another domain of research capacity is funding. The allocation of resources to different fields of study can reflect the current public health priorities of a country or region.26 We estimated perceived availability of research funding in Latin America for childhood obesity‐related topics by computing the proportion of survey respondents either strongly agreeing or agreeing that their country has sufficient funding opportunities to support childhood obesity research with a focus on (1) nutrition, (2) physical activity/sedentary behavior, (3) sleep, and (4) multi‐disciplinary approaches for prevention and control (of childhood obesity).
Finally, networking opportunities such as those provided by scientific gatherings are another critical element of research capacity as these provide opportunities to build new local and cross‐national collaborations.11, 17, 23 We used survey data to calculate the proportion of Latin American childhood obesity researchers (survey respondents) reporting that their country has scientific societies or groups hosting recurring gatherings/meetings/conferences/workshops/events centered on childhood obesity, nutrition, physical activity, and/or sleep.
3. RESULTS
The scoping review yielded 612 unique indexed, peer‐reviewed papers eligible for abstraction (Figure S1). Of these, 505 were of childhood obesity studies conducted in Latin America (82.5%), and 124 (20.3%) were of Latino‐focused research in the United States, with 17 papers (2.8%) reporting on studies with both Latin American and US sites (i.e., north–south collaborations).
3.1. Childhood obesity research production in Latin America
Of the total 505 articles from Latin America, 227 (45.0%; 1.1 articles per million inhabitants) reported research from Brazil, 103 (20.4%; 0.8 articles per million inhabitants) from Mexico, 73 (14.5%; 3.9 articles per million inhabitants) from Chile, and 39 (7.7%; 0.8 articles per million inhabitants) from Colombia. Together, childhood obesity papers involving these four countries accounted for 84.4% of all Latin American articles.
Among all childhood obesity‐related articles reporting research conducted in Latin America (n = 505), 269 (53.3%) were on obesity, 142 (28.1%) on nutrition, 162 (32.1%) on physical activity, 63 (12.5%) on sedentary behavior, and 32 (6.3%) on sleep. Because articles could be coded as having more than one central topic, these are not mutually exclusive groups.
Figure 1 shows differences in the geographic patterns of research productivity by childhood obesity‐related topic across Latin America. In an ideal scenario, research productivity would be proportional to population size by country (Panel B). Hence, a country area in Panels D–H (scaled by number of articles per country by topic) larger than the area of the same country in Panel B (scaled by population size) denotes relatively high research productivity, while a country area in Panels D–H, which is smaller than the area shown in Panel B for the same country, denotes relatively low research productivity.
FIGURE 1.
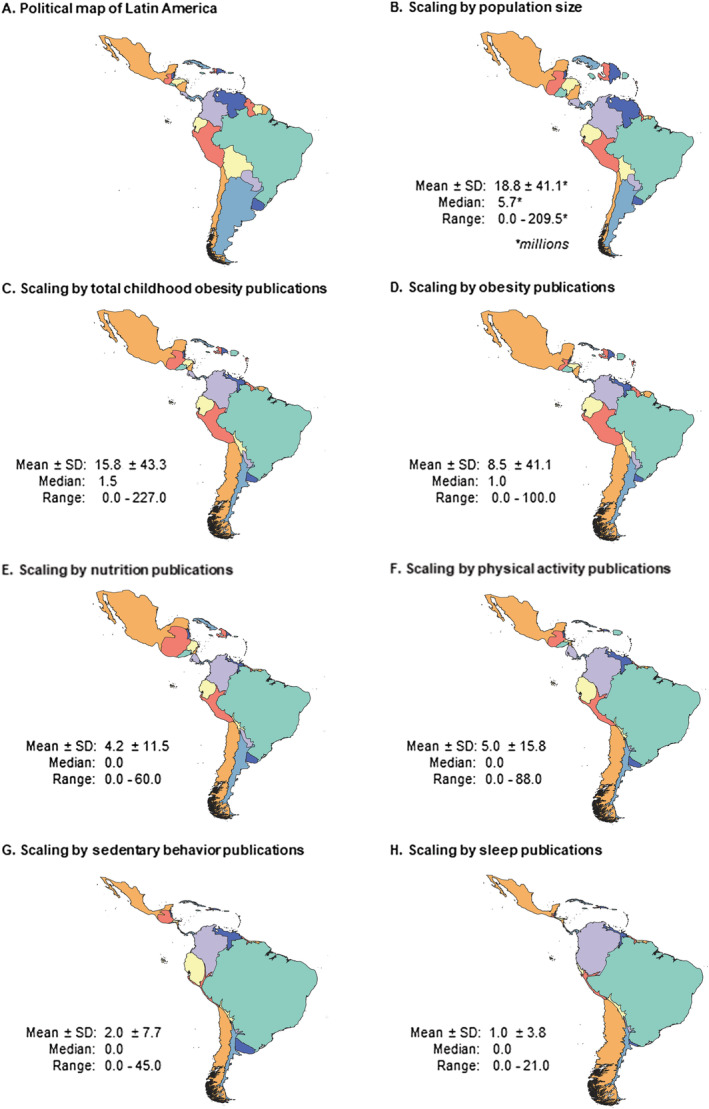
Childhood obesity‐related peer‐reviewed publications in Latin American countries (June 2015 to April 2020): density equalizing cartograms of population size and research productivity by country and topic. Countries with a larger area in Panels C–H than in Panel B have higher than expected research productivity, while countries with a smaller area in Panels C–H than in Panel B have lower than expected research productivity
Brazil is leading in research productivity across all topics of relevance for childhood obesity research. Meanwhile, Mexico's leadership in childhood obesity research in the region is mainly driven by a high production of obesity‐ and nutrition‐centered articles. However, Mexico has lower productivity in physical activity, sedentary behavior, and sleep research. Meanwhile, Colombia's area in the cartogram scaled by its population size (Figure 1B) is similar to the country's area when scaled by obesity‐centered publications and by nutrition‐centered publications (Figure 1D,E), suggesting an adequate amount of research productivity in those topics. Colombia was also found to have a high number of publications on physical activity, sedentary behavior, and sleep in comparison with other countries in the region. Likewise, Chile was found to be a leading country in childhood obesity research productivity across all relevant topics, with disproportionately high publication rates given its population size.
Other countries, which are not among the top publishers of overall childhood obesity‐related articles had a disproportionately high publication rate for specific topics. Such was the case of Peru for obesity‐centered publications and of Guatemala for nutrition‐centered work. Likewise, Ecuador appears to be publishing an adequate number of articles on obesity, nutrition, and physical activity given its population size and a high number of articles on sedentary behavior articles. Multiple countries across the region have low research outputs across all topics of relevance for childhood obesity, even while accounting for their population size (e.g., Argentina, which is fourth in population size in the region, had only 0.3 childhood obesity publications per million inhabitants).
Finally, a very low amount of research is being conducted on the topics of sedentary behavior and sleep within the context of childhood obesity research across Latin America, with a large number of countries virtually disappearing from the maps depicting research productivity in these fields (Figure 1G,H).
3.2. Latino‐focused childhood obesity research production in the United States
We identified 124 articles on Latino‐focused childhood obesity research from the United States, representing 2.2 articles per million Latino inhabitants in the United States. Of the total US articles, 66 (53.2%) had a central emphasis on obesity, 32 (25.8%) on nutrition, 38 (30.6%) on physical activity, and 11 (8.9%) on both sedentary behavior and sleep, respectively. In terms of geography, childhood obesity research with focus on Latino populations was most common in Texas (n = 30, 24.2%; second state with most Latinos; 4.5 articles per million Latino inhabitants) and California (n = 27, 21.8%; first US state with most Latinos; 2.5 articles per million Latino inhabitants). Twenty‐two additional states had a small number of publications. Additional data on Latino‐focused childhood obesity research production in the United States are available in Table S1.
3.3. Research productivity in leading Latin American countries and the United States by type of research and study design
The heat maps in Figure 2 show the relative occurrence of childhood obesity research topics for Brazil, Chile, Mexico, and Colombia (the countries with the most childhood obesity‐related publications in Latin America) and the United States. The majority of childhood obesity research in the four leading Latin American countries is stemming from studies about obesity, nutrition, and physical activity and is positioned in the first three stages of the behavioral epidemiological framework (health effects, surveillance and measurement, and correlates/determinants).22 In contrast, in the United States, the occurrence of intervention and policy research (the more advanced stages of the behavioral epidemiology framework22) on obesity, nutrition, and physical activity is relatively high. Some exceptions of higher production of research in the more advanced stages of the behavioral epidemiology framework in Latin America are country and topic specific, highlighting the importance of examining country‐level variations. Chile has relatively high levels of physical activity intervention research, while Mexico does so for obesity and nutrition articles. Meanwhile, Brazil, Colombia, and the United States are leading works on sedentary behavior, but this is mainly occurring through studies about correlates and determinants.
FIGURE 2.
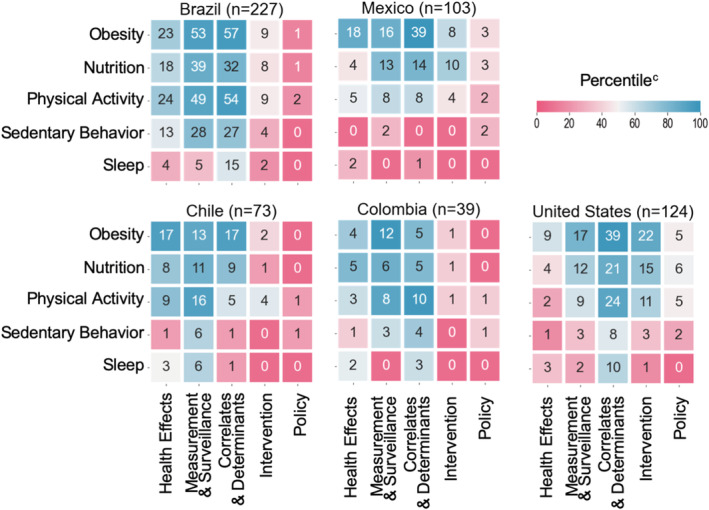
Heat map of the distribution of childhood‐obesity related publications in leading Latin American countries for childhood obesity prevention researcha and the United Statesb, by topic and type of study (June 2019 to April 2020). Blue indicates a relatively high proportion of articles in the given “topic‐by‐research type” combination. Red indicates a relatively low proportion of articles in the given “topic‐by‐research type” combination. Research types are ordered by the stages of the behavioral epidemiology framework by Sallis et al.22 ranging from early research stages (health effects, measurement, and surveillance) to mature research stages (intervention and policy research). aBrazil, Mexico, Chile and Colombia comprise 84.4% or all Latin America of childhood obesity‐related indexed scientific articles. bLatino‐focused childhood obesity research only. cThe sliding color scale depicts percentiles based on normalized cell counts (proportions) pooled from across all five countries (Brazil, Mexico, Chile, Colombia, and the United States). The numbers in the cells are number of articles
Cross‐sectional study designs were the most prevalent across countries. However, there was a notable difference between the United States and Latin America as a whole, with 45.2% and 70.9% of studies being cross‐sectional, respectively. Cohort studies constituted 16.1% of US Latino‐focused childhood obesity‐related work, versus 9.1% across all Latin American countries. Experimental study designs were employed in 19.4% of articles from the United States, versus in 8.5% in Latin American countries. Qualitative studies were also more commonly found in the United States (15.3% vs. 5.3% in Latin America), with Colombia being the country in Latin America with most research using this methodology (10.3%). Although our abstraction criteria included the use of systems (complexity) science methods, our scoping review did not find any childhood obesity study across all countries employing this type of methodology. The distribution of study designs among the leading Latin American countries in childhood obesity research productivity and the United States are shown in Figure S2.
3.4. Characteristics of childhood obesity research leaders (research infrastructure) and cross‐country collaborations
Table 1 summarizes key characteristics of researchers leading childhood obesity research in Latin America and the United States (with Latino population focus). In 13.3% of the total articles of childhood obesity‐related research from Latin America and in 9.7% of Latino‐focused US articles, neither the first nor the senior author had a primary affiliation in the country where the research took place. Furthermore, among the countries with at least 10 published articles since June 2015, this indicator ranged from 7.1% in Argentina to 58.3% in Guatemala. High numbers in this indicator denote limited local expertise or, alternatively, lack of leadership in multi‐site, international studies, for which investigators from another site are serving as leaders. As for advanced training among those conducting this type of work, a higher number of childhood obesity investigators had advanced training (doctorate) in the United States as compared with Latin America (86.3% vs. 70.5% for first authorship, and 88.7% vs. 82.0% for senior authorship). Among all Latin American countries, 59.6% of first authors of childhood obesity‐related articles and 40.2% of senior authors were women, while in the United States, this occurred in 79.8% and 62.1% of the time, respectively.
TABLE 1.
Authorship characteristics and international collaborations in Latin American childhood obesity researcha: scoping review of childhood obesity articles from Latin America and of US Latino populationsb published between 2015 and 2019
| Number of childhood obesity articles n (articles per million inhabitants) | Neither first nor senior author are from country % | Female first author % | Female senior author % | First author has a doctorate % | Senior author has a doctorate % | Multi‐country study: Latin American collaboration % | Multi‐country study: Latin America and US collaboration % | |
|---|---|---|---|---|---|---|---|---|
| Latin America | 505 (0.8) | 13.3 | 59.6 | 40.2 | 70.5 | 82.0 | 3.0 | 3.2 |
| Argentina | 14 (0.3) | 7.1 | 85.7 | 64.3 | 85.7 | 78.6 | 8.3 | 0.0 |
| Bolivia | 3 (0.3) | 66.7 | 66.7 | 33.3 | 66.7 | 100.0 | 66.7 | 0.0 |
| Brazil | 227 (1.1) | 8.4 | 59.5 | 38.3 | 64.3 | 91.2 | 5.3 | 4.8 |
| Chile | 73 (3.9) | 19.2 | 53.4 | 46.6 | 69.9 | 68.5 | 4.1 | 0.0 |
| Colombia | 39 (0.8) | 33.3 | 43.6 | 23.1 | 53.8 | 92.3 | 33.3 | 20.5 |
| Costa Rica | 2 (0.4) | 0.0 | 0.0 | 50.0 | 50.0 | 100.0 | 50.0 | 0.0 |
| Cuba | 1 (0.1) | 0.0 | 0.0 | 100.0 | 100.0 | 100.0 | 0.0 | 0.0 |
| Dominican Republic | 1 (0.1) | 100.0 | 100.0 | 0.0 | 100.0 | 100.0 | 100.0 | 0.0 |
| Ecuador | 12 (0.7) | 25.0 | 66.7 | 41.6 | 83.3 | 66.7 | 8.3 | 0.0 |
| El Salvador | 3 (0.5) | 100.0 | 100.0 | 66.7 | 66.7 | 100.0 | 33.3 | 0.0 |
| French Guyana | 1 (3.4) | 0.0 | 0.0 | 0.0 | 100.0 | 100.0 | 0.0 | 0.0 |
| Guadeloupe | 1 (6.0) | 0.0 | 100.0 | 100.0 | 100.0 | 100.0 | 0.0 | 0.0 |
| Guyana | 1 (1.3) | 100.0 | 100.0 | 0.0 | 100.0 | 100.0 | 100.0 | 0.0 |
| Guatemala | 12 (0.7) | 58.3 | 58.3 | 33.3 | 83.3 | 83.3 | 8.3 | 8.3 |
| Haiti | 2 (0.2) | 100.0 | 100.0 | 50.0 | 100.0 | 100.0 | 50.0 | 0.0 |
| Honduras | 2 (0.2) | 100.0 | 100.0 | 50.0 | 100.0 | 100.0 | 50.0 | 0.0 |
| Mexico | 103 (0.8) | 21.4 | 70.0 | 33.0 | 83.5 | 78.6 | 3.9 | 3.9 |
| Nicaragua | 1 (0.2) | 100.0 | 100.0 | 0.0 | 100.0 | 100.0 | 100.0 | 0.0 |
| Paraguay | 3 (0.4) | 33.3 | 100.0 | 66.7 | 66.7 | 66.7 | 33.3 | 0.0 |
| Peru | 26 (0.8) | 30.8 | 50.0 | 26.9 | 76.9 | 61.5 | 7.7 | 0.0 |
| Puerto Rico | 3 (0.9) | 100.0 | 66.7 | 33.3 | 100.0 | 100.0 | 0.0 | 33.3 |
| Uruguay | 3 (0.9) | 0.0 | 66.7 | 33.3 | 33.3 | 66.7 | 0.0 | 0.0 |
| Venezuela | 3 (0.1) | 0.0 | 66.7 | 66.7 | 100.0 | 33.3 | 0.0 | 0.0 |
| United States | 124 (2.2)c | 9.7 | 79.8 | 62.1 | 86.3 | 88.7 | N/A | 12.9 |
Abbreviation: N/A, not available.
Systematic search included terms for childhood obesity and associated research fields, including nutrition, physical activity, sedentary behavior, and sleep.
Only US studies with explicit focus on Latino populations, or with predominantly Latino samples, were included.
For the United States, the articles per million inhabitants indicator was calculated using total Latino population as the denominator instead of the total country population. Therefore, this number represents childhood obesity articles per million Latino inhabitants.
The scoping review results highlight that cross‐national collaborations remain fairly limited across the region, with only 15 articles reporting on “South–South” collaborations, that is, multi‐site studies with more than one participating Latin American country (3.0% of all Latin American articles), and 16 articles being of “North–South” collaborations, that is, Latin America–US collaborations (representing 3.2% of all Latin American articles and 12.9% of all US, Latino‐focused articles). The countries with most international collaborations coincided with those where more childhood obesity research is being produced: Brazil, Mexico, Colombia, the United States, and Chile. Argentina, Costa Rica, Dominican Republic, Ecuador, El Salvador, Guatemala, Guyana, Haiti, Honduras, Nicaragua, Paraguay, and Peru were additional countries for which at least one multi‐site, international study was found, but the occurrence of cross‐national publications was considerably lower than that of the four leading Latin American countries and the United States.
3.5. Perceptions on capacity for childhood obesity research among Latin American investigators
A total of 320 people accessed the online survey link, and among those, 247 (77.2%) confirmed eligibility to participate. The final analytic sample consisted of 185 self‐identified active childhood obesity researchers residing and working in a Latin American country, who provided full responses to the online survey (74.9% of those eligible to participate). Respondents stemmed from 16 Latin American countries, with participation from all countries of the region except Belize, Cuba, French Guiana, Guadeloupe, Haiti, Honduras, Martinique, Nicaragua, Saint Barthelme and Saint Martin. Self‐reported expertise was 55.9% for obesity, 44.1% for nutrition, 58.3% for physical activity, 32.4% for sedentary behavior, and 12.1% for sleep (non‐mutually exclusive; see Figure S3). A majority of participants were female (57.8%), reported either a doctorate (42.7%) or a master (34.6%) as their terminal degree, had completed their terminal degree less than 10 years ago (68.6%), worked in a university setting (60.5%), and identified as public health experts (67.2%). Over half (51.8%) of survey respondents reported receiving formal training in another country (Table S2).
Table 2 presents the results of perceptions on capacity for childhood obesity research among Latin American investigators. Latin American childhood obesity researchers reported lower availability and quality of graduate training programs (doctoral level) in their country specializing in physical activity and/or sedentary time than in nutritional sciences. Although the majority of respondents reported that their institution has formal mentoring mechanisms or policies in place (64.3%), a smaller proportion perceive that early career investigators have sufficient resources and support to attain independence (28.7%).
TABLE 2.
Perceived research capacity for childhood obesity research among Latin American researchers (online survey, 2020; n = 185)
| Research capacity domains and indicators | n | % |
|---|---|---|
| Training programs | ||
| Considering the public health situation/need, in my country there are sufficient doctoral program offerings in … | ||
| Nutrition | 80 | 43.2 |
| Physical activity/sedentary time | 58 | 31.4 |
| My country has high quality doctoral programs in … | ||
| Nutrition | 83 | 44.9 |
| Physical activity/sedentary time | 59 | 31.8 |
| My institution offers doctoral training with a focus on …a | ||
| Nutrition | 38 | 40.0 |
| Physical activity/sedentary behavior | 19 | 20.0 |
| Sleep | 5 | 5.3 |
| Mentoring | ||
| My institution has formal mentoring mechanisms/policies in place | 119 | 64.3 |
| In my institution, established researchers spend sufficient time mentoring early career researchers | 99 | 53.5 |
| In my institution, all students and trainees specializing in childhood obesity find experienced mentors in their sub‐area of interestb | 93 | 50.3 |
| In my institution, all students and trainees specializing in childhood obesity have the necessary resources and support to become independent investigators | 53 | 28.7 |
| Research infrastructure (human capital/expertise) | ||
| The field of childhood obesity research in my country has a substantial number of experts in … | ||
| Epidemiology | 96 | 51.9 |
| Behavioral science | 77 | 41.6 |
| Biostatistics | 87 | 47.0 |
| Health policy | 101 | 54.6 |
| Systems sciences | 44 | 23.8 |
| Teams conducting childhood obesity research in my country generally include experts in … | ||
| Nutrition | 136 | 73.5 |
| Physical activity/sedentary behavior | 86 | 46.5 |
| Sleep | 32 | 17.3 |
| Funding | ||
| My country has sufficient funding opportunities available to support research on … | ||
| Nutrition and childhood obesity | 75 | 40.5 |
| Physical activity/sedentary behavior and childhood obesity | 52 | 28.1 |
| Sleep and childhood obesity | 41 | 22.2 |
| Multidisciplinary approaches for preventing and controlling childhood obesity | 61 | 33.0 |
| Scientific Societies and Conferences (Networking) | ||
| My country has active scientific societies and/or recurring conferences on … | ||
| Childhood obesity | 102 | 55.1 |
| Nutrition | 118 | 63.8 |
| Physical activity/sedentary behavior | 92 | 49.7 |
| Sleep | 31 | 16.8 |
Based on respondents who reported that their institution offers graduate level training programs (n = 90). All other percentage‐based indicators on this table are based on the full analytic sample (n = 185).
Sub‐areas may include nutrition, physical activity, behavior sedentary, sleep, behavioral science, and systems science.
In terms of the existing research infrastructure and human capital, perceived deficiencies for local expertise for behavioral science (41.6%) and systems science (28.3%) were identified. Almost three quarters of respondents agreed that childhood obesity research teams in their countries usually include nutritional scientists, while less than half (46.5%) said so about physical activity/sedentary behavior experts, and only 17.3% did so for sleep researchers.
Generally, funding for the varying disciplines related to childhood obesity research was perceived to be low in Latin America. Funding for physical activity/sedentary behavior, sleep, and multidisciplinary research were perceived to be somewhat lower than that for nutritional research. Among respondents, only 16.8% reported that their country has active research groups, such as societies, networks, or conferences centered on sleep research, in contrast to 49.7% for physical activity and 63.8% for nutrition.
4. DISCUSSION
Our results suggest few changes in the landscape of childhood obesity research capacity in Latin America since 201511 and present new evidence on the status of childhood obesity research in the United States with focus on Latino populations. Brazil, Mexico, and Chile continue to be the leading producers of childhood obesity‐related publications and are, with Colombia, the countries most engaged with south–south and north–south cross‐national collaborations.11 In Latin America, most studies are still predominantly employing descriptive or correlational approaches. The United States, as expected, is producing research at a higher rate than most Latin American countries and is at a more advanced stage for childhood obesity research with more longitudinal, intervention, and policy studies.
In addition, we found evidence of some advances in the field in Latin America, which are worth highlighting. Physical activity work has continued to grow in the region over the past 5 years, and research in this area is now being published at a similar rate than nutrition‐centered work. A contributing factor may be the growing number of highly trained early career scientists in physical activity and public health research, who have begun to establish research units and to collaboratively engage with their peers in other Latin American countries with similar interests and career stages.16, 17 However, publications are only one component of research capacity. Our results revealed persistent inequalities in childhood obesity research capacity across sub‐fields of specialization. Physical activity researchers were found to be less likely than obesity‐ or nutrition‐centered researchers to be part of childhood obesity research teams, have fewer funding opportunities to support their work, have fewer high‐quality graduate programs in their countries to pursue advanced training, and have fewer networking opportunities (e.g., specialized conferences or recurring events). This is likely reflective of the stages of development22 of each of these areas of research in Latin America. Before any of the major health transitions occurred in the region, there was a pressing need to mitigate infectious diseases and their underlying causes.1, 27 Starting several decades ago, Latin America developed vast expertise in nutritional research, which originally had a strong focus on undernutrition. On the other hand, physical activity research is still an emerging field in the region,17 with recent rapid growth in a few countries due to the growing burden of obesity and non‐communicable chronic diseases.7, 28
Another observed improvement had to do with the geographic concentration of childhood obesity‐related research in the region. Colombia is emerging, alongside Brazil, Mexico, and Chile, as another regional leader, especially for physical activity and sedentary behavior work. A noteworthy amount of physical activity and sedentary behavior‐centered research is also stemming from Ecuador, and a similar scenario was observed for nutrition‐centered research from Guatemala. In the case of Guatemala, it is apparent that the main driver is the presence of the Institute of Nutrition of Central America and Panama (INCAP),29 which provides an important lesson on the importance of strong, specialized local institutions as hubs for regional research. However, more than half of the articles from Guatemala are not being led by local researchers, suggesting that the country has a strong infrastructure for data collection and technical operations, but might be somewhat lacking in advanced scientific leadership, and that a “helicopter research” model might be at play in some cases.30 Building and maintaining local expertise and leadership is as important as collecting in‐country data, because local experts usually have the best contextual background to ask the most pressing questions, develop and use culturally appropriate measures, and advocate for evidence‐based practice with local policy makers and stakeholders. Attaining a critical mass of local research experts also helps in ensuring the long‐term sustainability of a local research agenda. When building cross‐national collaborations, it is important to carefully consider an equitable distribution of leadership tasks and opportunities for all parties and countries involved.
On the other hand, Argentina, with the fourth largest population size in Latin America and a relatively strong economy, continues to have an underwhelming amount of childhood obesity‐related research productivity, as was also reported by Parra et al.11 This situation may improve over the next few years, given a new wave of multi‐site international studies taking place in the region and including countries with little previous involvement in these types of cross‐national collaborations, including Argentina as one of the leaders.31, 32, 33 International, multi‐site studies are known boosters of research capacity for Latin American countries. The information gleaned from these types of studies provides added value as it combines local relevance for promoting contextually appropriate public health action, and the ability to make international comparisons that contribute important knowledge to the field. This model has been especially effective when the collaborations involve funding and/or research partners from high‐income countries, like the United States.16, 17
Not surprisingly, the United States was found to produce more Latino‐centered childhood obesity research than most Latin American countries. This, in spite of the fact that the US search was limited to articles focused on Latino populations (a sub‐group of the total population), demonstrating that Latino‐based childhood obesity research in the United States is at a more advanced stage22 than overall childhood obesity research across most of Latin America. This is further evidenced by the higher proportion of intervention studies taking place in the United States, in contrast to mostly descriptive and correlational studies taking place in Latin America. Exceptions are Mexico, where intervention research for obesity and nutrition research is beginning to take place, and Chile, where some physical activity interventions were identified. Moreover, US first and senior authors are more likely to hold advanced degrees than their Latin American counterparts, highlighting a wide gap in the available research and training infrastructures for childhood obesity research in the US versus Latin American countries.
In 2017, Parra et al. called for strategic investments to strengthen research capacity in all the key fields of research, which can contribute to understanding and preventing childhood obesity in Latin America.11 Our results suggest that these investments should vary by topic and country, based on the stage of development of each sub‐field within each setting. Surprisingly, most Latin American childhood obesity researchers reported higher availability for nutrition‐only research funds in their countries than for multidisciplinary approaches for childhood obesity prevention. The complex, multi‐causal nature of childhood obesity urgently demands these types of multisectoral, systems‐oriented approaches.34 Funding incentives to integrate systems science experts into childhood obesity research teams and to conduct studies inclusive of all relevant health behaviors are warranted. The inclusion of additional relevant disciplines (e.g., implementation scientists, economists, communicators, urban planners, and policy researchers) should also be promoted.
The availability of strong local training programs is an essential step towards establishing a sustainable research agenda.23 Almost four out of ten Latin American researchers who participated in our online survey received formal training in a high‐income country. Not only is international training not accessible for the majority of people seeking advanced degrees in Latin America but it can also result in a high occurrence of “brain drain” (the relocation of Latin American investigators to high income countries).35 Improving the availability of local programs and clear pathways towards research independence and financial stability are critical areas to invest in for preventing brain drain and for building a strong and stable research human capital across the region.
The World Health Organization (WHO) now includes sleep recommendations as part of its movement behavior guidelines for children, citing several health benefits of adequate sleep duration and quality, including obesity prevention.14 Sleep research is mostly lacking across the region. The few available studies on sleep are from Latin America or the United States (with Latino focus), are descriptive studies characterizing sleep duration and quality in childhood populations; correlational analyses examining the associations between sleep duration and sleep quality measures with BMI or obesity status; and cross‐sectional studies examining individual‐level correlates of sleep measures. The strategies that have helped strengthen the field of physical activity in the region over the past two decades can serve as models to promote the inclusion of sleep research as a critical component of childhood obesity prevention work for Latin American populations. These include developing advanced intensive courses and workshops that bring together promising early career investigators from across the region36; facilitating in‐person academic exchanges through visiting scholar programs, both between Latin American countries, and between Latin America and the United States; and working collaboratively towards securing funds to conduct cross‐national, multi‐site studies. Beyond supporting small training or pilot research projects, which can have a positive impact in early stages of capacity building,36, 37 local and international funding agencies are encouraged to invest in larger scale training program grants for Latin America, which support the strengthening of (or creation of new) graduate degree programs in public health fields to include a critical mass of expert faculty members in topics where gaps have been identified (physical activity/sedentary behavior, sleep, behavioral science, systems science, and implementation science38).
Although plenty of work remains to be done for optimizing research capacity for childhood obesity prevention in Latin America, there are some success stories. Chile's is highly research productivity across all relevant topics for childhood obesity research, and has the highest proportion of experimental and cohort study designs among Latin American countries. Their publication rate is the highest in the region, with 3.9 childhood obesity‐related publications per million inhabitants (vs. 1.1 in Brazil, 0.8 in Mexico, 0.8 in Colombia, and 2.2 in the United States [based on total Latino population]). The drivers of this could be many, such as their local funding and academic rewards structures, strong academic programs and institutions, and long‐lasting collaborations with other Latin American, as well as and new and growing cross‐national initiatives involving US‐based investigators (e.g., Our Voice Global Network39). Chile is also the only high‐income country in Latin America according to World Bank classifications. The influence of Chilean childhood obesity researchers in local policy action is also worth pointing out. For example, recently, nutrition experts provided evidence supporting the implementation of the novel “octagon” front‐package warning food labeling system (a model which has begun to expand to other parts of the world, including other countries of the region, like Mexico, Peru, Uruguay, and Brazil).40 Chile's research capacity model is worth exploring in further depth, as it could provide important lessons for capacity building and cross‐national collaborations across the region.
4.1. Limitations
Our work should be interpreted with consideration of its limitations. Because we conducted a scoping review and not a standard systematic review, appraisal of the quality of the studies presented in each article did not take place. Our search criteria were intended to provide us with an overall picture of the state of the field. It is possible that if we had not used the title and abstract restrictions of our algorithm, we could have found additional articles on all topics (obesity, nutrition, physical activity, sedentary behavior, and sleep). However, this would not change our general findings describing the broad patterns of childhood obesity research in the region. The number of indexed research articles on a given topic provides an objective indicator of research productivity. Unfortunately, equivalently objective indicator data for other domains of research capacity (mentoring, training, funding, and networking infrastructures) were not readily available. Our online survey attempted to fill this gap. Given that the survey was disseminated online, it was impossible to determine a true response rate, as we ignore how many people read the recruitment materials but decided not to open the survey link. However, a large proportion of those who accessed the link and were eligible to participate completed the survey (74.9%). In addition to obtaining responses from 16 countries, representation was also fairly balanced across topics of expertise and methodological disciplines. Nevertheless, it is possible that our sample might be biased towards early career investigators (only 17.3% had completed their terminal degree more than 15 years ago, while 37.8% of the sample had graduated from their terminal degree within the past 5 years), perhaps driven by the use of online social media channels for dissemination. Finally, our work had a stronger focus on Latin American countries than the United States. This is because this review serves as a follow‐up to the Parra et al. paper, which focused exclusively on Latin America, and because Latin American countries require much more investment in capacity‐building efforts to level the playing field for attaining fair, productive, and sustainable north–south collaborations.
5. CONCLUSIONS
Realizing the promise of a unified childhood obesity research agenda for Latin America and the United States will require investment in all of the key domains of capacity building and across all relevant topics for childhood obesity prevention. In spite of the proven effectiveness of cross‐national collaborations involving multiple Latin American partners and sites and US‐based researchers and/or funding sources for increasing local research capacity,11, 16, 17 we found little evidence of ongoing international collaborations. Emphatic efforts to bridge research across topics and settings, explicitly engaging countries beyond Brazil, Mexico, Chile, Colombia, and the United States, and to attain a multidisciplinary focus, are urgently needed.
Latin American countries and the United States could greatly benefit from a cohesive, unified research agenda, which prioritizes multi‐directional capacity building as a key pillar. For Latin American countries, this offers the potential to access otherwise limited funding and to become exposed to and learn from leading US experts. From our own experience, this learning process especially benefits early career researchers from all involved countries, such as doctoral students, who often become assigned to lead different local and/or technical aspects of the work. The benefits for these young leaders are not just in the skills and technical expertise gained, but also in the expansion of their network and the opportunities to co‐author scientific manuscripts stemming from these large international studies. US‐based students, on the other hand, gain access to novel research settings and can improve their global literacy, international network, and cultural competencies. From the public health perspective, the double win is also evident: by improving research capacity, locally relevant evidence becomes available to guide effective policy action in Latin American countries. In the United States, this type of research provides useful insights for understanding and resolving the childhood obesity epidemic among US Latino populations.
Except for studies focused on sleep, new cross‐national childhood obesity research initiatives should begin to focus more on intervention, policy, and implementation research.38 The Urban Health in Latin America (SALURBAL) project offers a good example for this type of cross‐national, multi‐directional intervention and policy research,41 which could be transferred to childhood obesity research. Finally, given the importance of capacity building for understanding and resolving the childhood obesity situation affecting Latin Americans and US Latinos, progress in research capacity indicators should be tracked systematically and periodically across the region.
CONFLICT OF INTEREST
Authors declared no conflict of interest.
Supporting information
Table S1. Scoping review of Latino‐focused childhood obesity research in the US (2015‐2019): location of studies by research topic.
Table S2. Online survey on perception of childhood obesity research capacity in Latin America (2020): analytic sample characteristics.
Figure S1. Flow chart of the systematic scoping review of childhood obesity‐related peer‐reviewed publications from Latin America and of US‐based articles with focus in Latino populations (June 2015 to April 2020).
Figure S2. Distribution (percentages) of childhood‐obesity related publications from Latin Americaa and the USb, by study design (June 2015 to April 2020).
Figure S3. Self‐reported topics of research expertise among Latin American childhood obesity investigators: online survey results (May 2020).
Salvo D, Parra DC, Jáuregui A, et al. Capacity for childhood obesity research in Latin American and US Latino populations: State of the field, challenges, opportunities, and future directions. Obesity Reviews. 2021;22(S3):e13244. 10.1111/obr.13244
REFERENCES
- 1.Rivera JA, de Cossio TG, Pedraza LS, Aburto TC, Sanchez TG, Martorell R. Childhood and adolescent overweight and obesity in Latin America: a systematic review. Lancet Diabetes Endocrinol. 2014;2(4):321‐332. [DOI] [PubMed] [Google Scholar]
- 2.Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity among adults and youth: United States, 2015–2016. CDC Data Brief. 2017;288:1‐4. [PubMed] [Google Scholar]
- 3.Ferre JC. Economic inequalities in Latin America at the base of adverse health indicators. Int J Health Serv. 2016;46(3):501‐522. [DOI] [PubMed] [Google Scholar]
- 4.Klasen S, Nowak‐Lehmann F. Poverty, Inequality and Migration in Latin America. Peter Lang International Academic Publishers; 2018. [Google Scholar]
- 5.Rivera JA, Pedraza LS, Martorell R, Gil A. Introduction to the double burden of undernutrition and excess weight in Latin America. Am J Clin Nutr. 2014;100(6):1613S‐1616S. [DOI] [PubMed] [Google Scholar]
- 6.Corvalan C, Garmendia ML, Jones‐Smith J, et al. Nutrition status of children in Latin America. Obes Rev. 2017;18(Suppl 2):7‐18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Katzmarzyk PT, Mason C. The physical activity transition. J Phys Act Health. 2009;6(3):269‐280. [DOI] [PubMed] [Google Scholar]
- 8.Flores A, Lopez G, Radford J. Hispanic population in the United States statistical portrait. Pew Research Center. Pew Research Center: Hispanic Trends Web site. https://www.pewresearch.org/hispanic/2017/09/18/2015‐statistical‐information‐on‐hispanics‐in‐united‐states/#hispanic‐pop. Published 2015. Accessed Jan 7, 2020.
- 9.Vega WA, Rodriguez MA, Gruskin E. Health disparities in the Latino population. Epidemiol Rev. 2009;31(1):99‐112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Perez‐Escamilla R, Lutter CK, Rabadan‐Diehl C, et al. Prevention of childhood obesity and food policies in Latin America: from research to practice. Obes Rev. 2017;18(Suppl 2):28‐38. [DOI] [PubMed] [Google Scholar]
- 11.Parra DC, Vorkoper S, Kohl HW 3rd, et al. Research capacity for childhood obesity prevention in Latin America: an area for growth. Obes Rev. 2017;18(Suppl 2):39‐46. [DOI] [PubMed] [Google Scholar]
- 12.Felknor SA, Delclos GL, Gimeno D, et al. Funding of pilot projects in Latin America: a tool for capacity building in occupational health research. Int J Occup Environ Health. 2006;12(4):408‐414. [DOI] [PubMed] [Google Scholar]
- 13.Must A, Parisi SM. Sedentary behavior and sleep: paradoxical effects in association with childhood obesity. Int J Obes (Lond). 2009;33(Suppl 1):S82‐S86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Willumsen J, Bull F. Development of WHO guidelines on physical activity, sedentary behavior, and sleep for children less than 5 years of age. J Phys Act Health. 2020;17(1):96‐100. [DOI] [PubMed] [Google Scholar]
- 15.Ramirez AG, Gallion KJ, Despres CE, Adeigbe RT. Salud America!: a national research network to build the field and evidence to prevent Latino childhood obesity. Am J Prev Med. 2013;44(3):S178‐S185. [DOI] [PubMed] [Google Scholar]
- 16.Sallis JF, Cerin E, Kerr J, et al. Built environment, physical activity, and obesity: findings from the International Physical Activity and Environment Network (IPEN) adult study. Annu Rev Public Health. 2020;41(1):119‐139. [DOI] [PubMed] [Google Scholar]
- 17.Salvo D, Reis RS, Sarmiento OL, Pratt M. Overcoming the challenges of conducting physical activity and built environment research in Latin America: IPEN Latin America. Prev Med. 2014;69(Suppl 1):S86‐S92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA‐ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467‐473. [DOI] [PubMed] [Google Scholar]
- 19.Munn Z, Peters MD, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ramírez Varela A, Cruz GIN, Hallal P, et al. Global, regional, and national trends and patterns in physical activity research since 1950: a systematic review. Int J Behav Nutr Phys Act. 2021;18(1):5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gross T.ArcScript Cartogram geoprocessing tool version 2. In: ESRI Support Center; 2009. http://arcscripts.esri.com/details.asp
- 22.Sallis JF, Owen N, Fotheringham MJ. Behavioral epidemiology: a systematic framework to classify phases of research on health promotion and disease prevention. Ann Behav Med. 2000;22(4):294‐298. [DOI] [PubMed] [Google Scholar]
- 23.Nchinda TC. Research capacity strengthening in the South. Soc Sci Med. 2002;54(11):1699‐1711. [DOI] [PubMed] [Google Scholar]
- 24.Sitthi‐Amorn C, Somrongthong R. Strengthening health research capacity in developing countries: a critical element for achieving health equity. BMJ. 2000;321(7264):813‐817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Schrubbe KF. Mentorship: a critical component for professional growth and academic success. J Dent Educ. 2004;68(3):324‐328. [PubMed] [Google Scholar]
- 26.Conceicao C, Leandro A, McCarthy M. National support to public health research: a survey of European ministries. BMC Public Health. 2009;9(1):203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Perez‐Escamilla R, Bermudez O, Buccini GS, et al. Nutrition disparities and the global burden of malnutrition. BMJ. 2018;361:k2252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Barreira TV, Broyles ST, Tudor‐Locke C, et al. Epidemiological transition in physical activity and sedentary time in children. J Phys Act Health. 2019;16(7):518‐524. [DOI] [PubMed] [Google Scholar]
- 29.Pernet CA. Between entanglements and dependencies: food, nutrition, and national development at the Central American Institute of Nutrition (INCAP). In: International Organizations and Development, 1945–1990. Springer; 2014:101‐125. [Google Scholar]
- 30.Minasny B, Fiantis D, Mulyanto B, Sulaeman Y, Widyatmanti W. Global soil science research collaboration in the 21st century: time to end helicopter research. Geoderma. 2020;373:114299. [Google Scholar]
- 31.Fisberg M, Kovalskys I, Gomez G, et al. Latin American Study of Nutrition and Health (ELANS): rationale and study design. BMC Public Health. 2016;16:93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ferrari GLM, Kovalskys I, Fisberg M, et al. Socio‐demographic patterning of objectively measured physical activity and sedentary behaviours in eight Latin American countries: findings from the ELANS study. Eur J Sport Sci. 2020;20(5):670‐681. [DOI] [PubMed] [Google Scholar]
- 33.Kovalskys I, Fisberg M, Gomez G, et al. Energy intake and food sources of eight Latin American countries: results from the Latin American Study of Nutrition and Health (ELANS). Public Health Nutr. 2018;21(14):2535‐2547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Finegood DT, Merth TD, Rutter H. Implications of the foresight obesity system map for solutions to childhood obesity. Obesity (Silver Spring). 2010;18(Suppl 1):S13‐S16. [DOI] [PubMed] [Google Scholar]
- 35.White F. Capacity‐building for health research in developing countries: a manager's approach. Rev Panam Salud Publica. 2002;12(3):165‐172. [DOI] [PubMed] [Google Scholar]
- 36.Evenson KR, Dorn JM, Camplain R, Pate RR, Brown DR. Evaluation of the physical activity and public health course for researchers. J Phys Act Health. 2015;12(8):1052‐1060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Delisle H, Shrimpton R, Blaney S, et al. Capacity‐building for a strong public health nutrition workforce in low‐resource countries. Bull World Health Organ. 2017;95(5):385‐388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Pérez‐Escamilla R, Vilar‐Compte M, Rhodes E, et al. Implementation of childhood obesity prevention and control policies in the United States and Latin America: Lessons for cross‐border research and practice. Obes Rev. 2021;22(Suppl 3):e13247. 10.1111/obr.13247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.King AC, King DK, Banchoff A, et al. Employing participatory citizen science methods to promote age‐friendly environments worldwide. Int J Environ Res Public Health. 2020;17(5):1‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Corvalan C, Reyes M, Garmendia ML, Uauy R. Structural responses to the obesity and non‐communicable diseases epidemic: update on the Chilean law of food labelling and advertising. Obes Rev. 2019;20(3):367‐374. [DOI] [PubMed] [Google Scholar]
- 41.Diez Roux AV, Slesinski SC, Alazraqui M, et al. A novel international partnership for actionable evidence on urban health in Latin America: LAC‐urban health and SALURBAL. Glob Chall. 2019;3(4):1800013. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Scoping review of Latino‐focused childhood obesity research in the US (2015‐2019): location of studies by research topic.
Table S2. Online survey on perception of childhood obesity research capacity in Latin America (2020): analytic sample characteristics.
Figure S1. Flow chart of the systematic scoping review of childhood obesity‐related peer‐reviewed publications from Latin America and of US‐based articles with focus in Latino populations (June 2015 to April 2020).
Figure S2. Distribution (percentages) of childhood‐obesity related publications from Latin Americaa and the USb, by study design (June 2015 to April 2020).
Figure S3. Self‐reported topics of research expertise among Latin American childhood obesity investigators: online survey results (May 2020).