

Abstract
Objective:
To compare the mixed dentition incisor and molar overjet, severity of contraction of the dental arch, and the sagittal molar relationship on the cleft side vs the noncleft side in children with repaired complete unilateral cleft of the lip and palate (UCLP).
Materials and Methods:
Orthodontic records taken prior to orthodontic preparation for alveolar bone grafting were screened to select study casts from patients with nonsyndromic repaired complete UCLP who did not have mandibular skeletal or dental asymmetry. The study sample comprised dental casts from 74 children aged 8.9 ± 1 years. Standardized digital photographs were acquired at 1:1 magnification. A coordinate system was developed using digital image-processing software (Photoshop CS4 and Adobe Illustrator). Incisor and molar overjet, Angle's classification, and arch contraction were recorded. Descriptive statistics, paired t-tests, and kappa statistics were used to compare the cleft and noncleft sides.
Results:
A negative overjet of −1 to −5 mm was often present at the incisors, with greater frequency and magnitude on the cleft side. Class II molar relation was more frequent on the cleft side (61.1%) than on the noncleft side (47.2%). Significantly greater contraction of the cleft side deciduous canine and deciduous first molar was noted, while the difference was very minor at the first permanent molar.
Conclusions:
Cleft side maxillary arch contraction was most severe in the deciduous canine and first deciduous molar region and progressively less severe in the posterior region of the arch. A greater frequency and severity of negative overjet and Class II molar relationship was seen on the cleft side.
Keywords: Cleft, Malocclusion, Arch contraction, Negative overjet, Angle classification
INTRODUCTION
Maxillary arch contraction and crossbite are the main features of the malocclusion that receive attention in the orthodontic preparation performed in the mixed dentition period prior to the secondary alveolar bone graft surgery in children with repaired complete unilateral clefts of the lip and palate (UCLP). The permanent central incisor is palatally inclined,1–4 while the deciduous canine and deciduous molars are palatally inclined or displaced along with palatal collapse of the maxillary lateral segment.5
Numerous studies of maxillary dental arch dimension in UCLP at different ages have shown significantly smaller than normal maxillary arch width and length.6–11 While studies have described arch contraction in different regions of the arch in UCLP, maxillary arch width differences between the cleft and noncleft sides have been rarely discussed.9 Angle classification in UCLP has also been reported less frequently, with a wide range of presentations.12,13
Appropriate orthodontic preparation prior to alveolar bone grafting is associated with higher success rates of the graft as well as reduction in time spent for comprehensive orthodontic treatment following the graft.14–18 It is important for clinicians to recognize the characteristics of the malocclusion in order to enhance their clinical judgment and improve treatment outcomes. The aim of this study was to explore comprehensively those features of the dentoalveolar malocclusion in complete UCLP that have not been well elucidated in the literature. Our objectives were to qualitatively and quantitatively assess the overjet relation of the permanent maxillary central incisors and first permanent molars, sagittal molar occlusal relationships, and severity of contraction of the dental arch on the cleft side in comparison with the noncleft side.
MATERIALS AND METHODS
Following Research Ethics Board approval, a retrospective chart review was undertaken to select patients with nonsyndromic complete UCLP who had received all their lip and palate reparative surgeries at The Hospital for Sick Children, Toronto, Canada. Orthodontic records taken prior to orthodontic preparation for alveolar bone grafting were screened to include study models from those patients who had not received any orthodontic treatment in the primary or mixed dentition and had at least one maxillary central incisor and one maxillary first permanent molar fully erupted. Further inclusion criteria required that none of the selected subjects had mandibular dental asymmetry (verified from their clinic notes and photographs) or differential loss of arch length due to early loss of deciduous mandibular molars or caries. A pair of dividers was used to measure the linear distance from the mesial cervical margin of the mandibular central incisors to each of the mesial contact points of the mandibular first permanent molars on the right and left sides. Models in which the difference was less than 1 mm were selected.
Applying these criteria, the study sample comprised dental models from 74 children (53 boys, 21 girls) with complete UCLP. The mean age at which the models had been made was 8.9 ± 1 year. Thirty subjects had right UCLP and 44 had left UCLP. These differences in frequencies related to male predilection and laterality are well established in epidemiologic studies of orofacial clefts. The primary lip and palate repairs had been provided by any one of the hospital's five staff surgeons. Lip repair techniques included the Millard and Tennison techniques or their modifications and the Fisher anatomic subunit techniques. Palate repair techniques included the von Langenbeck, Wardill-Killner pushback, or hybrid techniques. These techniques are commonly used around the world. Therefore, the surgical treatment received by the sample can be viewed as being representative of typical surgical treatment in UCLP. In 10% of the sample, secondary surgical procedures had been provided prior to model acquisition, including rhinoplasty, pharyngoplasty, and, rarely, redo palatoplasty.
Each pair of models was mounted in centric occlusion according to the individual bite registration that was available. Overjet was recorded by adapting the methods described in the modified Huddart and Bodenham system.19 Rather than scoring the overjet as normal occlusion, positive or negative overjet (as described in the modified Huddart and Bodenham system), the actual overjet measured at the central incisors and first permanent molars was recorded to the nearest 1 mm. The sagittal molar relationship was recorded using Angle's classification.
To create a horizontal reference line for the analysis of the maxillary model, a line was drawn (using a 0.5-mm pencil) from the buccal groove of the lower first permanent molar to the bucco-occlusal surface of the occluded upper first permanent molar on each side. The maxillary models were then mounted on a stand with their occlusal planes parallel to the floor and maxillary teeth facing upward for photographing the occlusal surface of the teeth. A 12.3-megapixel digital single-lens reflex camera using a 90-mm macro lens was set with ISO 200, 1/30 second at f13, and occlusal photographs of the maxillary dental arch were acquired, perpendicular to the occlusal plane, with the resolution set at 4032 × 3024 pixels in a RAW format. Each image was calibrated using a 10-mm plastic scale placed at the correct depth of field and parallel to the lens of the camera. The images were processed using Photoshop CS4 for converting RAW format to EPS format, which then were compatible with the Adobe Illustrator (version 4.0, Adobe Systems Inc, San Jose, Calif) vector graphics image editor program. Through this image-editing program, lines were overlaid on the occlusal images of the maxillary models to allow measuring the mediolateral arch dimension at the deciduous canines, first and second molars, and the permanent first molars. With the Adobe Illustrator software program, a horizontal construct (hc) was drawn as the line connecting the right and left marks that had been made on the bucco-occlusal surface of the upper molars with pencil prior to the photographing of the models. A perpendicular line was drawn at the midpoint of this horizontal construct and was referred to as the midsagittal construct (msc) of the maxillary arch (Figure 1).
Figure 1.
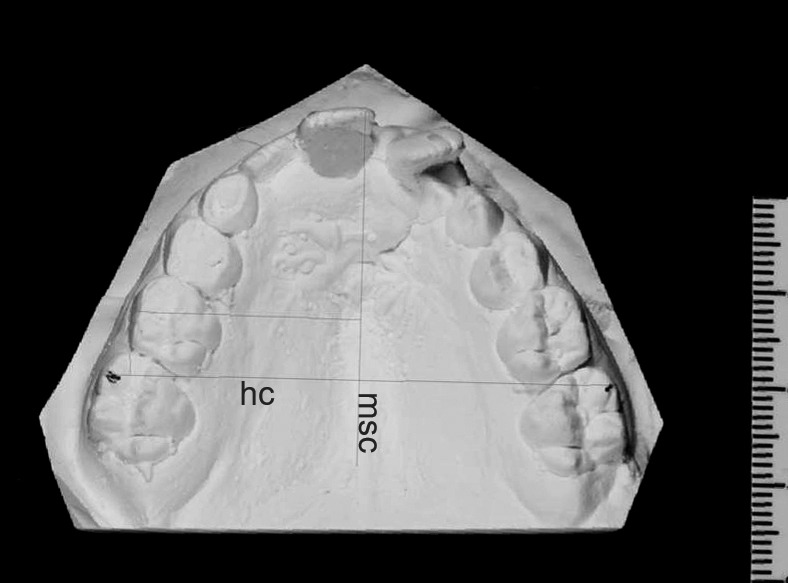
Standardized maxillary occlusal photograph with midsagittal construct (msc) and horizontal construct (hc) lines shown, along with the mediolateral arch width at the noncleft side deciduous second molar.
Mediolateral arch widths on the cleft and noncleft sides were measured as perpendicular distances from the msc to the cusp tip of the deciduous canine (or center of the wear facet if present), mesiobuccal groove of the deciduous first molar, mesiobuccal groove of the deciduous second molar, and the mesiobuccal groove of the permanent first molar (Figure 2).
Figure 2.

Mediolateral arch width measurements (shown on cleft side): 1, at the deciduous canine; 2, at the deciduous first molar; 3, at the deciduous second molar; 4, at the permanent first molar.
Statistical Analysis
All measurements were undertaken by one investigator (SD). After a period of 45 days, repeated measurements were made by the same investigator for 22 randomly selected models. Intraexaminer repeatability was assessed by intraclass correlation coefficient analysis. Errors were determined using Dahlberg's formula for continuous variables and level of agreement for categorical variables. Paired t-tests were used to compare the differences in arch contraction between the cleft and noncleft sides using paired measurements from only those maxillary models that exhibited no missing teeth in the deciduous canine or molar regions. Level of agreement or symmetry of classification of the molar relationship between the cleft and noncleft sides was derived using Cohen's kappa coefficient. The significance level for statistical tests was set at 5%.
RESULTS
Intraexaminer reliability tests showed that the repeatability of measurements was excellent and method errors were small (Table 1). There was 100% agreement of Angle's classification of molar relationship.
Table 1.
Repeatability of Measurements
| Variable |
First Measurement | Second Measurement | Measurement Errora |
ICCCb |
P Value |
| Mean ± SD |
Mean ± SD |
||||
| Cleft side mediolateral width at permanent first molar, mm | 26.04 ± 2.33 | 26.05 ± 2.31 | .13 | .997 | <.001 |
| Noncleft side mediolateral width at permanent first molar, mm | 26.31 ± 2.10 | 26.28 ± 2.20 | .22 | .989 | <.001 |
| Cleft side mediolateral width at deciduous canine, mm | 11.26 ± 2.69 | 11.36 ± 2.69 | .09 | .995 | <.001 |
| Noncleft side mediolateral width at deciduous canine, mm | 16.11 ± 2.08 | 16.10 ± 2.07 | .16 | .994 | <.001 |
| Cleft side mediolateral width at deciduous first molar, mm | 15.91 ± 3.37 | 15.90 ± 3.44 | .12 | .999 | <.001 |
| Noncleft side mediolateral width at deciduous first molar, mm | 19.29 ± 2.34 | 19.27 ± 2.27 | .14 | .996 | <.001 |
| Cleft side mediolateral width at deciduous second molar, mm | 20.67 ± 2.68 | 20.71 ± 2.73 | .20 | .999 | <.001 |
| Noncleft side mediolateral width at deciduous second molar, mm | 22.41 ± 2.07 | 22.41 ± 2.13 | .12 | .996 | <.001 |
| Cleft side incisor overjet, mm | −1.24 ± 2.61 | −1.29 ± 2.70 | .26 | .990 | <.001 |
| Noncleft side incisor overjet, mm | −0.67 ± 1.83 | −0.62 ± 1.88 | .26 | .979 | <.001 |
| Cleft side molar overjet, mm | 0.60 ± 1.19 | 0.60 ± 1.19 | .00 | 1.000 | <.001 |
| Noncleft side molar overjet, mm | 1.24 ± 0.44 | 1.19 ± 0.4 | .15 | .865 | <.001 |
Measurement error = √Σ D2/2N, where D is the difference in the repeated measurements and N is the number of double measurements.
Intraclass correlation coefficient.
Most maxillary first molars exhibited a positive overjet relative to their opposing teeth in occlusion (83.10% and 92.86% of the cleft and noncleft molars, respectively). A negative molar overjet of −1 to −5 mm was detected more frequently on the cleft side (16.90%) than on the noncleft side (7.14%). In contrast, most central incisors on the cleft and noncleft sides showed a negative overjet of −1 to −5 mm, with greater severity on the cleft side. Negative incisor overjet exceeding −5 mm was much less frequent on both cleft and noncleft sides (9.86% and 1.39%, respectively), and negative overjet that exceeded −10 mm was detected only once, on the cleft side. Positive overjet occurred more frequently and with greater magnitude on the noncleft side (37.50%; mean 1.07 ± 0.96 mm) than on the cleft side (25.35%; mean 0.72 ± 1.07 mm; Table 2).
Table 2.
Overjet Measured at Central Incisors and First Permanent Molars
| Overjet |
Cleft Side Incisor |
Noncleft Side Incisor |
Cleft Side Molar |
Noncleft Side Molar |
||||
| n (%) |
Mean ± SD, mm |
n (%) |
Mean ± SD, mm |
n (%) |
Mean ± SD, mm |
n (%) |
Mean ± SD, mm |
|
| Negative −1 to −5 mm | 46 (64.79) | −1.91 ± 1.03 | 44 (61.11) | −1.55 ± 0.93 | 12 (16.90) | −1.33 ± 0.78 | 5 (7.14) | −1.4 ± 0.55 |
| Negative −5 to −10 mm | 6 (8.45) | −7.83 ± 1.72 | 1 (1.39) | −9 | 0 (0) | N/A | 0 (0) | N/A |
| Negative > −10 mm | 1 (1.41) | −14 | 0 (0) | N/A | 0 (0) | N/A | 0 (0) | N/A |
| Positive 0 to +4 mm | 18 (25.35) | 0.72 ± 1.07 | 27 (37.5) | 1.07 ± 0.96 | 58 (83.10) | 1 ± 0.64 | 65 (92.86) | 1.15 ± 0.54 |
Class II molar relation was more frequent on the cleft side (61.11%) than on the noncleft side (47.22%). Overall, the agreement or symmetry between the Angle's classification of the first molar on the cleft and noncleft sides was seen in 58.34% of the models, and the Cohen's kappa coefficient was fair at 0.27. Class II molar relationship was more frequent (36.11%) than Class I (18.06%) or Class III (4.17%) when there was a symmetric molar relation on both sides (Table 3).
Table 3.
Angle's Classification of First Permanent Molar Occlusion on Cleft and Noncleft Sides, n (%)
| Noncleft |
||||
| Cleft |
Class I |
Class II |
Class III |
Total |
| Class I | 13 (18.06) | 8 (11.11) | 2 (2.78) | 23 (31.95) |
| Class II | 15 (20.83) | 26 (36.11) | 3 (4.17) | 44 (61.11) |
| Class III | 2 (2.78) | 0 | 3 (4.17) | 5 (6.94) |
| Total | 30 (41.67) | 34 (47.22) | 8 (11.11) | 72 (100) |
Significantly greater arch contraction at the deciduous canine and first and second deciduous molars was noted on the cleft side. The magnitude of differences was greatest at the level of the deciduous canines and progressively less in the posterior portion of the arch. Clinically, a very minor, although statistically significant, difference in arch contraction was noted at the maxillary first permanent molar (Table 4).
Table 4.
Arch Contraction (Pairwise Comparisons)
| Mediolateral Arch Width From msca |
N |
Cleft Side | Noncleft Side | Difference (Noncleft Side – Cleft Side) | Paired t-Test (P Value) |
| Mean ± SD, mm |
Mean ± SD, mm |
Mean ± SD, mm |
|||
| Deciduous canine | 46 | 11.16 ± 3.10 | 15.68 ± 2.08 | 4.51 ± 3.59 | .000*** |
| Deciduous first molar | 46 | 15.71 ± 3.00 | 18.96 ± 2.12 | 3.25 ± 2.80 | .000*** |
| Deciduous second molar | 46 | 20.65 ± 2.28 | 22.18 ± 2.10 | 1.53 ± 1.53 | .000*** |
| Permanent first molar | 46 | 25.75 ± 2.00 | 25.84 ± 2.09 | 0.10 ± 0.74 | .038* |
msc: midsagittal construct
P < .05, significant; *** P < .001, very highly significant.
DISCUSSION
Malocclusion in patients with CLP is characterized by dentoalveolar distortions of the maxillary arch with different severities on the cleft and noncleft sides. This study was not aimed at comparing the occlusal outcome of one type of surgical technique or protocol vs another but rather aimed to study comprehensively the patterns and magnitudes of several key characteristics of the dentoalveolar malocclusion typically seen in UCLP, an understanding of which would be helpful for planning prealveolar bone graft orthodontic treatment. To facilitate such an appraisal, reference lines to define symmetry of the arch were established. As described in several studies, the mandibular arch in patients with clefts has symmetry comparable with that seen in the mandibular arch in unaffected populations.8,9,11,20,21 In this study, the mandibular models were verified for symmetry by comparing the distance from the cervical midline between the mandibular central incisors to the mesial aspect of left and right mandibular first molars using a pair of dividers. Right- and left-side measurements differed by no more than 1 mm, confirming the integrity of the mandibular dental arch in the selected sample. A review of the photographic and clinic chart notes further confirmed that no significant facial asymmetry existed. These steps allowed using the mandibular dental arch to construct reference lines in the maxillary arch. Arguably, an analysis of symmetry based on cranial base landmarks through the use of craniofacial computed tomography (CT)22 or cone beam CT could be more precise but would have involved radiation. The system used in the current study did not involve any radiation and allowed using existing pretreatment models and records that were available for a reasonably large number of children who had received treatment at a single center. CT scans were not available for the subjects included in this retrospective study.
Several authors have suggested causes for incisor malposition in UCLP. Ross3,4 suggested that postsurgical scar tissue induced the periodontal ligament to pull anterior teeth backward toward the palate. Smahel et al.2 and Ishikawa et al.5 described that the lingual inclination of the dentoalveolar process on the cleft side was a result of periosteal denudation of the bone and its scar tissue. Wijdeveld et al.,23 in their histologic studies on beagle dogs, showed that the scar tissue covering denuded bone on lateral sides of the palate were mainly transversally orientated collagenous fibers that lacked blood supply and elastic fibers and had a continuation with the periodontal ligament. This was suggested to be responsible for narrowing of the arch. The main objective in comparing arch width between the cleft and noncleft sides in this study was to quantitatively measure the differences in the maxillary transverse arch dimension. Recognizing definite points of constriction helps clinicians to choose the most appropriate expanders, avoiding over- or underexpansion, thus minimizing posttreatment relapse. The current study's results corroborate the findings of some others,6,9–11 which noted the greatest arch constriction at the deciduous canine region. In the current study, maxillary arch contraction on the cleft side was most severe in the deciduous canine and first deciduous molar region and progressively less severe in the posterior regions of the arch. The clinical implication of this finding is that during the preparatory phase of orthodontics prior to alveolar grafting, expansion must be maximized at the intercanine level. We recommend that expanders such as Tri or Quad Helix that allow differential control of the segments (Figure 3), or fan-shaped expansion appliances, which deliver greater expansion anteriorly, are better suited to the prealveolar bone graft orthodontic preparation in UCLP.
Figure 3.
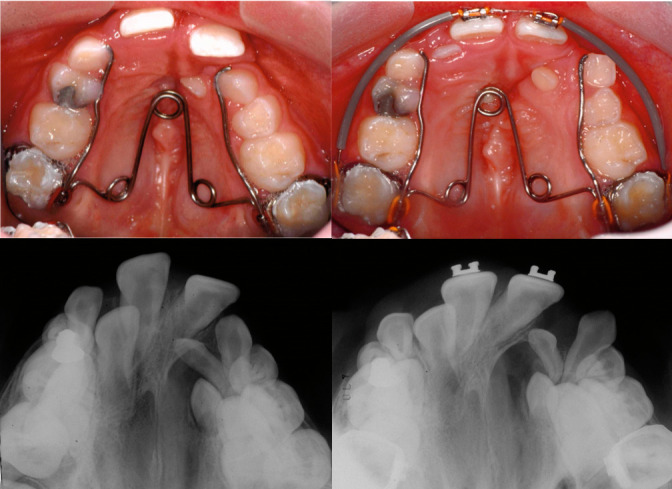
Selective activation at helicals and arms of a Tri Helix expander allows effective and differentially greater expansion of the contracted left segment, while a bracket bonded with distoincisal tilt allows the cleft side incisor root to remain within alveolar bone as a crossbite is corrected during the prealveolar bone graft orthodontic preparation (orthodontic treatment provided by Dr Sunjay Suri).
Maxillary first permanent molar relationships have been inadequately discussed in the literature on UCLP. Vettore and Sousa Campos12 described that most patients with cleft lip and palate during 6–12 years have Angle Class II malocclusion, whereas Baek et al.13 reported that Angle Class III malocclusion was most prevalent. Most of our study sample had Class II molar relationship on the cleft side. The high frequency of Angle Class II (61.11% on the cleft side and 47.22% on the noncleft side) could have also been influenced by the age of the patient, greater rotation of the maxillary first permanent molars on the cleft side, congenitally missing teeth in the maxilla, or early maxillary deciduous tooth loss in some patients. In our study sample, the maxillary lateral incisor was not seen in the models in 39.1% on the cleft side and 28.4% on the noncleft side, while the first deciduous molar was not present in 12.2% on the cleft side and 17.6% on the noncleft side, and the maxillary second deciduous molar was not seen in 13.5% on the cleft side and 12.2% on the noncleft side.
In agreement with Vettore and Sousa Campos12 who reported anterior crossbite in 70.3% of their sample of complete CLP in the 6- to 12-year age group, a negative overjet within a range of −1 to −5 mm was found to be the most common relationship of central incisors on both cleft and noncleft sides in our study, although the mean magnitude was twice as large on the cleft side (Table 2). A minor negative overjet resulting from overretroclined maxillary central incisors can be corrected by advancing them through archwire mechanics (Figure 3). This also helps facilitate surgical access for the alveolar bone graft by preventing overretroclined teeth from constricting the surgical site. In addition, it eliminates anterior traumatic occlusion caused by the negative overjet and improves the patient's facial esthetics and confidence. However, a more severe negative overjet at this age is an indication of skeletal dysplasia, which will likely get worse during adolescent facial growth. Severe skeletal dysplasia, when diagnosed in the mixed dentition period, should not be corrected by dental compensation.
CONCLUSIONS
-
•
The maxillary arch in this sample of patients with nonsyndromic complete UCLP whose mixed dentition stage dental models were examined revealed characteristic arch contractions in different regions of the arch.
-
•
Arch contraction was most severe on the cleft side in the deciduous canine and first deciduous molar regions, and a negative overjet of −1 to −5 mm was frequently present at the incisors.
-
•
A greater frequency of Class II molar relationship was seen on the cleft side.
-
•
Orthodontic mechanics that allow differential control of dental arch segments should be employed to correct these characteristics of the malocclusion and arch collapse.
ACKNOWLEDGMENTS
Parts of this research were presented at the 12th International Congress on Cleft Lip/Palate and Related Craniofacial Anomalies, May, 2013; Orlando, FL, USA.
REFERENCES
- 1.Subtelny JD. Orthodontic treatment of cleft lip and palate, birth to adulthood. Angle Orthod. 1966;36:273–292. doi: 10.1043/0003-3219(1966)036<0273:OTOCLA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Smahel Z, Tomanová M, Müllerová Z. Position of upper permanent central incisors prior to eruption in unilateral cleft lip and palate. Cleft Palate Craniofac J. 1996;33:219–224. doi: 10.1597/1545-1569_1996_033_0219_poupci_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 3.Ross RB, Johnston MC. Cleft Lip and Palate. Baltimore, Md: Williams & Wilkins; 1972. [Google Scholar]
- 4.Ross RB. Midfacial and mandibular dysmorphology and growth in facial clefting: clinical implications. In: Mooney MP, Siegel MI, editors. Understanding Craniofacial Anomalies. Hoboken, NJ: Wiley-Liss; 2002. pp. 391–421. [Google Scholar]
- 5.Ishikawa H, Iwasaki H, Tsukada H, Chu S, Nakamura S, Yamamoto K. Dentoalveolar growth inhibition induced by bone denudation on palates: a study of two isolated cleft palates with asymmetric scar tissue distribution. Cleft Palate Craniofac J. 1999;36:450–456. doi: 10.1597/1545-1569_1999_036_0450_dgiibb_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 6.Athanasiou AE, Mazaheri M, Zarrinnia K. Dental arch dimensions in patients with unilateral cleft lip and palate. Cleft Palate J. 1988;25:139–145. [PubMed] [Google Scholar]
- 7.McCance A, Roberts-Harry D, Sherriff M, Mars M, Houston WJ. Sri Lankan cleft lip and palate study model analysis: clefts of the secondary palate. Cleft Palate Craniofac J. 1993;30:227–230. doi: 10.1597/1545-1569_1993_030_0227_slclap_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 8.DiBiase AT, DiBiase DD, Hay NJ, Sommerlad BC. The relationship between arch dimensions and the 5-year index in the primary dentition of patients with complete UCLP. Cleft Palate Craniofac J. 2002;39:635–640. doi: 10.1597/1545-1569_2002_039_0635_trbada_2.0.co_2. [DOI] [PubMed] [Google Scholar]
- 9.Garrahy A, Millett DT, Ayoub AF. Early assessment of dental arch development in repaired unilateral cleft lip and unilateral cleft lip and palate versus control. Cleft Palate Craniofac J. 2005;42:385–391. doi: 10.1597/03-159.1. [DOI] [PubMed] [Google Scholar]
- 10.Lewis BR, Stern MR, Willmot DR. Maxillary anterior tooth size and arch dimensions in unilateral cleft lip and palate. Cleft Palate Craniofac J. 2008;45:639–646. doi: 10.1597/07-078.1. [DOI] [PubMed] [Google Scholar]
- 11.dos Santos PB, Janson G, Assis VH, Leite Battisti Mde P, Assis DG. Association between dental arch widths and interarch relationships in children with operated unilateral complete cleft lip and palate. Cleft Palate Craniofac J. 2015;52:e196–e200. doi: 10.1597/12-171. [DOI] [PubMed] [Google Scholar]
- 12.Vettore MV, Sousa Campos AE. Malocclusion characteristics of patients with cleft lip and/or palate. Eur J Orthod. 2011;33:311–317. doi: 10.1093/ejo/cjq078. [DOI] [PubMed] [Google Scholar]
- 13.Baek SH, Moon HS, Yang WS. Cleft type and Angle's classification of malocclusion in Korean cleft patients. Eur J Orthod. 2002;24:647–653. doi: 10.1093/ejo/24.6.647. [DOI] [PubMed] [Google Scholar]
- 14.Enemark H, Sindet-Pedersen S, Bundgaard M. Long-term results after secondary bone grafting of alveolar clefts. J Oral Maxillofac Surg. 1987;45:913–919. doi: 10.1016/0278-2391(87)90439-3. [DOI] [PubMed] [Google Scholar]
- 15.Da Silva Filho OG, Teles SG, Ozawa TO, Filho LC. Secondary bone graft and eruption of the permanent canine in patients with alveolar clefts: literature review and case report. Angle Orthod. 2000;70:174–178. doi: 10.1043/0003-3219(2000)070<0174:SBGAEO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Eppley BL, Sadove AM. Management of alveolar cleft bone grafting—state of the art. Cleft Palate Craniofac J. 2000;37:229–233. doi: 10.1597/1545-1569_2000_037_0229_moacbg_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 17.Williams A, Semb G, Bearn D, Shaw W, Sandy J. Prediction of outcomes of secondary alveolar bone grafting in children born with unilateral cleft lip and palate. Eur J Orthod. 2003;25:205–211. doi: 10.1093/ejo/25.2.205. [DOI] [PubMed] [Google Scholar]
- 18.Jia YL, Fu MK, Ma L. Long-term outcome of secondary alveolar bone grafting in patients with various types of cleft. Br J Oral Maxillofac Surg. 2006;44:308–312. doi: 10.1016/j.bjoms.2005.07.003. [DOI] [PubMed] [Google Scholar]
- 19.Mossey PA, Clark JD, Gray D. Preliminary investigation of a modified Huddart/Bodenham scoring system for assessment of maxillary arch constriction in unilateral cleft lip and palate subjects. Eur J Orthod. 2003;25:251–257. doi: 10.1093/ejo/25.3.251. [DOI] [PubMed] [Google Scholar]
- 20.Derijcke A, Kuijpers-Jagtman AM, Lekkas C, Hardjowasito W, Latief B. Dental arch dimensions in unoperated adult cleft-palate patients: an analysis of 37 cases. J Craniofac Genet Dev Biol. 1994;14:69–74. [PubMed] [Google Scholar]
- 21.Kurt G, Bayram M, Uysal T, Ozer M. Mandibular asymmetry in cleft lip and palate patients. Eur J Orthod. 2010;32:19–23. doi: 10.1093/ejo/cjp063. [DOI] [PubMed] [Google Scholar]
- 22.Suri S, Utreja A, Khandelwal N, Mago SK. Craniofacial computerized tomography analysis of the midface of patients with repaired complete unilateral cleft lip and palate. Am J Orthod Dentofacial Orthop. 2008;134:418–429. doi: 10.1016/j.ajodo.2006.09.065. [DOI] [PubMed] [Google Scholar]
- 23.Wijdeveld MG, Maltha JC, Grupping EM, De Jonge J, Kuijpers-Jagtman AM. A histological study of tissue response to simulated cleft palate surgery at different ages in beagle dogs. Arch Oral Biol. 1991;36:837–843. doi: 10.1016/0003-9969(91)90033-q. [DOI] [PubMed] [Google Scholar]