

Supplemental Digital Content is Available in the Text.
Background:
RESCUE and REVERSE were 2 Phase 3 clinical trials that assessed the efficacy and safety of intravitreal gene therapy with lenadogene nolparvovec (rAAV2/2-ND4) for the treatment of Leber hereditary optic neuropathy (LHON). RESTORE is the long-term follow-up study of subjects treated in the RESCUE and REVERSE trials.
Methods:
In RESCUE and REVERSE, 76 subjects with LHON because of the m.11778 G>A mutation in the mitochondrial gene ND4 received a single unilateral intravitreal injection of lenadogene nolparvovec. After 96 weeks, 61 subjects were enrolled in the long-term follow-up study RESTORE. The best-corrected visual acuity (BCVA) was assessed over a period of up to 52 months after onset of vision loss. A locally estimated scatterplot smoothing regression model was used to analyze changes in BCVA over time. Vision-related quality of life was reported using the visual function questionnaire-25 (VFQ-25).
Results:
The population of MT-ND4 subjects enrolled in RESTORE was representative of the combined cohorts of RESCUE and REVERSE for mean age (35.1 years) and gender distribution (79% males). There was a progressive and sustained improvement of BCVA up to 52 months after the onset of vision loss. The final mean BCVA was 1.26 logarithm of the minimal angle of resolution 48 months after the onset of vision loss. The mean VFQ-25 composite score increased by 7 points compared with baseline.
Conclusion:
The treatment effect of lenadogene nolparvovec on BCVA and vision-related quality of life observed 96 weeks (2 years) after treatment in RESCUE and REVERSE was sustained at 3 years in RESTORE, with a maximum follow-up of 52 months (4.3 years) after the onset of vision loss.
Leber hereditary optic neuropathy (LHON) is a rare maternally inherited mitochondrial disease that primarily affects retinal ganglion cells (RGCs) and leads to irreversible bilateral, often sequential, severe vision loss (1). Three primary point mutations affecting mitochondrial DNA (mtDNA) are responsible for 90% of LHON cases (2): m.11778G>A in the MT-ND4 gene, m.3460G>A in the MT-ND1 gene, and m.14484T>C in the MT-ND6 gene. MT-ND genes encode the mtDNA-related subunits of complex I, a key component of the respiratory chain. The LHON mutations impair complex I activity, leading to decreased efficiency in adenosine triphosphate (ATP) synthesis, accumulation of reactive oxygen species, eventually leading to RGCs degeneration and apoptosis.
The m.11778G>A mutation is the most prevalent and is associated with a poor visual prognosis (3). A recent meta-analysis reported that only 14.4% of patients with LHON of all ages, and 11.3% of those aged 15 years or older, carrying the m.11778G>A mutation (hereafter referred to as MT-ND4 patients), had visual recovery, although definitions of “recovery” varied greatly among studies (3). LHON is an orphan disease, with yet unmet therapeutic needs. Despite the European approval under exceptional circumstances of the oral drug idebenone (a synthetic ubiquinone analog) for the treatment of LHON (2,4,5), there is still a pressing medical need for further therapies with significant benefit in LHON.
In the last decade, gene therapies for LHON were developed based on the allotopic nuclear expression of therapeutic mitochondrial genes. Lenadogene nolparvovec (rAAV2/2-ND4) is an adeno-associated viral vector containing the modified cDNA encoding the human wild-type mitochondrial ND4 protein, flanked by 2 mitochondrial targeting sequences. This expresses the therapeutic mRNA from the intranuclear episomes, which in turn is translated by ribosomes at the surface of mitochondria, and, ultimately, the resulting therapeutic ND4 protein is translocated into the mitochondrial matrix. The therapeutic ND4 protein can then integrate into complex I to restore the electron flow and respiration. In vitro, lenadogene nolparvovec was able to improve ATP synthesis in fibroblasts of MT-ND4 patients (6,7). In rodent models of LHON with ND4-induced complex I deficiency, lenadogene nolparvovec prevented optic atrophy and vision loss (8). Administered as a unilateral intravitreal injection to MT-ND4 patients, lenadogene nolparvovec showed a good safety profile in a phase 1/2 clinical trial including 5 years of follow-up after treatment administration (9). Two phase 3 clinical trials—RESCUE and REVERSE—assessed the efficacy and safety of a unilateral intravitreal injection of lenadogene nolparvovec within 1 year of visual loss in MT-ND4 patients (10,11). Unexpectedly, in the group of fellow eyes that received a sham injection, the best-corrected visual acuity (BCVA) improved similarly to the group of eyes injected with lenadogene nolparvovec. Two years after treatment administration, a clinically significant bilateral improvement of BCVA from nadir (i.e., the lowest individual BCVA recorded during the trials) was reported in both studies, with a mean gain between −0.46 and −0.57 logarithm of the minimal angle of resolution (logMAR) (+23 to +29 Early-Treatment Diabetic Retinopathy Study [ETDRS] letters equivalent) (10,11).
This report presents interim results of RESTORE, the long-term follow-up study of RESCUE and REVERSE, 3 years after treatment administration.
METHODS
Design of the RESCUE and REVERSE Trials and Their Long-Term Follow-Up Study RESTORE
RESCUE (NCT02652767) and REVERSE (NCT02652780) were 2 randomized, double-masked, sham-controlled, Phase 3 clinical trials assessing the efficacy of lenadogene nolparvovec gene therapy for the treatment of LHON in MT-ND4 subjects who had vision loss due to LHON in at least one eye and were at least 15 years old at screening. Each patient's right eye was randomized to receive either a single intravitreal injection of lenadogene nolparvovec (9E10 viral genomes in 90 μL) or a sham intravitreal injection (the blunt edge of a needleless syringe was applied at the regular site of injection). The contralateral left eye received the treatment not allocated to the right eye. The objective was to evaluate the efficacy of lenadogene nolparvovec compared with a sham injection at weeks 48 (primary endpoint) and 96, using the difference in change in BCVA from baseline. The only difference between the 2 clinical trials was the duration of vision loss at screening, with RESCUE enrolling subjects with vision loss in at least one eye for less than 6 months and REVERSE enrolling subjects with vision loss for 6–12 months in both eyes.
Ninety-six weeks after treatment administration in RESCUE and REVERSE, subjects were offered to participate in RESTORE—the long-term follow-up study of RESCUE and REVERSE—for another 3 years, corresponding to 5 years post-treatment administration (Fig. 1).
FIG. 1.
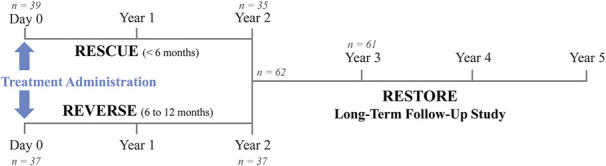
Study design of RESCUE and REVERSE and their long-term follow-up study RESTORE. RESCUE and REVERSE subjects were followed for 2 years (96 weeks) after which they were offered to participate in the long-term follow-up study RESTORE. The average time between the onset of vision loss and treatment administration was 3.9 months in RESCUE subjects and 9.8 months in REVERSE subjects. n: number of study participants at key time points.
Outcome Measures
In this publication, we report the outcome measures of BCVA and vision-related quality of life. BCVA was assessed using the Early-Treatment Diabetic Retinopathy Study letter chart at 1 or 4 m. Quality of life was monitored using the National Eye Institute (NEI) Visual Function Questionnaire (VFQ)-25, the 25-item version of the 51-item NEI Visual Function Questionnaire. The VFQ-25 consists of 25 vision-targeted questions representing 11 vision-related constructs, plus an additional single-item general health rating question. The overall composite score for the VFQ-25 is the average of the vision-targeted subscales scores, excluding the general health rating question (12).
Data Analyses
The RESTORE long-term follow-up study is still ongoing. A database freeze was performed on May 29, 2020, when all the active participants had completed their year 3 visit. One RESCUE subject who had received a partial dose of lenadogene nolparvovec was included in the analysis as a conservative approach.
Handling of Best-Corrected Visual Acuity Data
All BCVA measures were converted into logMAR. On-chart BCVA was converted into logMAR using the standard formula (13). Off-chart BCVA of counting fingers and hand motion were assigned a value of 2.0 and 2.3 logMAR, respectively, as described by Lange et al (14). Eyes with light perception and no light perception vision were assigned an arbitrary value of 4.0 and 4.5 logMAR, respectively.
Visual Function Questionnaire-25
Because all subjects received the active product, the treatment effect of lenadogene nolparvovec on the patients' quality of life was assessed in all subjects. The change from baseline of the VFQ-25 composite score and subscale scores was measured in each patient. A 4-point to 6-point change in NEI VFQ-25 scores represents a clinically meaningful change for each score (15).
Statistical Analysis
We explored graphically the evolution of BCVA starting at 12 months after vision loss, at which time all REVERSE and RESCUE patients would have been treated with lenadogene nolparvovec, using a locally estimated scatterplot smoothing (LOESS) nonparametric local regression model in which each patient's eyes were considered independently. Owing to the contralateral effect of lenadogene nolparvovec previously demonstrated in RESCUE and REVERSE (10,11), all eyes were included in this analysis regardless of whether they had received an injection of lenadogene nolparvovec or a sham injection. The smoothing parameter of the LOESS model was based on the corrected Akaike Information Criterion (AICc) (SAS default method with values from 0.3 to 0.6). The LOESS curve was presented with a 95% confidence interval (CI).
RESULTS
Characteristics of the Analyzed Population and Follow-Up Time
A total of 76 patients (152 eyes) were treated in the RESCUE and REVERSE trials. The RESCUE trial included 39 subjects and was completed in September 2019. The REVERSE trial included 37 subjects and was completed in April 2019. Subjects were mostly male (80.3%) with a mean (SD) age of 35.0 (15.3) years (Table 1). Nine (11.8%) subjects were below the age of 18 (Table 1).
TABLE 1.
Characteristics of the analyzed population
| Demographics* | Subjects in RESCUE and REVERSE n = 76 |
Subjects in RESTORE n = 61 |
| Sex, n (%) | ||
| Male | 61 (80.3%) | 48 (78.7%) |
| Female | 15 (19.7%) | 13 (21.3%) |
| Age at onset, yrs | ||
| Mean (SD) | 35.0 (15.3) | 35.1 (15.4) |
| Min, max | 15–69 | 15–69 |
| Subjects <18 yrs old at onset, n (%)* | ||
| Yes | 9 (11.8%) | 7 (11.5%) |
| No | 67 (88.2%) | 54 (88.5%) |
Subjects had to be at least 15 years old to be enrolled in RESCUE and REVERSE.
Of the 76 subjects, 72 completed the 2-year study follow-up and 62 (86.1%) agreed to participate in the long-term follow-up study RESTORE. One patient discontinued the RESTORE study before attending the first visit, scheduled 2.5 years after treatment administration, and was therefore excluded from the demographics analysis of RESTORE (n = 61) (Fig. 1).
Subjects enrolled in RESTORE were mostly male (78.7%) and had a mean (SD) age of 35.1 (15.4) years, including 7 (11.4%) subjects below the age of 18 years when initially enrolled in REVERSE and RESCUE (Table 1).
The mean number of visual acuity assessments per patient was 26.8. Patients had a median follow-up duration after vision loss of 39.8 months, with a quarter of patients followed for more than 44.1 months and a maximal follow-up of 51.5 months.
Visual Outcomes
Patients received treatment between 2.3 and 12.8 months after onset of vision loss (median 6.5 months; mean 7.4 months). Half of the eyes (53.8%) had received treatment at Month 6 ([3–9] months) after vision loss, nearly all eyes (92.7%) were treated at Month 12 ([9–15] months), and all patients (100%) at Month 18 ([15–21] months). We started BCVA analyses at Month 12, when 92.7% of eyes (139/150) had received treatment (Table 2). The LOESS analysis was run using all the BCVA data collected in the 152 eyes of subjects treated in RESCUE and REVERSE, from Month 12 to the last available measure, corresponding to 51.5 months after the onset of vision loss for the last available data point in the RESTORE study.
TABLE 2.
Evolution of the best-corrected visual acuity (BCVA) in MT-ND4 patients treated with lenadogene nolparvovec
| BCVA—LogMAR | |
| 12 (9–15) months after the onset of vision loss | |
| n (eyes) | 150 |
| Mean BCVA (SD) | 1.57 (0.55) |
| 95% CI | 1.48; 1.66 |
| 18 (15–21) months after the onset of vision loss | |
| n (eyes) | 149 |
| Mean BCVA (SD) | 1.46 (0.51) |
| 95% CI | 1.38; 1.54 |
| 24 (21–30) months after the onset of vision loss | |
| n (eyes) | 146 |
| Mean BCVA (SD) | 1.40 (0.59) |
| 95% CI | 1.30; 1.50 |
| 36 (30–42) months after the onset of vision loss | |
| n (eyes) | 128 |
| Mean BCVA (SD) | 1.33 (0.59) |
| 95% CI | 1.23; 1.44 |
| 48 (42–54) months after the onset of vision loss | |
| n (eyes) | 62 |
| Mean BCVA (SD) | 1.26 (0.45) |
| 95% CI | 1.14; 1.37 |
At each time point, the mean and 95% CIs were calculated on the individual BCVA data collected in the period indicated between brackets. For example, the 12-month mean BCVA is the average of 150 individual BCVA data points collected between 9 and 15 months after the onset of vision loss.
CI, confidence interval; logMAR, logarithm of the minimal angle resolution.
The LOESS regression model based on a scatterplot of individual BCVA data showed a progressive and sustained BCVA improvement from 12 to 51.5 months after onset (Fig. 2). The mean (SD) BCVA steadily improved from 1.57 (0.55) logMAR at 12 months after the onset of vision loss to 1.26 (0.45) logMAR at 48 months after onset (Table 2). The mean BCVA of MT-ND4 subjects remained on-chart, that is, better than 1.6 logMAR, throughout the follow-up period. The absolute difference in change from baseline between drug-treated and sham-treated eyes was 0.006 logMAR 2 years after treatment administration and 0.018 logMAR 3 years after treatment administration.
FIG. 2.
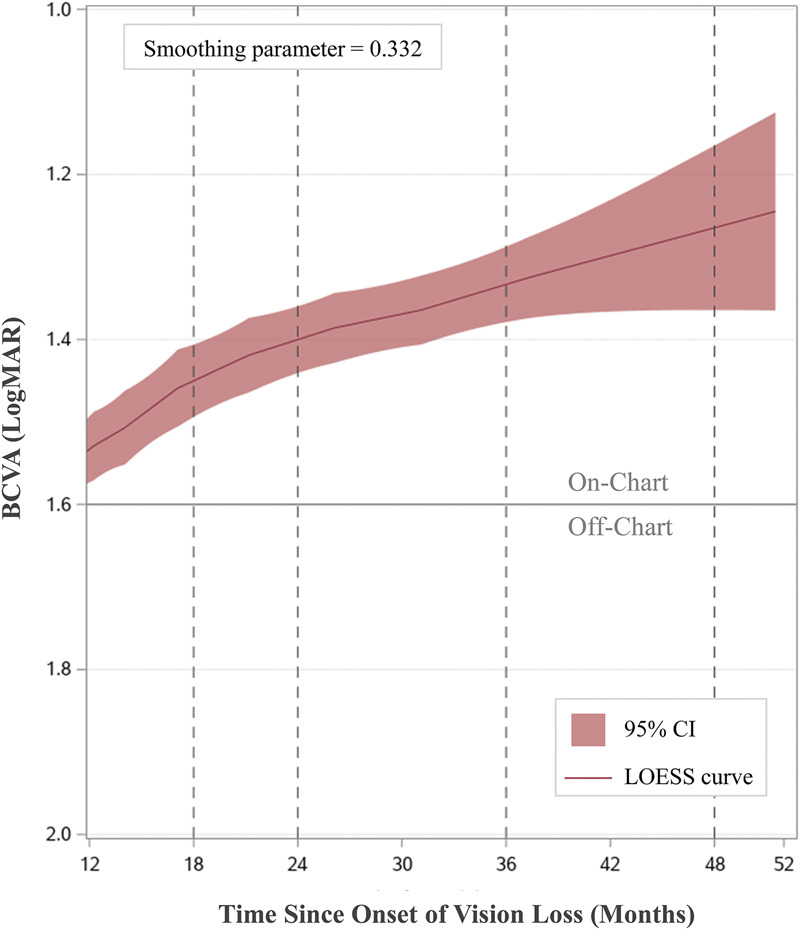
Evolution of the best-corrected visual acuity (BCVA) in MT-ND4-LHON subjects treated in RESCUE and REVERSE. The LOESS curve of the evolution of BCVA in all eyes is presented over time from 12 months to 51.5 months (last available data point) after the onset of vision loss.
Quality of Life
Most of the VFQ-25 metrics showed a clinically meaningful improvement from baseline to week 96: mental health (+16 points), dependency (+13 points), role difficulties (+12 points), near activities (+5 points), and general vision (+5 points). Overall, the composite score showed a clinically meaningful improvement of +4 points. At 3 years after treatment, a clinically meaningful overall improvement of quality of life was reported, with a mean gain of 7 points from baseline for the composite score (Table 3). Similarly, many subscales showed a clinically meaningful improvement from baseline: mental health (+21 points), role difficulties (+17 points), dependency (+15 points), general vision (+9 points), near activities (+6 points), and distance activities (+5 points) (Table 3).
TABLE 3.
Change in the visual function questionnaire-25 items (VFQ-25) subscale score at year 3 post-treatment administration
| VFQ-25 Subscales* | Baseline Score† Mean (SD) |
Change From Baseline at 3 Years After Treatment Administration |
| Mean (SD)† | ||
| Composite score | 46.2 (16.3) | +6.9 (20.1)‡ |
| Mental health | 30.0 (21.5) | +21.2 (25.7)‡ |
| Role difficulties | 31.4 (26.3) | +16.8 (31.9)‡ |
| Dependency | 32.5 (25.8) | +15.0 (33.6)‡ |
| General vision | 34.3 (16.5) | +9.0 (22.2)‡ |
| Near activities | 27.3 (20.4) | +5.9 (25.8)‡ |
| Distance activities | 38.4 (20.4) | +5.5 (26.5)‡ |
| Social functioning | 46.9 (25.5) | +3.5 (30.4) |
| Color vision | 72.5 (28.8) | −0.8 (34.2) |
| Peripheral vision | 61.9 (26.9) | −1.2 (34.3) |
| Ocular pain | 87.9 (18.0) | −7.8 (21.9) |
Subscales not reported in this table: general health (missing values) and driving (not applicable to LHON).
Mean scores calculated in the 61 subjects who completed the year 3 visit.
Scores and subscores with a clinically meaningful improvement (15).
DISCUSSION
Long-term follow-up of MT-ND4 subjects included in the RESCUE and REVERSE studies who were treated with a single unilateral intravitreal injection of lenadogene nolparvovec demonstrated a progressive and sustained improvement of BCVA in both eyes and improvement of quality of life up to 52 months after the onset of vision loss.
Sixty-two of 72 subjects who completed RESCUE or REVERSE agreed to participate in RESTORE. This substantial retention rate of 86% indicates that the RESTORE cohort is a representative of the entire study population. Indeed, the demographics of the RESTORE cohort of MT-ND4 subjects were very similar to the population originally treated. The mean age at onset and gender distribution in RESCUE, REVERSE, and RESTORE also corresponded to the typical LHON demographics reported in the literature (1,2).
The evolution of BCVA after treatment with lenadogene nolparvovec showed a progressive and sustained improvement up to 51.5 months (4.3 years) after the onset of vision loss. The mean BCVA of treated subjects remained clearly on-chart, contrary to the natural history of the disease reported in MT-ND4 patients aged 15 and over at onset (3). Importantly, the continuous improvement of BCVA was reported in both eyes of unilaterally treated subjects, confirming the contralateral treatment effect of lenadogene nolparvovec reported at earlier time points in the RESCUE and REVERSE trials (10,11). Indeed, the absolute difference in change from baseline between drug-treated and sham-treated eyes was similar 2 and 3 years after treatment administration.
Because all MT-ND4 subjects were treated with lenadogene nolparvovec, an intrapatient comparison before and after treatment was used to assess the impact of treatment on quality of life, highlighting daily benefits experienced by each treated patient. In the overall REVERSE and RESCUE population, most of the quality-of-life metrics showed a clinically meaningful improvement from baseline to week 96, consistent with reported improvement of the visual acuity (10,11). Similarly at 3 years after treatment, this clinically meaningful improvement of most metrics was maintained, consistent with the persistence of the treatment effect of lenadogene nolparvovec on BCVA. The worsening of the ocular pain score (Table 3) may be related to the occurrence of intraocular inflammation experienced by some patients during the REVERSE and RESCUE studies (10,11).
By design, gene therapy is assumed to be a treatment with a one-time administration. As such, the long-term benefits of a single dose of gene therapy need to be persistent over time. Here, we report that the efficacy of a single unilateral intravitreal injection of lenadogene nolparvovec on visual acuity and vision-related quality of life was clinically meaningful and sustained up to 4.3 years after the onset of vision loss. This report sheds promising light on the use of gene therapy in LHON, a disease with a pressing medical need for therapies with significant benefit.
STATEMENT OF AUTHORSHIP
Category 1: a. Conception and design: V. Biousse, N. J. Newman, P. Yu-Wai-Man, V. Carelli, M. L. Moster, C. Vignal-Clermont, T. Klopstock, A. A. Sadun, R. C. Sergott, and J.-A. Sahel; b. Acquisition of data: V. Biousse, N. J. Newman, P. Yu-Wai-Man, V. Carelli, M. L. Moster, C. Vignal-Clermont, T. Klopstock, A. A. Sadun, R. Hage, S. Esposti, C. La Morgia, C. Priglinger, and R. Karanja; c. Analysis and interpretation of data: V. Biousse, N. J. Newman, P. Yu-Wai-Man, C. Vignal-Clermont, L.Blouin, and M. Taiel. Category 2: a. Drafting the manuscript: L. Blouin, V. Biousse, M. Taiel, N. J. Newman, P. Yu-Wai-Man, V. Carelli, and J.-A. Sahel. Category 3: a. Final approval of the completed manuscript: V. Biousse, N. J. Newman, P. Yu-Wai-Man, V. Carelli, M. L. Moster, C. Vignal-Clermont, T. Klopstock, A. A. Sadun, R. C. Sergott, R. Hage, S. Esposti, C. La Morgia, C. Priglinger, R. Karanja, L. Blouin, M. Taiel, and J.-A. Sahel.
ACKNOWLEDGMENTS
The authors thank the patients who took part in REVERSE, RESCUE, and RESTORE studies. The authors are grateful to the study teams that have contributed to the conduct of REVERSE, RESCUE, and RESTORE studies, in the various recruitment centers. The names of centers and study teams' members are listed in the Supplemental Digital Content 1 (see LHON Study Group, http://links.lww.com/WNO/A496).
Footnotes
GenSight Biologics (Paris, France) fully funded and sponsored the studies. V. Biousse is supported in part by an ophthalmology department core grant from the NIH/NEI (P30 EY006360). N. J. Newman is supported in part by an ophthalmology department core grant from the NIH/NEI (P30 EY006360). P. Yu-Wai-Man is supported by a Clinician Scientist Fellowship Award (G1002570) from the Medical Research Council (UK) and also receives funding from Fight for Sight (UK), the Isaac Newton Trust (UK), Moorfields Eye Charity, the Addenbrooke's Charitable Trust, the National Eye Research Centre (UK), the International Foundation for Optic Nerve Disease (IFOND), the UK National Institute of Health Research (NIHR) as part of the Rare Diseases Translational Research Collaboration, the NIHR Cambridge Biomedical Research Centre (BRC-1215-20014), and the NIHR Biomedical Research Centre based at Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. V. Carelli is supported by grants from the Italian Ministry of Health (RF-2018-12366703), the Italian Ministry of Research (20172T2MHH), and Telethon-Italy (GUP15016). V. Carelli is also supported by patients' organizations MITOCON and IFOND and patients' donations. T. Klopstock is supported by the German Federal Ministry of Education and Research (BMBF, Bonn, Germany) through grants to the German Network for Mitochondrial Disorders (mitoNET, 01 GM1906A) and to the E-Rare project GENOMIT (01 GM1920B). J. A. Sahel is supported by the Agence Nationale de la Recherche within the Programme Investissements d’Avenir, Institut Hospitalo Universitaire FOReSIGHT (ANR-18-IAHU-0001) and LabEx LIFESENSES (ANR-10-LABX-65) and by an unrestricted grant from Research to Prevent Blindness.
V. Biousse is a consultant for GenSight Biologics and Neurophoenix. N. J. Newman is a consultant for GenSight Biologics, Santhera Pharmaceuticals, Stealth BioTherapeutics, and Neurophoenix and has received research support from GenSight and Santhera Pharmaceuticals. P. Yu-Wai-Man is a consultant for GenSight Biologics and Stealth BioTherapeutics and has received research support from GenSight Biologics and Santhera Pharmaceuticals. V. Carelli is a consultant for Santhera Pharmaceuticals, GenSight Biologics, and Stealth BioTherapeutics and has received research support from Santhera Pharmaceuticals and Stealth BioTherapeutics. M. L. Moster is a consultant for GenSight Biologics and has received research support from GenSight Biologics. C. Vignal-Clermont is a consultant for Santhera Pharmaceuticals and GenSight Biologics. T. Klopstock is a consultant for Santhera Pharmaceuticals and GenSight Biologics and has received research support from Santhera Pharmaceuticals and GenSight Biologics. A. A. Sadun is a consultant for Stealth BioTherapeutics. L. Blouin and M. Taiel are GenSight Biologics employees. J. A. Sahel is a cofounder and shareholder of GenSight Biologics and a patent coauthor on allotopic transport.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the full text and PDF versions of this article on the journal's Web site (www.jneuro-ophthalmology.com).
Clinical Trial Numbers: (ClinicalTrials.gov) REVERSE: NCT02652780; RESCUE: NCT02652767; and RESTORE: NCT03406104.
Contributor Information
Nancy J. Newman, Email: ophtnjn@emory.edu.
Patrick Yu-Wai-Man, Email: py237@cam.ac.uk.
Valerio Carelli, Email: valerio.carelli@unibo.it.
Mark L. Moster, Email: markmoster@gmail.com.
Catherine Vignal-Clermont, Email: cvignal@for.paris.
Thomas Klopstock, Email: thomas.klopstock@med.uni-muenchen.de.
Alfredo A. Sadun, Email: alfredo.sadun@gmail.com.
Robert C. Sergott, Email: rcs220@comcast.net.
Rabih Hage, Email: rhage@for.paris.
Simona Esposti, Email: Simona.Esposti@moorfields.nhs.uk.
Chiara La Morgia, Email: chiaralamorgia@gmail.com.
Claudia Priglinger, Email: claudia.priglinger@med.uni-muenchen.de.
Rustum Karanja, Email: karanjiar@gmail.com.
Laure Blouin, Email: lblouin@gensight-biologics.com.
Magali Taiel, Email: mtaiel@gensight-biologics.com.
José-Alain Sahel, Email: jose.sahel@gmail.com.
REFERENCES
- 1.Riordan-Eva P, Sanders MD, Govan GG, Sweeney MG, Da Costa J, Harding AE. The clinical features of Leber's hereditary optic neuropathy defined by the presence of a pathogenic mitochondrial DNA mutation. Brain. 1995;118:319–337. [DOI] [PubMed] [Google Scholar]
- 2.Carelli V, Carbonelli M, de Coo IF, Kawasaki A, Klopstock T, Lagrèze WA, La Morgia C, Newman NJ, Orssaud C, Pott JW, Sadun AA, van Everdingen J, Vignal-Clermont C, Votruba M, Yu-Wai-Man P, Barboni P. International consensus statement on the clinical and therapeutic management of Leber hereditary optic neuropathy. J Neuroophthalmol. 2017;37:371–381. [DOI] [PubMed] [Google Scholar]
- 3.Newman NJ, Carelli V, Taiel M, Yu-Wai-Man P. Visual outcomes in Leber hereditary optic neuropathy patients with the m.11778G>A (MTND4) mitochondrial DNA mutation. J Neuroophthalmol. 2020;40:547–557. [DOI] [PubMed] [Google Scholar]
- 4.Klopstock T, Yu-Wai-Man P, Dimitriadis K, Rouleau J, Heck S, Bailie M, Atawan A, Chattopadhyay S, Schubert M, Garip A, Kernt M, Petraki D, Rummey C, Leinonen M, Metz G, Griffiths PG, Meier T, Chinnery PF. A randomized placebo-controlled trial of idebenone in Leber's hereditary optic neuropathy. Brain. 2011;134:2677–2686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Catarino CB, von Livonius B, Priglinger C, Banik R, Matloob S, Tamhankar MA, Castillo L, Friedburg C, Halfpenny CA, Lincoln JA, Traber GL, Acaroglu G, Black GC, Doncel C, Fraser CL, Jakubaszko J, Landau K, Langenegger SJ, Muñoz-Negrete FJ, Newman NJ, Poulton J, Scoppettuolo E, Subramanian P, Toosy AT, Vidal M, Vincent AL, Votruba M, Zarowski M, Zermansky A, Lob F, Rudolph G, Mikazans O, Silva M, Llòria X, Metz G, Klopstock T. Real-world clinical experience with idebenone in the treatment of Leber hereditary optic neuropathy. J Neuroophthalmol. 2020;40:558–565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bonnet C, Augustin S, Ellouze S, Bénit P, Bouaita A, Rustin P, Sahel JA, Corral-Debrinski M. The optimized allotopic expression of ND1 or ND4 genes restores respiratory chain complex I activity in fibroblasts harboring mutations in these genes. Biochim Biophys Acta. 2008;1783:1707–1717. [DOI] [PubMed] [Google Scholar]
- 7.Bonnet C, Kaltimbacher V, Ellouze S, Augustin S, Bénit P, Forster V, Rustin P, Sahel JA, Corral-Debrinski M. Allotopic mRNA localization to the mitochondrial surface rescues respiratory chain defects in fibroblasts harboring mitochondrial DNA mutations affecting complex I or V subunits. Rejuvenation Res. 2007;10:127–144. [DOI] [PubMed] [Google Scholar]
- 8.Cwerman-Thibault H, Augustin S, Lechauve C, Ayache J, Ellouze S, Sahel JA, Corral-Debrinski M. Nuclear expression of mitochondrial ND4 leads to the protein assembling in complex I and prevents optic atrophy and visual loss. Mol Ther Methods Clin Dev. 2015;2:15003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Vignal-Clermont C, Girmens JF, Audo I, Said SM, Errera MH, Plaine L, O'Shaughnessy D, Taiel M, Sahel JA. Safety of intravitreal gene therapy for treatment of subjects with Leber hereditary optic neuropathy due to mutations in the mitochondrial ND4 gene: the REVEAL study. BioDrugs. 2021;35:201–214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Newman NJ, Yu-Wai-Man P, Carelli V, Moster ML, Biousse V, Vignal-Clermont C, Sergott RC, Klopstock T, Sadun AA, Barboni P, DeBusk AA, Girmens JF, Rudolph G, Karanjia R, Taiel M, Blouin L, Smits G, Katz B, Sahel JA; LHON Study Group. Efficacy and safety of intravitreal gene therapy for Leber hereditary optic neuropathy treated within 6 months of disease onset. Ophthalmology. 2021;128:649–660. [DOI] [PubMed] [Google Scholar]
- 11.Yu-Wai-Man P, Newman NJ, Carelli V, Moster ML, Biousse V, Sadun AA, Klopstock T, Vignal-Clermont C, Sergott RC, Rudolph G, La Morgia C, Karanjia R, Taiel M, Blouin L, Burguière P, Smits G, Chevalier C, Masonson H, Salermo Y, Katz B, Picaud S, Calkins DJ, Sahel JA. Bilateral visual improvement with unilateral gene therapy injection for Leber hereditary optic neuropathy. Sci Transl Med. 2020;12:eaaz7423. [DOI] [PubMed] [Google Scholar]
- 12.Mangione CM, Lee PP, Pitts J, Gutierrez P, Berry S, Hays RD. Psychometric properties of the national eye Institute visual function questionnaire (NEI-VFQ). Arch Ophthalmol. 1998;116:1496–1504. [DOI] [PubMed] [Google Scholar]
- 13.Holladay JT. Proper method for calculating average visual acuity. J Refract Surg. 1997;13:388–391. [DOI] [PubMed] [Google Scholar]
- 14.Lange C, Feltgen N, Junker B, Schulze-Bonsel K, Bach M. Resolving the clinical acuity categories ‟hand motion” and ‟counting fingers” using the Freiburg Visual Acuity Test (FrACT). Graefes Arch Clin Exp Ophthalmol. 2009;247:137–142. [DOI] [PubMed] [Google Scholar]
- 15.Suñer IJ, Kokame GT, Yu E, Ward J, Dolan C, Bressler NM. Responsiveness of NEI VFQ-25 to changes in visual acuity in neovascular AMD: validation studies from two phase 3 clinical trials. Invest Ophthalmol Vis Sci. 2009;50:3629–3635. [DOI] [PubMed] [Google Scholar]