

Abstract
Background
Delirium frequently occurs among patients admitted to the intensive care unit (ICU). There is limited evidence to support interventions to treat or resolve delirium in patients who have already developed delirium. Therefore, the early recognition and prevention of delirium are important in the management of critically ill patients.
Objective
This study aims to develop and validate a delirium prediction model within 24 hours of admission to the ICU using electronic health record data. The algorithm was named the Prediction of ICU Delirium (PRIDE).
Methods
This is a retrospective cohort study performed at a tertiary referral hospital with 120 ICU beds. We only included patients who were 18 years or older at the time of admission and who stayed in the medical or surgical ICU. Patients were excluded if they lacked a Confusion Assessment Method for the ICU record from the day of ICU admission or if they had a positive Confusion Assessment Method for the ICU record at the time of ICU admission. The algorithm to predict delirium was developed using patient data from the first 2 years of the study period and validated using patient data from the last 6 months. Random forest (RF), Extreme Gradient Boosting (XGBoost), deep neural network (DNN), and logistic regression (LR) were used. The algorithms were externally validated using MIMIC-III data, and the algorithm with the largest area under the receiver operating characteristics (AUROC) curve in the external data set was named the PRIDE algorithm.
Results
A total of 37,543 cases were collected. After patient exclusion, 12,409 remained as our study population, of which 3816 (30.8%) patients experienced delirium incidents during the study period. Based on the exclusion criteria, out of the 96,016 ICU admission cases in the MIMIC-III data set, 2061 cases were included, and 272 (13.2%) delirium incidents occurred. The average AUROCs and 95% CIs for internal validation were 0.916 (95% CI 0.916-0.916) for RF, 0.919 (95% CI 0.919-0.919) for XGBoost, 0.881 (95% CI 0.878-0.884) for DNN, and 0.875 (95% CI 0.875-0.875) for LR. Regarding the external validation, the best AUROC were 0.721 (95% CI 0.72-0.721) for RF, 0.697 (95% CI 0.695-0.699) for XGBoost, 0.655 (95% CI 0.654-0.657) for DNN, and 0.631 (95% CI 0.631-0.631) for LR. The Brier score of the RF model is 0.168, indicating that it is well-calibrated.
Conclusions
A machine learning approach based on electronic health record data can be used to predict delirium within 24 hours of ICU admission. RF, XGBoost, DNN, and LR models were used, and they effectively predicted delirium. However, with the potential to advise ICU physicians and prevent ICU delirium, prospective studies are required to verify the algorithm’s performance.
Keywords: clinical prediction, delirium, electronic health record, intensive care unit, machine learning
Introduction
Delirium, defined as acute brain dysfunction characterized by disturbances of awareness, attention, and cognition with a fluctuating course linked with an underlying medical condition, frequently occurs among patients admitted to intensive care units (ICUs) [1]. Up to 80% of critically ill patients affected by delirium are at an increased risk of requiring ventilation for a substantially long duration, high hospital and ICU mortality, and long-term cognitive impairment. The medical care for these patients also results in increased medical costs [2-4].
There is currently limited evidence to support interventions to treat or resolve delirium in patients who have already developed delirium [5]. Therefore, the early recognition and prevention of delirium are indispensable for patients with a high risk of developing delirium. Previous studies have shown that a proportion of the cases of delirium may be avoidable [6]. Accordingly, several prediction models have been developed to predict delirium in patients who may benefit from delirium prevention [7-9]. The models developed thus far focus on predicting delirium during the entire ICU stay using predisposing clinical features obtained within 24 hours of ICU admission or immediately upon ICU admission. Considering that ICU patients experience dynamic changes in medical conditions within the initial 24 hours after ICU admission, these models are limited because they focus on predicting only the long-term occurrence of delirium during the entire ICU stay. Furthermore, these prediction models only include variables that have already been identified as risk factors for delirium in other studies [7,9,10].
Therefore, we developed a machine learning–based model for the early prediction of delirium among medical and surgical ICU patients using electronic health record (EHR) data. This prediction model uses data obtained within 4 hours of ICU admission to predict delirium within 24 hours after ICU admission.
Methods
Study Setting and Population
We conducted a retrospective study of all critically ill patients admitted to the ICUs of the Samsung Medical Center (a 1989-bed university-affiliated, tertiary referral hospital in Seoul, South Korea) from July 1, 2016, to August 31, 2019. We only included patients who were 18 years or older at the time of admission and who stayed in the medical or surgical ICU. Patients were excluded if they lacked a Confusion Assessment Method for the ICU (CAM-ICU) record from the day of ICU admission or if they had a positive CAM-ICU record at the time of ICU admission. The flow diagram in Figure 1 shows the patient selection process. The study protocol was removed from all identifiers and approved by the SMC (Samsung Medical Center) Institutional Review Board (IRB No. 2020-02-026), as all identifiers were removed. The IRB approval form is presented in Multimedia Appendix 1.
Figure 1.
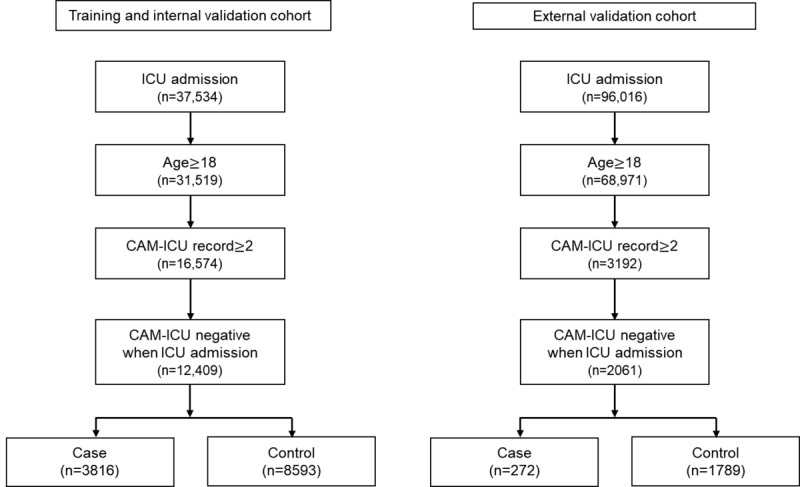
Flow diagram of the participant selection process. CAM-ICU: confusion assessment method for the intensive care unit; ICU: intensive care unit.
Source of Data
This study used data from the Clinical Data Warehouse Darwin-C database of the SMC and the Medical Information Mart for Intensive Care III (MIMIC-III) database (v1.4). The SMC data set was used for the derivation and validation cohort, and the MIMIC-III data set was used for the external validation cohort. The MIMIC-III database is a clinical database consisting of data from more than 38,000 ICU patients (medical, surgical, trauma-surgical, coronary, and cardiac-surgery data) admitted to Beth Israel Deaconess Medical center (Boston, MA) from June 2001 to October 2012 [11]. The MIMIC-III database can be accessed upon obtaining approval from its administrators.
Outcome
To screen for delirium, all ICU patients were assessed with the CAM-ICU [12]. The primary outcome of the study was the prediction of the occurrence of delirium within 24 hours of ICU admission. Delirium was defined as a negative CAM-ICU result obtained within the first 4 hours, and a positive CAM-ICU result obtained between 4 and 24 hours of ICU admission. In our institute, CAM-ICU results were obtained 3 times a day, and a senior nurse rechecked the recorded CAM-ICU scores.
Predictor Variables
We used clinical characteristics, ICU admission category (medical or surgical), primary cause of admission (respiratory, cardiovascular, gastrointestinal, neurology, perioperative, nephrology, metabolic, or trauma), primary diagnosis, vital signs, prescription medications, and laboratory test results as the predictor variables. All variables were extracted from the EHR data set.
Feature Selection and Data Processing
We first extracted all relevant variables for the prediction model from other studies. Next, 2 clinical experts (CRC and REK) reviewed the relevant variables and selected the crucial ones based on previous clinical studies and clinical relevance. We then further restricted the variables depending on whether they could be automatically extracted from EHRs and had low missing rates. Finally, for the external validation in the MIMIC-III data set, we selected variables found in both SMC and MIMIC-III. The MIMIC-III data set shows the final variables used as input for model development. The list of variables used is shown in Textbox 1, and the missing rate in the variable list is presented in Multimedia Appendix 2.
Variables used for model development.
General information
Age, sex, and invasive mechanical ventilation
Admission category
Medical intensive care unit (ICU) or surgical ICU
Reason for ICU admission
Respiratory, cardiovascular, gastrointestinal, neurology, perioperative, nephrology, metabolic, and trauma
Vital signs
Systolic blood pressure, diastolic blood pressure, heart rate, respiratory rate, peripheral capillary oxygen saturation, and Glasgow Coma Scale (eye, verbal, and motor)
Comorbidity
Charlson Comorbidity Index
Laboratory tests
-
Complete blood count:
white blood count, hemoglobin, hematocrit, platelet count, and erythrocyte sedimentation rate
-
Coagulation:
prothrombin time (INR) and activated partial thromboplastin time
-
Chemistry:
Total protein, albumin, total bilirubin, aspartate aminotransferase, alanine aminotransferase, glucose fasting, blood urea nitrogen, creatinine, phosphorus, sodium, potassium, magnesium, calcium (ionized), C-reactive protein quantitative, and lactic acid
-
Arterial Blood Gas Analysis:
pH, PaCO2, PaO2, HCO3, and O2 Saturation
Medications
Antibiotics, anticholinergic and antipsychotics, benzodiazepines, miscellaneous antidepressants, anxiolytics, sedatives and hypnotics, vasopressors, opiate agonists, opiate antagonists, cholinergic agents, and steroids
With regard to the general data processing, we first processed invalid values by eliminating them. Invalid values include extreme outliers in numerical values (for example, numerical values for vitals are eliminated using certain rules (ie, heart rate values should be between 0 and 300). Second, we processed numerical values by normalizing and scaling them. We performed standard normalization and min-max scaling such that the final numerical values were between 0 and 1. Finally, we processed the missing values. Missing values in the numerical data were filled with mean values, whereas missing values in categorical data were left blank such that the dummy variables were all equal to 0.
For certain variables with temporal information, such as vital values and laboratory test results, we determined statistical values such as the mean, standard deviation, min, max, and the closest values to the ICU admission to ensure multiple rows of numerical values can be summarized into one. Subsequently, to reduce the number of features necessary to train the model, we picked only one of the statistical values according to the feature importance of the random forest (RF). For example, there were initially multiple values for diastolic blood pressure (DBP) with respect to time. We calculated statistical values such as the mean, standard deviation, min, max, and the latest DBP values. Finally, we only selected the mean DBP because it was the most important among the statistical values of the DBP according to the feature importance of the RF.
Model Development and Validation
We split the data set into a development data set and a data set. For the development data set, we used the data obtained between July 1, 2016, and December 31, 2018. For the validation set, we used the data obtained between January 1, 2019, and August 31, 2019. Of the 37,543 admitted cases, 12,409 cases were selected in this study. These were divided into the development set (n=9589, 77.3%) and the internal validation set (n=2820, 22.7%). Among the 9589 cases in the development data set, there were 3060 (31.9%) cases of delirium, and among the 2820 cases in the validation data set, there were 756 (26.8%) cases of delirium. We did not apply specific methodology (eg, undersampling) to resolve the outcome imbalance problem because it was not extreme.
We employed RF, extreme gradient boosting (XGBoost), deep neural network (DNN), and logistic regression (LR) as the candidate prediction models.
Parameter Tuning
We also used an automated machine learning called the Tree-based Pipeline Optimization Tool for model selection and parameter searching [13].
For DNN, we used 512, 256, and 128 neurons for hidden layers, ReLU function for activation function in hidden layers, sigmoid function for activation function in the output layer, and binary cross-entropy function as the loss function. For XGBoost, we used a tree booster with 100 estimators, the learning rate as 0.1, and the subsample ratio as 0.75.
External Validation
After development and internal validation, we performed the external validation of our delirium prediction model using the MIMIC-III database. The validation set was extracted from the MIMIC-III database, which included patients with at least two CAM-ICU records obtained within at least 24 hours.
The model with the highest area under the receiver operating characteristics (AUROC) curve in the external validation was named the PRIDE (Prediction of ICU Delirium) algorithm.
Statistical Analysis
Continuous variables are presented in terms of means and SD, and categorical variables are presented in terms of their frequencies and percentages. The performances of the different models were compared using the AUROC, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) at the threshold. In the internal validation, model performance was evaluated through the average and 95% CI of the AUROCs. Additionally, we used a calibration curve and the Brier score to test the reliability of our model. To determine the clinically relevant threshold, we used a decision curve.
We employed the TRIPOD (Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis) statement to report the results of our prediction model. Data processing, statistical analysis, and the development and validation of the machine learning algorithms were performed using R version 3.6.2 [14] and Python version 3.6.8 [15].
The source code has been made available on Github [16].
Results
Study Population
During the study period, a total of 37,543 cases were collected. Patients who were 18 years or older at the time of ICU admission were included. Cases with less than two CAM-ICU records after admission to the ICU and those with a positive CAM-ICU upon ICU admission were excluded. After patient exclusion, 12,409 remained as our study population. The case group consisted of 3816 (30.8%) patients who experienced delirium incidents during the study period. With regard to the MIMIC-III (external validation) data set, patients younger than 18 years of age, those with less than two CAM-ICU records recorded within 24 hours, and those with positive CAM-ICU records upon ICU admission were excluded. Based on the exclusion criteria, out of the 96,016 ICU admission cases, 2061 cases were included, and 272 (13.2%) delirium incidents occurred.
Baseline characteristics of the training and test sets of the SMC and MIMIC-III data sets are shown in Table 1.
Table 1.
Baseline characteristics of data sets.
| Characteristics | Development | Internal validation | External validation (MIMIC-IIIa) | ||||||||||
|
|
Case (n=3060) | Control (n=6529) | Case (n=756) | Control (n=2064) | Case (n=272) | Control (n=1789) | |||||||
| Age (years), mean (SD) | 65.4 (14.4) | 61.1 (13.3) | 65.3 (14.7) | 59.7 (14.0) | 82.5 (59.7) | 73.7 (52.3) | |||||||
| Sex (male), n (%) | 1994 (65.2) | 4227 (64.7) | 466 (61.6) | 1190 (57.7) | 137 (50.4) | 925 (51.7) | |||||||
| Admission category, n (%) | |||||||||||||
|
|
Medical | 1431 (46.8) | 1639 (25.1) | 293 (38.8) | 344 (16.7) | 151 (55.5) | 1,141(63.8) | ||||||
|
|
Surgical | 1629 (53.2) | 4890 (74.9) | 1,720 (83.3) | 463 (61.2) | 121 (44.5) | 648(36.2) | ||||||
| Reason for ICUb admission, n (%) | |||||||||||||
|
|
Respiratory | 692 (22.6) | 374 (5.7) | 166 (22.0) | 71 (3.4) | 34 (12.5) | 247 (13.8) | ||||||
|
|
Cardiovascular | 480 (15.7) | 1166(17.9) | 105 (13.9) | 283 (13.7) | 73 (26.8) | 561 (31.4) | ||||||
|
|
Gastrointestinal | 145 (4.7) | 139 (2.1) | 28 (3.7) | 25 (1.2) | 55 (20.2) | 379 (21.2) | ||||||
|
|
Neurology | 102 (3.3) | 115 (1.8) | 46 (6.1) | 174 (8.4) | 57 (21.0) | 270 (15.1) | ||||||
|
|
Peri-operation | 1168 (38.2) | 4278 (65.5) | 320 (42.3) | 1448 (70.2) | 14 (5.1) | 81 (4.5) | ||||||
|
|
Nephrology | 83 (2.7) | 78 (1.2) | 17 (2.2) | 17 (0.8) | 4 (1.5) | 54 (3.0) | ||||||
|
|
Metabolic | 15 (0.5) | 6 (0.1) | 1 (0.1) | 0 (0.0) | 5 (1.8) | 85 (4.8) | ||||||
|
|
Hematology | 15 (0.5) | 22 (0.3) | 4 (0.5) | 6 (0.3) | 5 (1.8) | 33 (1.8) | ||||||
|
|
Trauma | 10 (0.3) | 10 (0.2) | 2 (0.3) | 0 (0.0) | 25 (9.2) | 79 (4.4) | ||||||
|
|
Others | 350 (11.4) | 341 (5.2) | 67 (8.9) | 40 (1.9) | — | — | ||||||
| Initial SOFAc, mean (SD) | 7.1 (3.6) | 3.2 (2.7) | 7.0 (3.7) | 2.8 (2.5) | 5.4 (3.3) | 3.1 (2.4) | |||||||
| Vasopressord, n (%) | 1,145 (37.4) | 793 (12.1) | 292 (38.6) | 175 (8.5) | 38 (14.0) | 71 (4.0) | |||||||
| Invasive mechanical ventilator, n (%) | 1,900 (62.1) | 1,165 (17.8) | 456 (60.3) | 344 (16.7) | 19 (7.0) | 73 (4.1) | |||||||
| CCIe, mean (SD) | 0.9 (2.2) | 0.3 (1.3) | 1.1 (2.5) | 0.4 (1.4) | 3.2 (1.8) | 2.8 (1.8) | |||||||
| Comorbidity, n (%) | |||||||||||||
|
|
Heart disease | 149 (4.9) | 123 (1.9) | 17 (2.2) | 20 (1.0) | 33 (12.1) | 232 (13.0) | ||||||
|
|
Stroke | 98 (3.2) | 33 (0.5) | 29 (3.8) | 24 (1.2) | 16 (5.9) | 57 (3.2) | ||||||
|
|
Malignancy | 434 (14.2) | 319 (4.9) | 80 (10.6) | 60 (2.9) | 5 (1.8) | 12 (0.7) | ||||||
|
|
Renal failure | 71 (2.3) | 99 (1.5) | 16 (2.1) | 26 (1.3) | 17 (12.1) | 106 (12.7) | ||||||
|
|
Liver disease | 146 (4.8) | 92 (1.4) | 23 (3.0) | 15 (0.7) | 38 (14.0) | 168 (9.4) | ||||||
|
|
Dementia | 55 (1.8) | 9 (0.1) | 17 (2.2) | 6 (0.3) | — | — | ||||||
| Vital signs, mean (SD) | |||||||||||||
|
|
Systolic BPf | 125.8 (24.7) | 127.4 (21.7) | 128.6 (26.4) | 130.8 (22.2) | 118.5 (25.0) | 119.5 (22.7) | ||||||
|
|
Diastolic BP | 71.6 (15.5) | 74.3 (14.1) | 72.3 (17.9) | 73.3 (14.7) | 63.3 (15.9) | 63.9 (15.4) | ||||||
|
|
Heart rate | 85.4 (20.7) | 80.7 (16.6) | 84.5 (20.5) | 80.6 (16.1) | 89.9 (20.3) | 85.8 (19.4) | ||||||
|
|
Respiratory rate | 19.3 (3.9) | 18.3 (2.5) | 18.8 (3.7) | 17.7 (2.5) | 20.5 (6.5) | 19.2 (5.4) | ||||||
|
|
SpO2g | 96.1 (5.5) | 96.9 (4.3) | 96.5 (4.0) | 97.4 (2.1) | 95.9 (3.6) | 96.2 (3.1) | ||||||
|
|
Body temperature (°C) | 36.7 (0.8) | 36.6 (0.5) | 36.7 (0.8) | 36.6 (0.4) | 36.8 (0.7) | 36.8 (0.6) | ||||||
| ABGAh, mean (SD) | |||||||||||||
|
|
pH | 7.4 (0.1) | 7.4 (0.1) | 7.4 (0.1) | 7.4 (0.1) | 7.4 (0.1) | 7.4 (0.1) | ||||||
|
|
PaCO2 | 35.5 (14.1) | 36.2 (7.5) | 35.3 (11.3) | 36.4 (6.2) | 42.0 (12.4) | 41.1 (12.1) | ||||||
|
|
PaO2 | 119.8 (83.4) | 184.4 (110.8) | 122.0 (82.5) | 190.4 (104.8) | 131.9 (106.0) | 125.0 (67.9) | ||||||
|
|
HCO3 | 22.0 (5.5) | 23.1 (3.6) | 22.0 (5.3) | 23.5 (2.9) | 24.1 (5.4) | 24.2 (4.7) | ||||||
aMIMIC-III: Medical Information Mart for Intensive Care III.
bICU: intensive care unit.
cSOFA: sequential organ failure assessment.
dVasopressor: epinephrine, norepinephrine, dobutamine, dopamine, vasopressin.
eCCI: Charlson Comorbidity Index.
fBP: blood pressure.
gSpO2: peripheral capillary oxygen saturation.
hABGA: arterial blood gas analysis.
Internal Validation
The average AUROCs and 95% CIs for internal validation were 0.919 (95% CI 0.919-0.919) for XGBoost, 0.916 (95% CI 0.916-0.916) for RF, 0.881 (95% CI 0.878-0.884) for DNN, and 0.875 (95% CI 0.875-0.875) for LR. For each model, we selected the highest value of specificity among sensitivities over 0.9 as the cut-off point for the threshold. The best model for the internal validation was XGBoost, with an AUROC of 0.919 (95% CI 0.919-0.919). Its sensitivity, specificity, PPV, and NPV were 0.904 (95% CI 0.904-0.905), 0.731 (95% CI 0.729-0.732), 0.565 (95% CI 0.563-0.566), and 0.952 (95% CI 0.952-0.952), respectively.
External Validation
For the external validation, the average AUROCs and 95% CI were 0.721 (95% CI 0.72-0.721) for RF, 0.697 (95% CI 0.695-0.699) for XGBoost, 0.655 (95% CI 0.654-0.657) for DNN, and 0.631 (95% CI 0.631-0.631) for LR. For the external validation on the MIMIC-III database, the model with the best AUROC was the RF model, with an AUROC of 0.721 and a sensitivity, specificity, PPV, and NPV of 0.91 (95% CI 0.909-0.912), 0.27 (95% CI 0.266-0.273), 0.159 (95% CI 0.159-0.16), and 0.952 (95% CI 0.951-0.953), respectively. A comparison of the performances of all of the models is shown in Table 2, and the ROC curves are shown in Figure 2.
Table 2.
Predictive performance of each model.
| Model and data set | AUROCa, mean (95% CI) | Sensitivity, mean (95% CI) | Specificity, mean (95% CI) | Positive predictive value, mean (95% CI) | Negative predictive value, mean (95% CI) | |
| Random forest | ||||||
|
|
Internal data set | 0.916 (0.916-0.916) | 0.904 (0.904-0.905) | 0.746 (0.744-0.747) | 0.579 (0.578-0.580) | 0.953 (0.952-0.953) |
|
|
External data set | 0.721 (0.720-0.721) | 0.910 (0.909-0.912) | 0.270 (0.266-0.273) | 0.159 (0.159-0.160) | 0.952 (0.951-0.953) |
| XGBoostb | ||||||
|
|
Internal data set | 0.919 (0.919-0.919) | 0.904 (0.904-0.905) | 0.731 (0.729-0.732) | 0.565 (0.563-0.566) | 0.952 (0.952-0.952) |
|
|
External data set | 0.697 (0.695-0.699) | 0.908 (0.906-0.909) | 0.250 (0.245-0.255) | 0.156 (0.155-0.156) | 0.946 (0.945-0.947) |
| Deep neural network | ||||||
|
|
Internal data set | 0.881 (0.878-0.884) | 0.906 (0.905-0.907) | 0.622 (0.608-0.635) | 0.485 (0.477-0.492) | 0.944 (0.943-0.945) |
|
|
External data set | 0.655 (0.654-0.657) | 0.907 (0.905-0.908) | 0.197 (0.192-0.201) | 0.147 (0.146-0.147) | 0.932 (0.931-0.933) |
| Logistic regression | ||||||
|
|
Internal data set | 0.875 (0.875-0.875) | 0.901 (0.901-0.901) | 0.605 (0.605-0.605) | 0.469 (0.469-0.469) | 0.940 (0.940-0.940) |
|
|
External data set | 0.631 (0.631-0.631) | 0.904 (0.904-0.904) | 0.155 (0.155-0.155) | 0.140 (0.140-0.140) | 0.914 (0.914-0.914) |
aAUROC: area under the receiver operating characteristic curve.
bXGBoost: extreme gradient boosting.
Figure 2.
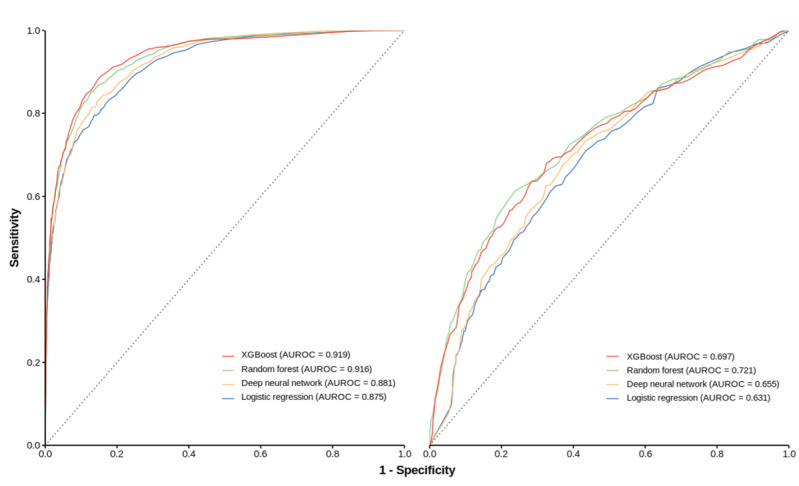
Receiver operating characteristic curves for all the prediction of intensive care unit delirium models. AUROC: area under the receiver operating characteristic curve; XGBoost: extreme gradient boosting.
For the external validation with MIMIC-III, we only selected variables that could be found both in SMC and MIMIC-III. As a result, only 59 variables were selected. The variables were categorized into general information, flowsheet, laboratory test results, and prescription of medication. The most important variable was the use of invasive mechanical ventilation in the general information. The importance of each final variable used in model development is shown in Figure 3.
Figure 3.
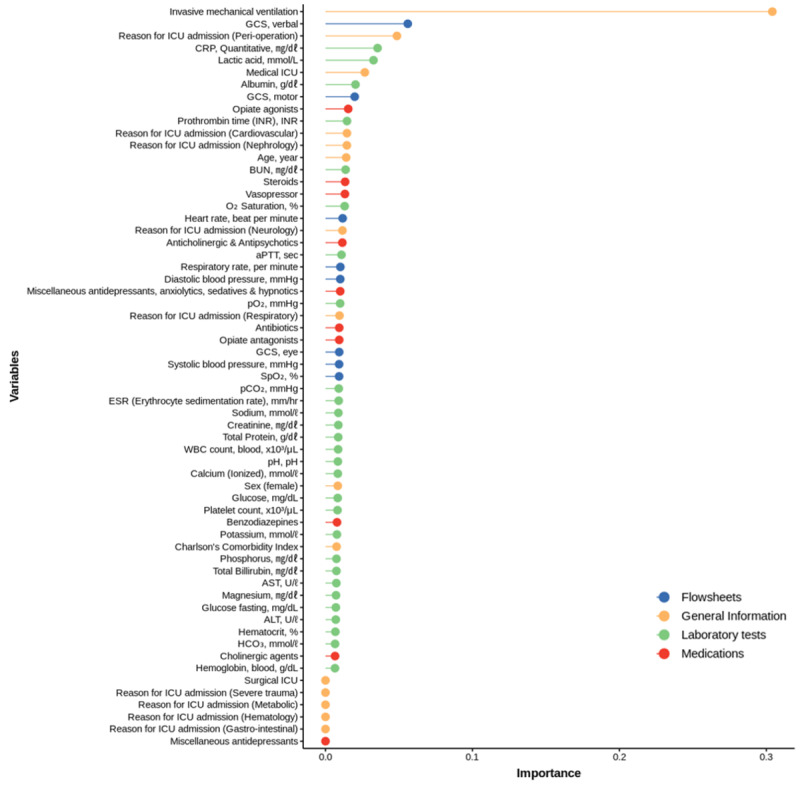
Variable importance of the prediction of intensive care unit delirium model. ALT: alanine aminotransferase; aPTT: activated partial thromboplastin time; AST: aspartate aminotransferase; BUN: blood urea nitrogen; CRP: C-reactive protein; GCS: Glasgow Coma Scale; ICU: intensive care unit; INR: international normalized ratio.
Model Assessment
For further model evaluation, calibration and decision curve analyses were performed. The Brier score for the XGBoost model with regard to predicting delirium was 0.094 for the internal validation data set, indicating that our model is reliable. The best model for external validation is RF, with the Brier score of 0.168. A Brier score of 0 indicates a perfect calibration, and the closest the value is to 0, the better model calibration. The calibration plot is shown in Multimedia Appendix 3. The decision curve analysis showed that the net benefit was useful for determining the threshold. For the PRIDE algorithm, the threshold for delirium prediction was selected as 0.13, and at this cut-off point, the net benefit was 0.234. The PRIDE model has a wide range of threshold probabilities and offers reasonable clinical applicability. The decision curve analysis is presented in Multimedia Appendix 4.
Discussion
Principal Results
We have demonstrated that the proposed delirium prediction model, which employs a machine learning algorithm with EHR data, can predict the development of delirium in medical and surgical ICU patients. In addition to our internal validation, we externally validated our findings using the MIMIC-III patient database. With the PRIDE model, we showed that delirium prediction models could be automated exclusively using risk factors derived from EHR data. The three main results of our study are as follows: (1) the model predicted delirium within the first 24 hours of ICU admission by only using data collected within the first 4 hours after ICU admission, (2) all variables were extracted from EMR data obtained from both medical and surgical intensive care patients, and (3) the model showed acceptable performance with regard to the external validation data set.
Among the various departments in a hospital, the incidence of delirium is the highest in the ICU, and it is well-documented that delirium occurs in 25% of critically ill adults in ICUs within the first 24 hours after admission [17-19]. This data shows that the early prediction of delirium upon initial ICU admission is crucial. Furthermore, the early prediction of the development of delirium can help clinicians make clinical decisions at an optimal time and provide preventive and personalized care with nondrug interventions for high-risk patients. Examples of such care are cognitive stimulation, orientation improvement, and early mobilization [20].
Comparison With Prior Work
Owing to the prevalence of delirium in patients admitted to ICUs, the routine use of preventive measures for delirium is recommended. However, previous studies have shown that clinicians’ predictions of the development of delirium are less accurate than those of ICU delirium prediction models [7]. Thus, delirium prediction models developed using machine learning can support clinicians in the early recognition of delirium, thereby immensely benefiting patients at high risk of delirium [21]. Furthermore, although several risk prediction models have been proposed, they are based on the manual evaluation of individual risk factors, and thus, may be challenging to implement [7,22,23]. Hence, in practice, automated models are preferable and more feasible. For these reasons, the implementation of automated tools for predicting the risk of delirium development using data extracted from EHR would improve clinical practices with regard to ICU management. Furthermore, the EHR-based prediction model uses a pipeline that automatically extracts variables and calculates models containing enough variables.
Previous studies have used several risk factors for delirium in ICUs, including age, severity score, cause of admission, usage of sedative agents, and laboratory results. In contrast with previous studies, the PRIDE model includes several additional variables such as vital signs (heart rate and blood pressure) and medication information that is excluded from EHRs. These differences allow our model to predict delirium incidents within 4 hours of ICU admission only using EHR data. Further, the PRIDE model did not include a severity score because this can only be obtained after 24 hours of ICU admission; in addition, since this information is separate from EMR data, using a severity score would require further efforts by the clinician. A few reports have also presented EMR-based machine learning models to predict delirium [24,25]. Whereas the prediction models presented in these reports are for all hospital-admitted patients, in this study, we developed a versatile model specifically for ICU patients at risk of delirium.
The strength of our study is the EMR-driven model that was both internally and externally validated, using SMC and MIMIC-III data, respectively. Although our result showed lower accuracy with external data than internal data, this result can be improved if the missing rate of key features decreases. In the case of CAM-ICU, 96% was missing in MIMIC-III. In addition, a decrease in accuracy with an external database was not uncommon in literature [26]. For example, a study predicting serious bacterial infections among fevers in children reported that the AUC of the external data was 0.26 lower than the internal data [27].
In clinical settings, missing values occur for various reasons. To handle missing data, we used mean values in the numerical data. We left the missing values in the categorical data blank such that the dummy variables were all equal to 0 method. Recently, deep learning–based advanced techniques, such as long short-term memory and recurrent neural network, were also introduced to impute missing data, and by employing these methods, they could improve model performances [28]. When choosing a missing handling method, knowing the missing pattern can improve model performance and work better when applied to clinical applications.
Limitations
There are potential limitations to our study that should be acknowledged. First, our study was retrospectively performed and validated. Prospective interventional studies are needed to verify the performance of the model and to reconfirm its clinical usefulness. Second, a selection bias might exist because we selected variables available in all cohorts, and this study was conducted in a retrospective manner. Furthermore, we excluded patients without CAM-ICU data (47% of the total number of ICU-admitted patients). In this regard, it should be noted that the purpose of this study was to develop a readily available model; therefore, we only selected the variables that could be used commonly in all cohorts. Finally, although the CAM-ICU tool is regarded as highly sensitive and specific to the detection of ICU delirium, it has critical limitations. As it only has binary labels, we cannot access the degree of delirium exacerbation. Furthermore, it is recorded in a “point-in-time” manner; thus, there may be some patients whose CAM-ICU tests were missed because they were completed outside the study’s time frame [29,30].
Conclusions
We have developed and validated the delirium prediction model, which can predict the occurrence of delirium within 24 hours of ICU admission, using clinical data obtained in the first 4 hours after ICU admission. The PRIDE algorithm has acceptable AUCROC and sensitivity; thus, it has the potential to help advise ICU physicians and prevent ICU delirium.
Acknowledgments
This research was supported by a Korea Health Technology R&D Project grant through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (grant HI19C0275). REK, WCC, and CRC contributed to the conception and study design. SH, JY, JH, WCC, and CRC performed the data analysis and interpretation. SH, REK, and CRC drafted the manuscript for intellectual content. SH, REK, WCC, JY, JH, and CRC revised the manuscript. All authors have read and approved the final manuscript.
Abbreviations
- AUROC
area under the receiver operating characteristic curve
- CAM-ICU
confusion assessment method for the intensive care unit
- DBP
diastolic blood pressure
- DNN
deep neural network
- EHR
electronic health record
- ICU
intensive care unit
- IRB
institutional review board
- LR
logistic regression
- MIMIC-III
Medical Information Mart for Intensive Care III
- NPV
negative predictive value
- PRIDE
Prediction of ICU Delirium
- PPV
positive predictive value
- RF
random forest
- SMC
Samsung Medical Center
- XGBoost
extreme gradient boosting
Appendix
Institutional review board approval form.
The missing rate in the variable list.
Calibration curve of the best model.
{kind=link}
Decision curve of the best model. PRIDE: prediction of intensive care unit delirium model.
{kind=link}
Footnotes
Authors' Contributions: SH and REK are co-first authors of this study. CRC (chiryang.chung@gmail.com) and WCC (docchaster@gmail.com) are co-corresponding authors for this article.
Conflicts of Interest: None declared.
References
- 1.Cavallazzi R, Saad M, Marik PE. Delirium in the ICU: An overview. Ann Intensive Care. 2012;2(1):49. doi: 10.1186/2110-5820-2-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Salluh JIF, Wang H, Schneider EB, Nagaraja N, Yenokyan G, Damluji A, Serafim RB, Stevens RD. Outcome of delirium in critically ill patients: systematic review and meta-analysis. BMJ. 2015 Jun 03;350(may19 3):h2538–h2538. doi: 10.1136/bmj.h2538. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=26041151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pandharipande PP, Girard TD, Jackson JC, Morandi A, Thompson JL, Pun BT, Brummel NE, Hughes CG, Vasilevskis EE, Shintani AK, Moons KG, Geevarghese SK, Canonico A, Hopkins RO, Bernard GR, Dittus RS, Ely EW, BRAIN-ICU Study Investigators Long-term cognitive impairment after critical illness. N Engl J Med. 2013 Oct 03;369(14):1306–16. doi: 10.1056/NEJMoa1301372. http://europepmc.org/abstract/MED/24088092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Milbrandt EB, Deppen S, Harrison PL, Shintani AK, Speroff T, Stiles RA, Truman B, Bernard GR, Dittus RS, Ely EW. Costs associated with delirium in mechanically ventilated patients. Crit Care Med. 2004 Apr;32(4):955–62. doi: 10.1097/01.ccm.0000119429.16055.92. [DOI] [PubMed] [Google Scholar]
- 5.Serafim RB, Bozza FA, Soares M, do Brasil PEA, Tura BR, Ely EW, Salluh JI. Pharmacologic prevention and treatment of delirium in intensive care patients: A systematic review. J Crit Care. 2015 Aug;30(4):799–807. doi: 10.1016/j.jcrc.2015.04.005. [DOI] [PubMed] [Google Scholar]
- 6.Brummel NE, Girard TD. Preventing delirium in the intensive care unit. Crit Care Clin. 2013 Jan;29(1):51–65. doi: 10.1016/j.ccc.2012.10.007. http://europepmc.org/abstract/MED/23182527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.van den Boogaard M, Pickkers P, Slooter AJC, Kuiper MA, Spronk PE, van der Voort P H J, van der Hoeven J G, Donders R, van Achterberg T, Schoonhoven L. Development and validation of PRE-DELIRIC (PREdiction of DELIRium in ICu patients) delirium prediction model for intensive care patients: observational multicentre study. BMJ. 2012 Feb 09;344(feb09 3):e420–e420. doi: 10.1136/bmj.e420. http://europepmc.org/abstract/MED/22323509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chen Y, Du H, Wei B, Chang X, Dong C. Development and validation of risk-stratification delirium prediction model for critically ill patients: A prospective, observational, single-center study. Medicine (Baltimore) 2017 Jul;96(29):e7543. doi: 10.1097/MD.0000000000007543. doi: 10.1097/MD.0000000000007543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wassenaar A, van den Boogaard M, van Achterberg T, Slooter AJC, Kuiper MA, Hoogendoorn ME, Simons KS, Maseda E, Pinto N, Jones C, Luetz A, Schandl A, Verbrugghe W, Aitken LM, van Haren FMP, Donders ART, Schoonhoven L, Pickkers P. Multinational development and validation of an early prediction model for delirium in ICU patients. Intensive Care Med. 2015 Jun 18;41(6):1048–56. doi: 10.1007/s00134-015-3777-2. http://europepmc.org/abstract/MED/25894620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wassenaar A, Schoonhoven L, Devlin JW, van Haren FMP, Slooter AJC, Jorens PG, van der Jagt M, Simons KS, Egerod I, Burry LD, Beishuizen A, Matos J, Donders ART, Pickkers P, van den Boogaard M. Delirium prediction in the intensive care unit: comparison of two delirium prediction models. Crit Care. 2018 May 05;22(1):114. doi: 10.1186/s13054-018-2037-6. https://ccforum.biomedcentral.com/articles/10.1186/s13054-018-2037-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Johnson AEW, Pollard TJ, Shen L, Lehman LH, Feng M, Ghassemi M, Moody B, Szolovits P, Celi LA, Mark RG. MIMIC-III, a freely accessible critical care database. Sci Data. 2016 May 24;3:160035. doi: 10.1038/sdata.2016.35. doi: 10.1038/sdata.2016.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ely EW, Margolin R, Francis J, May L, Truman B, Dittus R, Speroff T, Gautam S, Bernard GR, Inouye SK. Evaluation of delirium in critically ill patients: Validation of the confusion assessment method for the intensive care unit (CAM-ICU) Critical Care Medicine. 2001;29(7):1370–1379. doi: 10.1097/00003246-200107000-00012. [DOI] [PubMed] [Google Scholar]
- 13.Olson R, Moore J. TPOT: A tree-based pipeline optimization tool for automating machine learning. In: Automated Machine Learningpringer; 2019. May 18, p. A. [Google Scholar]
- 14.R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. [2020-04-03]. https://www.R-project.org/
- 15.van Rossum G, Drake F. Python reference manual. Netherlands: Centrum voor Wiskunde en Informatica Amsterdam; 1995. Apr 30, [Google Scholar]
- 16.juhha1 / Delirium Prediction. Github. [2021-07-19]. https://github.com/juhha1/Delirium_Prediction.
- 17.Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. The Lancet. 2014 Mar;383(9920):911–922. doi: 10.1016/s0140-6736(13)60688-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ely EW, Shintani Ayumi, Truman Brenda, Speroff Theodore, Gordon Sharon M, Harrell Frank E, Inouye Sharon K, Bernard Gordon R, Dittus Robert S. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004 Apr 14;291(14):1753–62. doi: 10.1001/jama.291.14.1753. [DOI] [PubMed] [Google Scholar]
- 19.Serafim RB, Dutra MF, Saddy F, Tura B, de Castro JEC, Villarinho LC, da Gloria Santos M, Bozza FA, Rocco JR. Delirium in postoperative nonventilated intensive care patients: Risk factors and outcomes. Ann Intensive Care. 2012 Dec 31;2(1):51. doi: 10.1186/2110-5820-2-51. http://europepmc.org/abstract/MED/23272945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawlik AJ, Esbrook CL, Spears L, Miller M, Franczyk M, Deprizio D, Schmidt GA, Bowman A, Barr R, McCallister KE, Hall JB, Kress JP. Early physical and occupational therapy in mechanically ventilated, critically ill patients: A randomised controlled trial. The Lancet. 2009 May;373(9678):1874–1882. doi: 10.1016/s0140-6736(09)60658-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Siddiqi N. Predicting delirium: Time to use delirium risk scores in routine practice? Age Ageing. 2016 Jan 13;45(1):9–10. doi: 10.1093/ageing/afv183. [DOI] [PubMed] [Google Scholar]
- 22.Inouye SK, Viscoli CM, Horwitz RI, Hurst LD, Tinetti ME. A predictive model for delirium in hospitalized elderly medical patients based on admission characteristics. Ann Intern Med. 1993 Sep 15;119(6):474–81. doi: 10.7326/0003-4819-119-6-199309150-00005. [DOI] [PubMed] [Google Scholar]
- 23.Kishi T, Hirota T, Matsunaga S, Iwata N. Antipsychotic medications for the treatment of delirium: A systematic review and meta-analysis of randomised controlled trials. J Neurol Neurosurg Psychiatry. 2016 Jul 04;87(7):767–74. doi: 10.1136/jnnp-2015-311049. [DOI] [PubMed] [Google Scholar]
- 24.Wong A, Young AT, Liang AS, Gonzales R, Douglas VC, Hadley D. Development and validation of an electronic health record–based machine learning model to estimate delirium risk in newly hospitalized patients without known cognitive impairment. JAMA Netw Open. 2018 Aug 03;1(4):e181018. doi: 10.1001/jamanetworkopen.2018.1018. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2018.1018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Corradi JP, Thompson S, Mather JF, Waszynski CM, Dicks RS. Prediction of incident delirium using a random forest classifier. J Med Syst. 2018 Nov 14;42(12):261. doi: 10.1007/s10916-018-1109-0. [DOI] [PubMed] [Google Scholar]
- 26.Shung D, Simonov M, Gentry M, Au B, Laine L. Machine learning to predict outcomes in patients with acute gastrointestinal bleeding: A systematic review. Dig Dis Sci. 2019 Aug 4;64(8):2078–2087. doi: 10.1007/s10620-019-05645-z. [DOI] [PubMed] [Google Scholar]
- 27.Bleeker S, Moll H, Steyerberg E, Donders A, Derksen-Lubsen G, Grobbee D, Moons K. External validation is necessary in prediction research. Journal of Clinical Epidemiology. 2003 Sep;56(9):826–832. doi: 10.1016/s0895-4356(03)00207-5. [DOI] [PubMed] [Google Scholar]
- 28.Han-Gyu K, Gil-Jin J, Ho-Jin C, Minho K, Young-Won K, Jaehun C. Recurrent neural networks with missing information imputation for medical examination data prediction. 2017 IEEE International Conference on Big Data and Smart Computing (BigComp); February 13-16, 2017; Jeju, South Korea. 2017. Feb 13, https://ieeexplore.ieee.org/abstract/document/7881685. [DOI] [Google Scholar]
- 29.van Eijk MM, van den Boogaard M, van Marum RJ, Benner P, Eikelenboom P, Honing ML, van der Hoven B, Horn J, Izaks GJ, Kalf A, Karakus A, Klijn IA, Kuiper MA, de Leeuw F, de Man T, van der Mast RC, Osse R, de Rooij SE, Spronk PE, van der Voort PH, van Gool WA, Slooter AJ. Routine use of the confusion assessment method for the intensive care unit. Am J Respir Crit Care Med. 2011 Aug;184(3):340–344. doi: 10.1164/rccm.201101-0065oc. [DOI] [PubMed] [Google Scholar]
- 30.Neto AS, Nassar AP, Cardoso SO, Manetta JA, Pereira VG, Espósito DC, Damasceno MC, Slooter AJ. Delirium screening in critically ill patients. Critical Care Medicine. 2012;40(6):1946–1951. doi: 10.1097/ccm.0b013e31824e16c9. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Institutional review board approval form.
The missing rate in the variable list.
Calibration curve of the best model.
Decision curve of the best model. PRIDE: prediction of intensive care unit delirium model.