

Abstract
Background and study aims Esophageal defects (leaks, fistulas, and perforations) are associated with significant morbidity and mortality. Endoluminal vacuum-assisted closure (EVAC) is a novel intervention that entails the use of sponges in the defect along with negative pressure to achieve granulation tissue formation and healing and has been gaining popularity. We performed a systematic review and pooled analysis of available literature to assess the safety and effectiveness of EVAC for esophageal defects.
Patients and methods We queried PubMed/Medline, Embase, Cochrane, and Web of Science through September 25, 2020 to include all pertinent articles highlighting the safety and effectiveness profile of EVAC for esophageal defects. Pooled rates, 95 % confidence intervals (CIs), and heterogeneity ( I 2 ) were assessed for each outcome.
Results A total of 18 studies with 423 patients were included (mean age 64.3 years and males 74.4 %). The technical success for EVAC was 97.1 % (CI: 95.4 %–98.7 %, I 2 = 0 %). The clinical success was 89.4 % (CI: 85.6 %–93.1 %, I 2 = 36.8 %). The overall all-cause mortality and adverse events (AEs) noted were 7.1 % (CI: 4.7 %–9.5 %, I 2 = 0 %) and 13.6 % (CI: 8.0 %–19.1 %, I 2 = 68.9 %), respectively. The pooled need for adjuvant therapy was 15.7 % (CI: 9.8 %–21.6 %, I 2 = 71.1 %).
Conclusions This systematic review and meta-analysis showed high rates of technical success, clinical success, and low all-cause mortality and AEs using EVAC. Although the technique is a promising alternative, the lack of comparative studies poses a challenge in making definite conclusions regarding use of EVAC compared to other endoscopic modalities, such as clips and stents.
Introduction
Esophageal defects (leaks, fistula, and perforation) are complications associated with esophageal procedures such as endoscopy, dilation, transesophageal echocardiography, variceal therapy, nasogastric tube placement, surgeries such as esophagectomy, trauma, malignancy, and ingestion 1 2 3 . Esophageal defects can also be spontaneous without the presence of external factors, as mentioned above 2 . Esophageal perforations, although rare, have a mortality rate ranging from 10 % to 40 % 4 . Esophageal leaks are also associated with increased mortality in patients (odds ratio [OR]: 3.00, 95 % confidence interval (CI) 1.2–7.2) compared to having no leaks 3 .
There are multiple ways to address these aforementioned defects. Historically, the only available modalities were a conservative approach or surgery 5 . For many patients, the traditional modalities lacked safety and effectiveness. With the development of biomaterials in the last two decades, endoscopic placement of self-expanding metal stent (SEMS) became the treatment of choice for less severe esophageal intrathoracic leaks 6 . SEMS was suitable for both nonsurgical and surgical candidates and showed superior effectiveness and a better safety profile than surgery or a conservative approach, when indicated 7 . Bleeding, stent migration, and perforation are adverse events (AEs) associated with SEMS that can be fatal; therefore, there has been a search for better modalities 8 . A promising emerging alternative is endoluminal vacuum-assisted closure (EVAC). EVAC consists of placement of a sponge in the defect cavity or the esophageal lumen via the endoscope and connection of it to a negative pressure continuous vacuum 9 . EVAC treats the defect via mechanisms of leak source control, granulation tissue formation, encouraging reperfusion, and debridement of necrotic tissue once sponges are removed or replaced 9 10 . Modified from skin wound vacuum therapy, EVAC was introduced a decade ago for lower rectal anastomosis leaks and recently has gained popularity as an alternative treatment for defects in the upper gastrointestinal tract 11 .
Literature is lacking regarding the overall effectiveness of outcomes related to the use of EVAC therapy for esophageal defects. We conducted a systematic review and pooled analysis of the available literature to assess the safety and effectiveness of EVAC for esophageal defects.
Methods
We performed this systematic review and meta-analysis using the framework laid out in “Preferred reporting items for systematic reviews and meta-analyses (PRISMA)” and “Meta-analyses Of Observational Studies in Epidemiology (MOOSE)” checklist 12 13 .
Literature search/strategy
The literature search was conducted in consultation with an experienced librarian (W.L.S). We queried the following databases from inception through September 25th, 2020: PubMed/Medline, Embase, Cochrane Register of Controlled Trials, and Web of Science Core Collection. Controlled subject terms and keyword synonyms for the concepts of “esophageal”, “leak”, “Fistula”, “perforation”, and “endoscopic vacuum therapy” were formulated for search on PubMed/Medline and translated to syntax / vocabulary of other databases. The search strategy created by the librarian (W.L.S) was cross checked by another reviewer (M.A.). Screening of studies was initially conducted based on titles and abstracts. Full text of relevant articles was further screened for interventions and outcomes of interests. Two independent reviewers (M.A. and H.H.) independently performed screening. Discrepancies were resolved through mutual discussion. A bibliography of the finalized articles was further hand screened to broaden the literature search and relevant articles were included. Details of the search strategy using EMBASE are highlighted in Supplementary Table 1 .
Study definitions
Leaks are defined as a disruption of anastomosis resulting in fluid collection. Perforation refers to a full-thickness defect of the gastrointestinal tract. Fistula is an abnormal connection between two epithelialized surfaces. Although different, studies in the literature have used these terms interchangeably 14 . For simplicity, we will refer to these as “defects.” The term nonsurgical iatrogenic refers to perforation caused by a diagnostic and/or therapeutic modality other than surgery on the esophagus. Technical success refers to the successful use of EVAC without technical failure. Clinical success refers to the successful use of EVAC therapy to achieve a clinical endpoint, that is, closure of the defect. Overall mortality is defined as mortality from any cause and not limited to intervention. AEs are defined as complications from the use of EVAC, such as stenosis, bleeding, dislocation of sponge, and visceral injury during the procedure.
Inclusion and exclusion criteria
Studies were included based on the following:
inclusion of patients with esophageal defects;
EVAC as an intervention;
control not applicable; and
outcomes of technical success, clinical success, all-cause mortality, treatment duration, hospital length of stay, and overall AEs.
We only included randomized controlled trials (RCTs), cohort studies (retrospective/prospective), and case control studies. Single-arm studies as well as an EVAC arm in comparative studies were included for this systematic review. We excluded other study designs, such as editorials, case reports, and case series with < 10 patients, review articles, and meta-analyses. We excluded abstracts as they provide limited information in terms of overall study quality. We did not restrict our search to language. If more than one study was available from a particular center, we used the information from the most recent and updated one.
Data collection
Data collection was performed by two independent reviewers (M.A. and H.H.). Any conflicts were resolved through mutual discussion. We extracted the following pertinent data: demographics (age, gender), cause of esophageal leak (nonsurgical iatrogenic, postsurgical, or spontaneous), use of adjuvant modalities/therapy (surgery, clips, stents, etc.) and outcomes (as above). The data were extracted directly in Microsoft Excel (Microsoft, Redmond, Washington, United States).
Data synthesis and analysis
The analysis was conducted using Open Meta Analyst (CEBM, University of Oxford, Oxford, United Kingdom) and Comprehensive Meta-Analysis (Biostat, Englewood, USA). Weighted random effects models were used to calculate proportional estimates of outcomes using DerSimonian-Laird method. Pooled outcomes with 95 % CIs were calculated and presented. A correction factor of 0.5 was applied if the event rate for a study outcome was 0. For each outcome, 95 % prediction interval (PI) was also generated 15 . Given the presumed heterogeneity of study population, random effects model was chosen over fixed effect model. The fixed effect model was used as a sensitivity tool. I2 statistics was used to calculate heterogeneity between studies with values of 0 %, 25 %, 50 %, and 75 % interpreted as absent, low, moderate, and high heterogeneity, respectively 16 .
Subgroup analysis
Subgroup analysis was performed for studies with sample size ≥ 20 patients and for studies published from 2015 on.
Bias assessment
Study quality was assessed using the Newcastle Ottawa score for cohort studies 17 . Publication bias was assessed using funnel plots (for qualitative assessment) and Begg’s rank correlation test (for quantitative assessment using P value).
Results
A total of 18 studies were included in the final analysis after applying the strict inclusion and exclusion criteria (supplementary material). Details of the study selection process are shown in Fig. 1 . A total number of 423 patients were included in these studies (mean age 64.3 years, CI 62.7–65.9 years, and males 74.4 %, CI 64.6 %–84.3 %). The studies were published between 2010 and 2020. Baseline demographics and study characteristics are highlighted in Table 1 . The type of vacuum and sponge type are delineated in Supplementary Table 2 . The causes of esophageal defects were as follows: surgery 74.0 %, nonsurgical iatrogenic 17.5 %, and spontaneous 8.5 %.
Fig. 1 .

PRISMA flow diagram.
Table 1. Baseline study characteristics and demographics of included patients.
| Study | Year | Study type | Total patients | Mean age, years (SD) | Male, n (%) | Etiology of “defect”, n | ||
| Surgery | Nonsurgical iatrogenic | Spontaneous | ||||||
| Berlth et al. | 2018 | Retrospective | 35 | 64.3 (11.8) | 29 (85.3 %) | 35 | 0 | 0 |
| Bludau et al. | 2018 | Retrospective | 77 | 63.2 (14.1) | 51 (66.2 %) | 59 | 12 | 6 |
| Brangewitz et al. | 2013 | Retrospective | 32 | 63.8 (11.3) | 28 (87.5 %) | 30 | 1 | 1 |
| Heits et al. | 2014 | NR | 10 | 66 (10.6) | 5 (50.0 %) | 0 | 4 | 6 |
| Jeon et al. | 2019 | Retrospective | 22 | 67.3 (7.2) | 17 (77.3 %) | 22 | 0 | 0 |
| Jung et al. | 2020 | Retrospective | 30 | 65.4 | 20 (66.7 %) | 23 | 5 | 2 |
| Kuehn et al. | 2015 | Retrospective | 21 | 68.3 (8.9) | 15 (71.4 %) | 11 | 8 | 2 |
| Laukoetter et al. | 2016 | Prospective | 52 | 66.3 (15.3) | 37 (71.2 %) | 39 | 9 | 4 |
| Loske (1) et al. | 2011 | Case Series | 14 | NR | NR | 10 | 3 | 1 |
| Loske (2) et al. | 2015 | Case Series | 10 | NR | 7 (70.0 %) | 0 | 10 | 0 |
| Mencio et al. | 2018 | Retrospective | 15 | 59.8 | 8 (53.3 %) | 2 | 8 | 5 |
| Mennigen et al. | 2015 | Retrospective | 15 | 57.5 (9.8) | 14 (93.3 %) | 15 | 0 | 0 |
| Min et al. | 2019 | Retrospective | 20 | 65.7 (6.9) | 20 (100.0 %) | 20 | 0 | 0 |
| Moschler et al. | 2015 | NR | 10 | 73.9 (11.7) | 5 (50 %) | 5 | 4 | 1 |
| Noh et al. | 2018 | Retrospective | 12 | 57.1 (3.3) | 12 (100.0 %) | 12 | 0 | 0 |
| Ooi et al. | 2018 | Retrospective | 10 | 56.7 (12.3) | NR | 6 | 3 | 1 |
| Pournaras et al. | 2018 | NR | 21 | NR | NR | 7 | 7 | 7 |
| Schneiwind et al. | 2013 | Retrospective | 17 | NR | NR | 17 | 0 | 0 |
EVAC, endoluminal vacuum-assisted closure; n, number of patients; NR, not reported; SD, standard deviation.
Outcomes
The outcomes for individual studies are listed in Table 2 . A total of 17 studies assessed technical and clinical success. The technical success rate was found to be 97.1 % (CI 95.4 %–98.7 %, PI: 95.2 %–98.9 %, I 2 = 0 %) ( Fig. 2a ). The clinical success rate was noted to be 89.4 % (CI 85.6 %–93.1 %, PI: 80.5 %–99.3 %, I 2 = 36.8 %) ( Fig. 2b , Supplementary Table 3 ).
Table 2. Outcomes of individual studies.
| Study | Total patients | Technical success, n (%) | Clinical success, n (%) | Treatment duration, mean (SD) | Hospital LOS, mean (SD) | Overall mortality, n (%) | Need for adjuvant therapy, n (%) | Adverse events, n | |||||
| Total | Esophageal defect related 1 | Other causes 2 | Stenosis | Bleeding | Dislocation | Visceral injury | |||||||
| Berlth et al. | 35 | 29 (82.9 %) | 30 (85.7 %) | 18.3 (12.4) | 54 (28.9) | 3 (8.6 %) | 3 (8.6 %) | 0 (0 %) | 7 (20.6 %) | 1 | 0 | 4 | 0 |
| Bludau et al. | 77 | 72 (93.5 %) | 60 (77.9 %) | 22 (18.5) | NR | 10 (13.0 %) | 10 (13.0 %) | 0 (0 %) | 21 (27.3 %) | 0 | 4 | 0 | 0 |
| Brangewitz et al. | 32 | 32 (100.0 %) | 27 (84.4 %) | 35.3 (22.3) | 60 (29.2) | 5 (15.6 %) | NR | NR | 2 (6.3 %) | 3 | 1 | 5 | 1 |
| Heits et al. | 10 | 9 (90.0 %) | 9 (90.0 %) | 19 (14.3) | 48 (15) | 1 (10.0 %) | 0 (0 %) | 1 (10.0 %) | 2 (20.0 %) | NR | NR | NR | NR |
| Jeon et al. | 22 | 21 (95.5 %) | 19 (90.5 %) | 19.7 (12.4) | 30 (13.9) | 0 (0 %) | 0 (0 %) | 0 (0 %) | 1 (4.5 %) | 0 | 0 | 0 | 0 |
| Jung et al. | 30 | 29 (96.7 %) | 25 (83.3 %) | NR | NR | 2 (6.7 %) | 1 (3.3 %) | 1 (3.3 %) | 6 (20.0 %) | 0 | 2 | 1 | 0 |
| Kuehn et al. | 21 | 19 (90.5 %) | 19 (90.5 %) | 19.7 (12.4) | NR | 1 (4.8 %) | 1 (4.8 %) | 0 (0 %) | 12 (57.1 %) | 1 | 0 | 0 | 0 |
| Laukoetter et al. | 52 | 52 (100.0 %) | 49 (94.2 %) | 37.7 (29.2) | 75.5 (47.4) | 5 (9.6 %) | 3 (5.77 %) | 2 (3.85 %) | 6 (11.5 %) | 4 | 5 | 11 | 0 |
| Loske (1) et al. | 14 | 14 (100.0 %) | 13 (92.9 %) | 12.7 (8) | NR | 1 (7.1 %) | 0 (0 %) | 1 (7.1 %) | 1 (7.1 %) | 1 | 0 | 0 | 0 |
| Loske (2) et al. | 10 | 10 (100.0 %) | 10 (100.0 %) | 5.2 (1.5) | NR | 0 (0 %) | 0 (0 %) | 0 (0 %) | 0 (0 %) | 0 | 0 | 0 | 0 |
| Mencio et al. | 15 | 15 (100.0 %) | 15 (100.0 %) | NR | NR | 0 (0 %) | 0 (0 %) | 0 (0 %) | 0 (0 %) | 0 | 0 | 0 | 0 |
| Mennigen et al. | 15 | 15 (100.0 %) | 14 (93.3 %) | 32.7 (20.8) | 61.3 (23.9) | 1 (6.7 %) | 1 (6.7 %) | 0 (0 %) | 4 (26.7 %) | 0 | 0 | 0 | 0 |
| Min et al. | 20 | 20 (100.0 %) | 19 (95.0 %) | 22.3 (15) | 51.7 (20.5) | 1 (5.0 %) | 0 (0 %) | 1 (5.0 %) | 1 (5.0 %) | 7 | 0 | 0 | 0 |
| Moschler et al. | 10 | 9 (90.0 %) | 7 (70.0 %) | 9.1 (8.8) | NR | 3 (30.0 %) | 3 (30.0 %) | 0 (0 %) | 3 (30.0 %) | 1 | 0 | 0 | 0 |
| Noh et al. | 12 | 12 (100.0 %) | 8 (66.7 %) | 11.4 (5) | NR | 1 (8.3 %) | 1 (8.3 %) | 0 (0 %) | 2 (6.7 %) | 1 | 1 | 0 | 0 |
| Ooi et al. | 10 | 9 (90.0 %) | 6 (60.0 %) | 25.5 (8.6) | 70.8 (17.2) | 3 (30.0 %) | 3 (30.0 %) | 0 (0 %) | 6 (60.0 %) | 0 | 0 | 0 | 2 |
| Pournaras et al. | 21 | 20 (95.2 %) | 20 (95.2 %) | NR | 61.3 (37.3) | 1 (4.8 %) | 0 (0 %) | 1 (4.8 %) | 2 (9.5 %) | 0 | 2 | 0 | 0 |
| Schneiwind et al. | 17 | NR | NR | NR | 57 (30) | 2 (11.8 %) | NR | NR | NR | NR | NR | NR | NR |
LOS, length of stay; n, number of patients; NR, not reported; SD, standard deviation.
Esophageal defect related causes included infection, sepsis, multiorgan failure.
Other causes include cancer metastasis, withdrawing care, heart failure, colitis, and pulmonary emboli.
Fig. 2.
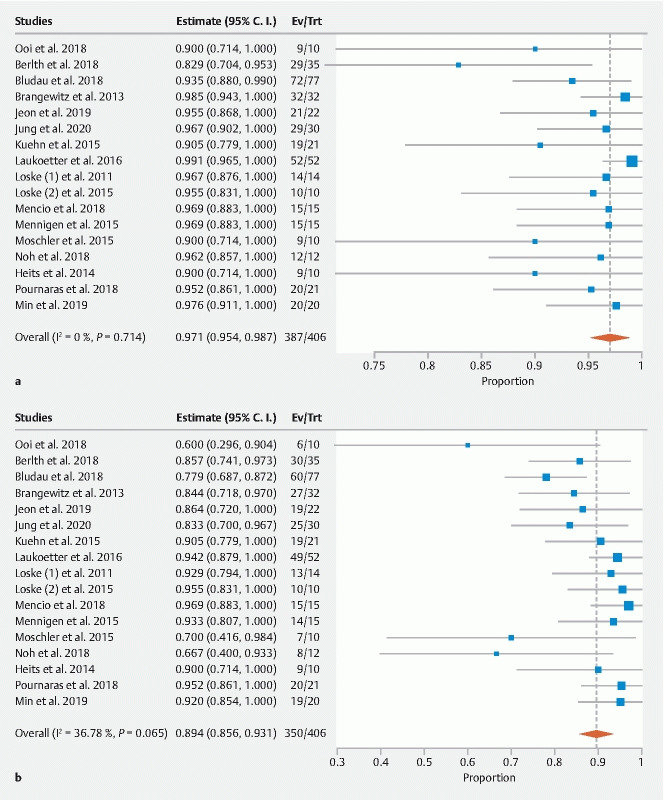
Forest plot. a Technical success. b Clinical success of EVAC. CI, confidence interval.
A total of 14 studies assessed the treatment duration, which was found to be 20.3 days (CI 14.9–25.7, PI: 0.0–42.5, I 2 = 96.1 %) ( Fig. 3a ). The length of hospital stay was 56.5 days (10 studies, CI: 46.6–66.4, PI: 20.1–92.9, I 2 = 89.5 %) ( Fig. 3b ).
Fig. 3.

Forest plot. a Treatment duration. b Length of hospital stay. CI, confidence interval.
A total 18 studies assessed the overall mortality for patients undergoing EVAC therapy. The rate of mortality was 7.1 % (CI 4.7 %–9.5 %, PI: 5.8 %–10.5 %, I 2 = 0 %) ( Fig. 4a ). The overall AE rate for use of EVAC was 13.6 % (CI 8.0 %–19.1 %, PI: 8.9 %–20.7 %, I 2 = 73.6 %) ( Fig. 4b ). The nature or type of AEs are highlighted in detail in Table 2 for individual studies. The need for adjuvant or second therapy was 15.7 % (9.8 %–21.6 %, PI: 10.4 %–23.7 %, I 2 = 71.3 %) ( Fig. 4c ).
Fig. 4.

Forest plot. a Overall mortality.
Fig. 4.

Forest plot. b Any adverse events.
Fig. 4.

Forest plot. c Need for adjuvant therapy. CI, confidence interval.
Subgroup analysis
Studies with ≥ 20 patients
The overall technical success rate was 96.6 % (CI: 94.3 %–98.9 %, PI: 94.0 %–99.3 %, I 2 = 24.4 %). The clinical success rate was 88.9 % (CI: 84.4 %–93.3 %, PI: 81.1 %–97.5 %, I 2 = 38.5 %). The overall rates of mortality and AEs were 7.0 % (CI: 4.2 %–9.8 %, PI: 4.8 %–10.3 %, I 2 = 0 %) and 15.0 % (CI: 7.5 %–22.6 %, PI: 8.9 %–25.3 %, I 2 = 78.3 %). The need for adjuvant therapy was 15.8 % (CI: 8.1 %–23.5 %, PI: 9.4 %–26.6 %, I 2 = 77.7 %). The treatment duration was 24.3 days (7 studies, CI: 19.6–29.0 days, PI: 8.5–40.1 days, I 2 = 80.6 %). The length of hospital stay was 54.8 days (6 studies, CI: 40.7–69.0, PI: 7.8–101.8, I 2 = 92.2 %).
Studies published from 2015 on
The overall technical success rate was 96.9 % (CI: 95.1 %–98.7 %, PI: 94.9 %–98.9 %, I 2 = 39.82 %). The clinical success rate was 89.2 % (CI: 84.9 %–93.6 %, PI: 79.8 %–99.7 %, I 2 = 46.5 %). The overall rates of mortality and AEs were 6.6 % (CI: 4.1 %–9.2 %, PI: 4.6 %–9.6 %, I 2 = 0 %) and 10.5 % (CI: 5.6 %–15.4 %, PI: 6.7 %–16.5 %, I 2 = 62.7 %). The need for adjuvant therapy was 17.5 % (CI: 10.4 %–24.6 %, PI: 11.2 %–27.4 %, I 2 = 77.7 %). The treatment duration was 19.9 days (11 studies, CI: 13.8–25.9 days, PI: 0.0–42.2, I 2 = 96.4 %). The length of hospital stay was 57.4 days (8 studies, CI: 43.5–71.2, PI: 8.2–106.6, I 2 = 92.6 %).
Bias assessment
The risk of bias for each study using the Newcastle Ottawa Scale is highlighted in Supplementary Table 4 . All studies had a score of 6 or more. The inspection of funnel plot revealed visible asymmetry for the studies included on the basis of clinical success with EVAC; however, the overall effect size did not change after adjustments were made using the “trim-and-fill” method ( Supplementary Fig. 1 ). Begg’s rank correlation pointed towards a potential publication bias ( P = 0.06); however, this was not statistically significant.
Discussion
This systematic review and meta-analysis evaluated the effectiveness of EVAC in the management of esophageal defects. Our results demonstrated high rates of technical and clinical success for EVAC. In addition, rates of mortality and overall AEs associated with the use of EVAC therapy were low. Our results support the potential use of EVAC for management of esophageal defects – leaks, fistula, and perforations of the esophagus.
As newer modalities are being assessed for safety and effectiveness, guidelines to treat esophageal transmural defects are evolving 18 . The basic principle is to seal the defect and drain the fluid collection to reduce chance of abscess formation and sepsis. The current approach includes conservative management, surgery, and endoscopy. The conservative approach consists of antibiotic therapy, parenteral nutrition, and insertion of nasogastric tube placement under direct vision 18 . A conservative approach is used for small leaks with early diagnosis and no sepsis. Surgery is indicated in patients with large leaks, significant necrosis, leaks unresponsive to other modalities, and those who have sepsis 19 20 . Surgical approaches include direct suturing, enforced suturing, pleural patches, or flaps which are reserved for more severe cases. Endoscopic approaches using clips, stents, suturing, or sealants are an alternative option for cases between the two extremes of the severity spectrum 21 . The clips can be either through-the-scope clips (TTSC) or over-the-scope clips (OTSC). For clip-based closure, the tissue surrounding the clip must be healthy, allowing adherence of clip. Friable, necrotic, or weak tissue will result in technical and clinical failure. The use of TTSC is limited to sealing very small defects, owing to their size. In a recent pooled analysis, OTSC was noted to achieve a clinical success rate of 78.4 % 22 . Esophageal stents, particularly self-expandable stents, are more popular for endoscopic management of leaks, fistula, and perforation. A recent systematic review demonstrated the overall clinical success of self-expandable stents to be 76.8 % 23 . In addition, stents are associated with AEs including fistulas, bleeding, migration, perforation, necrosis, and stricture 24 . Although a direct comparison was not feasible, we demonstrated a clinical success rate of 89.3 % for EVAC in successful closure of esophageal defects, which is notably higher than for either OTSC or stents.
In recent meta-analyses, EVAC was compared to SEMS and a lower overall AE rate (risk difference: 0.24, 95 % CI 0.13–0.35) and mortality (OR: 0.39, 95 % CI 0.18–0.83) was noted for EVAC 25 26 . The reason for fewer AEs with EVAC may stem from the difference in technique. Because the sponges need replacement every 3 to 4 days, wound healing can be observed every time sponges are exchanged 24 . We speculate that because there are short intervals of wound assessment, the presence of AEs can be detected before progression. This is not feasible with the covered SEMS. Moreover, in case of fluid collection in SEMS, drainage has to be performed externally 27 . Fluid accumulations are drained through a negative pressure apparatus with EVAC, while there is no negative pressure drainage with SEMS. This may contribute to the better safety profile for the EVAC compared with SEMS. Considering the fact that EVAC is relatively novel and there is variability in technique regarding amount of negative pressure and interval of sponge change, the rates of AEs, treatment duration, and length of hospital stay are variable, which may explain the heterogeneity noted in our analysis. As techniques are refined, future AE rates should be even lower than current reports.
Our study had some limitations. The included studies had inherent bias, given their observational nature. Moreover, the patient population was heterogenous. The reasons for that are manifold. First, esophageal transmural defects are secondary to a wide spectrum of etiologies. Furthermore, factors such as site and size of defect, presence of comorbidities, and treatment delay due to difficulty in diagnosis increase the heterogeneity of the patient population. In addition, because the EVAC technique is operator dependent and there have been no clear treatment algorithms such as for the extent of negative pressure and interval of sponge change, this would also increase the heterogeneity of cases. EVAC therapy is performed in advanced centers by highly skilled endoscopists, which may affect the reported effectiveness rate. Finally, our study suggests a potential publication bias, with negative studies possibly not being reported. Thus, our results should be interpreted with caution as there may be overestimation in terms of clinical effectiveness and success. Despite the limitations, there are several strengths. Our study is the first to pool the outcomes related to EVAC therapy from a diverse population. We used a stringent search strategy and performed an exhaustive search to include pertinent studies. Our major outcomes – technical success, clinical success, and overall mortality – did not have significant heterogeneity.
Conclusions
In conclusion, our meta-analysis demonstrated effective outcomes with the use of EVAC for esophageal defects and it should be considered clinically for such patients. Further studies are needed that directly compare EVAC to other modalities, such as OTSC, surgery, and stenting.
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Supplementary material :
References
- 1.Vidarsdottir H, Blondal S, Alfredsson H et al. Oesophageal perforations in Iceland: a whole population study on incidence, aetiology and surgical outcome. Thorac Cardiovasc Surg. 2010;58:476–480. doi: 10.1055/s-0030-1250347. [DOI] [PubMed] [Google Scholar]
- 2.Chirica M, Champault A, Dray X et al. Esophageal perforations. J Visc Surg. 2010;147:e117–e128. doi: 10.1016/j.jviscsurg.2010.08.003. [DOI] [PubMed] [Google Scholar]
- 3.Rutegård M, Lagergren P, Rouvelas I et al. Intrathoracic anastomotic leakage and mortality after esophageal cancer resection: a population-based study. Ann Surg Oncol. 2012;19:99–103. doi: 10.1245/s10434-011-1926-6. [DOI] [PubMed] [Google Scholar]
- 4.Huu Vinh V, Viet Dang Quang N et al. Surgical management of esophageal perforation: role of primary closure. Asian Cardiovasc Thorac Ann. 2019;27:192–198. doi: 10.1177/0218492319827439. [DOI] [PubMed] [Google Scholar]
- 5.Whyte R I, Iannettoni M D, Orringer M B. Intrathoracic esophageal perforation: The merit of primary repair. J Thoracic Cardio Surg. 1995;109:140–146. doi: 10.1016/S0022-5223(95)70429-9. [DOI] [PubMed] [Google Scholar]
- 6.Ong G KB, Freeman R K. Endoscopic management of esophageal leaks. J Thorac Dis. 2017;9:S135–S145. doi: 10.21037/jtd.2017.03.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Persson S, Rouvelas I, Irino T et al. Outcomes following the main treatment options in patients with a leaking esophagus: a systematic literature review. Dis Esophagus. 2017;30:1–10. doi: 10.1093/dote/dox108. [DOI] [PubMed] [Google Scholar]
- 8.Hindy P, Hong J, Lam-Tsai Y et al. A comprehensive review of esophageal stents. Gastroenterol Hepatol (NY) 2012;8:526–534. [PMC free article] [PubMed] [Google Scholar]
- 9.Leeds S G, Mencio M, Ontiveros E et al. Endoluminal vacuum therapy: How I do it. J Gastrointest Surg. 2019;23:1037–1043. doi: 10.1007/s11605-018-04082-z. [DOI] [PubMed] [Google Scholar]
- 10.Szymanski K, Ontiveros E, Burdick J S et al. Endolumenal vacuum therapy and fistulojejunostomy in the management of sleeve gastrectomy staple line leaks. Case Rep Surg. 2018;2018:2.494069E6. doi: 10.1155/2018/2494069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kuehn F, Schiffmann L, Janisch F et al. Surgical endoscopic vacuum therapy for defects of the upper gastrointestinal tract. J Gastrointest Surg. 2016;20:237–243. doi: 10.1007/s11605-015-3044-4. [DOI] [PubMed] [Google Scholar]
- 12.Moher D, Liberati A, Tetzlaff J et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi: 10.1136/bmj.b2535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Stroup D F, Berlin J A, Morton S C et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–2012. doi: 10.1001/jama.283.15.2008. [DOI] [PubMed] [Google Scholar]
- 14.Goenka M K, Goenka U. Endotherapy of leaks and fistula. World J Gastrointest Endosc. 2015;7:702–713. doi: 10.4253/wjge.v7.i7.702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Riley R D, Higgins J P, Deeks J J. Interpretation of random effects meta-analyses. BMJ. 2011;342:d549. doi: 10.1136/bmj.d549. [DOI] [PubMed] [Google Scholar]
- 16.Higgins J, Thompson S G, Deeks J J et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Deeks J, Dinnes J, DʼAmico R.Evaluating non-randomised intervention studies Health Technol Assess 20037(iii–x)1–173. [DOI] [PubMed] [Google Scholar]
- 18.Schaheen L, Blackmon S H, Nason K S. Optimal approach to the management of intrathoracic esophageal leak following esophagectomy: a systematic review. Am J Surg. 2014;208:536–543. doi: 10.1016/j.amjsurg.2014.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Crestanello J A, Deschamps C, Cassivi S D et al. Selective management of intrathoracic anastomotic leak after esophagectomy. J Thorac Cardiovasc Surg. 2005;129:254–260. doi: 10.1016/j.jtcvs.2004.10.024. [DOI] [PubMed] [Google Scholar]
- 20.Lampridis S, Mitsos S, Hayward M et al. The insidious presentation and challenging management of esophageal perforation following diagnostic and therapeutic interventions. J Thorac Dis. 2020;12:2724–2734. doi: 10.21037/jtd-19-4096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Willingham F F, Buscaglia J M. Endoscopic management of gastrointestinal leaks and fistulae. Clin Gastroenterol Hepatol. 2015;13:1714–1721. doi: 10.1016/j.cgh.2015.02.010. [DOI] [PubMed] [Google Scholar]
- 22.Bartell N, Bittner K, Kaul V et al. Clinical efficacy of the over-the-scope clip device: A systematic review. World J Gastroenterol. 2020;26:3495–3516. doi: 10.3748/wjg.v26.i24.3495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.van Halsema E E, van Hooft J E. Clinical outcomes of self-expandable stent placement for benign esophageal diseases: A pooled analysis of the literature. World J Gastrointest Endosc. 2015;7:135–153. doi: 10.4253/wjge.v7.i2.135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Plum P S, Herbold T, Berlth F et al. Outcome of self-expanding metal stents in the treatment of anastomotic leaks after Ivor Lewis esophagectomy. World J Surg. 2019;43:862–869. doi: 10.1007/s00268-018-4832-2. [DOI] [PubMed] [Google Scholar]
- 25.Scognamiglio P, Reeh M, Karstens K et al. Endoscopic vacuum therapy versus stenting for postoperative esophago-enteric anastomotic leakage: systematic review and meta-analysis. Endoscopy. 2020;52:632–642. doi: 10.1055/a-1149-1741. [DOI] [PubMed] [Google Scholar]
- 26.Do Monte Junior E S, de Moura D TH, Ribeiro I B et al. Endoscopic vacuum therapy versus endoscopic stenting for upper gastrointestinal transmural defects: Systematic review and meta‐analysis. Digest Endosc. 2020 doi: 10.1111/den.13813. [DOI] [PubMed] [Google Scholar]
- 27.Schubert D, Scheidbach H, Kuhn R et al. Endoscopic treatment of thoracic esophageal anastomotic leaks by using silicone-covered, self-expanding polyester stents. Gastrointest Endosc. 2005;61:891–896. doi: 10.1016/s0016-5107(05)00325-1. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.