

Abstract
Virtual learning environments (VLEs) such as games can greatly enhance medical education curriculum. In this monograph, we argue for the importance of identifying existing VLEs and analyzing their characteristics in order for medical educators to establish alignment with their curricular goals. We introduce the co-opted technological pedagogical content knowledge framework as an analytical lens for examining the context-attuned design features of games [1]. We apply the lens to study three games designed to advance medical education; namely, CD4 Hunter, Septris, and Microbe Invader. We conclude with implications for enhancing medical education curricula through the incorporation of digital games.
Keywords: Game-based learning, Virtual learning environments, Digital games, Pedagogy
Introduction
Health professionals face an ever-increasing volume of information to be mastered during and after training. Medical schools must focus not only on cultivating this knowledge but also supporting the development of communication and clinical skills (e.g., patient-centered interview and physical examination). In response, many medical schools have shifted from a teacher-centered, lecture-dominated curriculum to a learner-centered, small-group or problem-based pedagogy emphasizing self-directed learning [2]. However, the challenges of assuring an optimal breadth of clinical case exposure, promoting development of skills, and adequately assessing knowledge remain under-addressed. The use of digital games and simulations in medical education has surfaced as potential tools to help address some of the aforementioned challenges. Simulations, from models and task trainers to, more recently, computer-driven simulators and even virtual reality, have long been used in medical education in both training and assessment [3]. Game-based learning (GBL), on the other hand, is a more recent addition to the array of teaching tools used in medical education [4].
Digital games are conducive environments for learning because they can be designed to help learners acquire new knowledge and deepen existing knowledge targeted to specific academic domains. In addition, digital games can afford a balanced focus on learning with an emphasis on conceptual representation, simulation, or contextualization [5]. Furthermore, the elements of challenges, choices, and consequences in a game allow for practice, exploration, and knowledge construction within a given academic domain, i.e., games afford situated learning [6]. Central to the context of this monograph is the increasing interest in the use of games in medical education [7, 8]. The field is currently nascent in that limited literature is available to demonstrate the examination of games as a part of the medical school curriculum [4, 9].
In this monograph, we further establish the current trends and gaps in adopting virtual learning environments (VLEs) such as games to enhance medical education curricula. We address a specific need; that is, to empower medical educators to be proficient in identifying existing VLEs and analyzing their characteristics in order to establish alignment with their curricular goals. In doing so, we introduce the co-opted technological pedagogical content knowledge framework as an analytical lens for examining the context-attuned design features of games [1]. We use the analytical lens to describe three medical education games; namely, CD4 Hunter, Septris, and Microbe Invader. In this way, we hope to provide a framework for medical educators considering the use of these games and other games as tools for enhancing medical education curricula.
Games as Tools for Enhancing Medical Education
Games and other VLEs are conducive to situated cognition because they can be designed to include relevant content that can be emphasized through practice [6]. Games are used extensively in training in nonmedical industries such as finance, hospitality, and the military. However, much of the ongoing justification for the use of games in medical education focuses on the importance of giving learners room for practice and error within a controlled environment [10]. Despite a reported desire by medical educators to promote student-centered learning, many studies of games in medical education focus primarily on promoting knowledge acquisition. In an analysis by Gorbanev et al., of 21 studies of serious games or gamified apps, most (76%) focused on knowledge and skill acquisition, while the remainder focused on learner attitudes toward the intervention [11]. Indeed, one study of a pediatric radiology quiz game vs. an interactive lecture reported higher test scores and learner ratings compared to the didactic lecture group. However, the game consisted of a list of questions embedded in a tic-tac-toe format followed by informational slides, a format that reaches more toward traditional didactics than active learning [12].
Furthermore, in their systematic review, Gorbanev et al. found that most published studies of medical digital learning games were quizzes and simulations, emphasizing memory and skill development through repetition. Effectiveness in these studies was often tested via a multiple-choice question posttest [6, 11, 13]. Students’ performance was compared to scores pregame [14, 15] or scores of control groups given traditional lectures [6, 15]. For a broader view, others looked at overall end-of-rotation, midterm, and final exam performances [12, 16]. Some studies also used Likert-scale ratings of student preferences [12, 13]. Other testing methods included motivation questionnaires and self-efficacy assessments [6]. However, these assessments may not adequately address differences between lectures and VLEs in helping students master learning objectives.
Games and game-like experiences can enhance medical education by complementing information presented in lectures, for example, by simulating the complexities of medical decision-making. Because serious games, including VLEs, encompass a heterogeneous array of tools, the question of their underlying pedagogical strategies and how they may fit into a larger course curriculum remains open for educators. As such, in this paper, a description of the game can provide educators with a starting point to gain familiarity with the technological, pedagogical, and content characteristics. Whether this game is suitable for use in a specific context will depend on the educator playing the game and identifying the alignment of the game to his/her learning goals [1, 17].
The heterogeneity of serious games leaves open the question of their underlying pedagogical strategies and how they may fit into a larger course curriculum. In addition, the effectiveness of these games in helping students master learning objectives is not always apparent. Furthermore, the use of new technologies, including games, does not in itself effect a shift from teacher-centered to student-centered learning. Not surprisingly, despite the opportunities afforded by games to bolster and extend medical education curricula, there is a paucity of evidence on the effectiveness and utility of these tools (Figs. 1, 2, and 3).
Fig. 1.

In CD4 Hunter, visual cues allow players to connect the game objective (tagging the colored receptor) to the learning objective (HIV virions must bind to specific receptors in order to infect a cell). Image included with permission from the game creator, Dr. Urdaneta-Hartman
Fig. 2.

a In Septris, players must balance a careful assessment of complex patients from the standpoint of an ICU team member against the game element of time. b. Feedback on clinical decisions reinforces the learning objectives on sepsis management. Image included with permission from the game creator, Dr. Lisa Shieh
Fig. 3.
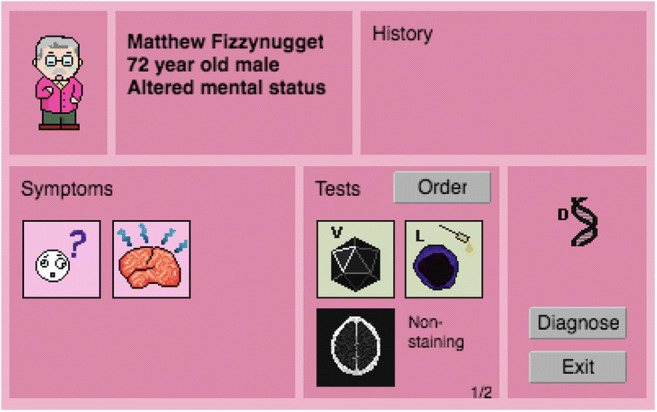
In Microbe Invader, players choose from a panel of cases and review basic clinical information (history, exam, studies) in order to identify a microbial pathogen. Images included with permission from the game creator, Dr. Li Tao
Part of the difficulty of reviewing serious games in medical education is due to the heterogeneity of the games themselves (in terms of structure, interface, implementation, and pedagogical underpinning) and part due to the lack of data collected on learner experiences and outcomes. In addition, few studies examine the limitations of digital games, including obsolescence due to rapidly evolving technology and limitations of costs and training [4]. Furthermore, published studies often report on testing of games in only one learning environment or institution; the restricted dissemination and narrow focus of many serious games limit related research and impede the generalizability of available studies.
We argue that the choice to use a game to promote learning is in part a design-based decision: the extent to which the designed features of a game afford medical educators an opportunity to enhance content and pedagogy make the game a desirable tool to incorporate into curricula. As such, the chosen game should support the desired learning outcomes. Thus, a systematic framework that educators can use to analyze game features in order to enhance medical education curricula is essential.
Framing and Outlining the Process and Purpose of Analyzing Games for Medical Education
The technological pedagogical content knowledge (TPACK) framework was developed by Mishra and Koehler as a way to conceptualize the dynamic and interconnected knowledge educators need to enhance their instruction with technology [18]. Foster co-opted the TPACK framework to serve as an analytical lens for game analysis and selection by helping educators approach a game as a curriculum with context-attuned affordances for technology, pedagogy, and content [1]. This analytical lens is a subset of Game Network Analysis (GaNA), a network of analytical and pedagogical frameworks that was developed for educators (medical educators, in this monograph) as a methodological process for designing and facilitating GBL experiences in a given context [1, 20].
To provide a historical context to the development of TPACK, Shulman argued for educators to cultivate pedagogical content knowledge in order to effectively teach a specific content area [19]. Mishra and Koehler further expanded this concept to include knowledge of technology for teachers when teaching with digital tools which was captured in the technological pedagogical content knowledge (TPACK) framework [18]. Mishra and Koehler represent TPACK as a Venn diagram of the three circular domains and resulting intersections. TPACK’s individual domains are relatively easy to comprehend: content knowledge, or the body of information required to teach the subject matter, pedagogical knowledge, or the theoretical basis for education including how learners learn and how best to assess their level, and technological knowledge, a facility with evolving technology and ability to use it in the classroom.
The technological pedagogical knowledge (TPK) domain refers to the understanding of the interplay between technological tools and specific pedagogical aims, such as what technologies are best suited to assessing students or facilitating discussion. Technological content knowledge (TCK) shifts this view to understanding how technology and content impact each other: how does the use of one form of technology (e.g., presentation software) vs. another (online videos) impact the content we are trying to teach, and how does the subject influence the choice of technology? Pedagogical content knowledge (PCK) is the interplay of how specific pedagogical approaches can impact what is to be learned. For instance, if the goal is to prepare students for a high-stakes standardized test with many brief multiple questions, a pedagogical approach that is akin to drill and practice may be more appropriate than a narrative approach.
The final “level” in TPACK is the overlap between all three domains (TPK, TCK, and PCK): technological pedagogical content knowledge. TPACK refers not only to the three interdependent areas of knowledge but also to the flexibility and expertise that teachers rely on in using all three to create an effective learning environment. For example, a specific technology can support instructional strategies to help learners struggling with one concept in pathophysiology, while other contexts of learner needs and subjects may require a different technological underpinning. TPACK allows us to understand that these areas of knowledge, especially that of technology, should not be learned and practiced separately but instead integrated and used to improve students’ learning experiences.
The purpose of analyzing a game is to gain deep familiarity with the affordances and constraints of the learning environment to inform educators’ decisions to implement the game in a chosen educational context. The first step in this pursuit involves helping educators to become aware that games, like any technology, are biased and context-dependent artifacts [18]. As such, educators need to approach games as designed experiences [21], whose cognitive, pedagogical, and experiential features can be leveraged in partnership with educators’ expertise [22].
The process of game analysis encompasses practicing direct and vicarious methods that can yield relevant knowledge about the game. These methods include playing the game, researching about it (e.g., looking for information about the game on the publisher’s website), and sometimes observing another individual play the game (e.g. watching a YouTube video) [1, 17]. Doing so yields insights about the game in relation to technical requirements (e.g., platform for running the game and ease of installation), pedagogy in general (e.g., objective of the game, intended target group, customization options, icons, and multimodal literacy needed), embedded content, and pedagogy specific to the content. This game knowledge is vital for educators to decide whether the game could be valuable when integrated within a curriculum [23].
In presenting our use of TPACK for game analysis, we first co-opt the framework as an analytical lens based on the work of Foster [1]. We use the categories of technology, pedagogy, and content separately for the sake of clarity to demonstrate how the design of the game can be decomposed. However, because TPACK and other frameworks used in game analysis are integrated, we discourage the conclusion that these game characteristics can solely be considered separately. Instead, we use TPACK as a lens through which we can examine, for example, how game technology (such as mode of gameplay) goes hand in hand with the game’s pedagogy (i.e., its genre) or how this pedagogy influences the content knowledge that can be imparted in the game [1]. Medical teachers should consider games and specifically VLEs as pedagogical tools that need to be thoughtfully examined in order to best understand their power; the co-opted TPACK framework allows for a systematic analysis of games.
Below we present a description of three games designed for medical education. For each game, we describe the pedagogical and content characteristics of games (as a form of technology for medical education). These characteristics are summarized in Table 1, showing how a deeper examination of medical education games allows educators to better utilize these resources within the curriculum.
Table 1.
Comparison of technological, pedagogical, and content characteristics among three medical education games allows educators to examine the best use of these games with respect to the level of learner and types of educational outcomes that can be supported
| Game | Technology | Pedagogy | Content |
|---|---|---|---|
| CD4 Hunter | Application for mobile device, action/shooter; rounds are played against a countdown timer for virion “lives” | Visual cues of color and pattern reinforce core concepts of receptor recognition and depict viral replication | HIV infection and replication: players identify binding sites on CD4+ T cells for HIV virions and learn about how the virus adapts to avoid immune system defense mechanisms |
| Septris | Browser-based, simulation; time elements and management of multiple cases increase sense of urgency within the game; cartoon-like graphics | Simulation emphasizes concept application to clinical cases on systemic inflammatory response syndrome (SIRS) | Sepsis management: players distinguish between causes of sepsis and apply best practice guidelines in treatment of sepsis and underlying diagnosis |
| Microbe Invader | Browser-based, role-playing game with features of resource management (obtaining antibiotic armamentarium for gameplay); cartoon-like graphics | Successive questions cue fact recall within a given brief clinical scenario | Microbiology facts: players must identify a variety of pathogens via clinical scenarios and answer factual questions on lab tests and antibiotic treatment |
CD4 Hunter
One recently developed online medical game is CD4 Hunter, created by a team of physicians and scientist in microbiology and immunology at Drexel University in conjunction with a team of game designers [24]. On the surface, it is advertised as a simulation video game: “play as an HIV virion,” reads the description of the game on the App store [20], and one of its creators, Dr. Carla Brown, states that players are “in the bloodstream…looking for the perfect target cell” [25]. On further examination using the TPACK framework, we can evaluate CD4 Hunter’s technology as not only a game but also an action/shooter game, in which the player/learner’s goal is to successfully infect cells and replicate the virus (i.e., generate more virions). These game principles determine the learning principles that are best emphasized and exemplified in CD4 Hunter.
Whereas shooter games usually involve a gun as the weapon of choice, in this case, the player, as an HIV virion, acts as the weapon. As in other action/shooter games, the skills in CD4 Hunter emphasized are speed and reaction time. Players must navigate through the bloodstream, using color clues to identify appropriate targets, and direct the virion to contact the target cell receptor in order to infect it before the cell moves away or is blocked by obstacles (other nontarget blood cells]. In addition, players battle a relatively quick countdown timer. Each cycle of successful viral infection and replication results in an increase in points (displayed on the screen as a “+10”) and an extra virion-life displayed on the top left of the screen. As a result, the game’s technological aspects support the feel of a “typical” action video game; even the name calls back to shooter games.
The learning principles embedded within CD4 Hunter are simple, though the subject matter is complex. Essentially, the player must recognize matching color combinations, representing the viral capsid proteins and target cell receptors that allow successful infection (the main content within the game). Gameplay involves memorizing these facts and associating them quickly with actions within the game (that is, TPK) but in this iteration does not build further concepts upon this foundation or give opportunities for exploration of these concepts outside of the game. The layers of the game not only add interest but also reveal its TCK underpinning. For example, play involves navigation through the bloodstream to find the appropriate cell receptors. In addition, the rapid timer on each virus “life” is another action-game feature that underscores a learning objective: each HIV virion has a limited lifespan, even in the bloodstream. In a second level, players must “shake off” target cells’ defense mechanisms, i.e., antibodies. Future proposals to further develop the complexity of the game include allowing players to mutate the HIV virus as well as introducing anti-HIV drugs [26].
The HIV-related content knowledge has a complex underpinning, but using PCK, we see that CD4 Hunter ties the learning content (how the HIV virus infects cells) to the visual clue of color. Recognition of the appropriately color-coded target cell allows players to advance and reinforces the learning objective that HIV must similarly recognize a cell-surface receptor in order to infect the cell. Thus, using the broader TPACK framework, we see that this action/shooter game uses visual cues to help players understand the concepts of receptor recognition and limited viral lifespan without yet extending to the complexities of viral replication. The TPACK framework helps us see that CD4 Hunter is better used for students beginning to learn about the concept of viral infection and HIV rather than students who need to understand more detail about viruses or HIV in general.
Septris
Stanford University’s School of Medicine has designed a set of online games specifically for medical education, including Septris, a simulation of interventions for early sepsis [27], and SICKO, a simulation of surgical management for different conditions. In Septris, players simultaneously manage two patients with systemic inflammatory response syndrome (SIRS) and are charged with curing them; players must identify the cause of the illness (sepsis and its source) as well as the appropriate management.
Septris’ game technology uses a simple graphic representation of patients’ health status, akin to a Galilean thermometer, with two patients in players’ care at one time. Players make choices in diagnosis and treatment; appropriate maneuvers increase point totals. The game also adds a level of difficulty in the form of time; patients’ “health” levels drop over time and lead to death if they are not managed correctly. Players are able to request information and apply treatments quickly, but some information is delivered slowly, and response to treatment is at times delayed. The strategy elements of the game in monitoring and managing septic patients and the controlled stress increase engagement with the game. As such, while Septris relies on simple graphics (a floating cartoon head represents the patient’s health), examination using the lens of TPK shows that it engages players more deeply than the interface might imply. Its pedagogy is more accurately a simulation, with Septris invoking the feeling of simultaneously managing septic patients in the intensive care unit in a safe, controlled environment without the potential dire consequences of failure.
Septris’ game interface not only works as a role-play but also in supporting the game’s learning objectives. Recognizing common features of septic/SIRS patients and related management principles (such as low blood pressure and the need for additional intravenous fluid), as well as distinguishing features in these conditions, is incorporated into gameplay. The game’s construction has players make their choices and receive immediate feedback on whether they are correct as well as answer knowledge-based questions which restate and reinforce facts about SIRS. Using the TCK frame, players cannot arrive at the correct strategy using game cues but must be able to recall and apply the pertinent knowledge. Septris’ approach is thus particularly well-suited to principles of SIRS management.
Using the PCK lens, we see that Septris both assumes baseline knowledge and reinforces application of complex content [27]. The game requires players to stabilize patients by treating the acute manifestations of SIRS (low blood pressure and organ damage) using best practice guidelines. In order to fully “cure” the patients, players must also identify and treat the causes of sepsis using clues from the provided history, physical exam, and available tests.
Thus, Septris makes full use of its pedagogy of simulation: the practice of decision-making and management bolsters the content. In addition, the interspersed knowledge questions make the content explicit [28], an important pedagogical choice which allows it to be used as review by students. From the TPACK standpoint, while Septris is not aimed at fully preparing students or physicians to manage septic patients independently, its use of simulation and its game features work well as a companion to reading about related guidelines and evidence in a journal or textbook.
Microbe Invader
Microbe Invader is an online game designed to teach details of microbiology [29]. It is primarily a role-playing game similar to Pokémon but its interface also shares elements with side-scrolling platform games such as Super Mario Brothers. In Microbe Invader, the player takes on the role of a medical student on an infectious disease rotation, collect resources, and navigate through the two-dimensional hospital world in order to find, evaluate, and treat a slate of patients. Correct answers and judicious resource use add to players’ point totals. The game technology, with its retro pixel graphic design, seems simple, but the game’s bank of cases is extensive, covering details of a wide range of microbes and pathogens. As such, an examination of Microbe Invader’s TPK shows that it is well-suited to updating information in order to support detail learning and recall.
Microbe Invader’s game-relevant knowledge is, of course, microbiology. Facts about pathogens, appropriate diagnostic tests, and treatment mechanisms are tested in succession. The breadth of information covered is substantial, covering many pathogens. Players also have the option of saving their progress in order to encounter new cases or to restart and reshuffle patients in order to review old ones; using the TCK frame, this game helps players recall factual knowledge most likely learned elsewhere. On the other hand, the given clinical contexts (history and physical exam details) are relatively brief, and the resolution of cases after, for example, antibiotic choice is accelerated. Thus, examination of PCK shows that players are asked to apply the recalled facts by associating pathogens and clinical scenarios with the appropriate diagnostic tests and treatments, but the reasoning occurs within single cases without being asked to provide justification or integrating possibilities into a differential diagnosis. Microbe Invader is a role-playing game rather than a simulation, reinforcing factual knowledge rather than in-depth application.
Microbe Invader is designed for students learning microbiology in a clinical context. The game’s technology allows it to cover the fundamentals of an extensive list of bacteria, viruses, and fungi, clinical presentations of infections, and antibiotic treatments (including mechanisms of action). Because of its breadth, these topics are not covered at great depth, and thus from the TPACK frame, Microbe Invader succeeds as a game for students first exposed to microbiology to review and reinforce these details.
What’s Next?
In this monograph, we argued for the adoption of virtual learning environments (VLEs) such as games to enhance medical education curricula. Specifically, we argued for the importance of identifying VLEs and analyzing their characteristics in order for medical educators to establish alignment with their curricular goals. We introduced the co-opted TPACK framework an analytical lens for examining the context-attuned design features of games and applied the lens to study three medical education games: CD4 Hunter, Septris, and Microbe Invader [1].
A key to a meaningful incorporation of games in medical education curricula is, as alluded to above, a careful consideration of game design as well as the place of the game within the curriculum. As is evident from the analysis of the three games, the environments can be designed to emphasize different concepts; different game genres support different types of player styles and impact the knowledge being facilitated [30]. Thus, in addition to their appeal as novel technological tools with engaging and entertaining as well as educational elements, games should be designed and chosen as components of the broader mosaic of the curricula [31].
This is, however, only the starting point in the effective use of games for achieving desired learning outcomes. Game-based learning (GBL) in medical education, as in other education settings, benefits from teacher intervention, including the opportunities educators design using students’ game play experiences, and provides support to further student learning through strategies such as problem-based activities, scaffolding, and debriefing at critical moments [20]. The expertise of medical teachers with respect to their designed learning environments as well as their familiarity with specific games, gleaned via gameplay, is essential to the success of game-based learning. Beginning with a careful consideration of game design, we can make well-informed decisions regarding the use of existing games as well as evaluate their educational value to our students more meaningfully and further enhance our curricula.
Acknowledgments
Dr. Jayatilleke’s and Dr. Shah’s work was conducted with the support of their prior institutions: Drexel University College of Medicine and Drexel University School of Education, respectively.
Compliance with Ethical Standards
Conflict of Interest
Dr. Shah reports no relevant conflicts of interest.
Funding Information
Dr. Jayatilleke’s research on technology and rheumatology education is supported by a grant from the Rheumatology Research Foundation.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
Not applicable; this article does not contain human subject research.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Arundathi Jayatilleke, Email: Arundathi.Jayatilleke@tuhs.temple.edu.
Mamta Shah, Email: m.shah@elsevier.com.
References
- 1.Foster AN. Assessing learning games for school content: framework and methodology. In: Ifenthaler D, Eseryel D, Ge X, editors. Assessment in Game-based Learning: Foundations, Innovations, and Perspectives. New York: Springer; 2012. [Google Scholar]
- 2.Ribeiro C, Monteiro M, Fernandes J, Corredoura S, Candeias F, Pereira J. Games in higher education: opportunities, expectations, challenges and results in medical education. In: de Freitas S, Ott M, Popescu MM, Stanescu I, editors. New pedagogical approaches in game enhanced learning – curriculum integration. Hershey: IGI Global; 2013. pp. 228–247. [Google Scholar]
- 3.Issenberg S, Gordon MS, Safford DL, Hart RE, Hart IR. Simulation and new learning technologies. Med Teach. 2001;23(1):16–23. doi: 10.1080/01421590020007324. [DOI] [PubMed] [Google Scholar]
- 4.Bigdeli S, Kaufman D. Digital games in health professions education: advantages, disadvantages, and game engagement factors. Med J Islam Repub Iran. 2017;31:117. doi: 10.14196/mjiri.31.117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ke F. Designing and integrating purposeful learning in game play: a systematic review. Educ Technol Res Dev. 2016;64(2):219–244. doi: 10.1007/s11423-015-9418-1. [DOI] [Google Scholar]
- 6.Dankbaar MEW, Richters O, Kalman CJ, Prins G, ten Cate OTJ, van Merrienboer JJG, Schuit SCE. Comparative effectiveness of a serious game and an e-module to support patient safety knowledge and awareness. BMC Med Educ. 2017;17:30. doi: 10.1186/s12909-016-0836-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Akl EA, Gunukula S, Mustafa R, Wilson MC, Symons A, Moheet A, Schünemann HJ. Support for and aspects of use of educational games in family medicine and internal medicine residency programs in the US: a survey. BMC Med Educ. 2010;10:26–30. doi: 10.1186/1472-6920-10-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Blakely G, Skirton H, Cooper S, Allum P, Nelmes P. Educational gaming in the health sciences: systematic review. J Adv Nurs. 2009;65(2):259–269. doi: 10.1111/j.1365-2648.2008.04843.x. [DOI] [PubMed] [Google Scholar]
- 9.Gee JP. What video games have to teach us about learning and literacy. 2. New York: Palgrave Macmillan; 2007. [Google Scholar]
- 10.Tolk A, Miller GT, Cross AE, Maestri J, Cawrse B. AIMS: Applying Game Technology to Advance Medical Education. Comput Sci Eng. 2013;15:82–91. doi: 10.1109/MCSE.2013.115. [DOI] [Google Scholar]
- 11.Gorbanev I, Agudelo-Londoño S, González RA, Cortes A, Pomares A, Delgadillo V, Yepes FJ, Muñoz Ó. A systematic review of serious games in medical education: Quality of evidence and pedagogical strategy. Med Educ Online. 2018;23:1–9. doi: 10.1080/10872981.2018.1438718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Courtier J, Webb EM, Phelps AS, Naeger DM. Assessing the learning potential of an interactive digital game versus an interactive-style didactic lecture: the continued importance of didactic teaching in medical student education. Pediatr Radiol. 2016;46:1787–1796. doi: 10.1007/s00247-016-3692-x. [DOI] [PubMed] [Google Scholar]
- 13.Boeker M, Andel P, Vach W, Frankenschmidt A. Game-based e-learning is more effective than a conventional instructional method: a randomized controlled trial with third-year medical students. PLoS ONE. 2013;8(12):e82328. doi: 10.1371/journal.pone.0082328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sward KA, Richardson S, Kendrick J, Maloney CM. Use of a web-based game to teach pediatric content to medical students. Ambul Pediatr. 2008;8(6):354–359. doi: 10.1016/j.ambp.2008.07.007. [DOI] [PubMed] [Google Scholar]
- 15.Rondon S, Sassi FC. Furquim de Andrade CR. Computer game-based and traditional learning method: a comparison regarding students’ knowledge retention. BMC Med Educ. 2013;13:1–8. doi: 10.1186/1472-6920-13-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kanthan R, Senger JL. The impact of specially designed digital games-based learning in undergraduate pathology and medical education. Arch Pathol Lab Med. 2011;135:135–142. doi: 10.5858/2009-0698-OAR1.1. [DOI] [PubMed] [Google Scholar]
- 17.Aarseth E. Playing research: Methodological approaches to game analysis. In: Miles A, editor. MelbourneDAC 2003 streamingworlds. Melbourne: RMIT Publishing; 2003. [Google Scholar]
- 18.Mishra P, Koehler M. Technological pedagogical content knowledge: a new framework for teacher knowledge. Teach Coll Rec. 2006;108(6):1017–1054. doi: 10.1111/j.1467-9620.2006.00684.x. [DOI] [Google Scholar]
- 19.Shulman LS. Those who understand: knowledge growth in teaching. Educ Res. 1986;15:4–14. doi: 10.3102/0013189X015002004. [DOI] [Google Scholar]
- 20.Shah M, Foster A. Developing and assessing teachers’ knowledge of game-based learning. J Technol Teach Educ. 2015;23(2):241–267. [Google Scholar]
- 21.Squire K, Barab S. Games, learning, and society: learning and meaning in the digital age. Cambridge: Cambridge University Press; 2012. pp. 279–305. [Google Scholar]
- 22.Moline T. Descriptors of quality teachers and quality digital games. In: Ferdig R, editor. Handbook of Research on Effective Electronic Gaming in Education. Hershey: IGI Global; 2009. pp. 652–669. [Google Scholar]
- 23.Zhao Y, Pugh K, Sheldon S, Byers JL. Conditions for classroom technology innovations. Teach Coll Rec. 2002.
- 24.Ingeno L. Biomedical researchers design mobile game for teaching about HIV. In: Drexel News Blog. 2017. https://newsblog.drexel.edu/2017/08/11/biomedical-researchers-design-mobile-game-for-studying-hiv/. Accessed 03 August 2018.
- 25.CD4 Hunter. In: App Store. 2018. https://itunes.apple.com/us/app/cd4-hunter/id1186846022?mt=8. Accessed 31 July 2018.
- 26.WHYY. Scientists and game designers show you what it’s like to be HIV. WHYY. 2017. https://whyy.org/articles/scientists-and-game-designers-show-you-what-its-like-to-be-hiv/. Accessed 31 July 2018.
- 27.Septris. In: Stanford Hospital and Clinics Department of Quality. 2011. http://med.stanford.edu/septris/. Accessed 02 August 2018.
- 28.Becker K. How are games educational? Learning theories embodied in games. In Proceedings of DiGRA 2005 Conference: Changing Views – Worlds in Play. Vancouver, BC, 2005.
- 29.Microbe Invader. 2013. http://www.microbeinvader.com/. Accessed 02 April 2019.
- 30.Foster AN. The process of learning in a simulation strategy game: disciplinary knowledge construction. J Educ Comp Res. 2011;45:1–27. doi: 10.2190/EC.45.1.a. [DOI] [Google Scholar]
- 31.Bochennek K, Wittekindt B, Zimmermann SY, Klingebiel T. More than mere games: a review of card and board games for medical education. Med Teach. 2007;29(9):941–948. doi: 10.1080/01421590701749813. [DOI] [PubMed] [Google Scholar]