

Many drugs have been used in the treatment of COVID-19 since the beginning of the pandemic. In a large multicenter cohort study of 137 870 individuals hospitalized with confirmed or suspected COVID-19, investigators assessed temporal and institutional variation in the use of 3 of the most widely used drugs: hydroxychloroquine, remdesivir, and dexamethasone.
Visual Abstract. Use of COVID-19 Drugs in Hospitalized U.S. Adults.

Many drugs have been used in the treatment of COVID-19 since the beginning of the pandemic. In a large multicenter cohort study of 137 870 individuals hospitalized with confirmed or suspected COVID-19, investigators assessed temporal and institutional variation in the use of 3 of the most widely used drugs: hydroxychloroquine, remdesivir, and dexamethasone.
Abstract
Background:
Relatively little is known about the use patterns of potential pharmacologic treatments of COVID-19 in the United States.
Objective:
To use the National COVID Cohort Collaborative (N3C), a large, multicenter, longitudinal cohort, to characterize the use of hydroxychloroquine, remdesivir, and dexamethasone, overall as well as across individuals, health systems, and time.
Design:
Retrospective cohort study.
Setting:
43 health systems in the United States.
Participants:
137 870 adults hospitalized with COVID-19 between 1 February 2020 and 28 February 2021.
Measurements:
Inpatient use of hydroxychloroquine, remdesivir, or dexamethasone.
Results:
Among 137 870 persons hospitalized with confirmed or suspected COVID-19, 8754 (6.3%) received hydroxychloroquine, 29 272 (21.2%) remdesivir, and 53 909 (39.1%) dexamethasone during the study period. Since the release of results from the RECOVERY (Randomised Evaluation of COVID-19 Therapy) trial in mid-June, approximately 78% to 84% of people who have had invasive mechanical ventilation have received dexamethasone or other glucocorticoids. The use of hydroxychloroquine increased during March 2020, peaking at 42%, and started declining by April 2020. By contrast, remdesivir and dexamethasone use gradually increased over the study period. Dexamethasone and remdesivir use varied substantially across health centers (intraclass correlation coefficient, 14.2% for dexamethasone and 84.6% for remdesivir).
Limitation:
Because most N3C data contributors are academic medical centers, findings may not reflect the experience of community hospitals.
Conclusion:
Dexamethasone, an evidence-based treatment of COVID-19, may be underused among persons who are mechanically ventilated. The use of remdesivir and dexamethasone varied across health systems, suggesting variation in patient case mix, drug access, treatment protocols, and quality of care.
Primary Funding Source:
National Center for Advancing Translational Sciences; National Heart, Lung, and Blood Institute; and National Institute on Aging.
As of 9 July 2021, more than 33 million infections and 598 000 deaths directly attributable to the COVID-19 pandemic have occurred in the United States (1). Because of this, major investments have been made to repurpose existing medications, as well as to develop new therapies, to prevent and treat COVID-19.
Although many investigational studies remain under way, 3 medications—hydroxychloroquine, remdesivir, and dexamethasone—have been subject to particular scientific scrutiny. Early interest in hydroxychloroquine, an antiinflammatory treatment of rheumatologic conditions and malaria, was based on evidence of in vitro activity against SARS-CoV-2 and small studies that assessed viral load and mortality (2). Although the U.S. Food and Drug Administration (FDA) issued an emergency use authorization (EUA) for hydroxychloroquine in March 2020 (3), that EUA was rescinded in June 2020 (4) on the basis of observational and randomized evidence failing to show benefit (5, 6). By contrast, remdesivir received an EUA in May 2020 on the basis of preliminary results from ACCT (Adaptive COVID-19 Treatment Trial) (7) and full FDA approval in October 2020 (8). Dexamethasone, already approved by the FDA for various indications, has been shown to reduce COVID-19 mortality among hospitalized patients requiring oxygen alone or mechanical ventilation (9, 10). Current clinical guidelines from the National Institutes of Health include both remdesivir and dexamethasone as treatments for some adults hospitalized with clinically suspected or laboratory-confirmed SARS-CoV-2 infection (11).
Despite rapidly accumulating evidence on safety and efficacy, far less is known about how treatments have been used in the United States. For example, although several studies have documented increases in use of hydroxychloroquine (12, 13) and remdesivir (14) and others have examined potential drivers of such use (14), analyses have generally been limited to aggregated, national-level claims or single institutions. Furthermore, how much the use of these products has varied across patients and health systems is unclear (15, 16). We used the National COVID Cohort Collaborative (N3C), a large, multicenter, longitudinal cohort of persons with confirmed or suspected COVID-19 in the United States, to comprehensively characterize the use of hydroxychloroquine, remdesivir, and dexamethasone to treat COVID-19. In addition to quantifying adoption, we also characterized hydroxychloroquine de-adoption and variation in treatments across varied health systems.
Methods
Data, Design, and Cohort Derivation
The N3C is a unique electronic health record repository supported by the National Institutes of Health whose structure, access, and analytic process have been previously described (17). In brief, the N3C represents the largest cohort of patients with COVID-19 in the United States to date and contains detailed, patient-level data for a racially, ethnically, and geographically diverse group of individuals. It queries electronic health record data from single- and multihospital health systems across the United States and stores data in a central location. As of 27 May 2021, the N3C included more than 2 million patients positive for COVID-19 (18). We used the limited data set, which contains deidentified data, patient ZIP codes, and exact dates of service use.
This retrospective cohort study included adults hospitalized with COVID-19 from 43 health centers between 1 February 2020 and 28 February 2021. We used the N3C definition to define COVID-19 (Supplement Table) (19–21). We limited our cohort to persons with an inpatient encounter and required the encounter to have occurred no longer than 21 days after the patient was designated as COVID-19–positive; we also allowed individuals to be diagnosed with COVID-19 within 5 days of their hospitalization to account for delays in access to testing and reporting. Given our interest in the use of therapeutics, we restricted analyses to people who remained hospitalized for at least 1 day. We considered only a first hospital stay related to COVID-19 and excluded subsequent inpatient encounters after initial discharge. Finally, we excluded 24 persons (0.02%) with missing information about sex, as well as all individuals younger than 18 years because of different treatment indications and COVID-19 trajectory in pediatric populations.
The results from the RECOVERY (Randomised Evaluation of COVID-19 Therapy) trial on dexamethasone were released in mid-June and showed clinical benefit among patients who received invasive mechanical ventilation or oxygen (9). In subanalyses to determine dexamethasone use per the clinical evidence, we restricted our cohort to persons hospitalized between July 2020 and February 2021. Furthermore, except in Figure 1, we did analyses for dexamethasone stratified by invasive mechanical ventilation.
Figure 1. Use of hydroxychloroquine, remdesivir, and dexamethasone among individuals hospitalized with COVID-19, 1 February 2020 to 28 February 2021 (n = 137 870).

Supplement Figure 2 shows dexamethasone use among persons with and without mechanical ventilation. EUA = emergency use authorization; FDA = U.S. Food and Drug Administration; RECOVERY = Randomised Evaluation of COVID-19 Therapy.
Key Variables of Interest
We used date-stamped records of inpatient medication to capture use of hydroxychloroquine, remdesivir, and dexamethasone. We examined sociodemographic and clinical characteristics, including age, sex, body mass index, comorbidity burden, and calendar week of hospital admission. We also examined race and ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, Asian, or another race), which are generally self-reported by patients or family members (24). We used information from COVID-19 admission and inpatient and outpatient data in the 1 year before the date of COVID-19 admission to characterize comorbid conditions using the Charlson Comorbidity Index, a validated measure that applies weights to 17 comorbid conditions (25). Severity of COVID-19 was measured by the development of acute kidney injury during hospitalization, use of invasive mechanical ventilation, or need for extracorporeal membrane oxygenation (20). All patients were classified into mutually exclusive categories of COVID-19 severity—for example, receipt versus no receipt of mechanical ventilation. For each center, we calculated weekly case volume of hospitalized patients with COVID-19 over the study period.
Statistical Analysis
In the overall cohort, we used descriptive statistics to examine trends in product use. First, we separately quantified the weekly proportion of persons within each health system exposed to each product of interest. Here, the denominator included all persons who were hospitalized at any point during the week. Next, we characterized and visually inspected time trends for the 3 products of interest, looking for inflection points, influential outliers, and general trends. We superimposed selected events of interest, including FDA regulatory actions and publication of major clinical trial results, as we evaluated trends in use. We also used box plots to visually show variation in drug use across the centers.
Among ventilated patients who were hospitalized between July 2020 and February 2021, we used descriptive statistics to quantify potential underuse of dexamethasone. Because glucocorticoids other than dexamethasone may have been used (26), we included any oral glucocorticoid use among patients hospitalized with COVID-19 from July 2020 to February 2021. Furthermore, we restricted analysis to patients who remained hospitalized for at least 1 day to ensure that they were eligible to receive dexamethasone or other glucocorticoids. We plotted percentage of dexamethasone use for each center to visualize variation across centers, stratified by mechanical ventilation status.
We used 2-level hierarchical logistic regression models, nesting patients within health centers, to model the odds of a given individual receiving hydroxychloroquine, remdesivir, or dexamethasone. Health centers were included as random intercepts in the model, and we did not control for any patient or hospital characteristics. We quantified variation in use across health systems and used a latent variable approach to estimate intraclass correlation coefficients (ICCs) for each product of interest. The ICCs from these models represent the amount of variation in the underlying propensity to be prescribed medication due to systematic differences between health centers.
We did 2 sensitivity analyses. First, because patients with diabetes may have been less likely to receive glucocorticoids because they can increase blood glucose levels, we examined glucocorticoid use stratified by diabetes status. Second, we determined variation in time to dexamethasone use and duration of use by race/ethnicity and health center.
We extracted data using queries in Spark SQL (Apache Software Foundation) and Python (Python Software Foundation) in the N3C Data Enclave and completed all analyses using R (R Foundation), version 3.5.1. The Johns Hopkins Medicine Institutional Review Boards waived the requirement for informed consent and deemed work in the N3C Data Enclave to be exempt research.
Role of the Funding Source
The funders had no influence on the study's design, conduct, or reporting.
Results
Characteristics of the Study Sample
Among 1 109 631 persons with confirmed or suspected COVID-19 in the N3C cohort through 5 March 2021, a total of 162 150 (14.6%) were hospitalized during the study period. After excluding individuals from 2 sites because of data quality issues (n = 6336), those who were younger than 18 years (n = 5828), those whose length of stay was 0 days (n = 12 092), and those with missing information on sex (n = 24), we had a final cohort of 137 870 persons (Appendix Figure). The Table describes characteristics of the study cohort. Among the 137 870 hospitalized patients, the mean age was 59.4 years (SD, 18.8), 50.4% were male, and 47.8% were non-Hispanic White. Nearly 34.2% of hospitalized participants had none of the comorbid conditions assessed by the Charlson Comorbidity Index, whereas 19.8% had a score of one, 11.9% a score of two, 8.4% a score of three, and 25.8% a score of four or greater. Overall, 6.3% patients received hydroxychloroquine, 21.2% remdesivir, 39.1% dexamethasone, and 17.2% both remdesivir and dexamethasone during their COVID-19 hospitalization.
Appendix Figure. Study flow diagram.
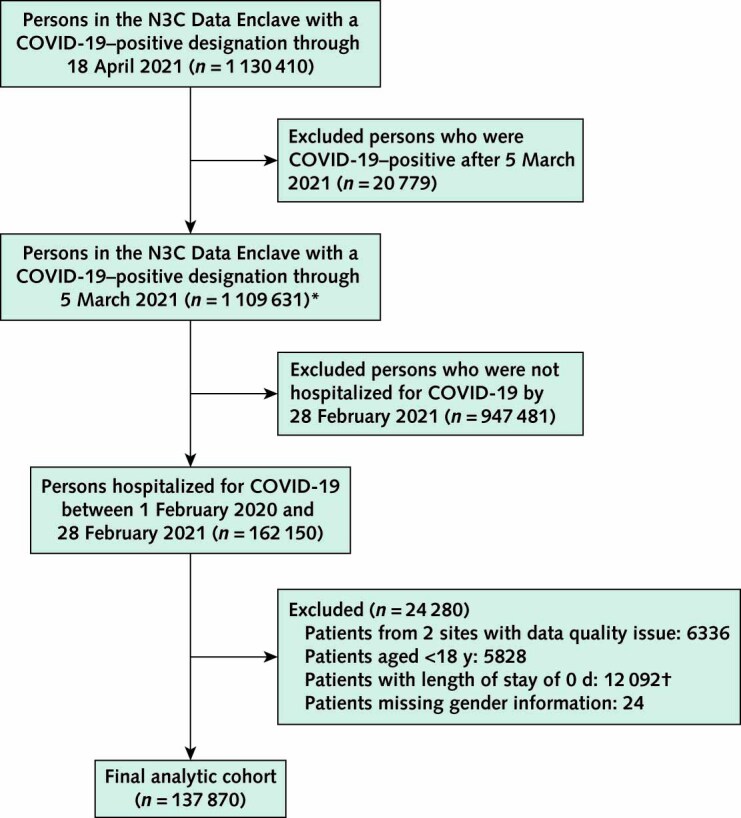
N3C = National COVID Cohort Collaborative.
* Our cohort definition allowed for persons to be designated as COVID-19–positive up to 5 d after admission, to account for delays in test reporting. For this reason, the first step allowed COVID-19–positive designation through 5 March 2021 and hospitalization through 28 February 2021.
† Of 12 092 individuals discharged on the same day who were excluded from the analysis, 188 (1.6%) died on that day.
Table.
Drug Use, by Patient Characteristics, Among Persons Hospitalized With COVID-19*

Trends in Hydroxychloroquine, Remdesivir, and Dexamethasone Use
Figure 1 shows trends in the use of hydroxychloroquine, remdesivir, and dexamethasone between February 2020 and February 2021. Beginning in March 2020, hydroxychloroquine use increased sharply, peaking at 42% of patients in late March before rapidly decreasing to approximately 7% by late April 2020 and subsequently to 0.6% by February 2021 among hospitalized individuals with COVID-19. By contrast, remdesivir use first increased rapidly in May 2020 from approximately 2% to 10% of patients, and since May 2020 it has increased gradually to 27% of those hospitalized in February 2021. Finally, about 4% of individuals or fewer used dexamethasone through May 2020; this percentage increased markedly during June and July 2020 to approximately 33%, continued to increase more gradually thereafter to about 53% of hospitalized individuals as of November 2020, and then declined to 33% by February 2021. Combined use of remdesivir and dexamethasone increased from 0.2% in May 2020 to 22.7% in February 2021 (Supplement Figure 1).
Characteristics of Persons Receiving COVID-19 Drugs
The Table shows the characteristics of persons in the cohort as well as those receiving each product. Dexamethasone was more commonly used among older adults (45.3% among those aged ≥75 years vs. 20.2% among those aged 18 to 34 years), males (41.3% vs. 36.8%), non-Hispanic White compared with non-Hispanic Black persons (45.4% vs. 33.6%), and those requiring mechanical ventilation (55.9% vs. 37.3%). We saw similar patterns when examining remdesivir use, with greater use among patients who were older, male, non-Hispanic White, or obese and those with more severe COVID-19 or comorbid illness.
Over the study period, dexamethasone use was higher among those who received mechanical ventilation than among those who did not (Supplement Figure 2). From July 2020 to February 2021, between 70% and 77% of mechanically ventilated patients received dexamethasone. After other glucocorticoids were accounted for, the use of dexamethasone or other glucocorticoids ranged from 78% to 84% (Supplement Figure 3 [A]), and the results persisted when we restricted the analysis to patients who remained hospitalized for 2 days or more (Supplement Figure 3 [B]).
Variation in Drug Use Across Health Centers
Figure 2 characterizes variation in the use of each product across the 43 health centers included in the study. We found wide variation in hydroxychloroquine use across health centers in March 2020, with reductions in such variation by late April 2020 (ICC, 36.7%). Remdesivir use varied substantially across health centers (ICC, 84.6%), and variation persisted from May 2020 to February 2021. The ICC for dexamethasone was lower (14.2%), indicating lower variation across health centers over the study period (February 2020 through February 2021). We saw greater variation in dexamethasone use across health centers among those who received mechanical ventilation than those who did not (ICC, 25.7% vs. 13.0%) (Figure 3 and Supplement Figure 4).
Figure 2. Variation in hydroxychloroquine, remdesivir, and dexamethasone use across health centers over time, 1 February 2020 to 28 February 2021 (n = 137 870).

Figure 3. Variation in dexamethasone use across health centers, stratified by invasive mechanical ventilation, 1 July 2020 to 28 February 2021 (n = 106 039).

All individuals were classified into mutually exclusive categories of mechanical ventilation. Left. Among patients who were mechanically ventilated; 40 centers were included. The dotted line shows the overall median of 79.7% of hospitalized adults with COVID-19 who were mechanically ventilated and received dexamethasone. Right. Among patients who were not mechanically ventilated; 43 centers were included. The dotted line shows the overall median of 44.9% of hospitalized adults with COVID-19 who were not mechanically ventilated and received dexamethasone.
Sensitivity Analyses
Among mechanically ventilated persons, use of dexamethasone or other glucocorticoids was more frequent among those with diabetes than those without (56.2% vs. 42.6%). The median time to initiation of dexamethasone therapy was 0 days (interquartile range, 0 to 1 days) among ventilated and nonventilated patients; median duration of use was 7 days (interquartile range, 1 to 10 days) among ventilated patients and 3 days (interquartile range, 1 to 7 days) among nonventilated patients (Supplement Figure 5). Time to dexamethasone initiation and duration of dexamethasone use did not differ by race/ethnicity (Supplement Figure 6) or health center (Supplement Figure 7).
Discussion
Despite enormous investments in the development of therapeutics to address COVID-19, relatively little is known about how treatments to address coronavirus infection have been used in the United States. Using the N3C, a large, multicenter, longitudinal, U.S. cohort, we characterized the use of hydroxychloroquine, remdesivir, and dexamethasone, overall as well as across individuals, health systems, and time. We found that brisk uptake and abandonment of hydroxychloroquine early in the pandemic has been offset by increases in use of remdesivir and, to an even greater degree, dexamethasone. Despite this, approximately one fifth of patients who were mechanically ventilated after the release of the RECOVERY trial results in mid-June, and therefore were potentially eligible for use, did not receive dexamethasone or any other glucocorticoid, and substantial variation in dexamethasone use was observed across sites. These findings are important because of continued high levels of morbidity and mortality in the United States due to COVID-19, as well as a robust evidence base supporting the value of dexamethasone in reducing the likelihood of death among persons with COVID-19 who require mechanical ventilation (10, 11).
There are many potential drivers of the treatment trends that we described. In the case of hydroxychloroquine, early enthusiasm and media coverage about its potential benefit was rapidly followed by accruing evidence of its ineffectiveness (27) and potential harms (28, 29), ultimately leading the FDA to revoke the EUA governing its use to treat COVID-19 (30). By contrast, both remdesivir and dexamethasone are supported by a rapidly growing body of evidence. Among hospitalized patients, remdesivir use was far less common than dexamethasone use—an interesting finding that may be due in part to remdesivir shortages and cost in the United States (31).
We also found that despite treatment guidelines from the National Institutes of Health regarding the use of dexamethasone for COVID-19, approximately one fifth of mechanically ventilated patients during the most recent months of observation in our cohort did not receive a glucocorticoid, a finding that persisted after those who may not have been eligible because of early discharge or death were excluded. Drug shortages of dexamethasone have been reported (32), and hospital policies may restrict its use to subsets of patients who are critically ill with COVID-19. The relatively high mortality in the control group of the RECOVERY trial (26%) might also raise questions about the applicability of those results to patients in the United States, where the in-hospital mortality from COVID-19 has been closer to 8% (33).
We found marked treatment variation across the 43 centers that we examined, consistent with a large and constantly evolving evidence base from other settings documenting variation across systems beyond that explainable by observable patient or provider characteristics alone (34–36). The centers contributing to the N3C represent a diverse group of health systems that differ in geographic region, size, profit status, staffing ratio, and managerial structure; although our study was not designed to evaluate the independent effect of these and other center characteristics, including clinical policies, they may nevertheless contribute to the variation that we found (37, 38). Clinicians may be reluctant to use corticosteroids in critically ill patients with COVID-19 because of the conflicting evidence for steroids in other forms of acute respiratory distress syndrome (39, 40). The fact that other trials of steroids in COVID-19 were stopped early and did not uniformly show the same mortality benefit may also contribute to the lack of universal use of steroids in mechanically ventilated patients with COVID-19 (41). Potential drug shortages, as well as a lack of clear and consistent communication about treatments in the context of an “infodemic,” has likely compounded matters (42–44). As we expected, variation in use was largest for remdesivir, a product shown to reduce hospital length of stay but not mortality (22), and smallest for dexamethasone, which has an established mortality benefit (10). Although not the direct focus of our research, several questions remain regarding how individual-level and health system characteristics may account for the variations in drug use that we describe.
Our study has limitations. First, the N3C is a database of aggregate reports from health systems with differing common data models, and thus some data of interest, such as oxygen delivery, were not available. Second, although the N3C is the largest U.S. cohort of patients with COVID-19 that has been assembled to date, the centers it includes are clustered in the Southeast, Mid-Atlantic, and Midwest regions, and because most data contributors are academic medical centers, our findings may not generalize to community-based hospitals (18, 45). However, the distributions of age, sex, race, and ethnicity in the N3C indicate a cohort that is representative of many segments of the U.S. population (18, 21). Third, our information on prescription drug exposure is a combination of information about medication ordering and medication administration, depending on the contributing center, and we do not have information about drug dose. Fourth, no baseline inpatient or outpatient information was available for about one third of individuals, and our data likely underestimate their comorbidity burden. Fifth, some persons may not have received dexamethasone because of its antecedent use before hospitalization. Finally, because of imprecise information on the start date of mechanical ventilation, we classified individuals as mechanically ventilated if they received ventilation at any point during their hospitalization.
Despite progress in identifying treatments of COVID-19, the pandemic continues to cause enormous morbidity and mortality in the United States. In this retrospective cohort study of the N3C, brisk uptake and abandonment of hydroxychloroquine early in the pandemic has been offset by increases in use of remdesivir and, to an even greater degree, dexamethasone. However, as many as one fifth of mechanically ventilated patients potentially eligible for dexamethasone did not receive it, and we noted substantial variation in remdesivir and dexamethasone use across sites.
Supplementary Material
Appendix: Members of the National COVID Cohort Collaborative (N3C)
Members of the N3C who authored this work: Hemalkumar B. Mehta, MS, PhD, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; Huijun An, MS, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; Kathleen M. Andersen, MSc, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; Omar Mansour, MHS, Monument Analytics, Baltimore, Maryland; Vithal Madhira, MS, Palila Software, Reno, Nevada; Emaan S. Rashidi, MHS, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; Benjamin Bates, MD, Rutgers Center for Pharmacoepidemiology and Treatment Science, New Brunswick, New Jersey; Soko Setoguchi, MD, DrPH, Rutgers Center for Pharmacoepidemiology and Treatment Science, New Brunswick, New Jersey; Corey Joseph, MPH, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; Paul T. Kocis, PharmD, MPH, Penn State Health, Milton S. Hershey Medical Center, Hershey, Pennsylvania; Richard Moffitt, PhD, Stony Brook University, Stony Brook, New York; Tellen D. Bennett, MD, MS, University of Colorado School of Medicine, University of Colorado, Aurora, Colorado; Christopher G. Chute, MD, DrPH, Schools of Medicine, Public Health, and Nursing, Johns Hopkins University, Baltimore, Maryland; Brian T. Garibaldi, MD, MEHP, Johns Hopkins University School of Medicine, Baltimore, Maryland; and G. Caleb Alexander, MD, MS, Johns Hopkins Bloomberg School of Public Health and Johns Hopkins School of Medicine, Baltimore, Maryland.
Members of the N3C who contributed to this work but did not author it: Melissa A. Haendel, PhD, Center for Health AI, University of Colorado Anschutz Medical Campus, Aurora, Colorado; Christopher G. Chute, DrPH, MPH, MD, Schools of Medicine, Public Health, and Nursing, Johns Hopkins University, Baltimore, Maryland; Carolyn Bramante, MPH, MD, University of Minnesota, Minneapolis, Minnesota; Farrukh M. Koraishy, PhD, MD, Stony Brook University, Stony Brook, New York; Stephanie S. Hong, BS, Johns Hopkins University School of Medicine, Baltimore, Maryland; and Richard L. Zhu, MD, MS, Johns Hopkins University School of Medicine, Baltimore, Maryland.
Footnotes
This article was published at Annals.org on 17 August 2021.
* For members of the National COVID Cohort Collaborative (N3C), see the Appendix.
References
- 1.Center for Systems Science and Engineering at Johns Hopkins University. COVID-19 Dashboard. 2021. Accessed at https://coronavirus.jhu.edu/map.html on 2 February 2021.
- 2.Keyaerts E, Vijgen L, Maes P, et al. In vitro inhibition of severe acute respiratory syndrome coronavirus by chloroquine. Biochem Biophys Res Commun. 2004;323:264-8. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hinton DM. Re: Request for emergency use authorization for use of chloroquine phosphate or hydroxychloroquine sulfate supplied from the Strategic National Stockpile for treatment of 2019 coronavirus disease. 28 March 2020. Accessed at www.fda.gov/media/136534/download on 2 February 2021.
- 4.U.S. Food and Drug Administration. FDA cautions against use of hydroxychloroquine or chloroquine for COVID-19 outside of the hospital setting or a clinical trial due to risk of heart rhythm problems. Updated 1 July 2020. Accessed at www.fda.gov/drugs/drug-safety-and-availability/fda-cautions-against-use-hydroxychloroquine-or-chloroquine-covid-19-outside-hospital-setting-or on 2 February 2021.
- 5.Rosenberg ES, Dufort EM, Udo T, et al. Association of treatment with hydroxychloroquine or azithromycin with in-hospital mortality in patients with COVID-19 in New York State. JAMA. 2020;323:2493-2502. [PMID: ] doi: 10.1001/jama.2020.8630 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tang W, Cao Z, Han M, et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: open label, randomised controlled trial. BMJ. 2020;369:m1849. [PMID: ] doi: 10.1136/bmj.m1849 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.National Institute of Allergy and Infectious Diseases. NIH clinical trial shows remdesivir accelerates recovery from advanced COVID-19. 29 April 2020. Accessed at www.niaid.nih.gov/news-events/nih-clinical-trial-shows-remdesivir-accelerates-recovery-advanced-covid-19 on 2 February 2021.
- 8.Hinton DM. Veklury (remdesivir) EUA letter of approval. 22 October 2020. Accessed at www.fda.gov/media/137564/download on 2 February 2021.
- 9.Ledford H. Coronavirus breakthrough: dexamethasone is first drug shown to save lives. Nature. 2020;582:469. [PMID: ] doi: 10.1038/d41586-020-01824-5 [DOI] [PubMed] [Google Scholar]
- 10.Horby P, Lim WS, Emberson JR, et al; RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384:693-704. [PMID: ] doi: 10.1056/NEJMoa2021436 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. 2021. Accessed at www.covid19treatmentguidelines.nih.gov on 2 February 2021. [PubMed]
- 12.Shehab N, Lovegrove M, Budnitz DS. US hydroxychloroquine, chloroquine, and azithromycin outpatient prescription trends, October 2019 through March 2020. JAMA Intern Med. 2020;180:1384-1386. [PMID: ] doi: 10.1001/jamainternmed.2020.2594 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bull-Otterson L, Gray EB, Budnitz DS, et al. Hydroxychloroquine and chloroquine prescribing patterns by provider specialty following initial reports of potential benefit for COVID-19 treatment — United States, January–June 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1210-1215. [PMID: ] doi: 10.15585/mmwr.mm6935a4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lin KJ, Schneeweiss S, Tesfaye H, et al. Pharmacotherapy for hospitalized patients with COVID-19: treatment patterns by disease severity. Drugs. 2020;80:1961-1972. [PMID: ] doi: 10.1007/s40265-020-01424-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McPherson K, Wennberg JE, Hovind OB, et al. Small-area variations in the use of common surgical procedures: an international comparison of New England, England, and Norway. N Engl J Med. 1982;307:1310-4. [PMID: ] [DOI] [PubMed] [Google Scholar]
- 16.Chassin MR, Brook RH, Park RE, et al. Variations in the use of medical and surgical services by the Medicare population. N Engl J Med. 1986;314:285-90. [PMID: ] [DOI] [PubMed] [Google Scholar]
- 17.Haendel MA, Chute CG, Bennett TD, et al; N3C Consortium. The national COVID Cohort Collaborative (N3C): rationale, design, infrastructure, and deployment. J Am Med Inform Assoc. 2021;28:427-443. [PMID: ] doi: 10.1093/jamia/ocaa196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.N3C Cohort Exploration. Accessed at https://covid.cd2h.org/dashboard on 21 April 2021.
- 19.N3C Phenotype Documentation. Updated 14 April 2020. Accessed at https://covid.cd2h.org/phenotyping on 2 February 2021.
- 20.COVID-19 phenotype documentation, version 3.0. Updated 12 November 2020. Accessed at https://github.com/National-COVID-Cohort-Collaborative/Phenotype_Data_Acquisition/wiki/Latest-Phenotype on 2 February 2021.
- 21.Bennett TD, Moffitt RA, Hajagos JG, et al; National COVID Cohort Collaborative (N3C) Consortium. Clinical characterization and prediction of clinical severity of SARS-CoV-2 infection among US adults using data from the US National COVID Cohort Collaborative. JAMA Netw Open. 2021;4:e2116901. [PMID: ] doi: 10.1001/jamanetworkopen.2021.16901 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Beigel JH, Tomashek KM, Dodd LE, et al; ACTT-1 Study Group Members. Remdesivir for the treatment of Covid-19 — final report. N Engl J Med. 2020;383:1813-1826. [PMID: ] doi: 10.1056/NEJMoa2007764 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Goldman JD, Lye DCB, Hui DS, et al; GS-US-540-5773 Investigators. Remdesivir for 5 or 10 days in patients with severe Covid-19. N Engl J Med. 2020;383:1827-1837. [PMID: ] doi: 10.1056/NEJMoa2015301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hasnain-Wynia R, Baker DW. Obtaining data on patient race, ethnicity, and primary language in health care organizations: current challenges and proposed solutions. Health Serv Res. 2006;41:1501-18. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-83. [PMID: ] [DOI] [PubMed] [Google Scholar]
- 26.Angus DC, Derde L, Al-Beidh F, et al; Writing Committee for the REMAP-CAP Investigators. Effect of hydrocortisone on mortality and organ support in patients with severe COVID-19: the REMAP-CAP COVID-19 corticosteroid domain randomized clinical trial. JAMA. 2020;324:1317-1329. [PMID: ] doi: 10.1001/jama.2020.17022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Horby P, Mafham M, Linsell L, et al; RECOVERY Collaborative Group. Effect of hydroxychloroquine in hospitalized patients with Covid-19. N Engl J Med. 2020;383:2030-2040. [PMID: ] doi: 10.1056/NEJMoa2022926 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mercuro NJ, Yen CF, Shim DJ, et al. Risk of QT interval prolongation associated with use of hydroxychloroquine with or without concomitant azithromycin among hospitalized patients testing positive for coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5:1036-1041. [PMID: ] doi: 10.1001/jamacardio.2020.1834 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Chorin E, Wadhwani L, Magnani S, et al. QT interval prolongation and torsade de pointes in patients with COVID-19 treated with hydroxychloroquine/azithromycin. Heart Rhythm. 2020;17:1425-1433. [PMID: ] doi: 10.1016/j.hrthm.2020.05.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hinton DM. Letter revoking EUA for chloroquine phosphate and hydroxychloroquine sulfate. 15 June 2020. Accessed at www.fda.gov/media/138945/download on 2 February 2021.
- 31.Boodman E. From Houston to Miami, hospitals running short of remdesivir for Covid-19 patients. STAT. 10 July 2020. Accessed at www.statnews.com/2020/07/10/hospitals-running-short-of-remdesivir-for-covid19-patients on 2 February 2021.
- 32.Silverman E. Hospitals see shortages of a cheap steroid that one study says helps Covid-19 patients. STAT. 25 June 2020. Accessed at www.statnews.com/pharmalot/2020/06/25/covid19-coronavirus-dexamethasone-shortages on 2 February 2021.
- 33.Asch DA, Sheils NE, Islam MN, et al. Variation in US hospital mortality rates for patients admitted with COVID-19 during the first 6 months of the pandemic. JAMA Intern Med. 2021;181:471-478. [PMID: ] doi: 10.1001/jamainternmed.2020.8193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wennberg J, Gittelsohn A. Variations in medical care among small areas. Sci Am. 1982;246:120-34. [PMID: ] [DOI] [PubMed] [Google Scholar]
- 35.Zhang Y, Baicker K, Newhouse JP. Geographic variation in the quality of prescribing. N Engl J Med. 2010;363:1985-8. [PMID: ] doi: 10.1056/NEJMp1010220 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Zhang Y, Steinman MA, Kaplan CM. Geographic variation in outpatient antibiotic prescribing among older adults. Arch Intern Med. 2012;172:1465-71. [PMID: ] doi: 10.1001/archinternmed.2012.3717 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.FACTBOX-U.S. hospitals differ on best use of hydroxychloroquine for coronavirus. Reuters. 6 April 2020. Accessed at www.reuters.com/article/health-coronavirus-usa-hydroxychloroquin-idUSL1N2BU1K5 on 2 February 2021.
- 38.Morgan SG, Cunningham CM, Hanley GE. Individual and contextual determinants of regional variation in prescription drug use: an analysis of administrative data from British Columbia. PLoS One. 2010;5:e15883. [PMID: ] doi: 10.1371/journal.pone.0015883 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Venkatesh B, Finfer S, Cohen J, et al; ADRENAL Trial Investigators and the Australian–New Zealand Intensive Care Society Clinical Trials Group. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378:797-808. [PMID: ] doi: 10.1056/NEJMoa1705835 [DOI] [PubMed] [Google Scholar]
- 40.Villar J, Ferrando C, Martínez D, et al; Dexamethasone in ARDS Network. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med. 2020;8:267-276. [PMID: ] doi: 10.1016/S2213-2600(19)30417-5 [DOI] [PubMed] [Google Scholar]
- 41.Carlet J, Payen D, Opal SM. Steroids for sepsis and ARDS: this eternal controversy remains with COVID-19 [Letter]. Lancet. 2020. [PMID: ] doi: 10.1016/S0140-6736(20)32132-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Eysenbach G. How to fight an infodemic: the four pillars of infodemic management [Editorial]. J Med Internet Res. 2020;22:e21820. [PMID: ] doi: 10.2196/21820 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Zarocostas J. How to fight an infodemic. Lancet. 2020;395:676. [PMID: ] doi: 10.1016/S0140-6736(20)30461-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Saag MS. Misguided use of hydroxychloroquine for COVID-19: the infusion of politics into science [Editorial]. JAMA. 2020;324:2161-2162. [PMID: ] doi: 10.1001/jama.2020.22389 [DOI] [PubMed] [Google Scholar]
- 45.National Center for Advancing Translational Sciences. Data Transfer Agreement Signatories. Accessed at https://ncats.nih.gov/n3c/resources/data-contribution/data-transfer-agreement-signatories on 2 February 2021.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.