

Key Points
Question
Is there an association between changes in atrial fibrillation (AF) burden and health-related quality of life after AF ablation?
Findings
In the CIRCA-DOSE randomized clinical trial including 346 patients with AF, a reduction in AF burden postablation was related to a statistically significant improvement in quality of life. At 12 months postablation, an absolute reduction in AF burden of 15.8 minutes or a relative reduction of 0.63% from baseline was associated with a 1-point improvement in Atrial Fibrillation Effect on Quality of Life (AFEQT) score.
Meaning
In this trial of patients with an overall low preablation AF burden, there was an inverse association between change in AF burden and AFEQT score following ablation, with a clinically meaningful improvement in quality of life being observed for every 30.2% relative reduction in AF burden from baseline.
This post hoc analysis of a randomized clinical trial evaluates the association between change in atrial fibrillation burden and quality of life among patients with a low preablation atrial fibrillation burden.
Abstract
Importance
Patients with atrial fibrillation (AF) have impaired health-related quality of life primarily owing to symptoms related to AF episodes; however, quality of life can be influenced by AF therapies, AF complications, the frequency of follow-up visits and hospitalizations, illness perceptions, and patient factors, such as anxiety or depression.
Objective
To determine the association between change in AF burden and quality of life in the year following ablation.
Design, Setting, and Participants
The current study is a secondary analysis of a prospective, parallel-group, multicenter, single-masked randomized clinical trial (Cryoballoon vs Irrigated Radiofrequency Catheter Ablation: Double Short vs Standard Exposure Duration [CIRCA-DOSE] study), which took place at 8 Canadian centers. Between September 2014 and July 2017, 346 patients older than 18 years with symptomatic, primarily low-burden AF refractory to antiarrhythmic therapy referred for first catheter ablation were enrolled. All patients received an implantable cardiac monitor at least 30 days before ablation and were followed up with up to December 2018. Data were analyzed from April 2020 to June 2021.
Interventions
Patients were randomized 1:1:1 to contact force–guided radiofrequency ablation, 4-minute cryoballoon ablation, or 2-minute cryoballoon ablation. The exposure in the present analysis is the absolute difference in AF burden prior to ablation and 12 months following ablation, as evaluated by the Atrial Fibrillation Effect on Quality of Life (AFEQT) Score.
Main Outcomes and Measures
Absolute difference in quality of life from baseline to 12 months postablation.
Results
Of 346 included patients, 231 (66.7%) were male, and the median (interquartile range) age was 60 (52-66) years. A total of 328 patients (94.8%) had paroxysmal AF. The median (interquartile range) preablation AF burden was 2.0% (0.1-11.9), and the AF burden decreased to 0% at 12 months postablation. At 12 months, a 1-point improvement in AFEQT score was observed for every absolute reduction in daily AF burden of 15.8 minutes (95% CI, 7.2-24.4; P < .001), or every 0.63% (95% CI, 0.30-0.95; P < .001) reduction in relative AF burden from baseline.
Conclusions and Relevance
In patients with primarily low-burden paroxysmal AF, the reduction in AF burden following ablation may be associated with a clinically meaningful improvement in quality of life.
Trial Registration
ClinicalTrials.gov Identifier: NCT01913522
Introduction
Atrial fibrillation (AF) is associated with significant impairments in functional capacity and health-related quality of life.1 These impairments have been noted across multiple quality-of-life domains, with a magnitude comparable with or worse than that observed in patients with coronary artery disease, with heart failure, or receiving long-term hemodialysis. As lower quality-of-life scores in patients with AF are associated with an increased risk of hospitalization, a key facet of AF management centers on symptomatic improvement with consequent reduction in disability and health care resource utilization (eg, emergency department visits, hospitalization).2,3,4
Catheter ablation has been shown to reduce recurrences of AF and has been associated with improvements in quality of life in multiple randomized trials.3,5,6,7 While the beneficial effect of catheter ablation has traditionally been linked to absolute freedom from recurrent arrhythmia, many patients report improvement in their functional status and quality of life even if they experience an AF recurrence.3,6,7,8,9,10 It has been proposed that quality-of-life improvements may be secondary to a reduction in the overall burden of arrhythmia and is not dependent on complete arrhythmia elimination.11
The Cryoballoon vs Irrigated Radiofrequency Catheter Ablation: Double Short vs Standard Exposure Duration (CIRCA-DOSE) randomized clinical trial5 provides a unique opportunity to assess the association of AF burden and quality of life in patients undergoing ablation by virtue of the universal use of implantable cardiac monitoring (ICM). Our objective was to determine the association of quality of life with change in AF burden postablation assessed by continuous rhythm monitoring.
Methods
Clinical Trial
The CIRCA-DOSE study was a multicenter, single-blind randomized clinical trial in which patients with predominantly low-burden paroxysmal AF refractory to therapy were randomized 1:1:1 to contact force–guided radiofrequency ablation, 4-minute cryoablation, or 2-minute cryoablation.5 Details of the protocol have been reported previously.5,12 The study was approved by the institutional review committee at each center and can be found in Supplement 1. All patients provided written informed consent.
Health-Related Quality of Life
Quality of life was evaluated with the disease-specific Atrial Fibrillation Effect on Quality of Life (AFEQT) questionnaire, with 0 representing the worst and 100 representing the best possible quality of life (ie, no impairment due to AF).2 Questionnaires were administered at enrollment (median 73.5 days prior to ablation) and at 6 and 12 months postablation. Quality of life scores at 6 and 12 months were subtracted from the preablation scores to measure the absolute difference in quality of life.
AF Burden
All patients underwent insertion of an ICM 30 to 90 days prior to ablation. AF burden was defined as the proportion of total time a patient was in AF and is reported as minutes of AF per day as well as the percentage of time spent in AF per day. Baseline AF burden was measured prior to ablation. Postablation AF burden was assessed in the 30-day interval prior to AFEQT questionnaire administration at 6 months and 12 months following ablation, as this corresponded directly to the period evaluated by the AFEQT quality-of-life questionnaire. The per-patient change in AF burden was computed as the absolute difference in AF burden from preablation to 6 and 12 months postablation.
Statistical Analysis
Descriptive statistics are reported as medians and interquartile ranges (IQRs) for continuous variables and counts and percentages for categorical variables. Medians and IQRs of the AF burden and AFEQT score at baseline, 6 months, and 12 months were compared with the Wilcoxon rank sum test. Linear regression was performed to determine the magnitude of the association between the absolute and relative difference in AF burden (minutes of AF and percentage change from baseline, respectively) and quality of life from preablation to 12 months postablation. Sensitivity analyses comparing the absolute difference in AF burden and quality of life between 6 months and baseline as well as subgroup analyses of patients with documented arrhythmia recurrence, patients with symptomatic/asymptomatic events, and by intervention arm were also conducted. Patients were classified as symptomatic if any AF events were reported as symptomatic. All statistical tests and confidence intervals were 2-sided, and P values less than .05 were considered statistically significant. All analyses were performed with Stata version 16 (StataCorp).
Results
A total of 346 patients were enrolled in the CIRCA-DOSE study. The median (IQR) age was 60 (52-66) years, 231 (66.7%) were male, and 328 (94.8%) had paroxysmal AF (Table 1). The median (IQR) preablation AF burden was 2.0% (0.1-11.9), and the AF burden decreased to 0% at 12 months postablation. There was a statistically significant decrease in AF burden from preablation to 6 months postablation (median [IQR] absolute difference, 24.62 [0.86-153.22] minutes per day; P < .001) and 12 months postablation (median [IQR] absolute difference, 23.90 [0.86-161.14] minutes per day; P = .001) (Table 2). Symptomatic AF recurrence was reported in 80 patients (23.1%).
Table 1. Baseline Characteristics.
| Characteristic | No. (%) |
|---|---|
| Total, No. | 346 |
| Age, median (IQR), y | 60 (52-66) |
| Male | 231 (66.7) |
| AF type | |
| Low-burden paroxysmal AF | 102 (29.5) |
| High-burden paroxysmal AF | 226 (65.3) |
| Persistent AF | 18 (5.2) |
| Hypertension | 120 (34.7) |
| Diabetes | 29 (8.4) |
| Coronary artery disease | 32 (9.2) |
| Myocardial infarction | 17 (4.9) |
| Peripheral artery disease | 4 (0.6) |
| Congestive heart failure | 6 (1.6) |
| Chronic kidney disease | 4 (1.2) |
| Chronic obstructive pulmonary disease | 7 (2.0) |
| Previous stroke or transient ischemic attack | 16 (4.6) |
| CHA2DS2-Vasc score, median (IQR) | 1 (0-2) |
Abbreviations: AF, atrial fibrillation; IQR, interquartile range.
Table 2. Atrial Fibrillation (AF) Burden and Quality of Life at Baseline, 6 Months, and 12 Months.
| Time | AF burden, median (IQR) | AFEQT score, median (IQR) | |||
|---|---|---|---|---|---|
| Time in atrial fibrillation, % | Absolute difference in time in AF, min of AF/da | Relative difference in AF burden, % | Score | Absolute differenceb | |
| Preablation baseline | 2.02 (0.12 to 11.91) | NA | NA | 53.70 (38.88 to 71.30) | NA |
| 6 mo Postablation | 0 (0 to 0.01) | –24.62 (–153.22 to –0.86)c | –100 (–100 to –67.09) | 92.59 (77.78 to 98.15) | 30.09 (14.81 to 45.89)c |
| 12 mo Postablation | 0 | –23.90 (–161.14 to –0.86)c | –100 (–100 to –71.00) | 93.52 (81.48 to 99.07) | 32.33 (17.78 to 48.79)c |
Abbreviations: AFEQT, Atrial Fibrillation Effect on Quality of Life; IQR, interquartile range; NA, not applicable.
Differences in AF burden are calculated as the AF burden at 6 months or 12 months minus the preablation AF burden.
Differences in AFEQT score was calculated as the score at 6 months or 12 months minus the preablation score.
P < .05.
There was a statistically significant improvement in AFEQT score at 6 and 12 months postablation compared with baseline (Table 2). Among all patients, a significant association was observed between the change in AFEQT score and the change in absolute and relative AF burden, with a 1-point improvement in AFEQT score being observed for every 15.8-minute (95% CI, 7.2-24.4; P < .001) absolute reduction in daily AF burden (Figure, A) or for every 0.63% (95% CI, 0.30-0.95; P < .001) relative reduction in AF burden (Figure, B).
Figure. Association Between Atrial Fibrillation (AF) Burden and Quality of Life.
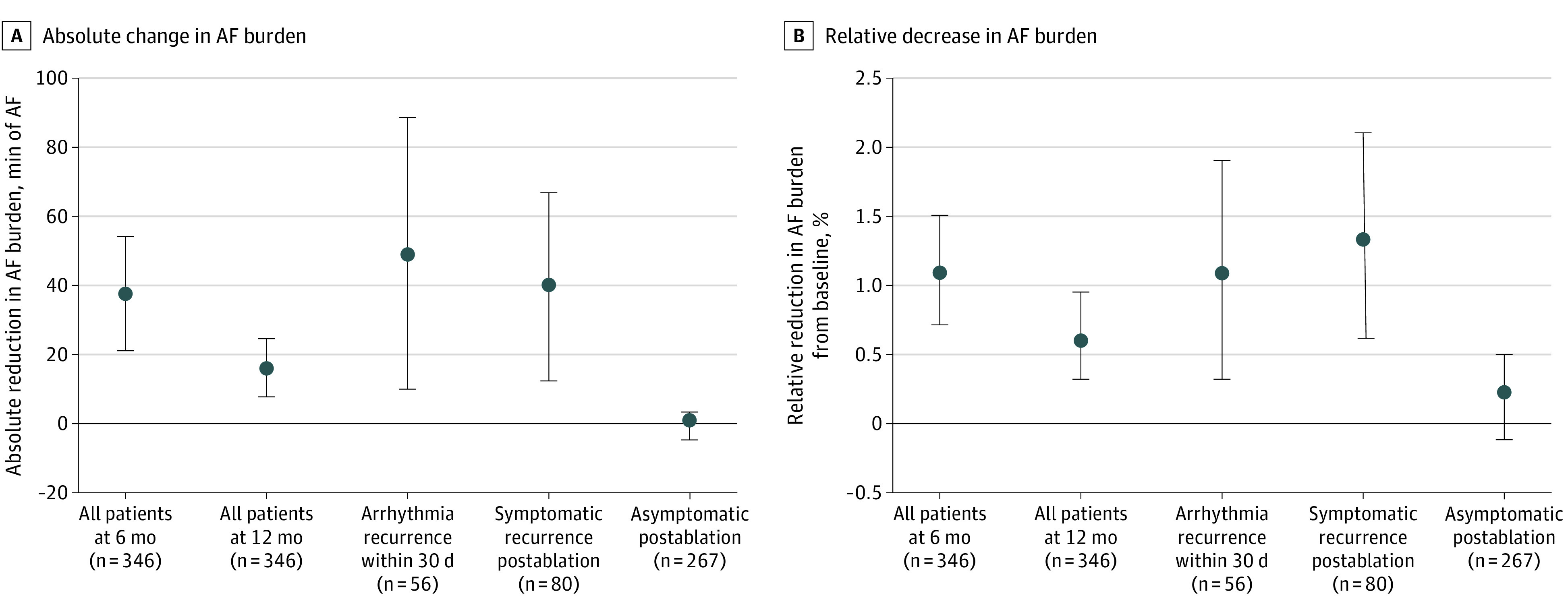
Effect estimates are presented as the change in AF burden associated with a 1-point improvement in the disease-specific Atrial Fibrillation Effect on Quality of Life score. A, Absolute change in AF burden as measured in minutes of AF per day. B, Relative decrease in AF burden as measured in percentage change from baseline. Error bars indicate 95% CIs.
Among patients who went to 0% time in AF, the mean (SD) improvement in AFEQT score was 33.8 (20.3) at 6 months and 33.6 (19.9) at 12 months. Among patients with a documented atrial tachyarrhythmia recurrence (eg, a nonzero AF burden), a significant association was observed between the change in AFEQT score and AF burden. At 12 months, a 1-point improvement in AFEQT score was observed for every 49.1-minute (95% CI, 9.4-88.8; P = .02) absolute reduction in daily AF burden or for every 1.08% (95% CI, 0.30-1.86; P = .008) relative reduction in AF burden from baseline. The direction and magnitude of association between the change in AFEQT score and reduction in AF burden was greater in subgroup patients with a higher baseline AF burden and those with symptomatic recurrences.
Among patients with a nonzero burden at baseline, a significant association was observed between the change in AFEQT score and the change in absolute and relative AF burden. At 12 months, a 1-point improvement in AFEQT score was observed for every 21.7-minute (95% CI, 10.4-32.9; P < .001) absolute reduction in daily AF burden or for every 0.69% (95% CI, 0.34-1.03; P < .001) relative reduction in AF burden from baseline.
Among patients with a symptomatic recurrence, a significant association was observed between change in AFEQT score and the absolute and relative AF burden. At 12 months, a 1-point improvement in AFEQT score was observed for every 39.7-minute (95% CI, 12.3-67.1; P = .005) absolute reduction in daily AF burden or for every 1.34% (95% CI, 0.59-2.09; P = .001) relative reduction in AF burden from baseline. This association was not observed in those without symptomatic recurrences. Randomized ablation technology did not impact the association between burden and quality of life.
Discussion
In this study, we demonstrated that a postablation reduction in AF burden was associated with an increase in the disease-specific AFEQT quality-of-life score. While traditional outcome parameters, such as freedom from 30 seconds of atrial tachyarrhythmia (eg, arrhythmia elimination), remain the focus of comparative treatment evaluations, patients often report improvements in quality of life in association with significant reductions in the frequency of arrhythmias.7 Limited data using noninvasive intermittent monitoring suggest that patients may experience improved quality of life despite the presence of 4 hours or more of recurrent AF per month.7,8,9 Thus, from a patient’s perspective, symptomatic improvement may be considered a procedural success even if it is not associated with complete elimination of AF. Considering AF as a binary outcome negates the complexity of the patient experience.
Dose-response relationships between atrial tachycardia burden and symptoms, heart failure, and stroke have been suggested in prior studies.7,9,13 Previous studies have suggested that quality of life may be improved with relative reductions in AF burden ranging from 78% to more than 99%; however, these studies used intermittent noninvasive monitoring, which is unreliable in estimating the true AF burden (high variability, low accuracy, low precision, and high uncertainty).14 In contrast, the continuous rhythm monitoring used in the CIRCA-DOSE study provided a unique opportunity to comprehensively assess the dose-response association between AF burden and quality of life.
Based on the current analysis, an approximate 7.9% relative reduction in AF burden exceeds the established minimal clinically important difference in AFEQT score (5 points), with a 30.2% relative reduction meeting the threshold for a meaningful improvement in AFEQT score (19 points).2,4 These improvements were tied to symptom status, with no association being observed in asymptomatic patients, even in the presence of documented recurrence. These findings reinforce the notion that catheter ablation is an effective treatment option to meaningfully improve quality of life.
Further, a 24% to 31% reduction in AF burden after ablation has been demonstrated among patients with a high preablation AF burden (mean, 51%) in the CASTLE-AF trial.15 Thus, ablation may also result in a clinically meaningful improvement in quality of life in patients with greater AF burden; however, additional studies are warranted.
Limitations
This study had limitations. Baseline quality of life was assessed between ICM implantation and catheter ablation, which was necessarily shorter preablation (median, 2.5 months) compared with postablation. While we inferred that the AF burden over this interval was representative of the period prior to ICM implantation, as paroxysmal AF is a disease of clusters, it is possible that the AF burden prior to ICM implantation may have differed. Assessment of quality of life was limited to participants who completed the questionnaires. Nevertheless, the participation rate was 99% at baseline and 94% at 12 months, suggesting that missing data are unlikely to influence the results. As all patients underwent catheter ablation, improvement in quality of life may be partially related to treatment expectancy. However, the median postablation improvement in AFEQT score was comparable with that observed in the Catheter Ablation vs Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) trial.10 Further, the generalizability of results should be limited to patients with characteristics similar to the study population, ie, relatively young with predominantly paroxysmal AF, few comorbidities, low CHA2DS2-VASc score (congestive heart failure, hypertension, age of 75 years or older [doubled], diabetes, stroke/transient ischemic attack/thromboembolism [doubled], vascular disease [prior myocardial infarction, peripheral artery disease, or aortic plaque], age 65 of 75 years, sex category [female]), and low AF burden. Additionally, we had limited power for subgroup analyses.
Conclusions
In patients with primarily low-burden paroxysmal AF, the reduction in AF burden following catheter ablation may be associated with a significant increase in AFEQT score in a dose-response manner. A 30% relative reduction in AF burden from baseline, an outcome often achieved by catheter ablation, was associated with a clinically meaningful improvement in quality of life.
Trial protocol.
Data sharing statement.
References
- 1.Andrade J, Khairy P, Dobrev D, Nattel S. The clinical profile and pathophysiology of atrial fibrillation: relationships among clinical features, epidemiology, and mechanisms. Circ Res. 2014;114(9):1453-1468. doi: 10.1161/CIRCRESAHA.114.303211 [DOI] [PubMed] [Google Scholar]
- 2.Dorian P, Burk C, Mullin CM, et al. Interpreting changes in quality of life in atrial fibrillation: how much change is meaningful? Am Heart J. 2013;166(2):381-387.e8. [DOI] [PubMed] [Google Scholar]
- 3.Andrade JG, Macle L, Verma A, et al. ; CIRCA-DOSE Study Investigators . Quality of life and health care utilization in the CIRCA-DOSE study. JACC Clin Electrophysiol. 2020;6(8):935-944. doi: 10.1016/j.jacep.2020.04.017 [DOI] [PubMed] [Google Scholar]
- 4.Holmes DN, Piccini JP, Allen LA, et al. Defining clinically important difference in the Atrial Fibrillation Effect on Quality-of-Life score. Circ Cardiovasc Qual Outcomes. 2019;12(5):e005358. doi: 10.1161/CIRCOUTCOMES.118.005358 [DOI] [PubMed] [Google Scholar]
- 5.Andrade JG, Champagne J, Dubuc M, et al. ; CIRCA-DOSE Study Investigators . Cryoballoon or radiofrequency ablation for atrial fibrillation assessed by continuous monitoring: a randomized clinical trial. Circulation. 2019;140(22):1779-1788. doi: 10.1161/CIRCULATIONAHA.119.042622 [DOI] [PubMed] [Google Scholar]
- 6.Packer DL, Mark DB, Robb RA, et al. ; CABANA Investigators . Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. 2019;321(13):1261-1274. doi: 10.1001/jama.2019.0693 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Marrouche NF, Brachmann J, Andresen D, et al. ; CASTLE-AF Investigators . Catheter ablation for atrial fibrillation with heart failure. N Engl J Med. 2018;378(5):417-427. doi: 10.1056/NEJMoa1707855 [DOI] [PubMed] [Google Scholar]
- 8.Kochhäuser S, Joza J, Essebag V, et al. The impact of duration of atrial fibrillation recurrences on measures of health-related quality of life and symptoms. Pacing Clin Electrophysiol. 2016;39(2):166-172. doi: 10.1111/pace.12772 [DOI] [PubMed] [Google Scholar]
- 9.Mantovan R, Macle L, De Martino G, et al. Relationship of quality of life with procedural success of atrial fibrillation (AF) ablation and postablation AF burden: substudy of the STAR AF randomized trial. Can J Cardiol. 2013;29(10):1211-1217. doi: 10.1016/j.cjca.2013.06.006 [DOI] [PubMed] [Google Scholar]
- 10.Mark DB, Anstrom KJ, Sheng S, et al. ; CABANA Investigators . Effect of catheter ablation vs medical therapy on quality of life among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. 2019;321(13):1275-1285. doi: 10.1001/jama.2019.0692 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ziegler PD, Koehler JL, Mehra R. Comparison of continuous versus intermittent monitoring of atrial arrhythmias. Heart Rhythm. 2006;3(12):1445-1452. doi: 10.1016/j.hrthm.2006.07.030 [DOI] [PubMed] [Google Scholar]
- 12.Andrade JG, Deyell MW, Badra M, et al. Randomised clinical trial of cryoballoon versus irrigated radio frequency catheter ablation for atrial fibrillation—the effect of double short versus standard exposure cryoablation duration during pulmonary vein isolation (CIRCA-DOSE): methods and rationale. BMJ Open. 2017;7(10):e017970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Go AS, Reynolds K, Yang J, et al. Association of burden of atrial fibrillation with risk of ischemic stroke in adults with paroxysmal atrial fibrillation: the KP-RHYTHM study. JAMA Cardiol. 2018;3(7):601-608. doi: 10.1001/jamacardio.2018.1176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Charitos EI, Ziegler PD, Stierle U, et al. Atrial fibrillation burden estimates derived from intermittent rhythm monitoring are unreliable estimates of the true atrial fibrillation burden. Pacing Clin Electrophysiol. 2014;37(9):1210-1218. doi: 10.1111/pace.12389 [DOI] [PubMed] [Google Scholar]
- 15.Brachmann J, Sohns C, Andresen D, et al. Atrial fibrillation burden and clinical outcomes in heart failure: the CASTLE-AF trial. JACC Clin Electrophysiol. 2021;7(5):594-603. doi: 10.1016/j.jacep.2020.11.021 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial protocol.
Data sharing statement.