

Abstract
Laser-assisted in situ keratomileusis (LASIK) is one of the most commonly performed kerato-refractive surgery globally. Since its introduction in 1990, there has been a constant evolution in its technology to improve the visual outcome. The safety, efficacy, and predictability of LASIK are well known, but complications with this procedure, although rare, are not unknown. Literature review suggests that intraoperative complications include suction loss, free cap, flap tear, buttonhole flap, decentered ablation, central island, interface debris, femtosecond laser-related complications, and others. The postoperative complications include flap striae, flap dislocation, residual refractive error, diffuse lamellar keratitis, microbial keratitis, epithelial ingrowth, refractive regression, corneal ectasia, and others. This review aims to provide a comprehensive knowledge of risk factors, clinical features, and management protocol of all the reported complications of LASIK. This knowledge will help in prevention as well as early identification and timely intervention with the appropriate strategy for achieving optimal visual outcome even in the face of complications.
Keywords: Diffuse lamellar keratitis, epithelial ingrowth, flap-related complications, laser in-situ keratomileusis, laser vision correction, LASIK; refractive surgery, LASIK complications
The field of refractive surgery has witnessed a major revolution in the past two decades with the introduction of phakic intraocular lens and small incision lenticule extraction. But laser-assisted in situ keratomileusis (LASIK) still remains the most commonly performed refractive surgery world over. In the current era, a postoperative visual acuity (VA) of <20/20 following refractive surgery has become unacceptable considering the high demands of patients and the fact that most patients have a best spectacle-corrected visual acuity of (BSCVA) of 20/20 before surgery. The technological advances in LASIK, ever since its introduction has increased its safety, efficacy, and predictability. However, one needs an in-depth knowledge of its intraoperative and postoperative complications. This will help surgeons take preventive measures to reduce its occurrence, early identification, and appropriate management for achieving an optimal outcome.
In this review, we aim to highlight the risk factors, clinical presentation, management, and prevention of various intraoperative and postoperative complications of LASIK [Fig. 1].
Figure 1.

Flowchart showing the various complications of LASIK
Methods
A literature search was performed using PubMed, Medline, Cochrane Library Database, EMBASE, and Scopus (1960 onwards), using the terms: Laser In-Situ Keratomileusis, LASIK, Complications of LASIK, Flap related complications, decentered ablation, Complications of FS LASIK, Diffuse lamellar keratitis, Post-LASIK Keratitis, Post-LASIK ectasia, Pressure-induced stromal keratitis, Post-LASIK Epithelial ingrowth, Post-LASIK Refractive regression and Visual outcome in LASIK. A total of 6249 articles matched our search strategy, of which 98 articles were selected by three experts (JR, RBV, and NS) and included in this review. Preference was given to meta-analysis, randomized control trials, and systematic review articles over case series and case reports.
Intraoperative Complications
Subconjunctival hemorrhage
A subconjunctival hemorrhage occurs in nearly one-third of cases.[1] [Fig. 2a] Risk factors include decentered or inappropriate size suction ring and large/decentered flap in cases with corneal pannus.[2] Pressure application with meroceal sponge helps to control the bleed. In case blood reaches the interface, it should be thoroughly irrigated before excimer laser delivery.[3]
Figure 2.
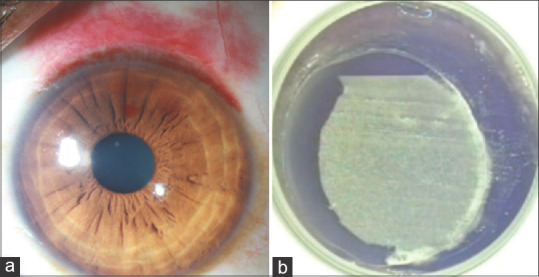
(a) Slit-lamp photograph of the right eye of a patient on day one after femtosecond LASIK showing subconjunctival hemorrhage and interface bleed; (b) Intraoperative image showing a peripheral asymmetric tear meniscus during femtosecond LASIK indicating suction loss resulting in incomplete flap formation
Spontaneous resolution occurs in 1–2 weeks.
Prophylaxis
A gradual, controlled, and well-centered application of suction ring with an average size and well-centered flap reduces its risk. Preoperative instillation of brimonidine or apraclonidine can be useful.[4]
Epithelial defect
An epithelial defect is observed in 0.6%–14% of cases.[2,5,6] Risk factors include epithelial basement membrane dystrophy (EBMD), old age, frequent instillation of topical anesthetic before surgery, active suction during microkeratome reverse pass, hyperopia, drying of the flap and iatrogenic trauma with instruments.[6] The shearing forces of the microkeratome blade results in its high incidence after microkeratome LASIK (m-LASIK). An epithelial defect can cause stromal edema and reduced flap adherence, which increases the risk for diffuse lamellar keratitis (DLK) and epithelial ingrowth.[7]
Management includes frequent preservative-free lubricants. Topical steroid is stepped up for 2-3 days to reduce the risk of DLK. In case of large epithelial defect (>3 mm), a bandage contact lens (BCL) is applied.[8]
Prophylaxis
Careful screening for EBMD, preoperative use of lubricants, avoiding excessive instillation of topical anesthetic before surgery, and switching off suction during microkeratome reverse pass can reduce its risk.
Suction loss
Suction loss occurs in 0.06%-4.4% cases.[5,9,10] It can cause incomplete flap formation. [Fig. 2b] Risk factors include narrow palpebral aperture, deep-set eye, flat cornea, improper eye or head position, improper application of suction ring, low suction pressure, and sudden eye movement.[2,10] In m-LASIK, suction loss is indicated by machine alarm, following which further forward movement of microkeratome is stopped. If the flap is larger than the intended optical zone (OZ), ablation can be performed; however, if the hinge is in the ablation zone, then the procedure is aborted, and re-treatment is planned, preferably surface ablation after three months.[5] In FS-LASIK, a peripheral asymmetric tear meniscus around the patient interface is the first sign of suction loss following which laser delivery is stopped.[11] A second attempt for docking while maintaining centration over the previous flap can be attempted.[11] In case the suction loss occurs before the sidecut, the same parameters are used; however, if it occurs during the sidecut, the second side cut diameter should be 0.5 mm smaller.[11]
Prophylaxis
Careful screening for risk factors and preoperative counseling to remain calm and maintain fixation is essential. Proper functioning microkeratome, draping of the eye to avoid lashes in the surgical field, and adequate suction pressure reduces its risk.
Flap-related complications
-
i. Decentered Flap
Misaligned suction ring can result in a decentered flap.[12] In case a decentered flap is formed, performing a pupil-centered ablation can result in an unexpected visual outcome.[12] Hence, the procedure should be aborted if the expected gap between the peripheral edge of ablation and flap margin is <1 mm, and a repeat procedure is performed after three months.[12]
Prophylaxis
If there is a misaligned suction ring, the suction should be turned off, and the suction ring should be repositioned. In cases with repeated unsuccessful attempts, waiting for 5-10 minutes helps by allowing the decentered gutter-like impression to disappear.
-
ii. Incomplete/Partial Flap
An incomplete flap occurs in 0.3% to 3.6% cases with a higher incidence in m-LASIK.[5,13] [Fig. 2b] The risk factors include suction loss, malfunctioning microkeratome, mechanical block with drape, eyelash, loose epithelium, or crystallized salt.[13,14] Management is the same as for suction loss.[15] Lamellar dissectors have been described to complete the flap in case the hinge lies in the optical zone. However, this adds the risk of buttonhole and uneven stromal bed, causing irregular astigmatism. Also, the OZ can be reduced to protect the flap, but the scotopic pupil size should be given due consideration.
Prophylaxis
Same measures as for suction loss
-
iii. Flap Tear
Flap tear, although rare, can occur during flap lift and is more common in FS-LASIK.[5,16] [Fig. 3a] Large diameter flap with corneal pannus, re-treatment procedure, presence of a corneal scar, and faulty instrumentation can result in this complication.[17] Flap tears at the hinge can result in a free cap. In case of small peripheral tear, the flap should be dissected away from the tear. However, if it involves the visual axis, the procedure should be aborted and followed by re-treatment with surface ablation.
Figure 3.
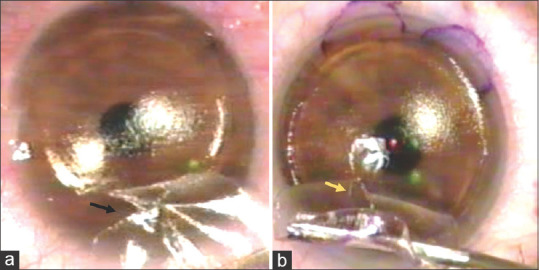
Intraoperative image showing (a) a peripheral flap tear (black arrow); (b) a buttonhole flap (yellow arrow)
Prophylaxis
Reducing the flap diameter in presence of corneal pannus and a careful dissection of the flap, especially in FS-LASIK, can reduce the risk.
-
iv. Buttonhole Flap
The failure to achieve a lamellar cut results in a hole in the flap. [Fig. 3b] It is observed in 0.03% to 2.6% of cases.[18] Steep cornea (>48 D), suction loss, large flap, second eye, m-LASIK, and vertical gas breakthrough (VGB) in FS-LASIK are the reported risk factors.[18,19] Management includes aborting the procedure and planning for re-treatment, preferably surface ablation after three months.[18,19] In case, LASIK is performed, the flap should be of a larger diameter and greater thickness.[5] Buttonhole flap can result in irregular astigmatism and epithelial ingrowth.
Prophylaxis
Preoperative assessment of risk factors, intraoperative precautions to avoid suction loss and lubrication of the second eye is helpful.[18]
-
v. Free Cap
Free cap is observed in 0.01%-1.8% cases.[14,20] Risk factors include malfunctioning or old model microkeratome, flat cornea (<42D), deep orbit, decentered suction ring, inadequate suction, and small hinge.[20] Also, avulsion at hinge during manipulation can result in a free cap.
If the flap is found intact and the stromal bed is of adequate size (>6.5 mm), the free cap is placed in an anti-desiccation chamber with the epithelial side down and kept moist.[20] After laser ablation, the free cap is placed on the stromal bed, allowed to air dry for > 5 mins, and BCL placed over it to achieve good adherence. 10-0 nylon sutures are used to secure flaps that are edematous or show a tendency to dislocate.[14] A slit-lamp examination after 2-3 hours is recommended. Pre-placed corneal markings help in avoiding rotational misalignment that can cause irregular astigmatism.
In case of intraoperative flap loss, the procedure should be abandoned. The surface heals by epithelization and corneal haze. The postoperative hyperopic shift in these cases is managed with contact lens (CL), PRK, or flap reconstruction with a donor cornea.[20]
Prophylaxis
Regular servicing of microkeratome, avoiding intraoperative drying of the flap and preoperative corneal marking can be useful.
-
vi. Thin flap
The LASIK flap is created by a lamellar cut below the bowman’s layer; however, a cut at or above the bowman’s layer results in a thin flap (<60 microns). The risk factors are similar to those for a free cap. In uniform thickness thin flap with adequate stromal bed (>6.5 mm), the procedure can be continued. However, for irregular thin flap having an inadequate stromal bed, the procedure is aborted, and re-treatment is planned after three months with a deeper cut to obtain a thicker flap.
Prophylaxis
Screening patients for risk factors, proper blade assembly, and adequate suction can reduce this complication.
-
vi. Corneal Perforation
Corneal perforation is a rare and dreaded complication of LASIK. It can occur during flap creation, especially with old microkeratome model that required assembly of the thickness footplate), and excimer laser ablation due to either miscalculation of the residual stromal bed thickness (RSBT) or excessive ablation due to corneal dehydration.[14,21]
If corneal perforation occurs during flap creation, suction should be immediately stopped. Conservative management by repositioning the flap and placing a BCL is done for small perforation; however, large perforation requires surgical repair under sterile conditions. Poor visual outcome due to corneal scar and recurrent epithelial ingrowth occur in these cases.[22]
Prophylaxis
Careful microkeratome assembly, preoperative calculation of RSBT and avoiding intraoperative dehydration of cornea.
Complications peculiar to femtosecond laser-assisted LASIK
-
i. Vertical Gas Breakthrough
Femtosecond laser (FSL) works on the principle of photo-disruption. It creates a plasma that spreads horizontally in the cornea, path of least resistance, as cavitation bubbles. In the presence of corneal scar or break/abnormality in the bowman’s layer, the gas dissects vertically towards the stroma or epithelium following the path of least resistance.[23,24] [Fig. 4a] This results in an incomplete dissection of the flap with a potential site for buttonholing. Rarely, the gas can breach the corneal epithelium resulting in an epithelial defect.[23]
Figure 4.
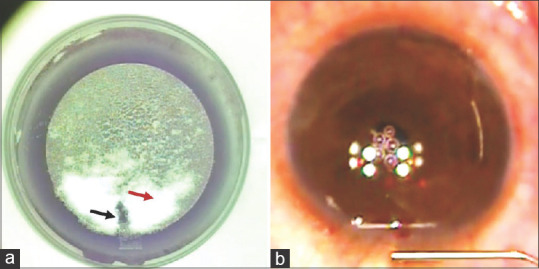
Intraoperative image showing (a) vertical gas breakthrough appearing as a dark patch (black arrow) and opaque bubble layer appearing as white stromal opacification (red arrow); (b) air bubbles in anterior chamber obscuring the pupil
VGB is noted in 0.03% to 0.13% cases.[23,25] If a VGB is observed ahead of the advancing edge of the flap, the procedure should be aborted.[2] However, if a VGB is noted behind the advancing edge of the flap, the procedure can be safely continued.[2]
Prophylaxis
Careful preoperative slit-lamp examination to look for corneal scar or any obvious break in the bowman’s layer.
-
ii. Opaque Bubble Layer
Opaque bubble layer (OBL) forms due to entrapment of gas from cavitation bubbles within the corneal stroma. [Fig. 4a] Variable incidence has been observed in the literature (5%-72.6%).[26,27] Thick cornea, small flap diameter, hard docking technique, corneal hysteresis, use of low laser frequency or energy, and small spot or line separation are the reported risk factors.[26,27]
OBL has been classified into early and late.[28] Early OBL or hard OBL, occurs at the time of laser delivery and appears to be dense. Late OBL or soft OBL, appears after laser delivery has passed through an area and is relatively transparent. The presence of OBL suggests flap adhesion; hence, flap lifting should be performed carefully. It disappears after a flap lift; however, its persistence can cause difficulty in pupil tracking for excimer laser delivery. Waiting for a few minutes and allowing it to disappear is prudent. Increase in higher-order aberration (HOA), especially trefoil, has been observed with occurrence of OBL.[1,2]
Prophylaxis
The use of a soft docking technique with a relatively large diameter flap can reduce its risk.[26,27] Soft docking implicates docking the patient interface just enough to leave a peripheral ring of tear meniscus that allows the dissipation of gas bubbles through the side cut.
-
iii. Anterior Chamber Air Bubbles
The incidence of an air bubble in the anterior chamber (AC) during LASIK is <1%.[29] [Fig. 4b] It occurs due to the migration of cavitation bubbles through the episclera, schlemm canal, and trabecular meshwork into the AC.[30] Large diameter flap and small corneal diameter are the reported risk factors.[2,11]
Bubbles in AC interfere with pupil tracking for excimer laser ablation. Hence, its ideal to wait for it to disappear before proceeding. However, few surgeons prefer to disable automatic tracking and proceed with manual tracking to reduce operating time.[2,11,29,30,31] No adverse effect is seen on the endothelial cell with its occurrence.[31]
Excimer laser ablation relation complication
-
i. Central Island
The central island represents a well-circumscribed area of unablated cornea with a relatively higher corneal power revealed on corneal topography.[32] Power of >3D and size of >1.5 mm is used for its definition, but few authors believe that any area of central steepening should be considered as a central island as it ultimately affects the VA.[14,32,33] Its incidence varies from 5.7% to 11%.[14,34] The risk factors include broad beam laser delivery pattern, non-uniform corneal hydration, or presence of debris on the stromal surface resulting in non-uniform excimer laser delivery.[14,32] Postoperatively, patients complain of glare, halo, ghost images, and monocular diplopia. On examination, VA and contrast sensitivity are reduced due to irregular astigmatism.[35] Corneal topography helps in diagnosis and shows an area of hot color surrounded by cool color in the OZ. As spontaneous regression occurs in 25-80% cases by six months, it is prudent to wait for refraction and corneal topography to stabilize before planning a re-intervention.[35] Wavefront or topography-guided LASIK can be planned for re-treatment; however, the results are unpredictable, considering the corneal contour’s complexity. Rigid gas-permeable (RGP) CL can be used for visual rehabilitation.[36]
Prophylaxis
Use of a scanning slit or flying spot pattern of laser delivery, drying of the stromal surface, and checking for the presence of debris prior to excimer laser delivery can reduce its risk.[32]
-
ii. Decentered Ablation
Corneal ablation centered over the pupil is essential for optimal visual outcome and >0.3 mm deviation compromises the visual outcome.[14] The causes for decentered ablation include poor fixation, sudden involuntary ocular or head movement, and surgeon’s error.[14,33] An inadvertent laser delivery to the stromal side of the flap can cause irregular astigmatism. Postoperatively, patients complain of poor vision, glare, halo, and monocular diplopia due to induced corneal astigmatism. Corneal topography shows asymmetric corneal contour with flattening on one side and steepening on the other. Management options include RGP CL, miotics to reduce optical aberrations, and decentered PRK or wavefront-guided LASIK or topo-guided LASIK for re-treatment.[37]
Prophylaxis
Use of pupil tracking system, dim lighting of the operating room during excimer laser delivery and preoperative counseling besides intraoperative verbal communication with patient to maintain central fixation during the procedure is helpful.
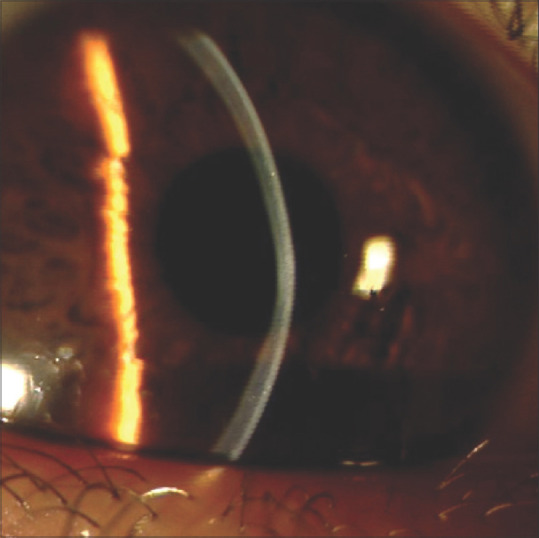
Interface debris
A variable incidence of interface debris has been reported (0.06% to 100%).[38,39] [Fig. 5] It is identified postoperatively on slit-lamp examination and should be carefully differentiated from an inflammatory and infectious reaction. The debris consists of talc from the glove, sponge fiber, metallic particle from microkeratome, meibomian gland secretion, and eyelash.[14] Most debris are biodegradable and does not induce inflammation; hence can be observed. However, if it involves the central visual axis or is suspected of causing inflammation, it is managed with flap lift and irrigation of interface.[39] Diffuse lamellar keratitis (DLK) and irregular astigmatism are its reported complication.[40]
Figure 5.
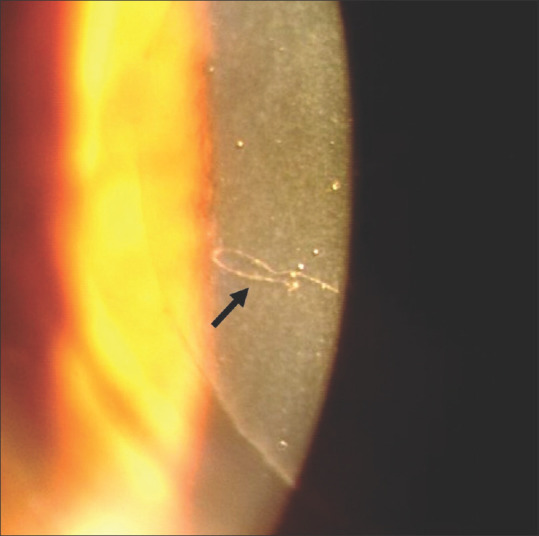
Slit-lamp photograph showing a cotton fiber in the LASIK interface
Prophylaxis
Careful draping of the eye to keep eyelashes and meibomian gland secretions away from the surgical site, use of powder-free gloves, non-fragmenting sponges, and fibrocellulose ring (Chayet ring) that isolates the ablation zone from the surrounding area is helpful.
Postoperative Complications
Early complications
-
i. Flap Dislocation
Flap dislocation is an ocular emergency. Its incidence varies from 0.012% to 2.5%.[5,11,14,41] Most cases present within the first postoperative week, as even minor trauma due to lid squeezing, forceful blinking and rubbing of eyes can dislodge the flap in this phase.[5,41] Dry ocular surface, m-LASIK, nasal hinged flap, large-diameter/thin flap, and hyperopic correction are the other risk factors.[5,11,14,41]
Patients present with sudden onset blurred or decreased vision, which may be associated with pain. Management includes flap lift, debridement of epithelium from stromal bed (if present), irrigation of interface for debris removal, and flap repositioning. The edges are dried meticulously to achieve good adherence, followed by BCL application. In some cases, sutures may be required to realign the flap. Complete visual recovery occurs in cases that present early.[41,42] Secondary complications like DLK, epithelial ingrowth, and interface haze are seen in a few cases.[29,42,43]
Prophylaxis
Preoperative counseling to avoid ocular trauma (squeezing/rubbing/contact sports) after surgery. Intraoperative superior hinge flap, adequate drying of flap edges, and use of BCL. Postoperative counseling to sleep after they return home, and use of protective shield for a week.[11,14]
-
ii. Flap Striae
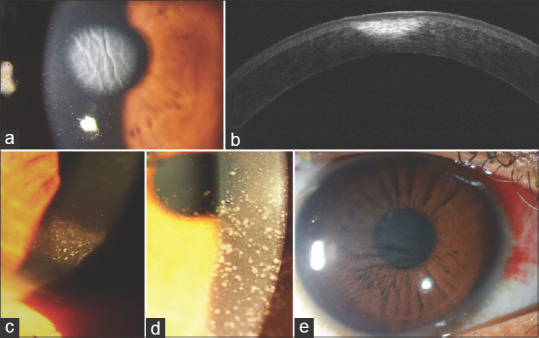
The incidence of flap striae varies from 0.03% to 3.5%.[11,42,44] [Fig. 6] Most cases present within the first few days of LASIK.[11,42,44] Flap striae are classified into micro-striae and macro-striae. Irregularities within flap are referred to as microstriae, while full-thickness flap-folds represent macrostriae. Flap striae involving visual axis affects vision by inducing irregular astigmatism and optical aberrations. They are best appreciated on slit-lamp examination in retro-illumination. Fine striae can be detected using fluorescein under cobalt blue filter as irregularities in the tear film.
Figure 6.
Slit-lamp photograph showing (a) flap striae in the visual axis one week following LASIK; (b) resolution of flap striae after flap lift and ironing out the striae
Risk factors include high refractive error, flap contracture, drying of the flap, misalignment during repositioning, and excessive manipulation of the flap during surgery.[5,11,14] Striae formation in high refractive error results from the “tenting” effect due to contour mismatch of the flap and stromal bed after ablation.[45] Management varies from gentle stroking of the flap with a wet sponge on slit-lamp perpendicular to striae (flap sliding technique) to flap lift and repositioning.[46,47] Fixed folds resulting from epithelial hyperplasia in crevices occur in cases presenting late. Management includes debridement of corneal epithelium from flap and exposed stromal bed along with flap lift, repositioning, and stroking with a sponge. Suturing of the flap is required if folds persist.[14] The visual outcome is good in cases presenting early.
Prophylaxis
Intraoperative careful handling of the flap, keeping it moist, and prior marking of surgical landmarks at its edge to achieve proper alignment during its repositioning is useful. After surgery, slit-lamp examination for flap position and uniformity of peripheral gutter is useful.[8]
-
iii. Residual Refractive Error
Overcorrection & Under-correction
Residual refractive error following LASIK has been reported in 5%-51% cases.[33,48] Inaccurate assessment of refraction or corneal contour change due to CL use, data entry errors in the LASIK machine, and lack of machine calibration can result in this complication. Environmental factors like operating room temperature, humidity, and atmospheric pressure have also been hypothesized to affect the tissue ablation depth. High humidity is presumed to cause stromal hydration and inadequate tissue ablation resulting in under-correction; however, this association is much debated.[49,50]
Management includes LASIK enhancement with flap re-lift, or PRK.[48,51] The visual outcome is comparable in both; however, epithelial ingrowth can occur in LASIK flap re-lift.[48,51]
Prophylaxis
Soft CL should be discontinued >2 weeks and RGP CL >4 weeks before refractive workup. Cycloplegic refraction should be performed in all cases.
Residual and Induced Astigmatism
In addition to the risk factors for over and under-correction, cyclotorsion from erect to supine position and poor centration of eye during laser ablation can cause postoperative astigmatism.[52,53] Management involves post-LASIK enhancement.
Prophylaxis
Pupil tracking and iris pattern registration (wavefront-guided LASIK) for torsion compensation reduces the risk of postoperative residual and induced astigmatism.[53,54] Preoperative manual limbal marking of cardinal meridians and intraoperative cyclotorsion adjustment can also be done.[53]
-
iv. Dry Eye
Dry eye disease (DED) is observed in >90% cases in the immediate postoperative period; however, symptoms are mostly transient.[55] The causes include pre-existing DED, peri-limbal goblet cell damage during suction, sub-basal nerve plexus and stromal nerve damage during flap creation, and postoperative inflammation.[14] Superior hinged flap is at greater risk as the long ciliary nerves enter at 3 and 9 O’ clock position; however, variable results have been observed.[56,57] Improvement in corneal sensation and DED by 3-6 months occur in most cases, but corneal re-innervation is delayed by 2-5 years.[58] Management includes lubricant drops for 3-6 months, topical cyclosporine, and slow tapering of topical steroids.[59] Temporary punctal plugs are considered in cases with severe DED.
Prophylaxis
Careful screening of patients for DED before surgery.
-
v. Central Toxic Keratopathy
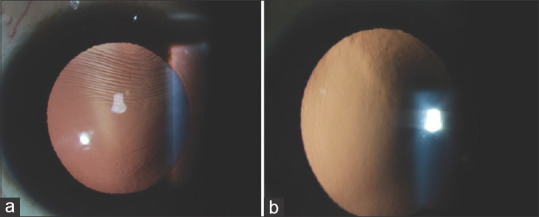
Central toxic keratopathy (CTK) is a rare complication observed in 0.2%-0.77% of cases.[60] [Fig. 7a and b] The pathogenesis of CTK is controversial; however, meibomian gland secretion, marking ink, and talc from glove are the reported inciting factors. Patients present with pain, redness, photophobia, glare, and halo between day 2 to day 6.[61] Clinical examination reveals central corneal opacification, hyperopic shift (3-6D), and corneal thinning, which progresses over one week followed by a stable phase for 2-3 months and recovery phase of 3-18 months wherein hyperopia decreases (1-3D) and corneal thickness increases.[60] Non-inflammatory stromal keratocyte apoptosis and enzymatic lysis of the stroma resulting in corneal thinning is the presumed cause for hyperopic shift.[62] DLK and microbial keratitis are the differential diagnosis.
Figure 7.
(a) Slit-lamp photograph showing central circumscribed scarring with striae suggestive of central toxic keratopathy; (b) ASOCT showing an inverse dome-shaped homogenous hyperreflectivity; Slit-lamp photograph showing (c) inflammatory cells extending from periphery suggestive of diffuse lamellar keratitis (DLK) stage 1; (d) central involvement of inflammatory cells with “sands of Sahara appearance” suggestive of DLK; (e) both peripheral and central involvement of inflammatory cells suggestive of DLK stage 2
Spontaneous regression occurs in most cases.[60] CTK is a non-inflammatory condition, and hence steroids are not indicated. On the contrary, it may hamper the healing process.
Prophylaxis
Use of powder-free gloves and proper draping to cover lid margins should be done.
-
vi. Diffuse Lamellar Keratitis
DLK is a non-infectious inflammatory condition that involves the LASIK interface in 0.13% to 18.9% of cases.[63,64] [Fig. 7c-e] Risk factors include glove talc, marking pen, old microkeratome blade, small suction ring, high energy FSL, large-diameter flap, chemical toxin and bacterial endotoxin on instruments, and meibomian gland secretions.[33,40,65,66] DLK presents within 24-48 hours of surgery with peripheral granular cells in the interface, which progresses to involve both the center and periphery (sands of Sahara). Linebarger et al. described stages of DLK to facilitate timely and appropriate intervention.[66] [Table 1]
Table 1.
Diffuse lamellar keratitis- Staging and management (Lenberger et al.)[66]
| Stage | Clinical feature | Visual acuity | Management |
|---|---|---|---|
| 1 | Peripheral white granular cells in the interface | Not affected | Aggressive topical steroids |
| 2 | Both central and peripheral white granular cells “sands of Sahara” | May be affected | Aggressive topical steroids |
| 3 | Aggregation of dense white clumped cells involving the visual axis with clearing of the periphery | Decreased by 1-2 lines | Aggressive topical steroids + Flap lift with irrigation of interface |
| 4 | Severe lamellar keratitis with stromal melting, fluid collection in central lamellae, overlying epithelial bullae. | Severely affected | - |
Stage 1 and 2 are managed with intensive topical steroid.[66] Follow-up at 24-48 hrs helps in early identification of cases progressing to Stage 3. Early flap lift and irrigation of interface with intensive topical steroids in stage 3 reduces the risk of progression to stage 4. There is no benefit of any intervention in stage 4.[40,66] Microbial keratitis and CTK are the differential diagnosis.
Prophylaxis
Preoperative screening and management of OSD and intraoperative use of powder-free gloves, drapes to cover lid margin, avoiding tear film debris from reaching the interface, and irrigating the interface after flap repositioning is useful. Topical steroids should be judiciously used postoperatively.[40] The used instruments should be cleaned and sterilization immediately after the procedure.
-
vii. Pressure-Induced Stromal Keratitis
Pressure-induced stroma keratitis (PISK) is also known as pressure induced interface keratitis, interface fluid syndrome, and pressure induced stromal keratopathy.[67] It is often misdiagnosed as DLK, but unlike DLK, it presents >1 week after surgery with high IOP, shows a poor response to steroids, good response to anti-glaucoma drugs, and absence of inflammatory cells in the interface.[68]
Patients present with poor vision and pain.[69] Interface haze is noted in mild cases, while severe cases have fluid clefts in the interface. Elevated IOP secondary to steroid response is the presumed cause for fluid accumulation. Dynamic contour tonometry and tonopen (reading from the peripheral cornea) are superior to Goldmann applanation tonometry in these cases for IOP measurement. Management includes anti-glaucoma medication and cessation of steroids to avoid glaucomatous optic neuropathy.[68,69]
-
viii. Interface Haze
Interface haze is rarely seen following LASIK. DLK, ultra-thin flap (<90 mm), and young age are the reported risk factors.[70] Most cases respond well to topical steroids in the early phase with good visual recovery.[70]
ix. Higher-Order Aberrations
Optical aberrations are observed in 2.3%-43.5% of cases.[71,72] Symptoms include glare, halo, difficulty in night vision, and blurred vision despite good VA. Most cases adapt to these symptoms in a few months, but it may be visually incapacitating for few. The risk factors include large mesopic pupil diameter (>6 mm), small OZ, decentered ablation, central island, flap striae, postoperative residual refractive error, and DED.[14,73,74] Light rays passing from the peripheral untreated cornea results in blur circles and affects vision quality. The optical aberrations are measured using the wavefront or ray tracing aberrometers.
Decreasing the pupil size with topical miotics or brimonidine, use of tinted CL with an artificial pupil and, topography/wavefront-guided enlargement of OZ are the treatment options.[14,75] The use of tear supplements or punctal plugs benefits patients with DED.
Prophylaxis
Screen for mesopic pupil diameter >6 mm and avoid LASIK in these cases.[73] A large OZ can be targeted if surgery is planned. Also, a wavefront-guided LASIK shows better results in cases with high preoperative HOA.[76]
-
x. Reduced Contrast Sensitivity
Contrast sensitivity (CS) better assesses functional VA, especially in patients complaining of poor vision quality despite 20/20 VA. Literature shows variable effect of LASIK on CS.[77] However, majority suggests an initial decrease in CS for 1-2 months, followed by complete recovery by 3-6 months.[3,78] The CS is more affected in cases with high refractive error, m-LASIK, and high postoperative HOA.[77,78] Wavefront-guided LASIK results in better CS.[76]
xi. Microbial Keratitis
Microbial keratitis is a rare sight-threatening complication observed in 0.005%-0.034% cases with decreased incidence over the years.[79,80,81] [Fig. 8] Based on onset, it is classified as early (<2 weeks) and late (2 weeks-3 months).[80] Bacteria, predominantly Staphylococcus, is noted in early infections while atypical mycobacteria, Nocardia, and fungus in late infections.[80,81] The risk factors include DED, blepharitis, immunocompromised state, contamination of surgical instruments or surroundings, intraoperative epithelial defect, use of CL, re-treatment, and trauma.[81] Patients present with blurred vision, photophobia, redness, and pain. Clinical examination reveals focal infiltrate confined to the interface that later spreads to the flap and underlying stroma. Differential diagnosis includes DLK and CTK. [Table 2]
Figure 8.
Slit-lamp photograph showing (a) central corneal infiltrate in the interface three weeks following LASIK suggestive of microbial keratitis; (b) signs of resolution of keratitis with residual corneal scarring after flap amputation and three months of anti-fungal therapy given based on the microbiological report that showed filamentous fungi
Table 2.
Differentiating Features Between Post-LASIK Microbial Keratitis and Diffuse Lamellar Keratitis
| Post-LASIK Microbial Keratitis | Diffuse Lamellar Keratitis | |
|---|---|---|
| Etiology | S. epidermidis, S. aureus, S. pneumonia, atypical mycobacteria, Fungi, Nocardia | Sterile inflammation |
| Onset | >2-3 days after surgery | <24 hours after surgery |
| Symptoms | Moderate-severe pain & photophobia | Mild pain and photophobia |
| Lid edema | Moderate-severe | Mild |
| Conjunctival congestion | Moderate-severe | Mild |
| Location of infiltrate | Interface (later involves the flap & stroma) | Confined to the interface, begins in the flap periphery |
| Appearance | Focal area of infiltration surrounded by diffuse inflammation | Interface inflammation initially involving the periphery and later both center and periphery “Sands of Sahara” appearance |
| Anterior chamber reaction | Present | Absent |
Management includes flap lift, scraping of bed, and irrigation of bed with antibiotics (vancomycin for early-onset and amikacin for late-onset). Other than routine stain and culture media, Ziehl-Neelsen stain and Lowenstein-Jensen media should be used to identify Mycobacteria and Nocardia. Topical fourth generation fluoroquinolone and vancomycin 5% are prescribed for early-onset infections while amikacin 2% and vancomycin 5% or topical clarithromycin and 4th generation fluoroquinolone for late-onset.[80,81] Besides, oral Doxycycline (100 mg BD) is used to reduce stromal collagenolysis. Steroids are discontinued.[80,81] Treatment should be reviewed following the availability of culture and sensitivity reports. In severe keratitis, flap amputation is needed for both diagnostic and therapeutic purposes.
Prophylaxis
Preoperative screening and treatment of OSD. Use of sterile gown, mask, cap, and gloves by surgeon and assistant. Proper sterilization of instruments, betadine preparation of lid, and eye and use of separate instruments for both eyes reduce its risk.[80]
-
xii. Transient light sensitivity syndrome
Transient light sensitivity syndrome (TLSS) is a complication peculiar to FS-LASIK seen in 1.1%-1.3% cases.[82] Patients present with good VA and photosensitivity without any signs of inflammation at 4-6 weeks.[82,83] The use of FSL causes more inflammation, and this is hypothesized as the cause of TLSS.[82,83] Topical steroids are used for management. Also, topical cyclosporine has shown good results.[82]
Prophylaxis
Reducing laser parameters (by 20-30%) and increasing postoperative steroid treatment has shown to reduce the occurrence of TLSS.[82,83]
Late complications
-
i. Regression
Refractive regression, defined as >0.25D shift in refractive error, is observed in nearly 30% hyperopes and 5.5%–27.7% myopes.[84] Risk factors include high refractive error, low RSBT, old age, chronic DED, m-LASIK, and small OZ.[84,85] Compensatory epithelial hyperplasia, decreased flap thickness, an anterior shift of cornea, stromal remodeling, and lenticular nuclear sclerosis are hypothesized to result in refractive regression.[84,85]
Management includes IOP lowering agents like timolol that reduces anterior shift of cornea.[86] However, the effect is temporary and reverts on cessation of treatment. Surgical treatment options include LASIK enhancement, PRK, and laser-assisted sub-epithelial keratomileusis (LASEK).[84] Careful RSBT calculation is essential in these cases to avoid corneal ectasia.
Prophylaxis
Corneal collagen cross-linking (CXL) performed with LASIK has shown to reduce the risk of regression.[87] However, these results need further validation.
-
ii. Epithelial Ingrowth
Epithelial ingrowth occurs in 0%-3.9% of cases undergoing primary treatment and 10%-20% in re-treatment cases.[88] [Fig. 9] Majority present within four weeks; however, a delayed presentation (upto ten years) is not unusual.[88] Pathogenesis involves implantation of epithelial cells in interface during surgery or later migration from flap edge. Risk factors include EBMD or recurrent erosion syndrome (RES), hyperopia, greater ablation depth, m-LASIK, small OZ, re-treatment, flap fold/dislocation.[88] Intraoperative faulty instrument handling, fluid from periphery reaching interface and epithelial defect adds to the risk. Probst and Machat suggested a grading system for epithelial ingrowth to guide its management.[88] [Table 3] Presence of epithelial pearls and fibrotic demarcation line in the interface and flap melting are signs of epithelial ingrowth.[88,89] Patients present with foreign body sensation and glare in early stages, and diminution of vision in later stages.
Figure 9.
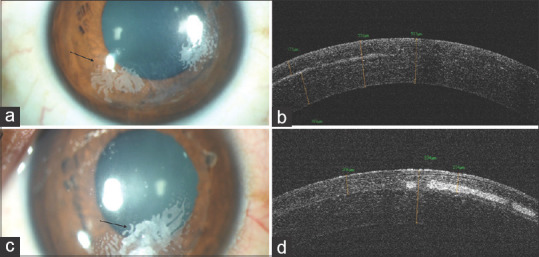
Slit-lamp photograph of (a) the right eye two years after LASIK showing white opacity extending up to 2 mm inside from the flap edge suggestive of grade 2 epithelial ingrowth; (b) ASOCT image of the same eye showing increased flap thickness with interface hyperreflectivity; (c) the left eye with white opacity extending beyond 2 mm of the flap edge suggestive of grade 3 epithelial ingrowth; (d) ASOCT image of the same eye showing increased flap thickness with interface hyperreflectivity
Table 3.
Grading and Management of Epithelial Ingrowth (Probst and Machat grading)[88]
| Grade | Signs | Location | Progression | Treatment |
|---|---|---|---|---|
| 1 | 1-2 cell thick fine growth with a white demarcated line along progressing edge; Difficult to identify on slit-lamp examination | Within 2 mm of the flap edge | No | Not required |
| 2 | Thick growth showing discrete cells in the epithelial nest with no demarcation line; Flap edge may be rolled or grey in appearance | Within 2 mm of the flap edge | Yes | Required within 2-3 weeks |
| 3 | Several cells thick opaque ingrowth with no demarcation line; The flap may be rolled with whitish-grey appearance; Peripheral confluent haze at the flap edge | >2 mm from flap edge | Yes | Urgently required |
| 4 | Aggressive growth with epithelial cells advancing towards the visual axis; Flap melt may be present | Threatening/involving visual axis | Yes | Urgently required |
Management includes observation for grade 1 and flap lift with mechanical debridement of epithelial ingrowth form interface and flap undersurface in grade 2-4.[88,89] Also, mitomycin-C 0.02% application on the interface, fibrin glue application at flap edge, BCL placement, and flap suturing prevents its recurrence, which occurs in one-third cases.[88,90] Recently, low energy (0.6 mJ) Nd-YAG laser has been used for management in few cases.[88,91]
Prophylaxis
Careful surgical approach avoiding intraoperative implantation of epithelial cells in the interface and achieving perfect flap apposition without any folds (especially near flap edge) reduces its risk.
-
iii. Corneal Ectasia
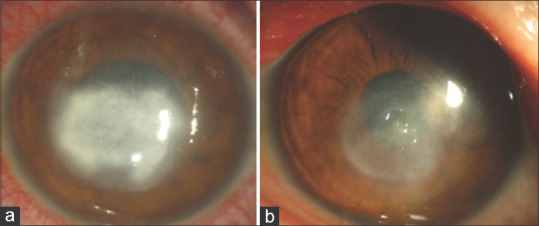
Post-LASIK corneal ectasia is a serious complication seen in 0.033%-0.6% cases.[14,92] [Fig. 10] The use of advanced topography devices and screening criteria like Randleman ectasia risk scoring system and percent tissue altered has reduced its incidence.[92,93] The risk factors include young age, high myopia, thin cornea, low RSBT, abnormal corneal topography, forme-fruste keratoconus, pregnancy, ocular allergy, and eye rubbing.[94] The onset varies from 1 week to several years. Patients present with diminution of vision and refraction shows progressive myopia with astigmatism. The topographic difference map on serial follow-up is instrumental in its diagnosis.
Figure 10.
Slit-lamp photograph showing LASIK flap, steep corneal contour with central corneal thinning suggestive of post-LASIK corneal ectasia
CXL is performed in cases with progressive ectasia.[95] Visual rehabilitation is achieved with spectacles, RGP CL, or intra-corneal ring segments. Advanced cases require anterior lamellar keratoplasty.
Prophylaxis
Stringent screening criteria for corneal topography reduces its risk.[92,93]
-
iv. Posterior Segment Complications
Posterior segment complications are rare following LASIK. It include rhegmatogenous retinal detachment (0.03% - 0.25%), choroidal neovascular membrane (0.1% - 0.33%), macular hole (0.03%), retinal hemorrhage and endophthalmitis.[96] The presence of myopia and sudden compression-decompression of the globe during suction application (60-100 mm of Hg) can result in various posterior segment complications.[96]
Prophylaxis
Careful preoperative fundus screening with appropriate management of treatable retinal lesions and counseling of patients with moderate-high myopia for annual fundus evaluation can reduce its risk.
-
v. Loss of Best Spectacle Corrected Visual Acuity
Loss of BSCVA occurs in 0.3%–4.8% of cases.[97] Most of the above-discussed complications result in loss of BSCVA if not managed in time. The highest incidence is seen in high myopes.[97,98] Development of cataract and myopic maculopathy are the other causes for its occurrence.
Conclusion
Various complications can occur with LASIK. However, the rarity of its occurrence results in non-familiarity of most of the ophthalmologist with these conditions. In-depth knowledge of the complications can help reduce its occurrence, and early identification with appropriate treatment in time can save these eyes from vision loss. Also, reporting complications is necessary as it is the only way to learn and improvise the surgical technique to reduce its occurrence in the future.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Dada T, Sharma N, Vaypayee RB, Dada VK. Subconjuctival hemorrhages after LASIK. Laser in situ keratomileusis. J Cataract Refract Surg. 2000;26:1570 T. doi: 10.1016/s0886-3350(00)00725-2. [DOI] [PubMed] [Google Scholar]
- 2.Tse SM, Farley ND, Tomasko KR, Amin SR. Intraoperative LASIK Complications. Int Ophthalmol Clin. 2016;56:47e SM. doi: 10.1097/IIO.0000000000000110. [DOI] [PubMed] [Google Scholar]
- 3.P rez-Santonja JJ, Sakla HF, Ali JL. Contrast sensitivity after laser in situ keratomileusis. J Cataract Refract Surg. 1998;24:183San. doi: 10.1016/s0886-3350(98)80198-3. [DOI] [PubMed] [Google Scholar]
- 4.Rodrodronja JJ, Sakla HF, Ali JL. Contrast sensitivity after laser in situ keratomileusis. J Cataract Refract Surg 1998;24fract Surg 2he correction of myopia: A contralateral eye study. J Refract Surg. 2010;26:28tral. doi: 10.1016/s0886-3350(98)80198-3. [DOI] [PubMed] [Google Scholar]
- 5.Moshirfar M, Gardiner JP, Schliesser JA, Espandar L, Feiz V, Mifflin MD, et al. Laser in situ keratomileusis flap complications using mechanical microkeratome versus femtosecond laser:Retrospective comparison. J Cataract Refract Surg. 2010;36:1925riso. doi: 10.1016/j.jcrs.2010.05.027. [DOI] [PubMed] [Google Scholar]
- 6.Randleman JB, Lynn MJ, Banning CS, Stulting RD. Risk factors for epithelial defect formation during laser in situ keratomileusis. J Cataract Refract Surg. 2007;33:1738lema. doi: 10.1016/j.jcrs.2007.05.038. [DOI] [PubMed] [Google Scholar]
- 7.Shah MN, Misra M, Wihelmus KR, Koch DD. Diffuse lamellar keratitis associated with epithelial defects after laser in situ keratomileusis. J Cataract Refract Surg. 2000;26:1312 MN. doi: 10.1016/s0886-3350(00)00570-8. [DOI] [PubMed] [Google Scholar]
- 8.Smirennaia E, Sheludchenko V, Kourenkova N, Kashnikova O. Management of corneal epithelial defects following laser in situ keratomileusis. J Refract Surg. 2001;17(2 Suppl):S196–9. doi: 10.3928/1081-597X-20010302-09. [DOI] [PubMed] [Google Scholar]
- 9.Rosman M, Hall RC, Chan C, Ang A, Koh J, Htoon HM, et al. Comparison of efficacy and safety of laser in situ keratomileusis using 2 femtosecond laser platforms in contralateral eyes. J Cataract Refract Surg. 2013;39:1066pari. doi: 10.1016/j.jcrs.2013.02.038. [DOI] [PubMed] [Google Scholar]
- 10.Haft P, Yoo SH, Kymionis GD, Ide T. OT, Oer in situ keratomileusis using 2 femtosecond laser platforms in contralateral eyes. J Cataract Refract Sur J Refract Surg. 2009;25:979t P. [Google Scholar]
- 11.Shah DN, Melki S. Complications of femtosecond-assisted laser in-situ keratomileusis flaps. Semin Ophthalmol. 2014;29:363h DN. doi: 10.3109/08820538.2014.959194. [DOI] [PubMed] [Google Scholar]
- 12.AmbrAmbr Melki S. Complications of femtosecond-assisted laser in-situ Etiology, prevention, and treatment. J Refract Surg. 2001;17:350even. doi: 10.3928/1081-597X-20010501-09. [DOI] [PubMed] [Google Scholar]
- 13.Romero-Diaz-de-Leon L, Serna-Ojeda JC, Navas A, Graue-HernHernin-situ keratomileusis flaps Semin Ophtflap complications in LASIK surgery performed by ophthalmology residents. J Ophthalmic Vis Res. 2016;11:263Oph. doi: 10.4103/2008-322X.188393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Melki SA, Azar DT. LASIK complications:Etiology, management, and prevention. Surv Ophthalmol. 2001;46:95anage. doi: 10.1016/s0039-6257(01)00254-5. [DOI] [PubMed] [Google Scholar]
- 15.Wilson SE. LASIK:Management of common complications. Laser in situ keratomileusis. Cornea. 1998;17:459emen. doi: 10.1097/00003226-199809000-00001. [DOI] [PubMed] [Google Scholar]
- 16.Salomalomof common complications. Laser in situ keratomileusis. Cornea. 1998 doi: 10.1097/00003226-199809000-00001. 17leusis flaps. Semin Ophthal:1024malo. [DOI] [PubMed] [Google Scholar]
- 17.Maldonado MJ. Juberuberlications. Laser in situ keratomileusis. Cornea 1998;17leusis flaps. Semin Ophthalmol 2keratomileusis retreatment. J Cataract Refract Surg. 2005;31:2016ona. doi: 10.1016/j.jcrs.2005.06.038. [DOI] [PubMed] [Google Scholar]
- 18.Jain V, Mhatre K, Shome D. Flap buttonhole in thin-flap laser in situ keratomileusis:Case series and review. Cornea. 2010;29:655es. doi: 10.1097/ICO.0b013e3181c377d5. [DOI] [PubMed] [Google Scholar]
- 19.Al-Mezaine HS, Al-Amro SA, Al-Obeidan S. Incidence, management, and visual outcomes of buttonholed laser in situ keratomileusis flaps. J Cataract Refract Surg. 2009;35:839Meza. doi: 10.1016/j.jcrs.2009.01.013. [DOI] [PubMed] [Google Scholar]
- 20.Geggel HS. Treatment of lost flaps and slipped flaps. Int Ophthalmol Clin. 2008;48:65ggel. doi: 10.1097/IIO.0b013e31815eb96d. [DOI] [PubMed] [Google Scholar]
- 21.Joo CK, Kim TG. Corneal perforation during laser in situ keratomileusis. J Cataract Refract Surg. 1999;25:1165CK. doi: 10.1016/s0886-3350(99)00117-0. [DOI] [PubMed] [Google Scholar]
- 22.Liu Q, Gong XM, Chen JQ, Yang B, Ge J, To CH. Laser in situ keratomileusis induced corneal perforation and recurrent corneal epithelial ingrowth. J Cataract Refract Surg. 2005;31:857 Q. doi: 10.1016/j.jcrs.2004.09.027. [DOI] [PubMed] [Google Scholar]
- 23.Seider MI, Ide T, Kymionis GD, Culbertson WW, OW O. in situ keratomileusis induced corneal perforation and recurrent corneal epithelial ingrowth. J Cataract Refract Surg. 2005 doi: 10.1016/j.jcrs.2004.09.027. 31t is mana:859der. [DOI] [PubMed] [Google Scholar]
- 24.Srinivasan S, Herzig S. SubS. Sub, Herzig S. Sub Sub recurrent corneal epithelial ingroreation for LASIK. Br J Ophthalmol. 2007;91:1373. doi: 10.1136/bjo.2007.129213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Davison JA, Johnson SC. Intraoperative complications of LASIK flaps using the IntraLase femtosecond laser in 3009 cases. J Refract Surg. 2010;26:851iso. doi: 10.3928/1081597X-20100114-07. [DOI] [PubMed] [Google Scholar]
- 26.Jung H-G, Kim J, Lim T-H. Possible risk factors and clinical effects of an opaque bubble layer created with femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg. 2015;41:1393 H-. doi: 10.1016/j.jcrs.2014.10.039. [DOI] [PubMed] [Google Scholar]
- 27.Lim DH, Hyun J, Shin E, Ko B-W, Chung E-S, Chung T-Y. Incidence and risk factors of opaque bubble layer formation according to flap thickness during 500-kHz FS-LASIK. J Refract Surg. 2019;35:583kHz. doi: 10.3928/1081597X-20190814-01. [DOI] [PubMed] [Google Scholar]
- 28.Kaiserman I, Maresky HS, Bahar I, Rootman DS. Incidence, possible risk factors, and potential effects of an opaque bubble layer created by a femtosecond laser. J Cataract Refract Surg. 2008;34:417serm. doi: 10.1016/j.jcrs.2007.10.026. [DOI] [PubMed] [Google Scholar]
- 29.Robert M-C, Khreim N, Todani A, Melki SA. Anterior chamber gas bubble emergence pattern during femtosecond LASIK-flap creation. Br J Ophthalmol. 2015;99:1201rt. doi: 10.1136/bjophthalmol-2014-306307. [DOI] [PubMed] [Google Scholar]
- 30.Srinivasan S, Rootman DS. Anterior chamber gas bubble formation during femtosecond laser flap creation for LASIK. J Refract Surg. 2007;23:828niva. doi: 10.3928/1081-597X-20071001-14. [DOI] [PubMed] [Google Scholar]
- 31.Tomita M, Watabe M, Waring GO, Durrie DS. Corneal endothelial cell density after myopic intra-LASIK and the effect of AC gas bubbles on the corneal endothelium. Eur J Ophthalmol. 2011;21:363ita. doi: 10.5301/EJO.2010.6100. [DOI] [PubMed] [Google Scholar]
- 32.Duffey RJ. Central islands and decentered ablations after LASIK. Int Ophthalmol Clin. 2000;40:93ffey. doi: 10.1097/00004397-200007000-00012. [DOI] [PubMed] [Google Scholar]
- 33.Sridhar MS, Rao SK, Vajpayee RB, Aasuri MK, Hannush S, Sinha R. Complications of laser-in-situ-keratomileusis. Indian J Ophthalmol. 2002;50:265dhar. [PubMed] [Google Scholar]
- 34.Kang SW, Chung ES, Kim WJ. Clinical analysis of central islands after laser in situ keratomileusis. J Cataract Refract Surg. 2000;26:536g SW. doi: 10.1016/s0886-3350(99)00458-7. [DOI] [PubMed] [Google Scholar]
- 35.Lee JS, Joo CK. Central islands after LASIK detected by corneal topography. Korean J Ophthalmol. 2001;15:8) e J. doi: 10.3341/kjo.2001.15.1.8. [DOI] [PubMed] [Google Scholar]
- 36.Johnson JD, Azar DT. Surgically induced topographical abnormalities after LASIK:Management of central islands, corneal ectasia, decentration, and irregular astigmatism. Curr Opin Ophthalmol. 2001;12:309entr. doi: 10.1097/00055735-200108000-00012. [DOI] [PubMed] [Google Scholar]
- 37.Manche E, Roe J. Recent advances in wavefront-guided LASIK. Curr Opin Ophthalmol. 2018;29:286che. doi: 10.1097/ICU.0000000000000488. [DOI] [PubMed] [Google Scholar]
- 38.Vesaluoma M PJ. Recent advances in wavefront-guided LASIK. Curr Opin Ophthalmol. 2018;298 doi: 10.1097/ICU.0000000000000488. 29almol 2001;1215act Refract Surg 2000;262002;502;50rneal end: 369aluo. [DOI] [PubMed] [Google Scholar]
- 39.Mimouni M, Vainer I, Assad N, Nemet A, Sela T, Munzer G, et al. Incidence, indications, and outcomes of eyes needing early flap lifting after LASIK. Cornea. 2018;37:1118. Co. doi: 10.1097/ICO.0000000000001617. [DOI] [PubMed] [Google Scholar]
- 40.Segev F, Mimouni M, Sela T, Munzer G, Kaiserman I. Risk factors for sporadic diffuse lamellar keratitis after microkeratome laser-assisted in situ keratomileusis:A retrospective large database analysis. Cornea. 2018;37:1124nea. doi: 10.1097/ICO.0000000000001674. [DOI] [PubMed] [Google Scholar]
- 41.Clare G, Moore TCB, Grills C, Leccisotti A, Moore JE, Schallhorn S. Early flap displacement after LASIK. Ophthalmology. 2011;118:1760e G. doi: 10.1016/j.ophtha.2011.01.053. [DOI] [PubMed] [Google Scholar]
- 42.Galvis V, Tello A, Guerra AR, Rey JJ, Camacho PA. Risk factors and visual results in cases of LASIK flap repositioning due to folds or dislocation:Case series and literature review. Int Ophthalmol. 2014;34:19ies. doi: 10.1007/s10792-013-9776-9. [DOI] [PubMed] [Google Scholar]
- 43.Ting DSJ, Danjoux J-P. Late-onset traumatic dislocation of laser in situ keratomileusis corneal flaps:A case series with many clinical lessons. Int Ophthalmol. 2019;39:1397serie. doi: 10.1007/s10792-018-0946-7. [DOI] [PubMed] [Google Scholar]
- 44.Wallerstein A, Gauvin M, Adiguzel E, Singh H, Gupta V, Harissi-Dagher M, et al. Clinically significant laser in situ keratomileusis flap striae. J Cataract Refract Surg. 2017;43:1523kera. doi: 10.1016/j.jcrs.2017.09.023. [DOI] [PubMed] [Google Scholar]
- 45.Probst LE, Machat J. Removal of flap striae following laser in situ keratomileusis. J Cataract Refract Surg. 1998;24:153bst. doi: 10.1016/s0886-3350(98)80193-4. [DOI] [PubMed] [Google Scholar]
- 46.Solomon R, Donnenfeld ED, Perry HD, Doshi S, Biser S. Slitlamp stretching of the corneal flap after laser in situ keratomileusis to reduce corneal striae. J Cataract Refract Surg. 2003;29:1292mon. doi: 10.1016/s0886-3350(03)00046-4. [DOI] [PubMed] [Google Scholar]
- 47.Abdelazeem K, Nassr MA, Abdelmotaal H, Wasfi E, El-Sebaity DM. Flap sliding technique for managing flap striae following laser in situ keratomileusis. J Ophthalmol. 2020;2020:5614327. doi: 10.1155/2020/5614327. doi:10.1155/2020/5614327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Netto MV, Wilson SE. Flap lift for LASIK retreatment in eyes with myopia. Ophthalmology. 2004;111:1362o M. doi: 10.1016/j.ophtha.2003.11.009. [DOI] [PubMed] [Google Scholar]
- 49.Seider MI, McLeod SD, Porco TC, Schallhorn SC. The effect of procedure room temperature and humidity on LASIK outcomes. Ophthalmology. 2013;120:2204er. doi: 10.1016/j.ophtha.2013.04.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Hood CT, Shtein RM, Veldheer D, Hussain M, Niziol LM, Musch DC, et al. The effect of humidity and temperature on visual outcomes after myopic corneal laser refractive surgery. Clin Ophthalmol. 2016;10:2231201. doi: 10.2147/OPTH.S118503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Schallhorn SC, Venter JA, Hannan SJ, Hettinger KA, Teenan D. Flap lift and photorefractive keratectomy enhancements after primary laser in situ keratomileusis using a wavefront-guided ablation profile:Refractive and visual outcomes. J Cataract Refract Surg. 2015;41:2501llho. doi: 10.1016/j.jcrs.2015.05.031. [DOI] [PubMed] [Google Scholar]
- 52.Venter J. Outcomes of myopic LASIK with and without NIDEK active torsion error correction. J Refract Surg. 2009;25:985ter. doi: 10.3928/1081597X-20091016-03. [DOI] [PubMed] [Google Scholar]
- 53.Shen EP, Chen W-L, Hu F-R. Manual limbal markings versus iris-registration software for correction of myopic astigmatism by laser in situ keratomileusis. J Cataract Refract Surg. 2010;36:431n E. doi: 10.1016/j.jcrs.2009.10.030. [DOI] [PubMed] [Google Scholar]
- 54.Neuhann IM, Lege BAM, Bauer M, Hassel JM, Hilger A, Neuhann TF. Static and dynamic rotational eye tracking during LASIK treatment of myopic astigmatism with the Zyoptix laser platform and Advanced Control Eye Tracker. J Refract Surg. 2010;26:17uhan. doi: 10.3928/1081597X-20101215-03. [DOI] [PubMed] [Google Scholar]
- 55.Cohen E, Spierer O. Dry eye post-laser-assisted in situ keratomileusis:Major review and latest updates. J Ophthalmol. 2018;2018:4903831. doi: 10.1155/2018/4903831. doi:10.1155/2018/4903831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Donnenfeld ED, Solomon K, Perry HD, Doshi SJ, Ehrenhaus M, Solomon R, et al. The effect of hinge position on corneal sensation and dry eye after LASIK. Ophthalmology. 2003;110 doi: 10.1016/S0161-6420(03)00100-3. 1023 effect of hinge pos30. [DOI] [PubMed] [Google Scholar]
- 57.Huang JC-C, Sun C-C, Chang C-K, Ma DH-K, Lin Y-F. Effect of hinge position on corneal sensation and dry eye parameters after femtosecond laser-assisted LASIK. J Refract Surg. 2012;28:625ng J. doi: 10.3928/1081597X-20120815-07. [DOI] [PubMed] [Google Scholar]
- 58.Darwish T, Brahma A, Oma A, OOA, OEfron N. Subbasal nerve fiber regeneration after LASIK and LASEK assessed by noncontact esthesiometry and in vivo confocal microscopy:Prospective study. J Cataract Refract Surg. 2007;33:1515. J. doi: 10.1016/j.jcrs.2007.05.023. [DOI] [PubMed] [Google Scholar]
- 59.Salib GM, McDonald MB, Smolek M. Safety and efficacy of cyclosporine 0.05% drops versus unpreserved artificial tears in dry-eye patients having laser in situ keratomileusis. J Cataract Refract Surg. 2006;32:772ib. doi: 10.1016/j.jcrs.2005.10.034. [DOI] [PubMed] [Google Scholar]
- 60.Moshirfar M, Hazin R, Khalifa YM. Central toxic keratopathy. Curr Opin Ophthalmol. 2010;21:274hir. doi: 10.1097/ICU.0b013e32833a8cb2. [DOI] [PubMed] [Google Scholar]
- 61.Jutley G, Aiello F, Robaei D, Maurino V. Central toxic keratopathy after laser in situ keratomileusis. J Cataract Refract Surg. 2014;40:1985ey G. doi: 10.1016/j.jcrs.2014.03.030. [DOI] [PubMed] [Google Scholar]
- 62.Hau SCH, Allan BD. In vivo confocal microscopy findings in central toxic keratopathy. J Cataract Refract Surg. 2012;38:710 co. doi: 10.1016/j.jcrs.2012.01.010. [DOI] [PubMed] [Google Scholar]
- 63.Gritz DC. LASIK interface keratitis:Epidemiology, diagnosis and care. Curr Opin Ophthalmol. 2011;22:251agn. doi: 10.1097/ICU.0b013e3283477b52. [DOI] [PubMed] [Google Scholar]
- 64.Smith RJ, Maloney RK. Diffuse lamellar keratitis. A new syndrome in lamellar refractive surgery. Ophthalmology. 1998;105:1721h R. doi: 10.1016/S0161-6420(98)99044-3. [DOI] [PubMed] [Google Scholar]
- 65.de Paula FH, Khairallah CG, Niziol LM, Musch DC, Shtein RM. Diffuse lamellar keratitis after laser in situ keratomileusis with femtosecond laser flap creation. J Cataract Refract Surg. 2012;38:1014aul. doi: 10.1016/j.jcrs.2011.12.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis:Diagnosis and management. J Cataract Refract Surg. 2000;26:1072ana. doi: 10.1016/s0886-3350(00)00468-5. [DOI] [PubMed] [Google Scholar]
- 67.Tourtas T, Kopsachilis N, Meiller R, Kruse FE, Cursiefen C. Pressure-induced interlamellar stromal keratitis after laser in situ keratomileusis. Cornea. 2011;30:920rta. doi: 10.1097/ICO.0b013e3182032002. [DOI] [PubMed] [Google Scholar]
- 68.Kurian M, Shetty R, Shetty BK, Devi SAV. In vivo confocal microscopic findings of interlamellar stromal keratopathy induced by elevated intraocular pressure. J Cataract Refract Surg. 2006;32:1563an. doi: 10.1016/j.jcrs.2006.03.041. [DOI] [PubMed] [Google Scholar]
- 69.Cabral-Macias J, GarcGarcy BK, Devi SAV. In vivo confocal microscopic findings of interlamellar stromal keratop. Pressure-induced stromal keratopathy after laser in situ keratomileusis:Acute and late-onset presentations. J Cataract Refract Surg. 2018;44:1284kera. doi: 10.1016/j.jcrs.2018.06.053. [DOI] [PubMed] [Google Scholar]
- 70.Rocha KM, Kagan R, Smith SD, Krueger RR. Thresholds for interface haze formation after thin-flap femtosecond laser in situ keratomileusis for myopia. Am J Ophthalmol. 2009;147:966ha KM, Kagan. doi: 10.1016/j.ajo.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 71.Jabbur NS, Sakatani K OK, O Krueger RR. Thresholds for interface haze formation after thin-flap femtosecond laser in situ keratomileusis for myopia. Am J Ophthalmol. 2009;147:966ha KM, Kagan. doi: 10.1016/j.ajo.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 72.Krueger RR, Thornton IL, Xu M, Bor Z, van den Berg TJTP. Rainbow glare as an optical side effect of IntraLASIK. Ophthalmology. 2008;115:1187–95.e1. doi: 10.1016/j.ophtha.2007.10.007. [DOI] [PubMed] [Google Scholar]
- 73.Schallhorn SC, Kaupp SE, Tanzer DJ, Tidwell J, Laurent J, Bourque LB. Pupil size and quality of vision after LASIK. Ophthalmology. 2003;110:1606llho. doi: 10.1016/S0161-6420(03)00494-9. [DOI] [PubMed] [Google Scholar]
- 74.Villa C, GutiGutiupp SE, Tanzer DJ, Tidwell J, Laurent J, Bourque LB. Pupil size and quality of vision after LASIK. Ophthalmology. 2003;1:1031a C. doi: 10.1016/S0161-6420(03)00494-9. [DOI] [PubMed] [Google Scholar]
- 75.Lee JH, You YS, Choe CM, Lee ES. Efficacy of brimonidine tartrate 0.2% ophthalmic solution in reducing halos after laser in situ keratomileusis. J Cataract Refract Surg. 2008;34:963 JH. doi: 10.1016/j.jcrs.2008.01.028. [DOI] [PubMed] [Google Scholar]
- 76.Roe JR, Manche EE. Prospective, randomized, contralateral eye comparison of wavefront-guided and wavefront-optimized laser in situ keratomileusis. Am J Ophthalmol. 2019;207:175comp. doi: 10.1016/j.ajo.2019.05.026. [DOI] [PubMed] [Google Scholar]
- 77.Yamane N, Miyata K, Samejima T, Hiraoka T, Kiuchi T, Okamoto F, et al. Ocular higher-order aberrations and contrast sensitivity after conventional laser in situ keratomileusis. Invest Ophthalmol Vis Sci. 2004;45:3986lar. doi: 10.1167/iovs.04-0629. [DOI] [PubMed] [Google Scholar]
- 78.MontMonthigher-order aberrations and contrast sensitivity after conventional laser in situ keratomileusis. Invest Ophthalmol Vis Sci. 2004;45:3986lar. doi: 10.1167/iovs.04-0629. [DOI] [PubMed] [Google Scholar]
- 79.Ortega-Usobiaga J, Llovet-Osuna F, Djodeyre MR, Llovet-Rausell A, Beltran J, Baviera J. Incidence of corneal infections after laser in situ keratomileusis and surface ablation when moxifloxacin and tobramycin are used as postoperative treatment. J Cataract Refract Surg. 2015;41:1210per. doi: 10.1016/j.jcrs.2014.09.041. [DOI] [PubMed] [Google Scholar]
- 80.Donnenfeld ED, Kim T, Holland EJ, Azar DT, Palmon FR, Rubenstein JB, et al. ASCRS white paper:Management of infectious keratitis following laser in situ keratomileusis. J Cataract Refract Surg. 2005;31:2008agem. doi: 10.1016/j.jcrs.2005.10.030. [DOI] [PubMed] [Google Scholar]
- 81.Chang MA, Jain S, Azar DT. Infections following laser in situ keratomileusis:An integration of the published literature. Surv Ophthalmol. 2004;49:269grat. doi: 10.1016/j.survophthal.2004.02.007. [DOI] [PubMed] [Google Scholar]
- 82.Stonecipher KG, Dishler JG, Ignacio TS, Binder PS. Transient light sensitivity after femtosecond laser flap creation:Clinical findings and management. J Cataract Refract Surg. 2006;32:91din. doi: 10.1016/j.jcrs.2005.11.015. [DOI] [PubMed] [Google Scholar]
- 83.Mu oz G. Albarr management. J Cataract Refract Surg 2006;32sient light sensitivity after femtosecond laser flap creation: s after laser in smtosecond laser Incidence and prevention. J Cataract Refract Surg. 2006;32:2075 Al. [Google Scholar]
- 84.Yan MK, Chang JS, Chan TC. Refractive regression after laser in situ keratomileusis. Clin Experiment Ophthalmol. 2018;46:934 MK. doi: 10.1111/ceo.13315. [DOI] [PubMed] [Google Scholar]
- 85.Lim SA, Park Y, Cheong YJ, Na KS, Joo CK. Factors affecting long-term myopic regression after laser in situ keratomileusis and laser-assisted subepithelial keratectomy for moderate myopia. Korean J Ophthalmol. 2016;30:92orean. doi: 10.3341/kjo.2016.30.2.92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Qi H, Gao C, Li Y, Feng X, Wang M, Zhang Y, et al. The effect of Timolol 0.5% on the correction of myopic regression after LASIK. Medicine (Baltimore) 2017;96:e6782. doi: 10.1097/MD.0000000000006782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Kanellopoulos AJ, Kahn J. Topography-guided hyperopic LASIK with and without high irradiance collagen cross-linking:Initial comparative clinical findings in a contralateral eye study of 34 consecutive patients. J Refract Surg. 2012;28(11 Suppl):S837–40. doi: 10.3928/1081597X-20121005-05. [DOI] [PubMed] [Google Scholar]
- 88.Ting DSJ, Srinivasan S, Danjoux J-P. Epithelial ingrowth following laser in situ keratomileusis (LASIK):Prevalence, risk factors, management and visual outcomes. BMJ Open Ophthalmol. 2018;3:e000133. doi: 10.1136/bmjophth-2017-000133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Neff KD, Probst LE. LASIK complications. In: Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea:Surgery of the Cornea and Conjunctiva. 3rd ed. St. Louis, MO: Mosby; 2011. [Google Scholar]
- 90.Chen LY, Kung JS, Manche EE. Management of complex epithelial ingrowth after laser in situ keratomileusis using fibrin tissue glue. Eye Contact Lens. 2018;44(Suppl 2):S210 2o. doi: 10.1097/ICL.0000000000000447. [DOI] [PubMed] [Google Scholar]
- 91.Mohammed OA, Mounir A, Hassan AA, Alsmman AH, Mostafa EM. Nd:YAG laser for epithelial ingrowth after laser in situ keratomileusis. Int Ophthalmol. 2019;39:1225mmed. doi: 10.1007/s10792-018-0923-1. [DOI] [PubMed] [Google Scholar]
- 92.Bohac M, Koncarevic M, Pasalic A, Biscevic A, Merlak M, Gabric N, et al. Incidence and clinical characteristics of post LASIK ectasia:A review of over 30,000 LASIK cases. Semin Ophthalmol. 2018;33:869 min. doi: 10.1080/08820538.2018.1539183. [DOI] [PubMed] [Google Scholar]
- 93.Santhiago MR. Percent tissue altered and corneal ectasia. Curr Opin Ophthalmol. 2016;27:311thi. doi: 10.1097/ICU.0000000000000276. [DOI] [PubMed] [Google Scholar]
- 94.Giri P, Azar DT. Risk profiles of ectasia after keratorefractive surgery. Curr Opin Ophthalmol. 2017;28:337i P. doi: 10.1097/ICU.0000000000000383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Tong JY, Viswanathan D, Hodge C, Sutton G, Chan C, Males JJ. Corneal collagen crosslinking for post-LASIK ectasia:An Australian study. Asia Pac J Ophthalmol (Phila) 2017;6:228ia P. doi: 10.22608/APO.2016197. [DOI] [PubMed] [Google Scholar]
- 96.Arevalo JF. Posterior segment complications after laser-assisted in situ keratomileusis. Curr Opin Ophthalmol. 2008;19:177valo. doi: 10.1097/ICU.0b013e3282fb7c15. [DOI] [PubMed] [Google Scholar]
- 97.Ikeda T, Shimizu K, Igarashi A, Kasahara S, Kamiya K. Twelve-year follow-up of laser in situ keratomileusis for moderate to high myopia. Biomed Res Int. 2017;2017:9391436. doi: 10.1155/2017/9391436. doi:10.1155/2017/9391436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Tomita M, Watabe M, Yukawa S, Nakamura N, Nakamura T, Magnago T. Safety, efficacy, and predictability of laser in situ keratomileusis to correct myopia or myopic astigmatism with a 750 Hz scanning-spot laser system. J Cataract Refract Surg. 2014;40:251ita. doi: 10.1016/j.jcrs.2013.07.043. [DOI] [PubMed] [Google Scholar]