

Abstract
Background
Inflammatory bowel disease (IBD), comprising Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic inflammatory disorder of the gastrointestinal tract that has been associated with increased risk of extraintestinal manifestations, amongst which is venous thromboembolism (VTE). We assessed the risk for VTE in patients with IBD through systematic review and meta-analysis.
Methods
A systematic search for English language studies was conducted in Medline, Scopus, and the Cochrane Library of publications from database inception till August 10, 2020, to identify relevant studies reporting the risk of VTE in patients with IBD. The random-effects and fixed-effect models were used to estimate relative risks (RRs) with their respective 95% confidence intervals (CIs). The quality of the included studies was assessed using the Newcastle-Ottawa scale.
Results
Eleven observational studies were included in this meta-analysis, involving 3,175,012 patients with IBD and 920,144,253 controls without IBD. The overall RR for VTE in patients with IBD compared to non-IBD individuals was 2.03 (95%CI 1.72-2.39). An analysis of studies with larger population size demonstrated a lower risk for VTE (RR 1.77, 95%CI 1.48-2.13) among patients with IBD, whereas studies with a smaller population size yielded a greater risk for VTE (RR 2.67, 95%CI 1.97-2.93). After adjustment for smoking and body mass index, the RR for VTE was moderately increased (RR 2.65, 95%CI 1.51-4.65).
Conclusions
The present meta-analysis shows that IBD is linked to a 2-fold increased risk for VTE. Thus, primary prevention against VTE is of the utmost importance.
Keywords: Inflammatory bowel disease, venous thromboembolism, systematic review, meta-analysis
Introduction
Inflammatory bowel disease (IBD) is an autoimmune systemic disorder that mainly affects the gastrointestinal tract and predominantly includes ulcerative colitis (UC) and Crohn’s disease (CD), as distinct clinical entities. Its exact cause is not yet fully understood, with genetic susceptibility, environmental factors and alterations in the host’s innate as well as adaptive immunity being the principal etiological factors. Apart from the gastrointestinal involvement, IBD is also responsible for a multitude of extraintestinal manifestations, including thromboembolic events (TEs) that significantly increase morbidity and mortality [1,2].
TEs in IBD are often missed, given the fact that the prevalence of thrombosis varies between 1.3% and 7.7% in patients with IBD, and the rate increases up to 39-41% in autopsy series [3,4]. The pathologic process of TEs in IBD patients involves multiple factors. Abnormalities in procoagulation, anticoagulation, and fibrinolytic factors have been proven to contribute to the development of thrombus in IBD, although several studies have not reported any risk factors in about 50% of IBD patients with TEs. Acquired risk factors for venous thromboembolism (VTE) include oral contraceptive use, surgical operation, body mass index (BMI) >30 kg/m2, trauma, pregnancy, puerperium, lupus anticoagulants, malignancy, long-distance travel, myeloproliferative disorders, and polycythemia vera [5,6]. Systemic corticosteroids in long-term courses were also associated with a significantly higher rate of VTE in IBD patients, compared to IBD patients without steroid medication [7]. Over half of the cases of VTE in IBD may be associated with factor V Leiden and prothrombin gene mutation, which may indicate that genetic factors play a role in VTE; however, this is inconsistent with other studies [8,9].
Venous thrombosis is commonly observed in deep veins of the lower extremities (deep venous thrombosis [DVT]) and the pulmonary arterial circulation (pulmonary embolism [PE]). Less frequently, cerebrovascular, portal, mesenteric, hepatic and retinal vein thrombosis is observed [10,11]. Even though several observational studies and a couple of meta-analyses have investigated the relationship between VTE and IBD [12-14], the exact risk estimate of VTE in the IBD population remains ambiguous because of methodological differences and heterogeneity across studies. The aim of this study was to evaluate the risk of VTE in patients with IBD compared to the non-IBD population. Accordingly, we conducted a systematic review and meta-analysis of observational studies that investigated the incidence of VTE, including DVT and/or PE in patients with IBD.
Materials and methods
This systematic review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines [15,16]. The study protocol is registered with the PROSPERO international prospective register of systematic reviews (protocol number: CRD42020204404) [17]. The present meta-analysis was performed based on previously published studies; therefore, no ethical approval or patient consent were required.
Search strategy
A systematic literature search of Medline, Cochrane Library and Scopus was conducted from inception till August 10, 2020, to identify studies that reported the risk of VTE in patients with IBD. Key questions were formulated according to the “PICO” method: “Do adults diagnosed with IBD have increased risk for VTE compared to adults without IBD?” [18]. Text words and, if applicable, database subject heading fields (e.g., Medical Subject Headings), were used to perform the searches: “inflammatory bowel disease”, “IBD”, “ulcerative colitis”, “Crohn’s disease”, “thromboembolism”, “pulmonary embolism”, “deep vein thrombosis”, “thrombosis”, “venous thromboembolism”, “VTE” and “DVT” (Supplementary material (50KB, pdf) ). In addition, we examined the references of each of the retrieved studies to identify further articles that met our criteria. Search filters of human and English language studies were used. The title and abstract of studies identified in the original search were reviewed by 2 independent authors (KA and AA) to eliminate studies that did not answer our research question, based on predetermined inclusion and exclusion criteria. The full text of the remaining articles was evaluated to determine whether it contained pertinent information. The coefficient of agreement between the 2 reviewers for article selection (k ¼ 0.87, 95% confidence interval [CI] 0.77-0.96) was excellent. Conflicts in study selection were resolved by consensus, referring back to the original article and, if an agreement failed to be reached, a third author (CK) was consulted.
Selection criteria
Studies in this meta-analysis were observational cohort or case-control studies that met the following inclusion criteria: 1) diagnosed IBD (CD and/or UC) according to well-defined criteria; 2) reported incident cases of first VTE/ DVT or PE event after the diagnosis of IBD; 3) included a non-IBD population for which VTE/ DVT or PE event rates were calculated (or could be inferred as expected event rates from a reference population); 4) reported relative risk ([RR] for cohort studies), rate or risk ratio (for cohort studies), odds ratios (for case-control studies), hazard ratio (for cohort studies) with 95%CIs or provided raw data for their calculation; and 5) assessed age and sex as confounding factors. We included peer-reviewed, observational controlled data (case-control and cohort studies) deriving from hospital, referral center and population based-studies. Studies evaluating only pediatric patients (age <18 years) were excluded. Cross-sectional studies, meta-analyses, review articles, short surveys, letters to the editor, notes, case reports, pilot studies and conference abstracts were excluded. In addition, studies including only pregnant or postoperative populations as control groups, studies that evaluated only recurrent VTEs and studies that did not contain primary data were excluded. Selection was not restricted by the number of participants in each study. If there were multiple published studies coming from the same population, only data from the most recent comprehensive report were included. VTE was defined as the presence of a first episode of DVT and/or PE, confirmed by objective imaging techniques. IBD, which included UC and/or CD, was defined based on medical diagnostic codes and records of clinical, endoscopic, histological, and radiological findings.
Data extraction
Two investigators (KA and AA) reviewed and abstracted the data independently onto a standardized form. The following data were collected from the studies: author and year of publication, study design, time period of study conduction, origin of the study population, type of exposure (IBD [CD and/or UC] and control population), primary outcome (VTE, DVT, and/or PE) and definition of outcome, total number of participants in each group (IBD vs. non-IBD controls), frequency of VTE, DVT, and PE adjusted for potential confounders, as well as confounding factors reported in each study. When frequencies of IBD patients and associated VTE events were not reported in the studies, we merged data on UC and CD to evaluate the VTE risk estimate for the IBD population as a whole. Risk estimates of outcomes were extracted as RRs and their 95%CIs. Data on the following covariates for DVT or PE were extracted from each study, wherever available: age, sex, history of cancer, history of major surgery, BMI, history of pregnancy, history of PE or DVT, and smoking habits.
Outcome measures
The primary analysis focused on assessing the RR of VTE, defined as DVT and/or PE, in patients diagnosed with IBD (CD and/or UC) according to well-defined criteria [19-21], compared with non-IBD subjects originating from the general population, hospital or referral center. Furthermore, based on information available from individual studies, we performed subgroup analysis evaluating the risk estimates for DVT and PE separately in patients diagnosed with IBD compared to controls, and additionally compared the risk for DVT vs. PE in IBD patients. Moreover, CD and UC risk estimates for VTE, DVT and PE compared to controls were calculated individually. In addition, risk estimates for VTE, DVT and PE events were separately estimated in patients with UC vs. CD. Risk estimates for VTE in IBD individuals were also calculated, according to the IBD population size. We separated studies into 2 groups (larger and smaller) based on the median value of the total number of IBD patients in each of the 11 studies, which was 13,756. The influence of sex on the occurrence of VTE in patients with IBD was also assessed. Finally, we assessed the risk for VTE in IBD patients vs. controls adjusted for BMI and smoking, based on the available data.
Data presentation
The PRISMA flow chart was used to report the selection process of the studies and includes an overall summary of the number and types of articles incorporated into the review (Fig. 1).
Figure 1.

Study selection flow diagram presented according to the PRISMA Statement
Quality assessment of the studies
The quality of case-control and cohort studies included in our meta-analysis was independently assessed by 2 investigators (KA and AA), using the Newcastle-Ottawa scale [22]. The scale is based on a “star system” that ranges from 0-9, with 0 being the lowest possible quality, and judges study quality according to 3 perspectives: selection of the study groups (4 questions), comparability of the groups (2 questions), and ascertainment of the outcome of interest (3 questions). Each question was rated with maximum 1 star except for “comparability of the groups”, for which separate stars were awarded for controlling age and/or sex (maximum 2 stars). Any differences between the 2 investigators were addressed via a reevaluation of the original article.
Statistical analysis
All information was reported according to the PRISMA and MOOSE guidelines for meta-analyses [15,16]. The Cochrane Collaboration’s Review Manager Software (version 5.4) was used to perform the data analysis. The generic inverse variance method was used to combine the studies with different scales of outcome estimates for random-effect meta-analysis, calculating ln(RRs) and the SE (ln(RR)) [23]. When RRs and their respective confidence intervals (CIs) were not reported in the studies, they were calculated using the original data. Because the evaluated outcomes are relatively rare and the effects estimated are generally small, odds ratios in case-control studies were considered reasonable approximations of the corresponding RRs in cohort studies [24,25]. We assessed the heterogeneity between study-specific estimates using 2 methods. First, the Cochran Q statistical test for heterogeneity, which tests the null hypothesis that all studies in a meta-analysis have the same underlying magnitude of effect, was measured. Because this test is underpowered to detect moderate degrees of heterogeneity, the presence of statistically significant heterogeneity across the studies was evaluated by utilizing a P-value <0.10. Second, to estimate what proportion of total variation across studies was caused by study-related factors (clinical setting, methodological or statistical differences) rather than chance, the I2 statistic was calculated, where I2=100% ×(Q−df)/Q represents the magnitude of the heterogeneity (moderate: 30-60%, substantial: 50-90%, considerable: 75-100%) [23,26,27]. Dichotomous outcomes were pooled using the Mantel-Haenszel random-effects model (when more than moderate heterogeneity was detected among studies), used to calculate the RRs and corresponding 95%CIs. The Mantel-Haenszel fixed effects model was used to calculate the RRs and corresponding 95%CIs in the case of homogenous studies. For all tests (except for heterogeneity), a probability level <0.05 was considered statistically significant.
Visual inspection of the funnel plot demonstrated the asymmetry typically associated with publication bias [28]. That is, smaller, less precise studies (those with the larger standard errors) appeared to have higher RRs than the larger, more precise studies. Evidence of publication bias was also confirmed by Egger’s test [29], which was performed using linear regression analysis in the IBM SPSS statistics 26.0 software, since the number of the included studies was n>10.
Results
Eligible studies
The search strategy identified 1547 articles (Fig. 1). After removal of duplicates and screening of titles, abstracts and keywords, 20 papers underwent full-text review. During this process, 6 articles were excluded because of irrelevant outcomes [30-35], while 1 study was excluded for its cross-sectional design [36]. In addition, 2 studies reported outcomes that originated from the same database [37,38]; accordingly, the study with the shorter follow-up period was excluded [38]. Another study was excluded because it neither provided an overall risk estimate for VTE, nor offered available data for calculating it [39]. The remaining 11 studies [37,40-49], published between 2001 and 2018, fulfilled the selection criteria.
Quality assessment of the included studies
We used the Newcastle-Ottawa scale to evaluate the quality of the studies included in our meta-analysis: 2 studies were rated as 9-star, 5 studies as 8-star and 4 studies as 7-star. The included studies averaged a quality score of 7.8. All studies provided a clear definition of the diagnosis of VTE, including the details of confirmation based on imaging techniques. Some studies used the international disease codes for VTE diagnosis (Table 1).
Table 1.
The Newcastle-Ottawa scale for assessing the risk of bias of the included studies

General characteristics
Our meta-analysis included 11 observational studies (10 cohort studies [40-49] and 1 case-control study [37]), the general characteristics of which are described in Table 2. Six studies were population-based, 4 were hospital-based and 1 study had a referral center as a population source. The primary analysis included 3,175,012 patients with IBD and 920,144,253 controls without IBD. In the analysis of secondary outcomes, regarding the evaluation of risk estimates for DVT and PE in IBD patients compared to controls without IBD, 5 studies were included [37,42,44,45,49]. In addition, 4 studies were included in the analysis regarding the risk of VTE in patients with UC compared to patients with CD [37,44,48,49], while 3 studies were used to evaluate the risk of DVT and PE [37,44,49], in the same subgroups. Articles had large differences in their selection of covariates for adjusted analyses. Covariates included demographics such as age and sex, past medical history (history of surgery, history of pregnancy, history of cancer, history of PE or DVT), as well as other risk factors, such as BMI and smoking habits. Six studies included in the analysis assessed the influence of sex on the risk for VTE in patients with IBD [37,41,42,45,48,49]. A subgroup analysis was also performed, including 3 studies that evaluated smoking and BMI as confounding factors [41,43,45].
Table 2.
Characteristics of the studies included in the meta-analysis of venous thromboembolic events in patients with inflammatory bowel disease

Quantitative analysis and evaluation of heterogeneity
The overall RR for VTE in patients with IBD compared to non-IBD individuals was 2.03 (95%CI 1.72-2.39). All individual studies had RR estimates above 1.0 with statistical significance. Significant heterogeneity was observed among studies (Q statistic=412.43, P<0.10, I2=98%). (Fig. 2).
Figure 2.

Forest plot demonstrating the summary relative risk for venous thromboembolic events in patients with inflammatory bowel disease. Studies are listed in chronological order.
IBD, inflammatory bowel disease; CI, confidence interval
To identify possible sources of heterogeneity, several subgroup analyses were performed relating to study size, IBD type, thrombosis location, and adjustment for confounders (Table 3). Analysis of studies with larger IBD population size [37,41,43,44,46,48] demonstrated a lower risk for VTE (RR 1.77, 95%CI 1.48-2.13) among patients with IBD, whereas studies with smaller IBD population size [40,42,45,47,49] yielded a greater risk for VTE (RR 2.67, 95%CI 1.97-2.93). A greater risk for VTE was found in both patients with UC (RR 1.8, 95%CI 1.15-2.82) and those with CD (RR 1.72, 95%CI 1.58-1.88), with no difference between the 2 groups (RR 1.03, 95%CI 0.72-1.46). Similar results were found in relation to the risk for DVT and PE in patients with UC and CD, with no difference between the 2 IBD clinical entities (Table 3). Additionally, patients with IBD presented a greater risk for DVT (RR 1.95, 95%CI 1.59-2.39) and PE (RR 1.91, 95%CI 1.75-2.08) compared to controls. The risk for DVT was almost 2-fold higher than that for PE in the IBD population (RR 1.96, 95%CI 1.34-2.86). Moreover, the risk for VTE in patients with IBD did not differ statistically significantly between male and female patients (RR 0.95, 95%CI 0.8-1.12). After adjustment for smoking and BMI, the RR for VTE was moderately increased (RR 2.65, 95%CI 1.51-4.65). The remaining 8 studies that did not adjust for these confounders demonstrated a lower risk for VTE in patients with IBD, but still greater compared to controls (RR 1.88, 95%CI 1.57-2.24).
Table 3.
Results of meta-analyses by type of outcome

There was significant heterogeneity among all the studies included in the aforementioned subgroup analyses (Table 3). Only studies evaluating the risk for PE in patients with IBD compared to non-IBD subjects demonstrated no evidence of heterogeneity (χ2=2.06, P=0.72, I2=0%). Finally, a secondary analysis was performed using the most recently published studies [41,42,49], which demonstrated a higher risk of VTE in patients with IBD (RR 1.88, 95%CI 1.70-2.07), without evidence of heterogeneity among them (Q statistic=0.43, P=0.81 I2=0%) (Table 3).
Publication bias
Upon inspection, the funnel plot of studies included in the primary analysis showed evidence of asymmetry suggestive of publication bias, which was confirmed statistically (Egger P=0.017) (Fig. 3). After 6 studies that appeared to be the cause of the asymmetry [40,43,44,46-48] were removed, little to no evidence of underlying bias could be found. Similarly, visual inspection of the funnel plots of the studies included in most of the subgroup analyses presented asymmetry that was indicative of possible publication bias.
Figure 3.
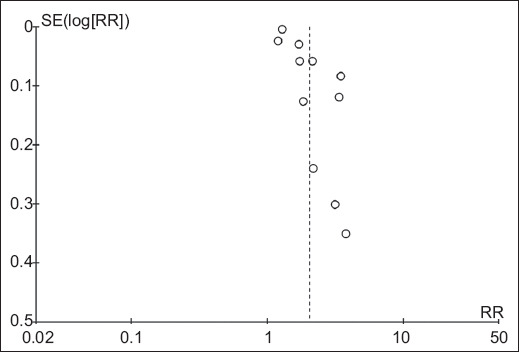
Funnel plot of the 11 studies included in the meta-analysis
SE, standard error; RR, relative risk
Discussion
Our meta-analysis, which evaluated pooled data from all currently available observational studies assessing the risk of VTE in patients with IBD, indicated that the overall risk of VTE was 2-fold higher in the IBD group, compared to the non-IBD control group. After both qualitative and quantitative confirmation of funnel plot asymmetry, publication bias was suspected of being the main culprit behind this relationship between VTE and IBD. As the pooled RR for VTE derived from the 6 studies with the largest sample sizes was substantially higher than the pooled RR from the “smaller” ones, the aforementioned assumption seemed quite plausible. However, the pooled RR for VTE derived from the “larger” studies did not differ greatly from the pooled RR of the primary analysis, indicating that publication bias on its own could not have been the causal factor for our results.
Subgroup analysis revealed that the risk of VTE in IBD was moderately increased after adjusting for smoking and BMI, indicating that, when considered together, these factors could act as confounders in the relationship between IBD and VTE. In addition, patients with IBD demonstrated an almost 2-fold higher risk for DVT compared to the risk for PE, in accordance with the yearly incidence of DVT and PE in the general population in Europe and the United States [50,51]. Various studies suggest that there is a 50% chance for patients with untreated proximal DVT to develop symptomatic PE within 3 months, and that in patients with superficial vein thrombosis, concomitant DVT and PE are prevalent in 18.1% and 6.9% of them, respectively [52,53]. Furthermore, the risk for VTE in patients with IBD was not influenced by sex, despite several reports demonstrating a higher risk in men [54,55]. Finally, a greater risk for VTE, as well as for DVT and PE, was found in patients with UC and CD, similar to that of the total IBD population.
In total, 2 meta-analyses have been published previously regarding the risk of VTE in patients with IBD. Fumery et al described an elevated risk of VTE in patients with IBD (RR 1.96, 95%CI 1.67-2.30) [12]. Yuhara et al, on the other hand, described an even greater risk of VTE in IBD patients (RR 2.20, 95%CI 1.83-2.65) [14]. The slight discrepancy in the size estimates between the previous meta-analyses and this study lies in the fact that different inclusion and exclusion criteria were used. In contrast to the previously published studies, we specifically excluded articles that included solely postoperative patients or pregnant women with IBD, to avoid selection bias. In general, pregnant women develop VTE 4-5 times more frequently than non-pregnant women [56,57], while a recent meta-analysis estimated the VTE risk in pregnant women with IBD to be 10-fold higher than that of non-pregnant ones without IBD [13]. Furthermore, major surgery has been proven to be a strong risk factor for VTE [58]. In addition, we excluded a study by Bernstein et al, included in the other meta-analyses [39], because it did not satisfy our inclusion criteria; in particular, the frequencies of VTE events in both the IBD population and the controls were not reported in the original study, while there was no overall risk estimate of VTE in patients with IBD; only age- and sex-specific comorbidity rates were reported.
There is a long-standing debate about the prevention methods and treatment options of VTE in patients with IBD. According to recent consensus statements regarding the prevention and treatment of VTE in patients with IBD [59], moderate to severe disease activity increases the risk of VTE and thus should be considered as a provoking factor. It is alarming that up to date, inadequate use of anticoagulants for VTE prophylaxis in IBD has been reported [60,61], and is mainly attributed to: (1) gastroenterologists’ lack of awareness of both the increased risk of VTE in IBD patients and the recommended use of pharmacological prophylaxis in hospitalized IBD patients [62]; and (2) concerns about the safety of anticoagulant drugs in patients with active IBD [63].
Pathophysiologic mechanisms that could explain the increased risk of thromboembolism in IBD have not yet been fully elucidated. Several studies have shown that glucocorticoid use in the setting of increased inflammatory activity, such as in patients with IBD, increases clotting factor levels and levels of plasminogen activator inhibitor-1, suggesting that glucocorticoid-induced alterations in fibrinolysis may contribute to the presence of a hypercoagulable state [64,65]. Moreover, emerging data indicate that neutrophil extracellular traps (NETs) expressing active tissue factor [66] are crucially implicated in the pathogenesis of various thromboinflammatory disorders [67-69]. A recent study pointed out that the local inflammatory response in the colon and peripheral blood in active UC was characterized by the presence of NETs carrying bioactive interleukin-1b and thrombogenic tissue factor, which could be responsible for the higher frequency of thrombosis in those patients than in healthy individuals [70]. Clinical studies have revealed an increased platelet count (reactive thrombocytosis) in IBD patients, proposed as a biomarker of disease activity in human IBD [71]. In addition, thrombocytosis appears to be accompanied by the presence of immature platelets in blood, suggesting that this response to IBD is linked to accelerated thrombopoiesis [72,73]. The intrinsic coagulation pathway can be activated by NETs released by polymorphonuclear neutrophils (PMNs) in a process called NETosis. NETs activate platelets as well as the complement system (C3a, C5a) and release proteases that inactivate endogenous anticoagulants. Platelets secrete alpha granules that recruit PMNs and macrophages, while stimulating PMNs to undergo NETosis, which in turn reactivates platelets, creating a feedback loop (platelet-mediated NET-driven thrombogenicity). They also activate the coagulation pathway by assembling enzyme–cofactor–substrate complexes on their exposed surface [74-76]. Clinical evaluation and interpretation of these findings could be promising, in order to develop novel diagnostic and therapeutic targets for clinically active IBD patients with an increased risk of immunothrombosis.
Several limitations of this study must be acknowledged. First of all, since no randomized controlled trials have been performed to explore the association between VTE and IBD, our meta-analysis included only observational studies, which are often susceptible to selection bias and may fail to take into account several potential confounders for the risk factor under investigation [77]. Second, significant heterogeneity (>90%) was observed among studies. That could be attributed to a variety of factors, such as different population characteristics of the included studies: 1) some studies were population-based cohorts, while in others data were abstracted from hospitalized patients or referral centers; and 2) studies had different follow-up periods and variability in the disease phenotype of IBD among patients. Although IBD severity, colonic involvement and extent of disease have been proven to correlate with VTE risk [45,46], not enough studies provided sufficient information on disease location or disease characteristics and severity, so we were not able to further analyze these factors. Third, since VTE is frequently diagnosed post mortem [78], some degree of differential misclassification of outcomes is to be expected in the studies of this meta-analysis. Finally, we cannot rule out that we omitted relevant articles by having imposed the English language as a filter on our search.
To conclude, patients with IBD carry a 2-fold greater risk of VTE compared to non-IBD subjects; it is therefore of utmost importance to increase gastroenterologists’ awareness of the primary prevention of VTE in this group of patients. Further, adequately conducted prospective cohort studies as well as randomized trials are warranted to provide more robust data regarding risk differences among certain subgroups.
Summary Box.
What is already known:
Inflammatory bowel disease (IBD) is responsible for a multitude of extraintestinal manifestations, including thromboembolic events that significantly increase morbidity and mortality
Thromboembolic events in patients with IBD are often missed, given the fact that the prevalence of thrombosis varies between 1.3% and 7.7% in patients with IBD, and the rate rises to 39-41% in autopsy series
The exact risk estimate of venous thromboembolism (VTE) in the IBD population still remains ambiguous, because of methodological differences and heterogeneity across published studies
What the new findings are:
The overall risk of VTE was found to be 2.03 times higher in the IBD group compared to the non-IBD control group
The risk of VTE in IBD was moderately increased after adjusting for smoking and body mass index, indicating that, when considered together, these factors could act as confounders in the relationship between IBD and VTE
Patients with IBD demonstrated an almost 2-fold higher risk for deep venous thrombosis compared to the risk for pulmonary embolism
Biography
University of Thessaly, School of Medicine, Larissa, Greece; AHEPA University Hospital, Aristotle University of Thessaloniki, Greece; University Hospital of Muenster, Muenster, Germany; Aristotle University of Thessaloniki, Hippokratio Hospital, Thessaloniki, Greece
Footnotes
Conflict of Interest: Alexandra Arvanitaki is the recipient of the International Training and Research “EMAH Stiftung Karla Voellm” Scholarship, Krefeld, Germany. For the remaining authors none were declared
References
- 1.Danese S, Papa A, Saibeni S, Repici A, Malesci A, Vecchi M. Inflammation and coagulation in inflammatory bowel disease:The clot thickens. Am J Gastroenterol. 2007;102:174–186. doi: 10.1111/j.1572-0241.2006.00943.x. [DOI] [PubMed] [Google Scholar]
- 2.Murthy SK, Nguyen GC. Venous thromboembolism in inflammatory bowel disease:an epidemiological review. Am J Gastroenterol. 2011;106:713–718. doi: 10.1038/ajg.2011.53. [DOI] [PubMed] [Google Scholar]
- 3.Loftus EV., Jr Clinical epidemiology of inflammatory bowel disease:incidence, prevalence, and environmental influences. Gastroenterology. 2004;126:1504–1517. doi: 10.1053/j.gastro.2004.01.063. [DOI] [PubMed] [Google Scholar]
- 4.Talbot RW, Heppell J, Dozois RR, Beart RW., Jr Vascular complications of inflammatory bowel disease. Mayo Clin Proc. 1986;61:140–145. doi: 10.1016/s0025-6196(12)65200-8. [DOI] [PubMed] [Google Scholar]
- 5.Koutroubakis IE. Therapy insight:Vascular complications in patients with inflammatory bowel disease. Nat Clin Pract Gastroenterol Hepatol. 2005;2:266–272. doi: 10.1038/ncpgasthep0190. [DOI] [PubMed] [Google Scholar]
- 6.Owczarek D, Cibor D, Głowacki MK, Rodacki T, Mach T. Inflammatory bowel disease:epidemiology, pathology and risk factors for hypercoagulability. World J Gastroenterol. 2014;20:53–63. doi: 10.3748/wjg.v20.i1.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sarlos P, Szemes K, Hegyi P, et al. Steroid but not biological therapy elevates the risk of venous thromboembolic events in inflammatory bowel disease:a meta-analysis. J Crohns Colitis. 2018;12:489–498. doi: 10.1093/ecco-jcc/jjx162. [DOI] [PubMed] [Google Scholar]
- 8.Spina L, Saibeni S, Battaglioli T, Peyvandi F, de Franchis R, Vecchi M. Thrombosis in inflammatory bowel diseases:role of inherited thrombophilia. Am J Gastroenterol. 2005;100:2036–2041. doi: 10.1111/j.1572-0241.2005.42029.x. [DOI] [PubMed] [Google Scholar]
- 9.Yan SL, Russell J, Harris NR, Senchenkova EY, Yildirim A, Granger DN. Platelet abnormalities during colonic inflammation. Inflamm Bowel Dis. 2013;19:1245–1253. doi: 10.1097/MIB.0b013e318281f3df. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Algahtani FH, Farag YM, Aljebreen AM, et al. Thromboembolic events in patients with inflammatory bowel disease. Saudi J Gastroenterol. 2016;22:423–427. doi: 10.4103/1319-3767.195558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Twig G, Zandman-Goddard G, Szyper-Kravitz M, Shoenfeld Y. Systemic thromboembolism in inflammatory bowel disease:mechanisms and clinical applications. Ann N Y Acad Sci. 2005;1051:166–173. doi: 10.1196/annals.1361.058. [DOI] [PubMed] [Google Scholar]
- 12.Fumery M, Xiaocang C, Dauchet L, Gower-Rousseau C, Peyrin-Biroulet L, Colombel JF. Thromboembolic events and cardiovascular mortality in inflammatory bowel diseases:a meta-analysis of observational studies. J Crohns Colitis. 2014;8:469–479. doi: 10.1016/j.crohns.2013.09.021. [DOI] [PubMed] [Google Scholar]
- 13.Kim YH, Pfaller B, Marson A, Yim HW, Huang V, Ito S. The risk of venous thromboembolism in women with inflammatory bowel disease during pregnancy and the postpartum period:A systematic review and meta-analysis. Medicine (Baltimore) 2019;98:e17309. doi: 10.1097/MD.0000000000017309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yuhara H, Steinmaus C, Corley D, et al. Meta-analysis:the risk of venous thromboembolism in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2013;37:953–962. doi: 10.1111/apt.12294. [DOI] [PubMed] [Google Scholar]
- 15.Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology:a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–2012. doi: 10.1001/jama.283.15.2008. [DOI] [PubMed] [Google Scholar]
- 17.Arvanitakis K, Arvanitaki A, Karkos C. The risk of venous thromboembolic events in patients with inflammatory bowel disease:A systematic review and meta-analysis. PROSPERO. 2020. [Accessed 4 April 2021]. p. CRD42020204404. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020204404 . [DOI] [PMC free article] [PubMed]
- 18.Fineout-Overholt E, Johnston L. Teaching EBP:asking searchable, answerable clinical questions. Worldviews Evid Based Nurs. 2005;2:157–160. doi: 10.1111/j.1741-6787.2005.00032.x. [DOI] [PubMed] [Google Scholar]
- 19.Annese V, Daperno M, Rutter MD, et al. European Crohn's and Colitis Organisation. European evidence based consensus for endoscopy in inflammatory bowel disease. J Crohns Colitis. 2013;7:982–1018. doi: 10.1016/j.crohns.2013.09.016. [DOI] [PubMed] [Google Scholar]
- 20.Dignass A, Van Assche G, Lindsay JO, et al. European Crohn's and Colitis Organisation (ECCO). The second European evidence-based Consensus on the diagnosis and management of Crohn's disease:Current management. J Crohns Colitis. 2010;4:28–62. doi: 10.1016/j.crohns.2009.12.002. [DOI] [PubMed] [Google Scholar]
- 21.Magro F, Langner C, Driessen A, et al. European Crohn's and Colitis Organisation (ECCO). European consensus on the histopathology of inflammatory bowel disease. J Crohns Colitis. 2013;7:827–851. doi: 10.1016/j.crohns.2013.06.001. [DOI] [PubMed] [Google Scholar]
- 22.Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle–Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2019. [Accessed 4 April 2021]. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp .
- 23.Altman DG. Confidence intervals for the number needed to treat. BMJ. 1998;317:1309–1312. doi: 10.1136/bmj.317.7168.1309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nurminen M. To use or not to use the odds ratio in epidemiologic analyses? Eur J Epidemiol. 1995;11:365–371. doi: 10.1007/BF01721219. [DOI] [PubMed] [Google Scholar]
- 25.Stare J, Maucort-Boulch D. Odds ratio, hazard ratio and relative risk. Metodološki zvezki. 2016;13:59–67. [Google Scholar]
- 26.Cochran WG. The combination of estimates from different experiments. Biometrics. 1954;10:101–129. [Google Scholar]
- 27.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Higgins JPT TJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed. Chichester (UK): John Wiley &Sons; 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bhandari S, Saeian K, Stein D. Increased rate of venous thromboembolism in hospitalized inflammatory bowel disease patients with Clostridium difficile infection. Inflamm Bowel Dis. 2018;24:661. doi: 10.1093/ibd/izx069. [DOI] [PubMed] [Google Scholar]
- 31.Grip O, Svensson PJ, Lindgren S. Inflammatory bowel disease promotes venous thrombosis earlier in life. Scand J Gastroenterol. 2000;35:619–623. doi: 10.1080/003655200750023589. [DOI] [PubMed] [Google Scholar]
- 32.Merrill A, Millham F. Increased risk of postoperative deep vein thrombosis and pulmonary embolism in patients with inflammatory bowel disease:a study of National Surgical Quality Improvement Program patients. Arch Surg. 2012;147:120–124. doi: 10.1001/archsurg.2011.297. [DOI] [PubMed] [Google Scholar]
- 33.Nguyen GC, Boudreau H, Harris ML, Maxwell CV. Outcomes of obstetric hospitalizations among women with inflammatory bowel disease in the United States. Clin Gastroenterol Hepatol. 2009;7:329–334. doi: 10.1016/j.cgh.2008.10.022. [DOI] [PubMed] [Google Scholar]
- 34.Yarur AJ, Deshpande AR, Pechman DM, Tamariz L, Abreu MT, Sussman DA. Inflammatory bowel disease is associated with an increased incidence of cardiovascular events. Am J Gastroenterol. 2011;106:741–747. doi: 10.1038/ajg.2011.63. [DOI] [PubMed] [Google Scholar]
- 35.Zöller B, Ohlsson H, Waehrens R, Sundquist J, Sundquist K. Association of irritable bowel syndrome and venous thromboembolism. Scand J Gastroenterol. 2018;53:784–789. doi: 10.1080/00365521.2018.1465118. [DOI] [PubMed] [Google Scholar]
- 36.Kuy S, Dua A, Chappidi R, et al. The increasing incidence of thromboembolic events among hospitalized patients with inflammatory bowel disease. Vascular. 2015;23:260–264. doi: 10.1177/1708538114541799. [DOI] [PubMed] [Google Scholar]
- 37.Kappelman MD, Horvath-Puho E, Sandler RS, et al. Thromboembolic risk among Danish children and adults with inflammatory bowel diseases:a population-based nationwide study. Gut. 2011;60:937–943. doi: 10.1136/gut.2010.228585. [DOI] [PubMed] [Google Scholar]
- 38.Huerta C, Johansson S, Wallander MA, García Rodríguez LA. Risk factors and short-term mortality of venous thromboembolism diagnosed in the primary care setting in the United Kingdom. Arch Intern Med. 2007;167:935–943. doi: 10.1001/archinte.167.9.935. [DOI] [PubMed] [Google Scholar]
- 39.Bernstein CN, Nabalamba A. Hospitalization-based major comorbidity of inflammatory bowel disease in Canada. Can J Gastroenterol. 2007;21:507–511. doi: 10.1155/2007/924257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bernstein CN, Blanchard JF, Houston DS, Wajda A. The incidence of deep venous thrombosis and pulmonary embolism among patients with inflammatory bowel disease:a population-based cohort study. Thromb Haemost. 2001;85:430–434. [PubMed] [Google Scholar]
- 41.Chu TPC, Grainge MJ, Card TR. The risk of venous thromboembolism during and after hospitalisation in patients with inflammatory bowel disease activity. Aliment Pharmacol Ther. 2018;48:1099–1108. doi: 10.1111/apt.15010. [DOI] [PubMed] [Google Scholar]
- 42.Chung WS, Lin CL, Hsu WH, Kao CH. Inflammatory bowel disease increases the risks of deep vein thrombosis and pulmonary embolism in the hospitalized patients:a nationwide cohort study. Thromb Res. 2015;135:492–496. doi: 10.1016/j.thromres.2014.12.025. [DOI] [PubMed] [Google Scholar]
- 43.Grainge MJ, West J, Card TR. Venous thromboembolism during active disease and remission in inflammatory bowel disease:a cohort study. Lancet. 2010;375:657–663. doi: 10.1016/S0140-6736(09)61963-2. [DOI] [PubMed] [Google Scholar]
- 44.Ha C, Magowan S, Accortt NA, Chen J, Stone CD. Risk of arterial thrombotic events in inflammatory bowel disease. Am J Gastroenterol. 2009;104:1445–1451. doi: 10.1038/ajg.2009.81. [DOI] [PubMed] [Google Scholar]
- 45.Miehsler W, Reinisch W, Valic E, et al. Is inflammatory bowel disease an independent and disease specific risk factor for thromboembolism? Gut. 2004;53:542–548. doi: 10.1136/gut.2003.025411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Nguyen GC, Sam J. Rising prevalence of venous thromboembolism and its impact on mortality among hospitalized inflammatory bowel disease patients. Am J Gastroenterol. 2008;103:2272–2280. doi: 10.1111/j.1572-0241.2008.02052.x. [DOI] [PubMed] [Google Scholar]
- 47.Rothberg MB, Lindenauer PK, Lahti M, Pekow PS, Selker HP. Risk factor model to predict venous thromboembolism in hospitalized medical patients. J Hosp Med. 2011;6:202–209. doi: 10.1002/jhm.888. [DOI] [PubMed] [Google Scholar]
- 48.Saleh T, Matta F, Yaekoub AY, Danescu S, Stein PD. Risk of venous thromboembolism with inflammatory bowel disease. Clin Appl Thromb Hemost. 2011;17:254–258. doi: 10.1177/1076029609360528. [DOI] [PubMed] [Google Scholar]
- 49.Weng MT, Park SH, Matsuoka K, et al. Incidence and risk factor analysis of thromboembolic events in East Asian patients with inflammatory bowel disease, a multinational collaborative study. Inflamm Bowel Dis. 2018;24:1791–1800. doi: 10.1093/ibd/izy058. [DOI] [PubMed] [Google Scholar]
- 50.Cohen AT, Agnelli G, Anderson FA, et al. VTE Impact Assessment Group in Europe (VITAE). Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost. 2007;98:756–764. doi: 10.1160/TH07-03-0212. [DOI] [PubMed] [Google Scholar]
- 51.Anderson FA, Jr, Zayaruzny M, Heit JA, Fidan D, Cohen AT. Estimated annual numbers of US acute-care hospital patients at risk for venous thromboembolism. Am J Hematol. 2007;82:777–782. doi: 10.1002/ajh.20983. [DOI] [PubMed] [Google Scholar]
- 52.Di Minno MN, Ambrosino P, Ambrosini F, Tremoli E, Di Minno G, Dentali F. Prevalence of deep vein thrombosis and pulmonary embolism in patients with superficial vein thrombosis:a systematic review and meta-analysis. J Thromb Haemost. 2016;14:964–972. doi: 10.1111/jth.13279. [DOI] [PubMed] [Google Scholar]
- 53.Moheimani F, Jackson DE. Venous thromboembolism:classification, risk factors, diagnosis, and management. ISRN Hematol. 2011;2011:124610. doi: 10.5402/2011/124610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Silverstein MD, Heit JA, Mohr DN, Petterson TM, O'Fallon WM, Melton LJ., 3rd Trends in the incidence of deep vein thrombosis and pulmonary embolism:a 25-year population-based study. Arch Intern Med. 1998;158:585–593. doi: 10.1001/archinte.158.6.585. [DOI] [PubMed] [Google Scholar]
- 55.Naess IA, Christiansen SC, Romundstad P, Cannegieter SC, Rosendaal FR, Hammerstrøm J. Incidence and mortality of venous thrombosis:a population-based study. J Thromb Haemost. 2007;5:692–699. doi: 10.1111/j.1538-7836.2007.02450.x. [DOI] [PubMed] [Google Scholar]
- 56.Heit JA, Kobbervig CE, James AH, Petterson TM, Bailey KR, Melton LJ., 3rd Trends in the incidence of venous thromboembolism during pregnancy or postpartum:a 30-year population-based study. Ann Intern Med. 2005;143:697–706. doi: 10.7326/0003-4819-143-10-200511150-00006. [DOI] [PubMed] [Google Scholar]
- 57.Virkus RA, Løkkegaard EC, Bergholt T, Mogensen U, Langhoff-Roos J, Lidegaard Ø. Venous thromboembolism in pregnant and puerperal women in Denmark 1995-2005. A national cohort study. Thromb Haemost. 2011;106:304–309. doi: 10.1160/TH10-12-0823. [DOI] [PubMed] [Google Scholar]
- 58.Lobastov K, Barinov V, Schastlivtsev I, Laberko L, Rodoman G, Boyarintsev V. Validation of the Caprini risk assessment model for venous thromboembolism in high-risk surgical patients in the background of standard prophylaxis. J Vasc Surg Venous Lymphat Disord. 2016;4:153–160. doi: 10.1016/j.jvsv.2015.09.004. [DOI] [PubMed] [Google Scholar]
- 59.Nguyen GC, Bernstein CN, Bitton A, et al. Consensus statements on the risk, prevention, and treatment of venous thromboembolism in inflammatory bowel disease:Canadian Association of Gastroenterology. Gastroenterology. 2014;146:835–848. doi: 10.1053/j.gastro.2014.01.042. [DOI] [PubMed] [Google Scholar]
- 60.Kaddourah O, Numan L, Jeepalyam S, Abughanimeh O, Ghanimeh MA, Abuamr K. Venous thromboembolism prophylaxis in inflammatory bowel disease flare-ups. Ann Gastroenterol. 2019;32:578–583. doi: 10.20524/aog.2019.0412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Dwyer JP, Javed A, Hair CS, Moore GT. Venous thromboembolism and underutilisation of anticoagulant thromboprophylaxis in hospitalised patients with inflammatory bowel disease. Intern Med J. 2014;44:779–784. doi: 10.1111/imj.12488. [DOI] [PubMed] [Google Scholar]
- 62.Papa A, Gerardi V, Marzo M, Felice C, Rapaccini GL, Gasbarrini A. Venous thromboembolism in patients with inflammatory bowel disease:focus on prevention and treatment. World J Gastroenterol. 2014;20:3173–3179. doi: 10.3748/wjg.v20.i12.3173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Tinsley A, Naymagon S, Trindade AJ, Sachar DB, Sands BE, Ullman TA. A survey of current practice of venous thromboembolism prophylaxis in hospitalized inflammatory bowel disease patients in the United States. J Clin Gastroenterol. 2013;47:e1–e6. doi: 10.1097/MCG.0b013e31824c0dea. [DOI] [PubMed] [Google Scholar]
- 64.van Zaane B, Nur E, Squizzato A, et al. Systematic review on the effect of glucocorticoid use on procoagulant, anti-coagulant and fibrinolytic factors. J Thromb Haemost. 2010;8:2483–2493. doi: 10.1111/j.1538-7836.2010.04034.x. [DOI] [PubMed] [Google Scholar]
- 65.Johannesdottir SA, Horváth-Puhó E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism:a nationwide population-based case-control study. JAMA Intern Med. 2013;173:743–752. doi: 10.1001/jamainternmed.2013.122. [DOI] [PubMed] [Google Scholar]
- 66.Boeltz S, Amini P, Anders HJ, et al. To NET or not to NET:current opinions and state of the science regarding the formation of neutrophil extracellular traps. Cell Death Differ. 2019;26:395–408. doi: 10.1038/s41418-018-0261-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Chrysanthopoulou A, Kambas K, Stakos D, et al. Interferon lambda1/IL-29 and inorganic polyphosphate are novel regulators of neutrophil-driven thromboinflammation. J Pathol. 2017;243:111–122. doi: 10.1002/path.4935. [DOI] [PubMed] [Google Scholar]
- 68.Kambas K, Chrysanthopoulou A, Vassilopoulos D, et al. Tissue factor expression in neutrophil extracellular traps and neutrophil derived microparticles in antineutrophil cytoplasmic antibody associated vasculitis may promote thromboinflammation and the thrombophilic state associated with the disease. Ann Rheum Dis. 2014;73:1854–1863. doi: 10.1136/annrheumdis-2013-203430. [DOI] [PubMed] [Google Scholar]
- 69.Papay P, Miehsler W, Tilg H, et al. Clinical presentation of venous thromboembolism in inflammatory bowel disease. J Crohns Colitis. 2013;7:723–729. doi: 10.1016/j.crohns.2012.10.008. [DOI] [PubMed] [Google Scholar]
- 70.Angelidou I, Chrysanthopoulou A, Mitsios A, et al. REDD1/autophagy pathway is associated with neutrophil-driven IL-1b inflammatory response in active ulcerative colitis. J Immunol. 2018;200:3950–3961. doi: 10.4049/jimmunol.1701643. [DOI] [PubMed] [Google Scholar]
- 71.Heits F, Stahl M, Ludwig D, Stange EF, Jelkmann W. Elevated serum thrombopoietin and interleukin-6 concentrations in thrombocytosis associated with inflammatory bowel disease. J Interferon Cytokine Res. 1999;19:757–760. doi: 10.1089/107999099313604. [DOI] [PubMed] [Google Scholar]
- 72.Harries AD, Fitzsimons E, Fifield R, Dew MJ, Rhoades J. Platelet count:a simple measure of activity in Crohn's disease. Br Med J (Clin Res Ed) 1983;286:1476. doi: 10.1136/bmj.286.6376.1476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Nielsen OH, Vainer B, Madsen SM, Seidelin JB, Heegaard NH. Established and emerging biological activity markers of inflammatory bowel disease. Am J Gastroenterol. 2000;95:359–367. doi: 10.1111/j.1572-0241.2000.t01-1-01790.x. [DOI] [PubMed] [Google Scholar]
- 74.Kambas K, Markiewski MM, Pneumatikos IA, et al. C5a and TNF-alpha up-regulate the expression of tissue factor in intra-alveolar neutrophils of patients with the acute respiratory distress syndrome. J Immunol. 2008;180:7368–7375. doi: 10.4049/jimmunol.180.11.7368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Ritis K, Doumas M, Mastellos D, et al. A novel C5a receptor-tissue factor cross-talk in neutrophils links innate immunity to coagulation pathways. J Immunol. 2006;177:4794–4802. doi: 10.4049/jimmunol.177.7.4794. [DOI] [PubMed] [Google Scholar]
- 76.Walsh PN. Platelet coagulation-protein interactions. Semin Thromb Hemost. 2004;30:461–471. doi: 10.1055/s-2004-833481. [DOI] [PubMed] [Google Scholar]
- 77.Hammer GP, du Prel JB, Blettner M. Avoiding bias in observational studies:part 8 in a series of articles on evaluation of scientific publications. Dtsch Arztebl Int. 2009;106:664–668. doi: 10.3238/arztebl.2009.0664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Stein PD, Henry JW. Prevalence of acute pulmonary embolism among patients in a general hospital and at autopsy. Chest. 1995;108:978–981. doi: 10.1378/chest.108.4.978. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.