

Abstract
Introduction:
Association between oral health and rheumatoid arthritis is well established. Oral health-related quality of life was determined in patients diagnosed with rheumatoid arthritis (RA).
Materials and Methods:
This study was conducted among 45 patients (males 25 and female 20) (Group I) of RA and 45 healthy participants as control (Group II). Disease activity score 28 test, health assessment questionnaire (HAQ), and general oral health assessment index (GOHAI) questionnaire were applied.
Results:
The mean HAQ score in Group I was 1.14 and in Group II was 0.36. The mean GOHAI score in Group I was 36.4 and in Group II was 52.8. The mean HAQ in males was 0.94 and in females was 34.6. The mean GOHAI in males was 12.6 and in females was 38.2. In Group I, there were 15 patients with HAQ level 1 and 30 with HAQ level 2 and in Group II was 40 with HAQ levels 1 and 5 with HAQ level 2. In Group I, 42 had Dt GOHAI = 0 and 3 had Dt GOHAI = 1 and in Group II, 10 had Dt GOHAI = 0 and 35 had Dt GOHAI = 1. The difference was statistically significant (P < 0.05). There was a statistically significant difference in the mean value of HAQ and GOHAI in degree of disease activity (P < 0.05). There was an increase in HAQ and decreases GOHAI scores with the deterioration of disease. There was a correlation between age and involved joints with HAQ and inverse relationship between age and involved joints with GOHAI.
Conclusion:
Authors found that RA patients had poor oral health quality of life. It was found that aging and with the deterioration of disease, GOHAI, and the oral health quality of life of patients decreased.
KEYWORDS: General oral health assessment index, health assessment questionnaire, rheumatoid arthritis
INTRODUCTION
Rheumatoid arthritis (RA) is autoimmune disease which is highly prevalent nowadays. It is inflammatory in origin affecting joints. It is commonly encountered in both genders; however, female prevalence is three times higher than males.[1] The prevalence rate of RA is 0.5%–1%. Commonly affecting the age group is third to fifth decades of life. The exact cause of RA is not well known. The role of genetics and environmental factors is highly appreciated. Inflammation of joints may result from triggering factors such as infection and autoimmunity.[2]
It is also evident that various cytokines, growth factors, immune cell types, and proteinases lead to interactions which promote joint destruction and systemic complications. Patients complain of pain, stiffness, and swelling of both major and minor joints. There is symmetrical bilateral involvement of joints. Long-standing disease induces deformation, functional restriction and reduction in routine daily activities, and deteriorating quality of life. The onset of disease is insidious and the involvement of joints is seen in months. Weakness and fatigue are common complaints of patients.[3]
Periodontitis is the destruction of periodontium, which subsequent bone loss, tooth mobility, and ultimately loss of teeth. Recent literature highlights the relationship between RA and periodontitis. It is evident that RA may developed from patients with periodontal breakdown.[4] Periodontium may be exacerbated by RA and similarly, periodontitis can degrade the inflammation status of RA. Patients possess compromised quality of life. Oral health-related quality of life (OHRQOL) is affected. General oral health assessment index (GOHAI) is widely employed to determine the quality of life as well as dental diseases in the elderly.[5] The present study was conducted to determine OHRQOL in patients with RA.
MATERIALS AND METHODS
This questionnaire study was conducted among 45 patients (males 25 and female 20) (Group I) diagnosed clinically as well as radiologically of RA involving both genders. Equal number of healthy participants was taken as control (Group II). The study was commenced after obtaining ethical clearance from the ethical committee with the consent of the patients obtained in vernacular language.
Demographic data of each patients were recorded in case history proforma. Laboratory investigations such as complete blood count, C-reactive protein level, and erythrocyte sedimentation rate were performed. A thorough clinical examination was performed. Disease activity score 28 (DAS28) test was also applied to all patients which was recorded as disease in remission mode (DAS28 <3.2), moderate (DAS28 ≤5.1 ≥3.2), and active (DAS28 >5.1). Daily routine activities such as dressing, walking, working out, cleaning, and doing homework were determine with the help of the health assessment questionnaire (HAQ) (20 questions). A score of 0 was designated in patients with no problem, one to few problems, two to many problems, and three to inability to do activity. Patients were also subjected to GOHAI questionnaire (12 questions) with five options: never = 5, rarely = 4, sometimes = 3, often = 2, and always = 1. The score ranged from 60 to 12. Add-GOHAI scores were classified into two groups: Dt GOHAI = 0 (Add GOHAI ≤50) having poor quality of life and Dt-GOHAI = 1 (Add-GOHAI ≥50) having moderate to a high quality of life. Results were tabulated and statistically analyzed with a significance level set below 0.05.
RESULTS
Table 1 shows that the mean HAQ score in Group I was 1.14 and in Group II was 0.36. The mean GOHAI score in Group I was 36.4 and in Group II was 52.8 (P < 0.05).
Table 1.
Assessment of health assessment questionnaire and general oral health assessment index score in both groups
| Score system | Group I (RA) | Group II (Control) | P |
|---|---|---|---|
| HAQ | 1.14 | 0.36 | 0.01 |
| GOHAI | 36.4 | 52.8 | 0.03 |
HAQ: Health assessment questionnaire, GOHAI: General oral health assessment index, RA: Rheumatoid arthritis
Graph 1 shows that the mean HAQ in males was 0.94 and in females was 34.6. The mean GOHAI in males was 12.6 and in females was 38.2 (P > 0.05).
Graph 1.
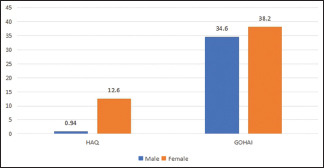
Assessment of health assessment questionnaire and general oral health assessment index score in both genders
Table 2 shows that in Group I, there were 15 patients with HAQ level 1 and 30 with HAQ level 2 and in Group II was 40 with HAQ level 1 and 5 with HAQ level 2. In Group I, 42 had Dt GOHAI = 0 and 3 had Dt GOHAI = 1 and in Group II, 10 had Dt GOHAI = 0 and 35 had Dt GOHAI = 1. The difference was statistically significant (P < 0.05).
Table 2.
Levels of quality of life indicators in both groups
| Score system | Group I | Group II | P |
|---|---|---|---|
| HAQ | |||
| Level 1 | 15 | 40 | 0.02 |
| Level 2 | 30 | 5 | |
| GOHAI | |||
| Dt GOHAI=0 | 42 | 10 | 0.01 |
| Dt-GOHAI=1 | 3 | 35 |
HAQ: Health assessment questionnaire, GOHAI: General oral health assessment index
Graph 2 shows that there was a significant difference in the mean value of HAQ and GOHAI in terms of disease activity (P < 0.05). Deterioration of disease increases HAQ and decreases the GOHAI score.
Graph 2.
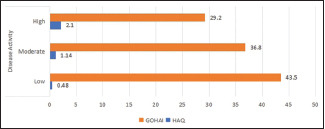
Oral health-related quality of life and disease activity in both groups
Table 3 shows that there was a correlation between age and involved joints with HAQ and inverse relationship between age and involved joints with GOHAI.
Table 3.
Correlation between the indicators of quality of life and age and the number of involved joints
| Indicator | Age (r, P) | Involved joints (r, P) |
|---|---|---|
| HAQ | 0.51, 0.01 | 0.53, 0.01 |
| GOHAI | 0.32, 0.02 | 0.56, 0.01 |
HAQ: Health assessment questionnaire, GOHAI: General oral health assessment index
DISCUSSION
RA is a leading inflammatory disease with limitation of routine daily activities such as walking, difficulty in standing, and swelling of joints. RA progresses to synovitis due to the accumulation of pro-inflammatory cells in the synovial membrane, degradation of cartilage, and musculoskeletal tissue. Several studies have mentioned the occurrence of antibodies against Porphyromonas gingivalis in RA patients and in patients with chronic periodontitis citrullinated proteins and their antibodies and association between anti-P. gingivalis and periodontal parameters, and the titers of rheumatoid factor and antibodies anticyclic citrullinated peptide, which were also related to the severity of PD.[6,7]
Dental and oral diseases significantly affect the quality of life. It has a great impact on mental as well as on the physical health of person. RA leads to difficulty in eating, speaking, swallowing, and tasting due to the involvement of the temporomandibular joint (TMJ). There are muscular pain, popping, and crepitus sound during mouth opening or closing. TMJ is tender on palpation and patients avoid opening the mouth. Failure to do routine oral activities accelerates plaque accumulation over teeth, which subsequently leads to periodontitis. Patients with RA experience a lack of self-confidence and have compromised quality of life and short the life expectancy.[8] The present study was conducted to determine OHRQOL in RA patients.
In the present study, we enrolled 45 patients of RA in Group I and 45 healthy participants in Group II. We found that the mean HAQ score in Group I was 1.14 and in Group II was 0.36. The mean GOHAI score in Group I was 36.4 and in Group II was 52.8. Nosratzehi et al.[9] conducted a study on eighty patients of RA and eighty healthy control. The mean of HAQ score was 1.17 ± 0.89 in RA patients and 0.35 ± 0.12 in control. The mean of GOHAI score in patients was 37.46 ± 9.53 and in control was 53.21 ± 11.35. It was found that the HAQ score (≥1) was seen in 62.5% and the GOHAI score (≤50) was seen in 91.2%.
We found that the mean HAQ in males was 0.94 and in females was 34.6. The mean GOHAI in males was 12.6 and in females was 38.2. Iikuni et al.[10] in their study found that the mean score of HAQ in females was significantly higher than that of males as observed in our study; however, the difference was non- significant. The difference in HAQ and GOHAI scores between males and females may be due to etiology and sample size selection.
In Group I, there were 15 patients with HAQ level 1 and 30 with HAQ level 2 and in Group II was 40 with HAQ level 1 and 5 with HAQ level 2. In Group I, 42 had Dt GOHAI = 0 and 3 had Dt GOHAI = 1 and in Group II, 10 had Dt GOHAI = 0 and 35 had Dt GOHAI = 1. Gamal et al.[11] measured the quality of life with a 36-question QA questionnaire in RA patients. The result of the study demonstrated that educated and unemployed had poor quality of life and the rheumatoid factor was positive and higher disease activity was significantly lower in patients with >5 years of disease.
In this study, we found that HAQ and GOHAI in terms of disease activity (P < 0.05) exhibited significant difference. We observed increase HAQ level and decrease GOHAI score with disease deterioration. There was a correlation between age and involved joints with HAQ and inverse relationship between age and involved joints with GOHAI. This shows that with advancing age, there is more involvement of joints and difficulty in walking, using stairs, and sitting. Han et al.[12] in their study observed mean HAQ score of 76.6 ± 0.69 in RA patients was, and HAQ score ≥1 was seen in 42.2% of patients.
The shortcoming of the study is the small sample size. Follow-up of the patients was not performed.
CONCLUSION
The authors found that there was poor oral health quality of life in RA patients. With aging and disease deterioration, GOHAI and the oral health quality of life of patients decreased.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Pischon N, Pischon T, Kröger J, Gülmez E, Kleber BM, Bernimoulin JP, et al. Association among rheumatoid arthritis, oral hygiene, and periodontitis. J Periodontol. 2008;79:979–86. doi: 10.1902/jop.2008.070501. [DOI] [PubMed] [Google Scholar]
- 2.Monsarrat P, Vergnes JN, Blaizot A, Constantin A, de Grado GF, Ramambazafy H, et al. Oral health status in outpatients with rheumatoid arthritis: The OSARA study. Oral Health Dent Manag. 2014;13:113–9. [PubMed] [Google Scholar]
- 3.Ahola K, Saarinen A, Kuuliala A, Leirisalo-Repo M, Murtomaa H, Meurman JH. Impact of rheumatic diseases on oral health and quality of life. Oral Dis. 2015;21:342–8. doi: 10.1111/odi.12285. [DOI] [PubMed] [Google Scholar]
- 4.Blaizot A, Monsarrat P, Constantin A, Vergnes JN, de Grado GF, Nabet C, et al. Oral health-related quality of life among outpatients with rheumatoid arthritis. Int Dent J. 2013;63:145–53. doi: 10.1111/idj.12023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Slade GD, Strauss RP, Atchison KA, Kressin NR, Locker D, Reisine ST. Conference summary: Assessing oral health outcomes—measuring health status and quality of life. Community Dent Health. 1998;15:3–7. [PubMed] [Google Scholar]
- 6.Mikuls TR, Thiele GM, Deane KD, Payne JB, O’Dell JR, Yu F, et al. Porphyromonas gingivalis and disease-related autoantibodies in individuals at increased risk of rheumatoid arthritis. Arthritis Rheum. 2012;11:352230. doi: 10.1002/art.34595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nesse W, Westra J, van der Wal JE, Abbas F, Nicholas AP, Vissink A, et al. The periodontium of periodontitis patients contains citrullinated proteins which may play a role in ACPA (anti-citrullinated protein antibody) formation. J Clin Periodontol. 2012;39:599–607. doi: 10.1111/j.1600-051X.2012.01885.x. [DOI] [PubMed] [Google Scholar]
- 8.Tubert-Jeannin S, Riordan PJ, Morel-Papernot A, Porcheray S, Saby-Collet S. Validation of an oral health quality of life index (GOHAI) in France. Community Dent Oral Epidemiol. 2003;31:275–84. doi: 10.1034/j.1600-0528.2003.t01-1-00006.x. [DOI] [PubMed] [Google Scholar]
- 9.Nosratzehi T, Nosratzehi S, Nosratzehi M, Ghaleb I. Oral health-related quality of life in patients with rheumatoid arthritis. Open Access Rheumatol. 2019;11:309–13. doi: 10.2147/OARRR.S222607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Iikuni N, Sato E, Hoshi M, Inoue E, Taniguchi A, Hara M, et al. The influence of sex on patients with rheumatoid arthritis in a large observational cohort. J Rheumatol. 2009;36:508–11. doi: 10.3899/jrheum.080724. [DOI] [PubMed] [Google Scholar]
- 11.Gamal RM, Mahran SA, El Fetoh NA, Janbi F. Quality of life assessment in Egyptian rheumatoid arthritis patients: Relation to clinical features and disease activity. Egypt Rheumatol. 2016;38:65–70. [Google Scholar]
- 12.Han C, Li N, Peterson S. THU0043 minimal important difference in HAQ: A validation from health economic perspectives in patient with rheumatoid arthritis using real-world data from Adelphi database. Ann Rheum Dis. 2016;75:193. [Google Scholar]