

Abstract
Introduction:
Preventive oral health of a child is dependent on the parental knowledge toward caries control, care of deciduous tooth, use of space maintainers for malocclusion, and utilization of various procedures available for preventing oral diseases by oral health professionals. This study was aimed to assess the attitude and awareness of preventive dentistry among parents residing in Riyadh city, Kingdom of Saudi Arabia.
Methodology:
A cross-sectional, questionnaire study was conducted among 300 male parents. Questionnaire was sent through the use of social media, and responses were collected.
Results:
Seventy-four percent of male Saudi parents were aware of prevention of oral diseases. 38.45% of male parents were aware of preventive dentistry procedure, but preventive dentistry utilization rate was seen among 6% population only. Attitude toward the prevention of oral disease was statistically not significant according to the age group and income but statistically significant according to education. The utilization of preventive procedures was significant according to education and income (P < 0.05).
Conclusion:
Awareness about preventive dentistry was more among Saudi parents but utilization rate was directly correlated to their education and income. After The utilization of preventive procedures was significant according to education and income (P < 0.05).
KEYWORDS: Dental services, malocclusion, preventive procedures, primary teeth
INTRODUCTION
The main diseases of the oral cavity include dental caries and periodontitis which results from the activity of bacterial dental plaque. Dental plaque consists of many microorganisms colonized on tooth surfaces, especially on pit and fissures and along the gingival margin.[1] Dentists deal with carious lesions or previously treated caries lesions known as recurrent or secondary caries lesions.
One of the main reasons for tooth loss in primary teeth among in Saudi children is due to carious lesions in deciduous teeth.[2] Dental caries is increasing in Saudi Arabia due to change in lifestyle, increased sugar consumption, carbonated drinks, and improper oral hygiene maintenance.[3,4] A recent study conducted reported 83% of prevalence of dental caries in Riyadh.[5]
Many oral health conditions are preventable and can be treated in their early stages. Primary prevention aims at the initial stages, whereas secondary aims to stop disease progression.[6] Interception is done best at earliest or initial stages. Dental plaque can be prevented by reducing dietary sugar exposure and improving the resilience of the teeth. Routine dental check-up spaced at 6 months' interval is the best way toward the prevention of dental decay along with population focused prevention.
Children oral health largely depends on parents who make decisions for their child's dental therapy. There are various preventive procedures available for children such as topical and systemic fluorides, rematerializing dentifrices/chewing gums, pit and fissure sealants, fluoride varnish, mouth guards for protecting accidental injuries during contact sports, and also interceptive orthodontics to prevent malocclusion. These procedures require a professional guidance. Dental appliances which aid in guided jaw growth corrects minor problems but may affect at later stages.[7]
Early intervention prevents many diseases including oral diseases.[8] Preventive dentistry is the area of dentistry prevent the beginning or progression of oral disease. It starts from home dental care by patients, as well as professional care and education by dental staff in office or clinic.
Preventive dental care should begin from infancy, i.e., before the teeth appearance and throughout the life like for infants, cleaning gums after feeding, brushing and flossing in adolescence, and wearing custom-made mouth guards in contact sports.
Knowledge of parents about preventive dentistry procedures is essential for the utilization of the dental services.
Regarding the vaccination, diet and nutrition and prevention of injuries and accidents, parents are usually educated during their routine visit to hospital, whereas there is less information on oral health which make them to visit the dentist at a later stage of caries progression or malocclusion etc.
Parents feel or believe it's not worth to spend time/money on deciduous teeth as they will be shed anyway. Even in developed nations, curative treatments were the choice than preventive for their kids by parents. Hence, the present study was planned to check the parental awareness toward the prevention of oral diseases and awareness and utilization of preventive dentistry procedures among male parents at Riyadh Kingdom of Saudi Arabia.
METHODOLOGY
The present study assessed attitude toward the preventive oral health and awareness and utilization of preventive dentistry procedures among male parents at Riyadh, Saudi Arabia. A total of 350 questionnaires were sent through WhatsApp and Snap chat out of which 300 giving a response rate of 85.7%.
Study population
The study population comprised male Saudi parents who live in Riyadh city. Ethical clearance was obtained from Institutional Review Board of College of dentistry, Prince Sattam Bin Abdul-Aziz University. Informed consent was asked from the participants before the study. Those participants denying giving consent were excluded. The questionnaire was in the Arabic and English language. It was sent through the social media, i.e., WhatsApp, Snap chat and was asked people to send link to their friends and family after answering the questions. Questionnaire consisted of consent form those participants who did not agree were excluded from the survey.
Sample size
The sample size was calculated by using the following formula:

Where,
Z = 1.96 (confidence level or 5% level of significance).
P = positive attitude toward the prevention of oral diseases 75% = 0.75.
q = (1−p) 100–75 = 25% = 0.25.
d = Precision limit or proportion of sampling error which is usually 5% confidence limit = 0.05.
By substituting the values, sample size was found to be 288 which were rounded to 300.
Questionnaire
An anonymous, objective type questionnaire was requested to fill by parents without providing any information about preventive dentistry. Personal information (age and educational status), uses of fluoride, space maintainers, source of information, and utilization of preventive services were asked. Educational status included was secondary schooling, diploma graduate, degree graduate, and master degree graduate. Responses consisted of agree, disagree, and don't know for questions related to the prevention of oral diseases and for awareness about preventive dentistry procedures it was dichotomous response of yes or no.
Validation of questionnaire
To validate the questionnaire, questions were prepared in the English language initially and translated to the Arabic language, and it was back translated again to English.
Method
Questionnaire was sent to individual parents through the social media, i.e., WhatsApp and Snap chat which also had a consent form and explanation about the study.
Statistical analysis
Descriptive statistics were computed, and the data were analyzed statistically using the Chi-square test with 95% confidence interval, and P < 0.05 was considered statistically significant.
RESULTS
Table 1 shows the distribution of study population according to age group, educational status, and family income. Majority of the participants were belonging to 20–30 years of age group (39.7%). 51.3% of the participants had a Bachelor's degree. 39.3% of the study participants had a family income of 4000–10,000 SAR.
Table 1.
The distribution of study population according to age group, educational status, and income
| Study subjects | Parameters | Frequency (%) |
|---|---|---|
| Age group (years) | 23-30 | 103 (34.3) |
| 30-40 | 119 (39.7) | |
| 40-50 | 61 (20.3) | |
| <50 | 17 (5.7) | |
| Educational status | Not educated | 15 (5.0) |
| Up to secondary | 111 (37.0) | |
| Bachelor | 154 (51.3) | |
| Master | 16 (5.3) | |
| PhD | 4 (1.3) | |
| Income (SAR) | >4000 | 86 (28.7) |
| 4000-10,000 | 118 (39.3) | |
| 10,000-20,000 | 81 (27.0) | |
| <20,000 | 15 (5.0) |
SAR: Saudi riyal
Table 2 shows attitude of Saudi parents toward preventive oral health 81.7% of study subjects have stated that primary teeth are important for child's health. 68.7% of parents agreed that problem in deciduous teeth will affect permanent teeth. Sixty-seven percent agreed that oral health affects general health. 79.7% of population agreed for fluoridated toothpaste helps in preventing tooth decay. Ninety-five percent of parents reported that they have a role in developing a child's dental attitude. 65.7% of study subject thinks that visiting a dentist as early as possible is important. 90.3% of parents think that correct method of brushing can prevent dental decay. Only 41.3% of subjects agreed malocclusion can be preventable whereas 45% reported that they don't know. Majority of the questions were not statistically significant according to age group and income. Whereas majority of questions are statistically significant according to education [Table 2].
Table 2.
Responses of Saudi parents toward preventive oral health
| Questions | Response | Frequency (%) | Age (χ2, P) | Education (χ2, P) | Income (χ2, P) |
|---|---|---|---|---|---|
| Primary teeth are important for child’s health | Agree | 245 (81.7) | 7.73, 0.25 (NS) | 14.90, 0.06 (NS) | 7.28, 0.29 (NS) |
| Disagree | 22 (7.3) | ||||
| Don’t know | 33 (11.0) | ||||
| Primary teeth will affect child’s permanent teeth | Agree | 206 (68.7) | 13.8, 0.03 (S) | 28.37, <0.01 (HS) | 24.39, <0.01 (HS) |
| Disagree | 51 (17.0) | ||||
| Don’t know | 43 (14.3) | ||||
| Oral health affects general health | Agree | 201 (67.0) | 5.9, 0.43 (NS) | 35.09, <0.01 (HS) | 8.37, 0.21 (NS) |
| Disagree | 66 (22.0) | ||||
| Don’t know | 33 (11.0) | ||||
| Using fluoridated toothpaste helps to prevent tooth decay | Agree | 239 (79.7) | 2.48, 0.87 (NS) | 43.10, <0.01 (HS) | 11.49, 0.07 (NS) |
| Disagree | 15 (5.0) | ||||
| Don’t know | 46 (15.3) | ||||
| Parents have an important role in developing a child’s dental attitude | Agree | 245 (95.0) | 18.64, 0.005 (S) | 21.55, <0.01 (HS) | 8.51, 0.203 (NS) |
| Disagree | 7 (2.3) | ||||
| Don’t know | 8 (2.7) | ||||
| It is important to visit the dentist as early as possible | Agree | 197 (65.7) | 9.92, 0.12 (NS) | 19.02, 0.015 (NS) | 6.48, 0.371 (NS) |
| Disagree | 73 (24.3) | ||||
| Don’t know | 30 (10.0) | ||||
| Correct method of cleaning teeth can prevent dental decay | Agree | 271 (90.3) | 1.38, 0.96 (NS) | 4.85, 0.77 (NS) | 6.66, 0.353 (NS) |
| Disagree | 12 (4.0) | ||||
| Don’t know | 17 (5.7) | ||||
| Malocclusion can be preventable | Agree | 124 (41.3) | 12.26, 0.06 (S) | 33.07, <0.01 (HS) | 5.60, 0.46 (NS) |
| Disagree | 41 (13.7) | ||||
| Don’t know | 135 (45.0) |
S: Significant, HS: Highly significant, NS: Not significant
Figure 1 shows Saudi parents awareness toward the prevention of oral diseases. Overall 74% of male Saudi parents were aware about the prevention of oral disease. Around 12% of participants are not aware.
Figure 1.
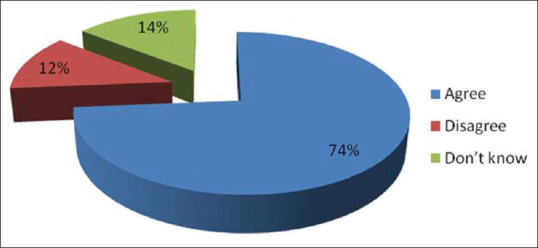
Mean percentage of preventive oral health attitude among Saudi parents
Table 3 shows awareness and utilization of preventive dentistry procedures among Saudi parents. Awareness of preventive dentistry procedures varied among the study population from 6.3% for fluoride varnish to 62.3% for dental floss. Utilization rate was highest topical fluoride application with 17.7% followed by r pit and fissure sealant with 6.3%. Statistically few of the procedures are significant according to education and income (P < 0.05). No difference was found with age group and preventive dentistry procedures (P > 0.05).
Table 3.
Awareness about preventive dentistry procedures
| Questions | Responses | Frequency (%) | Statistics |
|---|---|---|---|
| Serial extraction | Yes | 76 (28.0) | Age>0.05 (NS) |
| No | 216 (72.0) | Education>0.05 (NS) | |
| Utilization | 8 (2.7) | Income>0.05 (NS) | |
| Topical fluoride application | Yes | 77 (43.3) | Age>0.05 (NS) |
| No | 170 (56.7) | Education>0.05 (NS) | |
| Utilization | 53 (17.7) | Income<0.05 (S) | |
| Mouth guards | Yes | 40 (17.0) | Age>0.05 (NS) |
| No | 249 (83.0) | Education>0.05 (NS) | |
| Utilization | 11 (3.7) | Income<0.05 (S) | |
| Pit and fissure sealants | Yes | 134 (58.0) | Age>0.05 (NS) |
| No | 126 (42.0) | Education>0.05 (NS) | |
| Utilization | 40 (13.3) | Income>0.05 (NS) | |
| Fluoride varnish | Yes | 281 (6.3) | Age>0.05 (NS) |
| No | 19 (93.7) | Education>0.05 (NS) | |
| Utilization | 0 (0.0) | Income>0.05 (NS) | |
| Dental floss | Yes | 184 (62.3) | Age>0.05 (NS) |
| No | 113 (37.7) | Education<0.05 (S) | |
| Utilization | 3 (1.0) | Income>0.05 (NS) | |
| Fluoride mouth rinses | Yes | 151 (54.3) | Age>0.05 (NS) |
| No | 137 (45.7) | Education<0.05 (S) | |
| Utilization | 12 (4.0) | Income>0.05 (NS) |
S: Significant, HS: Highly significant, NS: Not significant
Figure 2 shows overall awareness of preventive dentistry procedure it was about 38.45% among Saudi parents. Preventive dentistry utilization rate was only 6%. Around 61.54% of the study population is not aware of the preventive dentistry procedures.
Figure 2.
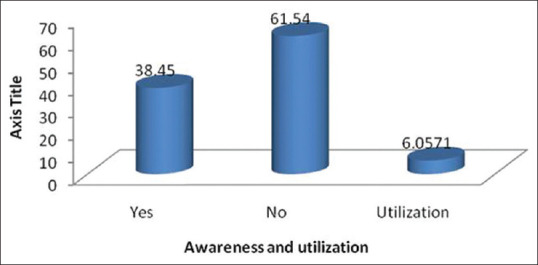
Shows mean percentage of awareness and utilization of preventive dentistry procedures by Saudi parents
Figure 3 shows the source of information of preventive dentistry procedures. Dentist was the main source of information about preventive dentistry procedures (50%) followed by media (31.3%). Least was by physicians (2.3%).
Figure 3.
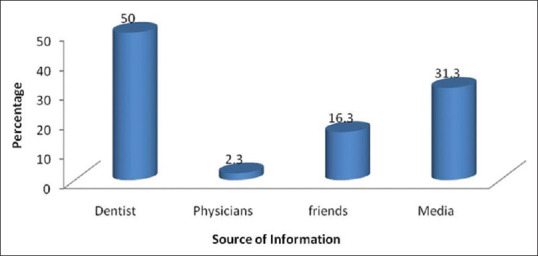
Source of information about preventive dentistry procedures among Saudi parents
DISCUSSION
The role for parents is very important to address oral disease prevention in children as oral health of children is associated with oral health knowledge of their parents.[9]
Seventy-four percent Saudi male parent had positive attitude toward the prevention of oral diseases which can be compared to a study done by Duguma and Banchiamilak[10] at Ethiopia where 72.5% had participants had positive attitude toward childhood caries. Attitude toward dental disease prevention depends on their knowledge. 65.7% of study participants agreed that the first dental visit should be very early this result is in accordance to American Academy of Pediatric Dentistry.[11]
81.7% of male parents agreed that primary teeth are important and 68.7% said that problems in primary teeth will lead to problems on permanent teeth. This was in accordance with the study done by Alaa et al.[12] where it was mentioned that consideration of primary teeth is very important as they are considered as the natural space maintainers for permanent teeth.
Awareness of preventive dentistry among parents depends on its practice and different preventive measures among dental staff.[13,14,15] This differs from country to country, but the common goal is improvement in oral health. The reasons behind the differences can be legislation, work load, dental workforce, insurance, age of practice, etc.[13,16,17]
The differences are due to legislation on oral health care, acceptance, and appreciation of preventive approaches by patients and the community, availability of preventive agents, and work load of restorative care, as well as dentists' age, location, experience, and income.[12,15,16]
Fluoride have a great role in reducing caries incidence, and the present study shows that 82.8% of the parent were highly educated that reflects good knowledge about fluoride and it's mechanism to prevent caries, as compared with the study of Horst JA et al., which reported that only 46% of the responded parents know the importance of fluoride.[12]
The present study showed good information about various preventive procedures available for the prevention of oral diseases among male parents, but there are very few studies on this among male parents in Riyadh Saudi Arabia.
Many studies assessed knowledge, attitude, and practice of preventive dentistry and different preventive measures among dentists and dental auxiliaries.[12,13,14,15] It showed the choice of preventive measures and its use by dental practitioners differ between countries, individual dentists. The differences are due to many factors,[12,16,17] but the ultimate truth was it seemed to be a distance between what is known about preventing oral diseases and what is provided in private practice, dental schools, and community-based programs.[18]
There is no separate oral health policy in many countries, which influence on knowledge and utilization of preventive dentistry utilization. In general, people were aware of the importance of oral hygiene for the prevention of oral diseases which was similar to our study. Lower educational level is consistently associated with a low level of knowledge.[19]
CONCLUSION
Majority of parents in Saudi had a preventive dental knowledge, which is related to their educational level and occupation. The role of dentists was observed to be more in creating awareness among the parents regarding preventive procedure. However, still, there is a gap in knowledge and utilization of services making it part of dentists role to re-emphasise on utilization of services.
Hence, it should be the duty of every dentist to practice these preventive modalities and also educate the patients at either the office and/or at the community. Dental education programs about preventive dentistry and its utilization should be conducted on a regular basis.
Financial support and sponsorship
Self sponsored.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We would like to acknowledge Deanship of Scientific Research, Prince Sattam Bin Abdul Aziz University, Alkharj KSA for supporting this research and all the study participants for helping to provide information and sparing their time.
REFERENCES
- 1.Holt R, Roberts G, Scully C. Dental damage, sequelae, and prevention. West J Med. 2001;174:288–90. doi: 10.1136/ewjm.174.4.288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alesia K, Khalil HS. Reasons for and patterns relating to the extraction of permanent teeth in a subset of the Saudi population. Clin Cosmet Investig Dent. 2013;5:51–6. doi: 10.2147/CCIDE.S49403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Musaiger AO, Takruri HR, Hassan AS, Abu-Tarboush H. Food-based dietary guidelines for the arab gulf countries. J Nutr Metab. 2012;2012:905303. doi: 10.1155/2012/905303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sohn W, Burt BA, Sowers MR. Carbonated soft drinks and dental caries in the primary dentition. J Dent Res. 2006;85:262–6. doi: 10.1177/154405910608500311. [DOI] [PubMed] [Google Scholar]
- 5.Alhabdan YA, Albeshr AG, Yenugadhati N, Jradi H. Prevalence of dental caries and associated factors among primary school children: A population-based cross-sectional study in Riyadh, Saudi Arabia. Environ Health Prev Med. 2018;23:60. doi: 10.1186/s12199-018-0750-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Horst JA, Tanzer JM, Milgrom PM. Fluorides and other preventive strategies for tooth decay. Dent Clin North Am. 2018;62:207–34. doi: 10.1016/j.cden.2017.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Khanna P, Sunda S, Mittal S. “Keep My Space” – A review article. Int J Oral Health Dent. 2015;1:11–5. [Google Scholar]
- 8.Johnsen DC. Baby bottle tooth decay: A preventable health problem in infants. Update Pediatr Dent. 1988;2:1–4. [PubMed] [Google Scholar]
- 9.Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N. Parental influence and the development of dental caries in children aged 0-6 years: A systematic review of the literature. J Dent. 2012;40:787–872. doi: 10.1016/j.jdent.2012.07.013. [DOI] [PubMed] [Google Scholar]
- 10.Duguma FK, Banchiamilak Z. Assessment of Knowledge, Attitude and Practice (KAP) of parents towards childhooddental caries attending pediatrics and dental clinic at alert center, Addis Ababa, Ethiopia, January 2018. Adv Dent Oral Health. 2019;11:29–42. [Google Scholar]
- 11.American Academy of Pediatric Dentistry Clinical Affairs Committee – Infant Oral Health Subcommittee. Guideline on infant oral health care. Pediatr Dent. 2012;34:e148–52. [PubMed] [Google Scholar]
- 12.Alaa HS, Mohammed IA, Robert JS, Aghareed MG. Parent's perception on the importance of their children's first dental visit (A cross sectional pilot study in Malaysia) J Oral Res. 2013;1:17–24. [Google Scholar]
- 13.Chen M. Preventive dentistry in Texas, USA. Community Dent Oral Epidemiol. 1990;18:239–43. doi: 10.1111/j.1600-0528.1990.tb00067.x. [DOI] [PubMed] [Google Scholar]
- 14.Gonzalez CD, Frazier PJ, Messer LB. Sealant use by general practitioners: A Minnesota survey. ASDC J Dent Child. 1991;58:38–45. [PubMed] [Google Scholar]
- 15.Main PA, Lewis DW, Hawkins RJ. A survey of general dentists in Ontario, Part I: Sealant use and knowledge. J Can Dent Assoc. 1997;63:542, 545–53. [PubMed] [Google Scholar]
- 16.Helminen SE, Vehkalahti M, Lammi R, Ketomäki TM, Murtomaa H. Dentists' decisions as to mode of preventive treatment in adolescents and young adults in Finland. Community Dent Health. 1999;16:250–5. [PubMed] [Google Scholar]
- 17.Helminen SK, Vehkalahti MM. Does caries prevention correspond to caries status and orthodontic care in 0- to 18-year-olds in the free public dental service? Acta Odontol Scand. 2003;61:29–33. doi: 10.1080/ode.61.1.29.33. [DOI] [PubMed] [Google Scholar]
- 18.Horowitz AM. The public's oral health: The gaps between what we know and what we practice. Adv Dent Res. 1995;9:91–5. doi: 10.1177/08959374950090022201. [DOI] [PubMed] [Google Scholar]
- 19.Roberts-Thomson KF, Spencer AJ. Public knowledge of the prevention of dental decay and gum diseases. Aust Dent J. 1999;44:253–8. doi: 10.1111/j.1834-7819.1999.tb00229.x. [DOI] [PubMed] [Google Scholar]