

Abstract
Background:
Oral diseases such as dental caries, gingivitis, and periodontitis are common among population. The present study was conducted to assess dental caries status and oral hygiene practice among school children.
Materials and Methods:
This school-based study was conducted on 520 children of age group of 12–14 years of both genders. Location, education, and employment status of parents, use of toothbrush, frequency of brushing, dental floss, total number of meals in a day, number of snacks between meals and sugar consumption, and decayed, missing, filled teeth were recorded.
Results:
There were 266 males and 254 females. Age group 12 years had 80 males and 90 females, 13 years had 70 males and 60 females, and 14 years had 116 males and 104 females. Ninety-six males and 110 females were from urban and 170 males and 144 females were from rural. The mean plaque score in 12-year male children was 0.61 ± 0.32, in 13-year children was 0.68 ± 0.45, and in 14 years was 0.74 ± 0.48. In males, the mean plaque score was 0.70 ± 0.38 and in females was 0.66 ± 0.42. In children from urban area, the mean plaque score was 0.62 ± 0.34 and from rural area was 0.74 ± 0.40. Four hundred and eighteen children were using toothpaste and they had plaque score of 0.76 and 102 children were using floss and they had plaque score of 0.89. Three hundred and twenty children were brushing once, 90 twice, and 110 irregular and there mean plaque score was 0.70, 0.61, and 0.76, respectively. The difference was significant (P < 0.05).
Conclusion:
Authors found that oral health status of children consuming high sugar, more snacks per day, and brushing occasionally was poor.
KEYWORDS: Brushing, dental caries, oral hygiene status
INTRODUCTION
Oral health is the mirror of general body health. Oral diseases such as dental caries, gingivitis, and periodontitis are common among population.[1] Dental caries is defined as irreversible microbial disease of calcified tissue characterized by destruction of organic and dimeralization of inorganic portion of teeth. These diseases have an impact on social health.[2] Oral diseases affecting children have a great impact on school as well as home activities. They have psychosocial impact also. In India, over the past two decades, dental caries is on the rise in prevalence and severity affecting approximately 80% of children and 60% of adults.[3] It affects both deciduous as well as permanent teeth. Dental caries and periodontal diseases can be prevented by meticulous oral hygiene.[4] Toothbrushing is the method which are advisable at early age as soon as the first tooth erupts in the oral cavity. Children should be taught about methods, frequency, duration of brushing, and flossing of teeth in the schools.[5] The consumption of sugar in the form of candies, chocolates, etc., lead to tooth decay, especially in children. There should be check on children, and parent can play a significant role in this aspect. The trend of using fast food is on the rise. All these products are caries-favoring agents.[6]
It is evident that ineffective brushing, poor diet, consumption of sugar products are the leading causes of dental caries. Early detection of this and timely intervention will certainly prevent disease progression.[7] The present study was conducted to assess dental caries status and oral hygiene practice among school children.
MATERIALS AND METHODS
This school-based study was conducted by the department of pedodontics involving 520 children of the age group of 12–14 years of both genders. Parents were made aware of the study, and their consent was obtained before starting the study. School authority gave the permission for conducting the study.
A demographic profile such as name, age, gender, location, education, and employment status of parents was self-reported. A self-designed questionnaire was prepared and distributed to children with the help of class teachers. It comprised questions regarding the use of toothbrush, frequency of brushing, dental floss, total number of meals in a day, number of snacks between meals, and sugar consumption.
Oral examination by a trained pedodontist was conducted. Dental caries status was evaluated using decayed, missing, and filled teeth (DMFT). D represented decayed, M missing, and F filled. Results were entered in MS Excel sheet for assessment. Results were expressed as mean ± standard deviation Assessment was done using SPSS (IBM, St. Louis, MO, United States) software version 21. P < 0.05 was considered statistically significant.
RESULTS
Table 1 shows that there were 266 males and 254 females. Age group 12 years had 80 males and 90 females, 13 years had 70 males and 60 females, and 14 years had 116 males and 104 females. Ninety-six males and 110 females were from urban and 170 males and 144 females were from rural. Father education was up to high standard in 161 males and 44 females, secondary standard in 40 males and 60 females, and up to graduation in 65 males and 50 females. Mother education was up to high in 200 males and 194 females, secondary in 36 males and 40 females, and graduation in 30 males and 20 females. In 224 males and 219 females, fathers were employed, and in 42 males and 35 females, mothers were unemployed. In 45 males and 72 females, mothers were employed, and in 221 males and 182 females, mothers were unemployed. The difference was significant (P < 0.05).
Table 1.
Demographic profile
| Parameters | Males (n=266) | Females (n=254) | P |
|---|---|---|---|
| Age (years) | |||
| 12 | 80 | 90 | 0.81 |
| 13 | 70 | 60 | 0.84 |
| 14 | 116 | 104 | 0.05 |
| Location | |||
| Urban | 96 | 110 | 0.05 |
| Rural | 170 | 144 | |
| Father education | |||
| High | 161 | 144 | 0.05 |
| Secondary | 40 | 60 | |
| Graduation | 65 | 50 | |
| Mother education | |||
| High | 200 | 194 | 0.02 |
| Secondary | 36 | 40 | |
| Graduation | 30 | 20 | |
| Father occupation | |||
| Employed | 224 | 219 | 0.15 |
| Unemployed | 42 | 35 | |
| Mother occupation | |||
| Employed | 45 | 72 | 0.01 |
| Unemployed | 221 | 182 |
Table 2 shows that the mean plaque score in 12-year male children was 0.61 ± 0.32 and in 13-year children was 0.68 ± 0.45 and in 14 years was 0.74 ± 0.48. In males, the mean plaque score was 0.70 ± 0.38 and in females was 0.66 ± 0.42. In children from urban area, the mean plaque score was 0.62 ± 0.34 and from the rural area was 0.74 ± 0.40.
Table 2.
Mean plaque score in children
| Variables | Mean±SD | P |
|---|---|---|
| Age group (years) | ||
| 12 | 0.61±0.32 | 0.05 |
| 13 | 0.68±0.45 | |
| 14 | 0.74±0.48 | |
| Gender | ||
| Male | 0.70±0.38 | 0.01 |
| Female | 0.66±0.42 | |
| Location | ||
| Urban | 0.62±0.34 | 0.02 |
| Rural | 0.74±0.40 |
Table 3 and Graph 1 show that 418 children were using toothpaste and they had plaque score of 0.76 and 102 children were using floss, and they had a plaque score of 0.89. Three hundred and twenty children were brushing once, 90 twice, and 110 irregular, and there mean plaque score was 0.70, 0.61, and 0.76, respectively. The difference was significant (P < 0.05).
Table 3.
Mean plaque score and oral hygiene habits
| Oral hygiene habits | n | Plaque score | P |
|---|---|---|---|
| Tooth paste | 418 | 0.76 | 0.02 |
| Flossing | 102 | 0.89 | 0.04 |
| Brushing | |||
| Once | 320 | 0.70 | 0.01 |
| Twice | 90 | 0.61 | |
| Irregular | 110 | 0.76 |
Graph 1.
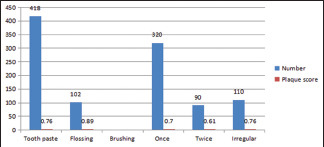
Mean plaque score and oral hygiene habits
Table 4 shows that number of patients with eating frequency 1–2 times per day was 45, 2–3 times per day were 310, and >4 were 165, and their mean DMFT score was 0.62, 0.74, and 0.78, respectively. There were 195 low sugar usage children, 185 were medium usage, and 140 were high usage, and their mean DMFT score was 0.56, 0.64, and 0.76, respectively.
Table 4.
Mean decayed, missing, and filled teeth score and dietary habits
| Dietary habits | n | DMFT score | P |
|---|---|---|---|
| Eating frequency per day | |||
| 1-2 | 45 | 0.62 | 0.02 |
| 3-4 | 310 | 0.74 | |
| >4 | 165 | 0.78 | |
| Sugar usage per day | |||
| Low | 195 | 0.56 | 0.01 |
| Medium | 185 | 0.64 | |
| High | 140 | 0.76 | |
| Snacks per day | |||
| Once | 182 | 0.57 | 0.02 |
| Twice | 208 | 0.67 | |
| Three or more | 130 | 0.74 |
DMFT: Decayed, missing, and filled teeth
DISCUSSION
Oral health affects the general body health. Oral diseases are universally present.[8] The number of dental and oral diseases is increasing day by day, especially in school children. An adoption to meticulous oral hygiene is beneficial in preventing it.[9] Plaque accumulation due to ineffective mechanical and chemical methods of brushing leads to gingivitis and periodontitis.[10] School-going children are more prone to these diseases due to high sugar consumption and failure to maintain oral hygiene. Hence, parents should look after their children oral status.[11] Fluoridated toothpaste is indicated. The frequency of toothbrushing also determines oral hygiene. Brushing twice a day removes dental plaque more effectively than brushing once or occasionally.[12] The present study was conducted to assess dental caries status and oral hygiene practice among schoolchildren.
In the present study, there were 520 school children age 12, 13, and 14 years of both genders. There were 266 males and 254 females. Age group 12 years had 80 males and 90 females, 13 years had 70 males and 60 females, and 14 years had 116 males and 104 females. Ninety-six males and 110 females were from urban and 170 males and 144 females were from rural. Babu et al.[13] in their study determined the prevalence of dental caries and oral hygiene status in 1590 children of twenty schools in both rural and urban areas aged 7–12 years. Results showed that 796 were male and 794 were female children. There was 65.6% prevalence of dental caries. Age group 7–9 and 10–12 years of urban school children exhibited higher prevalence of dental caries and rural school children showed poor oral hygiene status. Female children showed a higher prevalence of dental caries.
We found that father education was up to high standard in 161 males and 44 females, secondary standard in 40 males and 60 females, and up to graduation in 65 males and 50 females. Mother education was up to high in 200 males and 194 females, secondary in 36 males and 40 females, and graduation in 30 males and 20 females. In 224 males and 219 females, fathers were employed, and in 42 males and 35 females, mothers were unemployed. In 45 males and 72 females, mothers were employed, and in 221 males and 182 females, mothers were unemployed.
Quadri et al.[14] assessed oral hygiene practices among 500 school children. The mean plaque score in male was 0.69 and females was 0.66. Increased frequency of snacks and sugar consumption per day significantly showed higher values of DMFT. Dental caries in children who were irregular in brushing their teeth was higher than to the children brushing once per day.
We found that mean plaque score in 12-year male children was 0.61 ± 0.32 and in 13-year children was 0.68 ± 0.45 and in 14 years was 0.74 ± 0.48. In males, the mean plaque score was 0.70 ± 0.38 and in females was 0.66 ± 0.42. In children from urban area, the mean plaque score was 0.62 ± 0.34 and from rural area was 0.74 ± 0.40. Mahesh et al.[15] determined oral health status of 5- and 12-year-old school-going children, in which 600 were 5 years old and 600 were 12 years old. It was found that, in 5-year boys, dmft was 3.53 ± 3.07 and in girls was 3.49 ± 2.83. In 12 years, the DMFT for boys was 3.80 ± 3.43 and for girls was 4.11 ± 2.98. There was no statistically significant difference between dmft/DMFT of boys and girls in both age groups.
In the present study, the number of patients with eating frequency 1–2 times per day was 45, 2–3 times per day were 310, and >4 were 165, and their mean DMFT score was 0.62, 0.74, and 0.78, respectively. There were 195 low sugar usage children, 185 were medium usage, and 140 were high usage, and their mean DMFT score was 0.56, 0.64, and 0.76, respectively.
The shortcoming of the study is the small sample size.
CONCLUSION
Authors found that oral health status of children consuming high sugar, more snacks per day, and brushing occasionally was poor.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Rao A, Sequeira SP, Peter S. Prevalence of dental caries among school children of Moodbidri. J Indian Soc Pedod Prev Dent. 1999;17:45–8. [PubMed] [Google Scholar]
- 2.Sogi GM, Bhaskar DJ. Dental caries and oral hygiene status of school children in Davangere related to their socio-economic levels: An epidemiological study. J Indian Soc Pedod Prev Dent. 2002;20:152–7. [PubMed] [Google Scholar]
- 3.Subrata S, Subrata S. Prevalence and severity of dental caries and oral hygiene status in rural and urban areas of Calcutta. J Indian Soc Pedod Prev Dent. 1996;14:17–20. [PubMed] [Google Scholar]
- 4.Retnakumari N. Prevalence of dental caries and risk assessment among primary school children of 6-12 years in the Varkala municipal area of Kerala. J Indian Soc Pedod Prev Dent. 1999;17:135–42. [PubMed] [Google Scholar]
- 5.Dhar V, Jain A, van Dyke TE, Kohli A. Prevalence of dental caries and treatment needs in the school-going children of rural areas in Udaipur district. J Indian Soc Pedod Prev Dent. 2007;25:119–21. doi: 10.4103/0970-4388.36560. [DOI] [PubMed] [Google Scholar]
- 6.Chironga L, Manji F. Dental caries in 12-year-old urban and rural children in Zimbabwe. Community Dent Oral Epidemiol. 1989;17:31–3. doi: 10.1111/j.1600-0528.1989.tb01822.x. [DOI] [PubMed] [Google Scholar]
- 7.Omar SM, Pitts NB. Oral hygiene, gingivitis and periodontal status of Libyan school children. Community Dent Health. 1991;8:329–33. [PubMed] [Google Scholar]
- 8.Saravanan S, Kalyani V, Vijayarani MP, Jayakodi P, Felix J, Arunmozhi P, et al. Caries prevalence and treatment needs of rural school children in Chidambaram Taluk, Tamil Nadu, South India. Indian J Dent Res. 2008;19:186–90. doi: 10.4103/0970-9290.42948. [DOI] [PubMed] [Google Scholar]
- 9.Chaffin JG, Pai SC, Bagramian RA. Caries prevalence in northwest Michigan migrant children. J Dent Child (Chic) 2003;70:124–9. [PubMed] [Google Scholar]
- 10.Mittal M, Chaudhary P, Chopra R, Khattar V. Oral health status of 5 years and 12 years old school going children in rural Gurgaon, India: An epidemiological study. J Indian Soc Pedod Prev Dent. 2014;32:3–8. doi: 10.4103/0970-4388.127039. [DOI] [PubMed] [Google Scholar]
- 11.Pauraite J, Milciuviene S, Sakalauskiene J. The prevalence of gingivitis among 4-16 year old schoolchildren in Kaunas. Stomatol Baltic Dent Maxillofac J. 2003;5:97–100. [Google Scholar]
- 12.Jessri M, Jessri M, Rashidkhani B, Kimiagar SM. Oral health behaviours in relation to caries and gingivitis in primary-school children in Tehran, 2008. East Mediterr Health J. 2013;19:527–34. [PubMed] [Google Scholar]
- 13.Babu MM, Nirmala S, Sivakumar N. Oral hygiene status of 7-12 year old school children in rural and Urban population of Nellore district. J Indian Assoc Public Health Dent. 2011;18:1075–80. [Google Scholar]
- 14.Quadri MF, Shubayr MA, Hattan AH, Wafi SA, Jafer AH. Oral hygiene practices among saudi arabian children and its relation to their dental caries status. Int J Dent. 2018;2018:3234970. doi: 10.1155/2018/3234970. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5926499/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mahesh Kumar P, Joseph T, Varma RB, Jayanthi M. Oral health status of 5 years and 12 years school going children in Chennai city – An epidemiological study. J Indian Soc Pedod Prev Dent. 2005;23:17–22. doi: 10.4103/0970-4388.16021. [DOI] [PubMed] [Google Scholar]