

Abstract
Objective:
Studies support the Transtheoretical Model’s (TTM) ability to describe behavior change processes and guide interventions; however, the temporal sequencing of constructs is less understood. This cohort study tested five sequences to identify TTM construct changes related to physical activity.
Methods:
A random sample provided baseline data (n=689; 63% female; Mage (SD)=47(17); 37% white), with 401 participants providing 24-month data, at six-month intervals.
Results:
Structural equation models revealed processes to cognitions to stage (AIC=29313.093, BIC=29514.883, CFI=0.999, RMSEA=0.006, SRMR=0.026); processes to stage to cognitions (AIC=27788.651, BIC=27973.268, CFI=0.978, RMSEA=0.024, SRMR=0.038), self-efficacy/temptations to processes to decisional balance to stage (AIC=13914.771, BIC=14031.169, CFI=0.981, RMSEA=0.018, SRMR=0.034), and stage to processes to cognitions (AIC=22048.324, BIC=22212.986, CFI=0.976, RMSEA=0.026, SRMR=0.029) all fit well. However, cognitions to processes to stage did not fit the data well (AIC=10353.555, BIC=10444.179, CFI=0.937, RMSEA=0.038, SRMR=0.035).
Conclusions:
Integrating results revealed a cyclical model so that intervention efforts should focus on processes to change cognitions related to barrier self-efficacy and decisional balance, which then lead to change in stage and then renew focus on the processes.
Keywords: stage of change, decisional balance, perceived barriers, processes of change, self-efficacy, temptations
Introduction
Physical activity is a noted component in the prevention of obesity and chronic disease (United States Department of Health and Human Services: Office of Disease Prevention and Health Promotion, 2008); however, less than half of US adults report enough physical activity to meet current guidelines (Centers for Disease Control and Prevention, 2009). Various behavior change theories have been proposed to help individuals adopt more active lifestyles.
The Transtheoretical Model (TTM) is a widely-used framework for understanding the initiation and maintenance of health behaviors (Burkholder & Nigg, 2002). “Transtheoretical Model” or “Transtheoretical Model of behavior change” has been referenced in over 1500 publications in the National Library of Medicine database and PsycINFO from 1948 to today. Studies using TTM have examined a range of health-related behaviors such as physical activity (Geller, Nigg, Motl, Horwath, & Dishman, 2012), healthy eating (Johnson et al., 2008), cancer screening (Trauth, Ling, Weissfeld, Schoen, & Hayran, 2003), and stress management (Evers et al., 2006). This model characterizes behavior change as a process of temporal advancement through five distinct stages: precontemplation (“no intention to change”), contemplation (“seriously considering change”), preparation (“making small changes”), action (“actively engaged in changing behavior”), and maintenance (“continuation of successful change efforts”) (Prochaska & Velicer, 1997). According to the model, barrier self-efficacy, temptations, decisional balance, and processes of change influence movement through the stages (Prochaska & Velicer, 1997). A key strength of the TTM is that it defines individuals’ readiness for change allowing for the selection of constructs and tailoring of interventions. Interventions using the TTM to change physical activity behaviors have primarily tailored interventions based on participant’s stage of change (Adams & White, 2003; Spencer, Adams, Malone, Roy, & Yost, 2006). Such interventions have been found to have better outcomes in the short-term compared to non-tailored interventions (Adams & White, 2003) and potentially impact both activity duration and frequency (Mastellos, Gunn, Felix, Car, & Majeed, 2014). Recent meta-analyses reported that TTM-based interventions are effective in promoting physical activity (Gourlan et al., 2016) and that processes of change and self-efficacy are the most important moderators of the TTM in physical activity (Romain et al., 2018).
However, a lack of long-term effects, measurement and research design issues, and the complexity of physical activity behaviors have been noted as continued concerns (Adams & White, 2003; Adams & White, 2005; Marshall & Biddle, 2001; Spencer et al., 2006). TTM was originally developed for use in smoking, a behavior where cessation is the goal, while physical activity is a behavior where adoption or adherence are the goals (Nigg et al., 2011). This difference in outcomes combined with the complexity of physical activity behavior change (i.e., different types of activities; changing duration, intensity, frequency, or some combination) may make the way TTM constructs are conceptualized for physical activity behavior change different (Adams & White, 2003; Nigg et al., 2011). For example, stages of change may work less as five distinct stages and more as a continuum (Brug et al., 2005; Marshall & Biddle, 2001).
In addition to the ambiguity of how TTM may work to help change physical activity behaviors, criticisms have been leveled at the TTM in general (Bandura, 1997a; Herzog, Abrams, Emmons, & Linnan, 2000; West, 2005). One of the most theoretically serious challenges is the lack of evidence for an explicit temporal sequencing of the model constructs. According to the TTM, use of the processes of change leads to increased self-efficacy and shifts in decisional balance which, in turn, lead to movement forward through the stages (Prochaska & Velicer, 1997) (Figure 1a). However, some researchers have suggested that self-efficacy and decisional balance are not determinants, but secondary outcomes of stage transition (Velicer, DiClemente, Rossi, & Prochaska, 1990). According to this perspective, the processes of change lead to stage progression, which subsequently enhances self-efficacy and shifts decisional balance (Figure 1b). The self-efficacy and outcome expectation constructs of Social Cognitive Theory (Bandura, 1997a; Bandura, 1997b) suggest increases in self-efficacy may lead to increased use of self-regulatory and other processes of change, a shift in outcome expectancies that underlie decisional balance, and thus a change in stage (Figure 1c) (Bandura, 2004). Additionally, changes in self-efficacy and decisional balance could lead to change in stage (Figure 1d). Lastly, behavior change itself may be the driving force instead of an outcome, such that changes in stage lead to changes in processes, decisional balance, and self-efficacy (Figure 1e).
Figure 1.
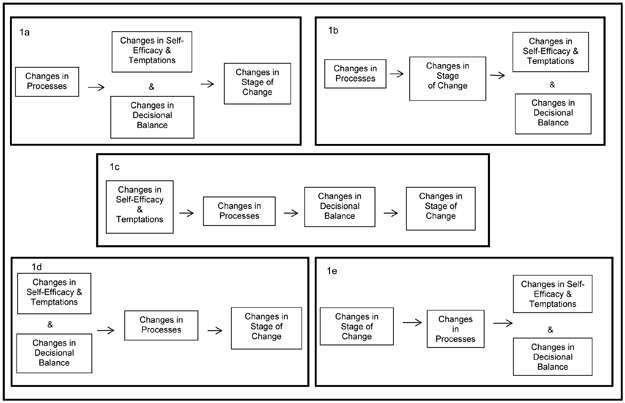
The five hypothesized temporal sequences for transtheoretical model constructs.
These various conceptualizations have direct implications for intervention development, delivery, and success as constructs may ultimately be outcomes instead of determinants of stage change and vice versa. Intervention design and delivery would change focus altogether if the constructs prove to be outcomes instead of determinants. For example, if decisional balance variables are determinants, interventions would need to focus on increasing the importance of the pros and decreasing the importance of the cons of a behavior; however, if decisional balance variables are outcomes, the intervention focus shifts to influencing upstream variables that would lead to an increase in perceptions of pros and a decrease in perception of cons. Thus, it is vital to ascertain each construct’s role within the TTM. Determining constructs’ temporal order is also important for theoretical reasons, as such information would help to elucidate the mechanisms underlying stage change. Mechanism identification is an important step toward evolving the TTM from a descriptive model to an explanatory theory.
Despite the practical and theoretical importance of the correct temporal sequencing of TTM variables, we are unaware of any published study that has addressed this issue. To do so requires a longitudinal design with repeated measures of constructs and multivariate tests of competing temporally ordered models (Nigg et al., 2011). Although TTM studies have employed longitudinal designs (Dishman et al., 2009; Dishman, Vandenberg, Motl, & Nigg, 2010; Marcus, Simkin, Rossi, & Pinto, 1996; Plotnikoff, Hotz, Birkett, & Courneya, 2001; Schumann et al., 2005), virtually all have tested the hypothesis that core constructs function as predictors of change in stage or another measure of physical activity.
We are aware of only one study that tested an alternative model. In that study, a panel design was used to understand decreasing exercise participation in late adolescents (Nigg, 2001). Exercise time decreased and the panel analyses indicated that none of the baseline constructs were significantly associated with exercise at follow-up. However, the pathway between behavioral processes and exercise was the largest. Exercise at baseline had a significant negative association with pros and cons and a significant positive association with self-efficacy at follow-up (Nigg, 2001). These results suggest that an alternatively ordered temporal model may be present. However, the study had only two time points, focused on bivariate relationships rather than simultaneous multivariate relationships, and included a lengthy time between measurements. The present study was designed to overcome these limitations.
The purpose of the present study was to test five competing models of temporally-ordered TTM variables measured over five, six-month intervals (i.e., baseline, 6-, 12-, 18-, and 24-months). The models are outlined above and shown in Figure 1. Behavior was not included to avoid giving more weight to later stages (i.e. action and maintenance) and masking the importance of intention building, present in contemplation and preparation (Nigg, 2005). Given the original conceptualization of the TTM, Figure 1a is hypothesized to be the superior model.
Methods
Participants
Participants were a random sample of 700 adults (limited to 1 participant per household) over the age of 18 (Mage = 47.1, SD = 17.1) living in Hawaii, who provided consent and were contacted every six months for two years. Participants were 63% female, and 37% white, 31% Asian, 22% Native Hawaiian/Pacific Islander, and 8% other. A more detailed description of recruitment, demographics, and the physical activity characteristics of the participants have been previously reported (Dishman et al., 2009; Dishman et al., 2010; Geller et al., 2012; Paxton et al., 2008). For this study, 689 participants (98%) provided usable data (completed questionnaire item on stage and at least one item for each construct) at baseline and 401 participants provided usable data at two years (58% of participants retained).
Procedures
A local survey firm conducted all recruitment with random digit dialing and survey administration, which were programmed into a computer assisted telephone interview system. Before survey administration, all questionnaires were pilot tested for interpretability and ease of administration. A total of 4,392 calls resulted in 2,785 (63.4%) calls reaching eligible households (residents and English speakers). When contact was made, the adult living in the home, whose birthday was closest to the date of the phone call, was invited to participate. Participation was described as five 30-minute interviews about physical activity and dietary intake over the next two years for which participants would receive $10 per interview and $25 for the last interview. In total, 700 participants were recruited (25.1% of eligible households). Informed consent was obtained before completing the first interview. The University of Hawaii Institutional Review Board approved all procedures.
Measures
Stages of change.
Four statements were used to assess participant’s current stage of change for physical activity (Nigg, 2002). Participants who indicated they were not currently meeting the criterion (at least 30 minutes for five days a week of moderate or higher intensity physical activity) and had no intention to do so were classified as precontemplation stage. Participants indicating they did not meet the criterion, but had an intention to do so within the next six months were classified as contemplation stage. Participants not meeting the criterion, but indicating they had an intention to start within the next 30 days were classified as preparation stage. Participants classified as action stage indicated they had been at criterion for less than six months. Participants classified as maintenance stage indicated they had been at criterion for six months or more (Nigg & Riebe, 2002). The stages were coded from 1-precontemplation to 5-maintenance. This type of stage measure has been validated against self-reported and objective physical activity indicators (Hellsten et al., 2008; Schumann et al., 2002; Schumann, Estabrooks, Nigg, & Hill, 2003).
Barrier self-efficacy.
A six-item scale was used to measure participant’s confidence to be physically active in the presence of barriers (Paxton et al., 2008). Respondents rated each item on a five-point scale (1 = not at all confident; 5 = completely confident), and responses were averaged to derive a self-efficacy score. Baseline internal consistency was α = 0.85 and factorial invariance was seen across gender, age, ethnic subgroups (Paxton et al., 2008), and time (Geller et al., 2012).
Temptations.
A two-factor (temptations-affect, temptations-competing demands), seven-item scale was modified for physical activity behavior from a previous scale assessing temptation (Geller et al., 2012; Hausenblas et al., 2001; Paxton et al., 2008). Items were preceded by the statement: “Using the scale below, please indicate how tempted you are NOT to exercise in the following situations.” Responses were made on a scale ranging from 0% (not at all tempted) to 100% (extremely tempted). Average response scores were computed for each subscale. In the present study, baseline Cronbach’s alpha was α = 0.87 for the affect subscale and α = 0.91 for the competing demands subscale, and factorial invariance was seen across gender, age, ethnic subgroups (Paxton et al., 2008), and time (Geller et al., 2012).
Decisional balance.
A two-factor, nine-item scale was used to assess decisional balance. Participants rated the importance of five pros and four cons of PA on a five-point scale (1 = not important; 5 = extremely important) (Paxton et al., 2008). Responses were averaged for each scale. Baseline internal consistencies were α = 0.83 and α = 0.71 for the pros and cons subscales, respectively, and factorial invariance was seen across gender, age, ethnic subgroups (Paxton et al., 2008) and time (Geller et al., 2012).
Processes of change.
The process of change questionnaire assessed the frequency with which participants used processes of change over the past month (1 = never; 5 = repeatedly) (Nigg & Riebe, 2002). Alpha coefficients ranged from 0.72 to 0.88 for experiential processes and from 0.76 to 0.85 for the behavioral processes. However, as noted in a previous report, the hypothesized ten-factor solution for the processes of change was not supported in this cohort (Paxton et al., 2008). An alternative, better-fitting model was supported (Paxton et al., 2008) and provides the measurement model used in this and previous studies involving this cohort (Dishman et al., 2010). Using this model, five processes were measured. The process of self-reevaluation/self-liberation/reinforcement management (SRF) was represented by a total of six items, dramatic relief/environmental reevaluation (DE) by a total of five items, and the processes of counter conditioning (CC), helping relationships (HR), and consciousness raising (CR) by three items each. Scores for each subscale were computed as the average across the subscale items. This model showed factorial invariance across gender, age, ethnic subgroups (Paxton et al., 2008) and time (Geller et al., 2012).
Data Analysis
Descriptive statistics were assessed for all variables and change scores computed for each of the four intervals between time points. Skewness and kurtosis, in general, indicated the change scores met the assumptions of normality (less than 2 and less than 4, respectively). The pros and cons change scores were marginal in kurtosis (3-5); however, had almost no skew (less than 0.6). Therefore no transformations were deemed necessary. Missing data were minimal and appeared at random, ranging from 1% to 4% for each TTM factor, and were imputed using Full Information Maximum Likelihood (FIML) estimation..
Initially, latent growth modeling approaches were examined; however, all but one model failed to converge and that model’s fit statistics did not indicate a good fit. Structural equation modeling (SEM) was then employed to analyze the ability of TTM constructs to predict other constructs according to the progressions indicated in Figure 1. Computed change scores (later time point minus earlier time point of scale score) were used, and in all of the models, processes of change, decisional balance and temptations were treated as separate manifest variables. Processes of change were measured by five factors, SRF, DE, CC, HR and CR while decisional balance and temptation were measured by two factors each. For example, to test Figure 1a, change in processes was from baseline to six months, changes in self-efficacy, decisional balance, and temptations were from six months to 12 months, and change in stage was from 12 months to 18 months. Theoretically as individuals’ progress through the stages of change, self-efficacy should increase as temptations decrease and thus these variables may be highly correlated (Nigg et al., 2011). We added this correlation to the models and compared them to models without the correlation (Burnham & Anderson, 2002). Fit indices AIC, BIC, CFI, RMSEA, and SRMR were examined to determine validity of SEM models.
Descriptive statistics were conducted using IBM SPSS Statistics 22 (IBM Corp, 2013) and SEM using Mplus7 (Muthen & Muthen, 1998-2015).
Results
Descriptive statistics are presented for variables at all time points (Table 1) and for changes between time points (Table 2). Overall, the study population was active with a reported baseline stage of 4.07 (SD = 1.31), corresponding on average to the action stage, with over 50% of participants in the Maintenance stage. At baseline, barrier self-efficacy was moderately high with a mean rating of 3.16 (SD = 1.00), whereas there was a high mean rating for pros and low mean ratings for temptations and cons. Means for processes ranged from 2.50 (SD = 1.50) to 3.99 (SD = 0.88). Stage showed only small positive changes across the time points. Small reductions were seen in other variables between time points, especially for processes between the first three time points. Many of the variables were significantly correlated in a positive direction (see Table 3), especially those measuring parts of the same construct (i.e. temptations, processes). In addition, stage of change and barrier self-efficacy had high correlation as did these constructs with the processes SRF and CC.
Table 1.
Descriptive Statistics for TTM Construct Variables at All Time Points
| Model Variable Scales and Subscales | Baseline (n=689) |
6 Months (n=516) |
12 Months (n=454) |
18 Months (n=427) |
24 Months (n=401) |
||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | ||
| Stages of Change | |||||||||||
| Pre-contemplation (Stage1) | 60 | 8.7 | 48 | 9.3 | 37 | 8.1 | 31 | 7.3 | 31 | 7.7 | |
| Contemplation (Stage 2) | 36 | 5.2 | 27 | 5.2 | 22 | 4.8 | 33 | 7.7 | 18 | 4.5 | |
| Preparation (Stage 3) | 98 | 14.2 | 54 | 10.5 | 48 | 10.6 | 41 | 9.6 | 41 | 10.2 | |
| Action (Stage 4) | 98 | 14.2 | 66 | 12.8 | 64 | 14.1 | 50 | 11.7 | 43 | 10.7 | |
| Maintenance (Stage 5) | 397 | 57.6 | 321 | 62.2 | 283 | 62.3 | 272 | 63.7 | 268 | 66.8 | |
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Stages of Change | 4.07 | 1.31 | 4.13 | 1.33 | 4.18 | 1.28 | 4.17 | 1.29 | 4.24 | 1.26 | |
| Barrier Self-Efficacya | 3.16 | 1.00 | 3.19 | 0.96 | 3.23 | 0.95 | 3.35 | 0.93 | 3.29 | 0.95 | |
| Temptationsb | |||||||||||
| Affect | 37.63 | 27.00 | 34.28 | 27.44 | 34.77 | 27.00 | 27.87 | 24.88 | 27.03 | 25.22 | |
| Competing Demands | 43.65 | 28.96 | 44.54 | 30.25 | 49.02 | 28.92 | 45.12 | 30.56 | 45.51 | 29.71 | |
| Decisional Balancea | |||||||||||
| Pros | 4.08 | 0.88 | 4.00 | 0.92 | 3.92 | 0.93 | 3.91 | 0.93 | 4.02 | 0.92 | |
| Cons | 1.70 | 0.81 | 1.68 | 0.80 | 1.67 | 0.78 | 1.50 | 0.66 | 1.52 | 0.72 | |
| Processes of Changea | |||||||||||
| SRF | 3.98 | 0.88 | 3.84 | 0.94 | 3.83 | 0.90 | 3.81 | 0.94 | 3.88 | 0.91 | |
| DE | 3.30 | 1.01 | 3.21 | 1.05 | 3.17 | 1.03 | 3.18 | 1.00 | 3.21 | 0.99 | |
| CC | 3.00 | 1.06 | 2.91 | 1.05 | 2.91 | 1.02 | 2.91 | 1.07 | 2.93 | 1.02 | |
| HR | 2.56 | 1.15 | 2.39 | 1.09 | 2.38 | 1.08 | 2.29 | 1.07 | 2.43 | 1.05 | |
| CR | 2.50 | 1.05 | 2.31 | 1.02 | 2.27 | 0.99 | 2.36 | 1.01 | 2.35 | 1.01 | |
CC = Counter Conditioning, CD = Competing Demands, CR = Consciousness Raising, DE= Dramatic relief/Environmental reevaluation, HR = Helping Relationships, SRF = Self-revaluation/Reinforcement management/Self-liberation
A scale of 1-5 was used.
A scale of 0-100 was used
Table 2.
Means and Standard Deviations for TTM Construct Change Variables between Time Points
| Model Variable Scales and Subscales | Baseline to 6 Months (n=689) |
6 to 12 Months (n=516) |
12 to 18 Months (n=454) |
18 to 24 Months (n=427) |
|||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Stages of Change | 0.10 | 1.27 | 0.03 | 1.29 | 0.02 | 1.17 | 0.08 | 1.13 | |
| Barrier Self-Efficacya | −0.12 | 5.13 | 0.12 | 4.61 | 0.49 | 4.64 | −0.12 | 4.78 | |
| Temptationsb | |||||||||
| Affect | −2.64 | 34.77 | 0.70 | 32.33 | −6.15 | 27.90 | −1.37 | 25.06 | |
| Competing Demands | 0.46 | 37.16 | 5.34 | 34.82 | −3.40 | 30.16 | −1.07 | 28.97 | |
| Decisional Balancea | |||||||||
| Pros | −0.55 | 4.16 | −0.35 | 3.97 | −0.23 | 3.96 | 0.60 | 3.86 | |
| Cons | 0.00 | 3.51 | 0.04 | 3.17 | −0.65 | 3.22 | 0.09 | 3.28 | |
| Processes of Changea | |||||||||
| SRF | −1.25 | 5.76 | −0.16 | 4.92 | −0.30 | 4.89 | 0.68 | 5.24 | |
| DE | −0.50 | 4.48 | −0.31 | 3.89 | −0.16 | 3.50 | 0.26 | 3.40 | |
| CC | −0.31 | 3.03 | −0.04 | 2.66 | −0.05 | 2.78 | 0.28 | 2.65 | |
| HR | −0.47 | 3.21 | −0.05 | 2.92 | −0.18 | 2.58 | 0.35 | 2.75 | |
| CR | −0.65 | 2.72 | −0.10 | 2.25 | 0.05 | 2.17 | 0.12 | 2.39 | |
CC = Counter Conditioning, CD = Competing Demands, CR = Consciousness Raising, DE= Dramatic relief/Environmental reevaluation, HR = Helping Relationships, SRF = Self-revaluation/Reinforcement management/Self-liberation
A scale of 1-5 was used.
A scale of 0-100 was used.
Table 3.
Correlations of Baseline TTM Construct Variables
| Stages of Change |
Barrier Self- Efficacy |
Temptations - Affect |
Temptations - CD |
Pros | Cons | SRF | DE | CC | HR | CR | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Stages of Change | 1.00 | 0.47** | −0.14** | −0.08* | 0.23** | −0.10** | 0.50** | 0.21** | 0.52** | 0.15** | 0.21** |
| Barrier Self-Efficacy | 1.00 | −0.27** | −0.17** | 0.28** | −0.18** | 0.51** | 0.24** | 0.63** | 0.13** | 0.35** | |
| Temptations - Affect | 1.00 | 0.52** | 0.02 | 0.22** | −0.11** | −0.002 | −0.17** | 0.02 | −0.10* | ||
| Temptations - CD | 1.00 | 0.02 | 0.05 | −0.09* | −0.06 | −0.09* | 0.03 | −0.06 | |||
| Pros | 1.00 | 0.11** | 0.58** | 0.50** | 0.35** | 0.24** | 0.34** | ||||
| Cons | 1.00 | −0.09* | 0.13** | −0.06 | 0.14** | 0.10** | |||||
| SRF | 1.00 | 0.59** | 0.62** | 0.32** | 0.45** | ||||||
| DE | 1.00 | 0.40** | 0.32** | 0.46** | |||||||
| CC | 1.00 | 0.32** | 0.46** | ||||||||
| HR | 1.00 | 0.30** | |||||||||
| CR | 1.00 |
CC = Counter Conditioning, CD = Competing Demands, CR = Consciousness Raising, DE= Dramatic relief/Environmental reevaluation, HR = Helping Relationships, SRF = Self-revaluation/Reinforcement management/Self-liberation
p<0.05
p<0.01
All models converged and showed significantly more acceptable fit indices when the addition of the correlation between self-efficacy and temptations was included (Table 4). The models based on Figure 1a had an acceptable fit (AIC = 29313.093, BIC = 29514.883, CFI = 0.999, RMSEA = 0.006, SRMR=0.026) after adding the correlation between self-efficacy and temptations. Models based on Figure 1d, with the addition of the correlation between self-efficacy and temptations, however had poor fit (AIC = 10353.555, BIC = 10444.179, CFI = 0.937, RMSEA = 0.038, SRMR=0.035). With the addition of the correlation between self-efficacy and temptations. models based also on Figures1b, 1c, and 1e all had acceptable fit indices: Model 1b (AIC = 27788.651, BIC = 27973.268, CFI = 0.978, RMSEA = 0.024, SRMR=0.038), Model 1c (AIC = 13914.771, BIC = 14031.169, CFI = 0.981, RMSEA = 0.018, SRMR=0.034), Model 1e (AIC = 22048.324, BIC = 22212.986, CFI = 0.976, RMSEA = 0.026, SRMR=0.029) (Burnham & Anderson, 2002; Burnham & Anderson, 2004).
Table 4.
Structural Equation Model statistics for Figures 1a-1e
| Model | AIC | BIC | adjusted BIC | CFI | RMSEA | SRMR |
|---|---|---|---|---|---|---|
| Figure 1a | NC | |||||
| Figure 1a with correlation between temptations and SE | 29313.093 | 29514.883 | 29365.688 | 0.999 | 0.006 | 0.026 |
| Figure 1b | NC | |||||
| Figure 1b with correlation between temptations and SE | 27788.651 | 27973.268 | 27836.770 | 0.978 | 0.024 | 0.038 |
| Figure 1c | NC | |||||
| Figure 1c with correlation between temptations and SE | 13914.771 | 14031.169 | 13939.147 | 0.981 | 0.018 | 0.034 |
| Figure 1d | NC | |||||
| Figure 1d with correlation between temptations and SE | 10353.555 | 10444.179 | 10371.205 | 0.937 | 0.038 | 0.035 |
| Figure 1e | 22062.717 | 22195.250 | 22090.535 | 0.932 | 0.040 | 0.048 |
| Figure 1e with correlation between temptations and SE | 22048.324 | 22212.986 | 22082.886 | 0.976 | 0.026 | 0.029 |
NC= did not converge, SE=self-efficacy
Discussion
The TTM provides a framework that has guided the development of many health behavior change interventions; however, few attempts have been made to examine the sequence of the model’s theoretical constructs and their influence on one another. Using physical activity data collected over two years, this study was able to temporally link constructs of the TTM with regards to physical activity stage change. Examining sequences that showed good fit indices supports more of a cyclical model rather than a linear one. Changes in processes seem to lead to changes in barrier self-efficacy, temptations, and decisional balance; plus it seems changes in processes lead to stage change. The changes in barrier self-efficacy, temptations, and decisional balance led to changes in stage but not change in processes. Changes in stages of change seem to lead to change in processes. Thus, integrating these results point to processes changes leading to the cognitive variable changes which lead to stage change which leads to process change. This cyclical ordering is akin to the reciprocal determinism described in the social cognitive theory (Bandura, 1997b). In short the how leads to the why which leads to the when, which leads to the how again.
These findings provide guidance for physical activity interventions suggesting strategies should focus on processes to change cognitions favorably, which then help participants progress through the stages of change, and then to renew efforts to alter processes and continue progression.
Participants reported being primarily in higher stages of physical activity change, with a greater percentage of participants in the maintenance stage at 24 months compared to baseline (58% versus 67%). Previous research suggests self-efficacy increases linearly (Marshall & Biddle, 2001; Nigg, 2001) with stage progression while constructs such as temptations, decisional balance, and processes may decrease with stage transition or be irrelevant once an individual reaches later stages (Marshall & Biddle, 2001; Nigg et al., 2011; Prochaska & Velicer, 1997), although this is partially arguable as a recent study suggested a linear increase in experiential and behavioral processes with stage progression (Lipschitz et al., 2015). Overall, participants reported behavioral constructs that supported being in more advanced stages as well as positive changes in stage including moderate barrier self-efficacy, low temptations, a positive decisional balance, and low to moderate use of processes.
The results showed good fit for the sequences outlined in Figure 1a, 1b, 1c, and 1e. . Past research on TTM processes indicate a two-level structure whereby experiential processes are more important in earlier stages, while behavioral process may be more important in later stages (Biddle & Nigg, 2000; Nigg et al., 2011; Prochaska, Velicer, DiClemente, & Fava, 1988). However, a previous analysis from the current study found participants used both experiential and behavioral processes to increase and maintain physical activity (Dishman et al., 2010). Additional studies have reported similar results for physical activity (Lipschitz et al., 2015). This divergence from past TTM research is a particularity of the TTM when applied to physical activity. However, it has been argued that general and behavior-specific versions of a theory’s application could coexist (Noar & Head, 2014) and may explain why a mix of experiential processes (e.g., DRE) and behavioral processes (e.g., SRF, CC) showed statistically significant influences on stage in this study.
When the results are interpreted integrating all the fitting models, a cyclical sequence is evident. This finding matches the theoretical underpinnings of TTM in that behavior change is dynamic (Marshall & Biddle, 2001) and stage progression is believed to be cyclical, with individuals progressing and regressing through the stages towards a sustained behavior (Prochaska, DiClemente, & Norcross, 1992). Current study findings indicate this cyclical process is fueled by processes, which then impact the cognitive variables. Another longitudinal study, using data from three time-points collected over four months, also concluded interventions should first target processes; however, they found a distinction between cognitive (i.e., experiential) processes and behavioral processes (Kosma, Ellis, & Bauer, 2012). This may be due in part to the evolution of the measurement of processes (Kosma et al., 2012; Paxton et al., 2008) as well as the inclusion of behavior change in the model.
A study of Chinese adolescents over six months concluded that while TTM constructs did not work in totality as theorized, stage change would be most likely if self-efficacy, pros, and processes were intervened upon (Callaghan, Khalil, & Morres, 2010). This conclusion matches with the next phases of the cyclical model in which changes in barrier self-efficacy, temptations, and decisional balance lead to changes in stage.
This study provides valuable insight regarding the temporal sequencing of TTM constructs. Although this study was naturalistic, participants reported being primarily in higher stages of change across time points, Further, it should be noted that the change scores for stages were positive whereas the changes scores in the processes and cognitive variables tended to be in the negative direction, which explain the negative path coefficients in the SEM models which is actually congruent with expectations.. Using self-report data may have introduced social desirability bias. Studies with a wider range in physical activity stages and using an experimental design may find stronger associations. Only TTM constructs related to physical activity were used in this study making additional analyses necessary to examine other behaviors (e.g., diet, smoking). Despite these limitations, this analysis is one of the first longitudinal analysis of TTM constructs to include periodic evaluations over the course of two years and data from nearly 700 adults, providing a robust dataset with which to conduct this type of analysis.
Findings from this study suggest intervention efforts should focus on processes to help participants change in cognitions related to barrier self-efficacy and decisional balance, which then lead to change in stage. Then as participants move through these changes in stage, additional intervention strategies aimed at processes will be needed to help participants’ further progress. Subsequent investigations should test such strategies as well as test whether the temporal sequence seen with physical activity stage change is replicated in other health behaviors.
Figure 2.
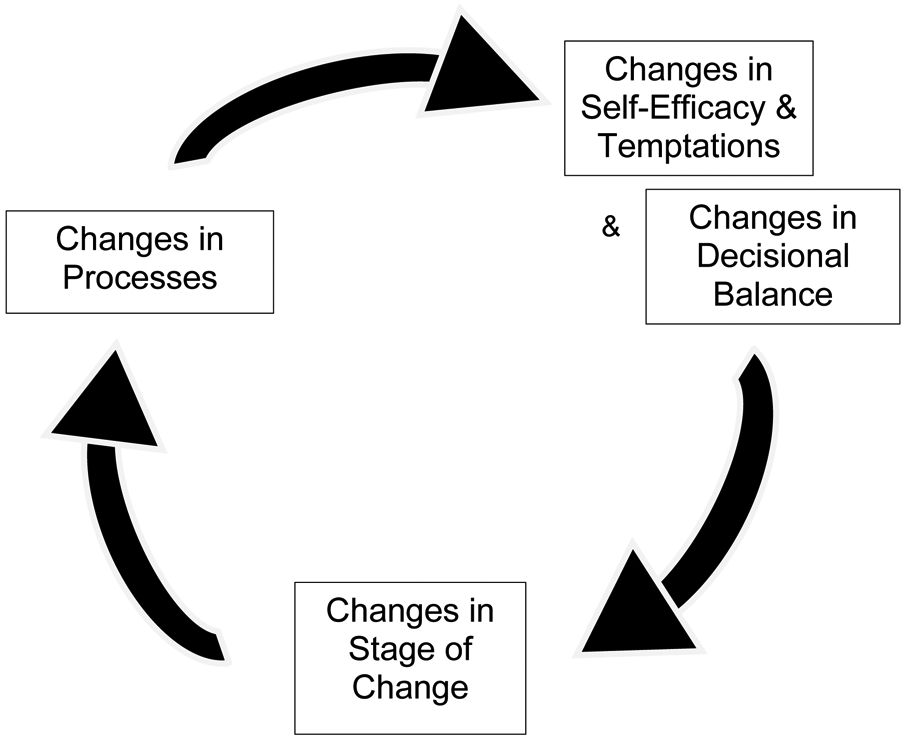
The cyclical model supported by findings from the analysis of five potential temporal sequences
Highlights.
The temporal sequencing of Transtheoretical Model (TTM) constructs was tested
Data on TTM constructs related to physical activity were collected over two years
A cyclical model where processes change initially led to cognition change was supported
Cognition change was followed by stage change, which led back to processes change
Renewed focus on processes is needed to further promote cognition change
Acknowledgements
This project was funded by the National Cancer Institute R01 CA109941 and a Cancer Education and Career Development Program (R25CA90956).
Footnotes
Declarations of interest: None
References
- Adams J, & White M (2003). Are activity promotion interventions based on the Transtheoretical Model effective? A critical review. British Journal of Sports Medicine, 37(2), 106–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adams J, & White M (2005). Why don't stage-based activity promotion interventions work? Health Education Research, 20(2), 237–43. doi: 10.1093/her/cyg105 [DOI] [PubMed] [Google Scholar]
- Bandura A (1997a). The anatomy of stages of change. American Journal of Health Promotion, 12(1), 8–10. [DOI] [PubMed] [Google Scholar]
- Bandura A (1997b). Self-efficacy - the exercise of control. New York: W.H. Freeman and Company. [Google Scholar]
- Bandura A (2004). Health promotion by social cognitive means. Health Education & Behavior, 31(2), 143–164. doi: 10.1177/1090198104263660 [DOI] [PubMed] [Google Scholar]
- Biddle SJH, & Nigg CR (2000). Theories of exercise behavior. International Journal of Sport Psychology, 31, 290–304. [Google Scholar]
- Brug J, Conner M, Harre N, Kremers S, McKellar S, & Whitelaw S (2005). The Transtheoretical Model and stages of change: a critique: Observations by five commentators on the paper by Adams, J. and White, M. (2004) Why don't stage-based activity promotion interventions work? Health Education Research, 20(2), 244–58. doi: 10.1093/her/cyh005 [DOI] [PubMed] [Google Scholar]
- Burkholder GJ, & Nigg CR (2002). Overview of the Transtheoretical Model. In Burbank P, Riebe D (Eds.), Promoting exercise and behavior change in older adults: Interventions with the Transtheoretical Model (pp. 57–84). New York, NY: Springer. [Google Scholar]
- Burnham KP, & Anderson DR (2002). Model selection and multimodel inference: A practical information-theoretic approach. New York, NY: Springer. [Google Scholar]
- Burnham KP, & Anderson DR (2004). Multimodel inference: Understanding AIC and BIC in model selection. Sociological Methods & Research, 33, 261–304. doi: 10.1177/0049124104268644 [DOI] [Google Scholar]
- Callaghan P, Khalil E, & Morres I (2010). A prospective evaluation of the Transtheoretical Model of change applied to exercise in young people. International Journal of Nursing Studies, 47(1), 3. doi: 10.1016/j.ijnurstu.2009.06.013 [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2009). Behavioral risk factor surveillance system: Prevalence and trend data nationwide. http://apps.nccd.cdc.gov/brfss/page.asp?cat=PA&yr=2009&state=US#PAAccessed 5 March 2014.
- Dishman RK, Thom NJ, Rooks CR, Motl RW, Horwath C, & Nigg CR (2009). Failure of post-action stages of the Transtheoretical Model to predict change in regular physical activity: A multiethnic cohort study. Annals of Behavioral Medicine, 37(3), 280–93. doi: 10.1007/s12160-009-9113-8 [DOI] [PubMed] [Google Scholar]
- Dishman RK, Vandenberg RJ, Motl RW, & Nigg CR (2010). Using constructs of the Transtheoretical Model to predict classes of change in regular physical activity: A multiethnic longitudinal cohort study. Annals of Behavioral Medicine, 40, 150–163. doi:0.1007/s12160-010-9196-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evers KE, Prochaska JO, Johsnon JL, Mauriello LM, Padula JA, & Prochaska JM (2006). A randomized clinical trial of a population- and Transtheoretical Model-based stress-management intervention. Health Psychology, 25(4), 521–529. doi: 10.1037/0278-6133.25.4.521 [DOI] [PubMed] [Google Scholar]
- Geller KS, Nigg CR, Motl RW, Horwath CC, & Dishman RK (2012). Transtheoretical Model constructs for physical activity behavior are invariant across time among ethnically diverse adults in Hawaii. Psychology of Sport and Exercise, 13(5), 606–613. doi: 10.1016/j.psychsport.2012.02.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gourlan M, Bernard P, Bortolon C, Romain AJ, Lareyre O, Carayol M, … Boiché J (2016). Efficacy of theory-based interventions to promote physical activity. A meta-analysis of randomised controlled trials. Health Psychology Review, 10, 50–66. 10.1080/17437199.2014.981777 [DOI] [PubMed] [Google Scholar]
- Hausenblas HA, Nigg CR, Dannecker EA, Symons DA, Ellis SR, Fallon EA, … Loving MG (2001). A missing piece of the Transtheoretical Model applied to exercise: Development and validation of the temptation to not exercise scale. Psychology & Health, 16, 381–390. [Google Scholar]
- Hellsten L, Nigg C, Norman G, Burbank P, Braun L, Breger R, … Wang T (2008). Accumulation of behavioral validation evidence for physical activity stage of change. Health Psychology, 27(1S), S43–S53. doi: 10.1037/0278-6133.27.1 [DOI] [PubMed] [Google Scholar]
- Herzog TA, Abrams DB, Emmons KA, & Linnan L (2000). Predicting increases in readiness to quit smoking: A prospective analysis using the contemplation ladder. Psychology and Health, 19, 369–381. doi: 10.1080/08870440008401999 [DOI] [Google Scholar]
- IBM Corp. (2013). IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp. [Google Scholar]
- Johnson SS, Paiva AL, Cummins CO, Johnson JL, Dyment SJ, Wright JA, … Sherman K (2008). Transtheoretical Model-based multiple behavior intervention for weight management effectiveness on a population basis. Preventive Medicine, 46(3), 238–46. doi: 10.1016/j.ypmed.2007.09.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB, & Santor DA (1999). Principles and practice of structural equation modelling. Canadian Psychology, 40(4), 381–383. [Google Scholar]
- Kosma M, Ellis R, & Bauer JJ (2012). Longitudinal changes in psychosocial constructs and physical activity among adults with physical disabilities. Disability and Health Journal, 5(1), 1–8. doi: 10.1016/j.dhjo.2011.09.002 [DOI] [PubMed] [Google Scholar]
- Lipschitz JM, Yusufov M, Paiva A, Redding CA, Rossi JS, Johnson S, … Prochaska JO (2015). Transtheoretical principles and processes for adopting physical activity: A longitudinal 24-month comparison of maintainers, relapsers, and nonchangers. Journal of Sport & Exercise Psychology, 37, 592–606. 10.1123/jsep.2014-0329 [DOI] [PubMed] [Google Scholar]
- Marcus BH, Simkin LR, Rossi JS, & Pinto BM (1996). Longitudinal shifts in employees' stages and processes of exercise behavior change. American Journal of Health Promotion, 10(3), 195–200. doi: 10.4278/0890-1171-10.3.195 [DOI] [PubMed] [Google Scholar]
- Marshall SJ, & Biddle JH (2001). The Transtheoretical Model of behavior change: A meta-analysis of applications to physical activity and exercise. Annals of Behavioral Medicine, 23(4), 229–246. doi: 10.1207/S15324796ABM2304_2 [DOI] [PubMed] [Google Scholar]
- Mastellos N, Gunn LH, Felix LM, Car J, & Majeed A (2014). Transtheoretical Model stages of change for dietary and physical exercise modification in weight loss management for overweight and obese adults. Cochrane Database of Systematic Reviews, 2(2), CD008066. doi: 10.1002/14651858.CD008066.pub3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthen LK, & Muthen BO (1998-2015). Mplus: Statistical analysis with latent variables (version 7.4). Los Angeles, CA: Muthén and Muthén. [Google Scholar]
- Nigg CR (2002). Physical activity assessment issues in population based interventions: A stage approach. In Welk GJ (Ed.), Physical activity assessments for health-related research (pp. 227–239). Champaign, IL: Human Kinetics. [Google Scholar]
- Nigg CR (2005). There is more to stages of exercise than just exercise. Exercise and Sport Science Reviews, 33(1), 32–35. [PubMed] [Google Scholar]
- Nigg CR (2001). Explaining adolescent exercise behavior change: A longitudinal application of the Transtheoretical Model. Annals of Behavioral Medicine, 23(1), 11–20. doi: 10.1207/S15324796ABM2301_3 [DOI] [PubMed] [Google Scholar]
- Nigg CR, Geller KS, Motl RW, Horwath CC, Wertin KK, & Dishman RK (2011). A research agenda to examine the efficacy and relevance of the Transtheoretical Model for physical activity behavior. Psychology of Sport and Exercise, 12(1), 7–12. doi: 10.1016/j.psychsport.2010.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nigg CR, & Riebe D (2002). The Transtheoretical Model: Research review of exercise behavior and older adults. In Burbank PM, & Riebe D (Eds.), Promoting exercise and behavior change in older adults: Interventions with the Transtheoretical Model (pp. 147–180). New York, NY: Springer. [Google Scholar]
- Noar SM, & Head KJ (2014). Mind the gap: Bringing our theories in line with the empirical data – a response to commentaries. Health Psychology Review, 8, 65–69. 10.1080/17437199.2013.855593 [DOI] [PubMed] [Google Scholar]
- Paxton RJ, Nigg CR, Motl RW, McGee K, McCurdy D, Horwath C, & Dishman RK (2008). Are constructs of the Transtheoretical Model for physical activity measured equivalently between sexes, age groups, and ethnicities? Annals of Behavioral Medicine, 35(3), 308–318. doi: 10.1007/s12160-008-9035-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plotnikoff RC, Hotz SB, Birkett NJ, & Courneya KS (2001). Exercise and the Transtheoretical Model: A longitudinal test of a population sample. Preventative Medicine, 33(5), 441–52. doi: 10.1006/pmed.2001.0914 [DOI] [PubMed] [Google Scholar]
- Prochaska JO, DiClemente CC, & Norcross JC (1992). In search of how people change. Applications to addictive behaviors. The American Psychologist, 47(9), 1102–14. doi: 10.1037/0003-066X.47.9.1102 [DOI] [PubMed] [Google Scholar]
- Prochaska JO, & Marcus BH (1994). The Transtheoretical Model: Applications to exercise. In Dishman RK (Ed.), Advances in exercise adherence (pp. 161–180). Champaign, IL: Human Kinetics. [Google Scholar]
- Prochaska JO, & Velicer WF (1997). The Transtheoretical Model of health behavior change. American Journal of Health Promotion, 12(1), 38–48. doi: 10.4278/0890-1171-12.1.38 [DOI] [PubMed] [Google Scholar]
- Prochaska JO, Velicer WF, DiClemente CC, & Fava J (1988). Measuring processes of change: Applications to the cessation of smoking. Journal of Consulting and Clinical Psychology, 56(4), 520–8. doi: 10.1037/0022-006X.56.4.520 [DOI] [PubMed] [Google Scholar]
- Romain AJ, Bortolon C, Gourlan M, Carayol M, Lareyre O, Ninot G, … Bernard P (2018). Matched or nonmatched interventions based on the transtheoretical model to promote physical activity. A metaanalysis of randomized controlled trials. Journal of Sport and Health Science. 10.1016/j.jshs.2016.10.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schumann A, Estabrooks PA, Nigg CR, & Hill J (2003). Validation of the stages of change with mild, moderate, and strenuous physical activity behavior, intentions, and self-efficacy. International Journal of Sports Medicine, 5, 363–365. doi: 10.1055/s-2003-40706 [DOI] [PubMed] [Google Scholar]
- Schumann A, Kohlmann T, Rumpf H, Hapke U, John U, & Meyer C (2005). Longitudinal relationships among Transtheoretical Model constructs for smokers in the precontemplation and contemplation stages of change. Annals of Behavioral Medicine, 30(1), 12–20. doi: 10.1207/s15324796abm3001_2 [DOI] [PubMed] [Google Scholar]
- Schumann A, Nigg CR, Rossi JS, Jordan PJ, Norman GJ, Garber CE, … Benisovich SV (2002). Construct validity of the stages of change of exercise adoption for different intensities of physical activity in four samples of differing age groups. American Journal of Health Promotion, 16(5), 280–287. [DOI] [PubMed] [Google Scholar]
- Spencer L, Adams TB, Malone S, Roy L, & Yost E (2006). Applying the Transtheoretical Model to exercise: A systematic and comprehensive review of the literature. Health Promotion Practice, 7(4), 428–43. doi: 10.1177/1524839905278900 [DOI] [PubMed] [Google Scholar]
- Trauth JM, Ling BS, Weissfeld JL, Schoen RE, & Hayran M (2003). Using the Transtheoretical Model to stage screening behavior for colorectal cancer. Health Education & Behavior, 30(3), 322–336. doi: 10.1177/1090198103030003007 [DOI] [PubMed] [Google Scholar]
- United States Department of Health and Human Services: Office of Disease Prevention and Health Promotion. (2008). Physical activity guidelines for Americans. https://health.gov/paguidelines/guidelines/Accessed 7 August 2016.
- Velicer WF, DiClemente CC, Rossi JS, & Prochaska JO (1990). Relapse situations and self-efficacy: An integrative model. Addictive Behaviors, 15, 271–283. doi: 10.1016/0306-4603(90)90070-E [DOI] [PubMed] [Google Scholar]
- West R (2005). Time for a change: Putting the Transtheoretical (stages of change) Model to rest. Addiction, 100, 1036–1039. doi: 10.1111/j.1360-0443.2005.01139.x [DOI] [PubMed] [Google Scholar]