

Abstract
Purpose. The goal of our study was to investigate the prevalence of late DDH cases in breech infants who had a normal screening hip ultrasound and subsequent follow-up hip x-ray imaging. Methods. Infants with a history of intrauterine breech position, normal hip ultrasound within 3-months of birth, and follow-up hip x-rays within 2-years were included. Acetabular indices were measured on a supine AP pelvis radiograph. Results. Fifty-six patients had breech presentation at birth, a normal hip ultrasound, and returned for radiographic evaluation within 2 years. Of those, 11/112 (10%) of hips had late DDH based on their radiographic images at 1 standard deviation greater than normative values from age-adjusted controls. No infants showed hip dysplasia at 2 standard deviations greater than normative values from age-adjusted controls. Conclusions. Our results support previous studies that follow up should be considered for infants with breech presentation and normal hip ultrasounds near birth. Level of evidence. II.
Keywords: developmental dysplasia of the hip, breech infant, hip radiology
Introduction
Developmental dysplasia of the hip (DDH) is one of the most common orthopedic conditions of the newborn and, left untreated, can lead to pain, gait abnormalities, increased intra-articular cartilage wear, and early-onset hip osteoarthritis.1 Early diagnosis of infant DDH is integral to care, as most cases can be treated nonoperatively with success. Delayed diagnosis can result in the need for invasive procedures and longstanding complications.2 In the United States, DDH is screened for with a physical examination at every well-child check-up until walking age.3 Imaging with ultrasound or x-ray is reserved for patients with one or more major risk factors or clinical signs.
Several risk factors for DDH at birth include maternal age, biological sex, birth order, birthweight, and the intrauterine breech position.4 Birth in the breech position is considered one of the greatest predictors of developing DDH, with estimates ranging between 2% and 27%.5-7 While there is little argument that breech presentation in the third trimester significantly increases the risk of DDH, several studies have attempted to elucidate whether a single screening hip ultrasound is sufficient to rule out DDH in this population.7-9 Three prominent research studies have emerged in recent years arguing that late DDH in breech infants who initially had a normal screening hip ultrasound occurs at much higher rates than previously thought7-9; however, the studies presented variable results and utilized a variety of criteria to define DDH. The goal of our study was to review our data to investigate the prevalence of late DDH cases in breech infants who had a normal screening hip ultrasound and subsequent follow-up hip x-ray imaging.
Methods
After the approval of our Institutional Review Board was obtained, records of all infants who had a history of intrauterine breech position and who presented to our institution for evaluation of their hips were reviewed. Infants were included in our study if they had a history of intrauterine breech position, had a normal hip ultrasound within 3-months of birth, and had a follow-up hip x-ray within 2-years. None of the included children had any interventions for their hips between the ultrasound and radiographs. A normal hip ultrasound was defined as an alpha angle greater than 60° with femoral head coverage greater than 50% and no subluxation with stress maneuver (Figure 1).10 Acetabular indices were measured on a supine AP pelvis radiograph by a single investigator (Figure 2).11 Late DDH was defined as having acetabular indices at least 1 standard deviations greater than normative values from age-adjusted controls.11
Figure 1.
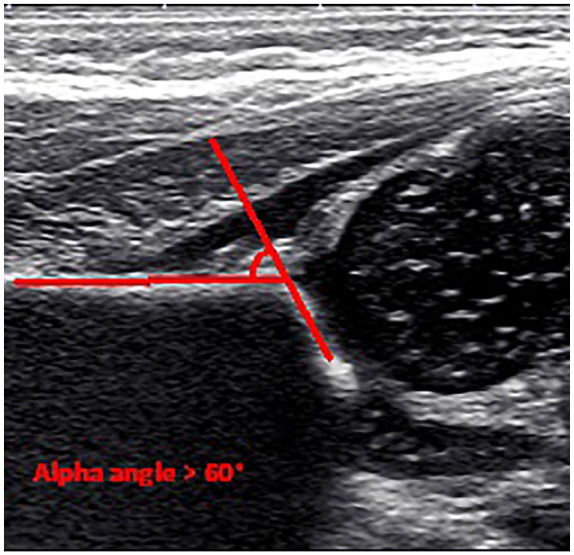
Normal acetabular angle on a hip ultrasound within 3 months of birth. Reproduced with permission from the Children’s Orthopaedic Center, Los Angeles.
Figure 2.
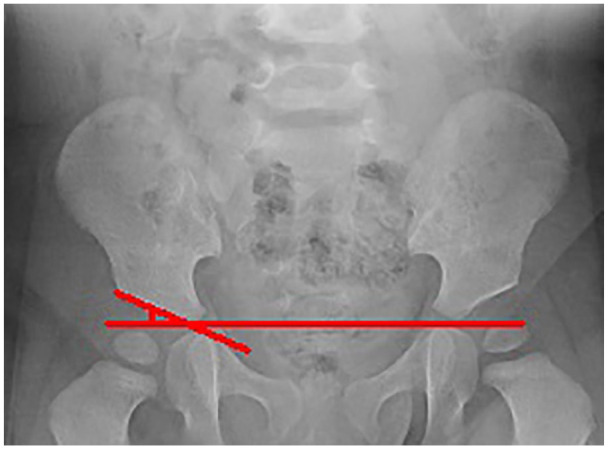
Measuring acetabular index. Reproduced with permission from the Children’s Orthopaedic Center, Los Angeles.
Statistical analysis was performed using StataIC 14 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP). Descriptive statistics were shown as means with standard deviations for continuous variables and proportions with percentages for categorical variables. Inferential statistics were performed using independent-sample t-tests.
Results
A total of 292 patients referred for evaluation of possible hip dysplasia were noted to have had breech presentation at birth. Of those patients, 56 (73% girls, and 27% boys) had a normal hip ultrasound and returned for radiographic evaluation within 2 years. The mean age at hip ultrasound was 8 weeks (range: 1-13 weeks), and the mean age at radiographic imaging was 10 months (range: 2-27 months) (Figure 3 and 4). The mean acetabular index was 20° (range: 9°-31°, Table 1). None of our infants were found to have late DDH based on their radiographic images at 2 standard deviations deviation greater than normative values from age-adjusted controls; however, 11/112 hips (10%) showed dysplasia at 1 standard deviation greater than normative values from age adjusted controls with a mean acetabular indices of 28° (range: 25°-31°) (Table 2 and 3). For those subjects, the mean age at the time of the ultrasound was 10 weeks (range: 5-13 weeks) and the mean age at the follow up x-ray was 10 months (range: 3-18 months).
Figure 3.

Mean acetabular angle by sex.
Figure 4.

AI and DDH incidence over time.
Table 1.
Descriptive Statistics for Hips of Breech Infants With a Normal Hip Ultrasound and Follow Up Hip X-Ray Within 2-Years of Birth.
| N = 56 infants | Proportion (%), Means ± SD |
|---|---|
| Sex | |
| Male | 15/56 (27) |
| Female | 41/56 (73) |
| Mean age at ultrasound, weeks | 8 ± 3 |
| Male, n = 15 | 7 ± 2 |
| Female, n = 41 | 8 ± 3 |
| Mean age at X-ray, months | 10 ± 5 |
| Male, n = 15 | 10 ± 4 |
| Female, n = 41 | 10 ± 5 |
| Mean hip angle, degrees | 22 ± 4 |
| Male, n = 15 | 20 ± 4 |
| Female, n = 41 | 22 ± 4 |
Table 2.
Incidence of Hip Dysplasia by Diagnostic Criteria.
| Diagnostic criteria | Incidence (%) | ||
|---|---|---|---|
| All (n = 112) | Male (n = 15) | Female (n = 41) | |
| AI > 1 SD above age- and sex-matched population mean | 11/112 (10) | 2/15 (13) | 9/41 (22) |
| AI > 2 SD above age- and sex-matched population mean | 0/112 (0) | 0/15 (0) | 0/41 (0) |
| AI ≥ 30° | 1/112 (1) | 0/15 (0) | 1/41 (2) |
Table 3.
Incidence of Hip Dysplasia by Diagnostic Criteria and Research Group.
| Diagnostic criteria | Incidence (%) | |||
|---|---|---|---|---|
| Our study | Brusalis et al8 | Imrie et al7 | Morris et al9 | |
| Mean age at X-ray, months | 10 ± 5 | 6.4 ± 0.5 | 4-6 | 13 ± 1 |
| AI > 1 SD above age- and sex-matched population mean | 20% (11/56) infants | 20.2% (19/94) hips | x | x |
| 10% (11/112) hips | ||||
| AI > 2 SD above age- and sex-matched population mean | 0% (0/56)infants | 4.3% (4/94 ) hips | 18% (24/131) infants | 8.3% (4/48) infants |
| 0% (0/112) hips | ||||
| AI ≥ 30° | 2% (1/56) infants | 10.6% (10/94) hips | x | x |
| 1% (1/112) hips | ||||
Discussion
Breech presentation is a known risk factor for infant hip dysplasia.4 Whether any differences exist in the rate of late dysplasia in breech infants compared to other at risk children is unclear. Previous studies have attempted to determine whether additional screening beyond an initial screening hip ultrasound is necessary in infant born via breech presentation. These studies have drawn variable conclusions utilizing a variety of definitions of hip dysplasia.
Eleven percent of hips in our study who were at risk for DDH due to intrauterine breech presentation, and who had a normal screening hip ultrasound, developed late DDH on radiographic imaging, though, like other studies, we had a high loss to follow up. These results echo recent studies; which all reported high rates of late DDH cases detected by follow-up radiographic imaging or exams. These studies showed a rate ranging between 4.3% and 29% of late dysplasia.7-9
One recent study measured the acetabular index of 94 infant hips from breech infants with normal ultrasounds at approximately 6-weeks and who had follow-up pelvic x-rays at approximately 6-months of age. They defined DDH as the single threshold of acetabular index (AI) ≥30. The authors reported that, using the single threshold value (AI ≥ 30°), 10/94 hips (10.6%) had DDH. This number was much higher than our own rate of 1/112 (<1%) at the threshold value. They also showed their results using AI stratified by sex and age as described by Tonnis et al. With this method, 19/94 (20.2%) hips with AI 1 standard deviation above the population mean had DDH and 4/94 (4.3%) hips with an AI 2 standard deviations above the population mean had DDH at 6-months.8 These results were comparable to our own, where 11/112 (10%) of hips with AI 1 standard deviation above the population mean had DDH, and 0/112 (0%) with an AI 2 standard deviations above the population mean had DDH. The difference in results at 2 standard deviations may be explained by our longer follow up time.
Another study examined DDH in a group of 314 breech infants. Of these 314 infants, 131 had normal ultrasounds at approximately 6-weeks of age and follow up pelvic x-rays and clinical exams at 4 to 6 months of age and were included in the final analysis. The authors determined if infants had DDH based on various radiographic parameters, including acetabular blunting and angular differences between hips. They found that, of the 131 infants included in the final analysis, 28 (29%) had DDH at 4 to 6 months.
A final study included 90 breech infants with normal hip ultrasounds. Patients were randomized into an observational or treatment arm, where patients in the treatment arm wore a Healthy Hip Diaper. Forty percent of patient elected to go against their randomization group. Hip x-rays were taken at approximately 13-months. DDH was defined as AI greater than 2 standard deviations above the population mean. Of the 48 infants in the observational arm included in the final analysis, 4 (8.3%) were found to have DDH at 13-months.9
In contrast to these other studies,7-9 we reported lower incidence of DDH at 2 standard deviations above the population mean, but comparable results at 1 standard deviation above the population mean. Our results varied potentially because of the longer length of time between the initial normal ultrasound and the follow x-ray in our study compared to recent studies, 2 of which had radiographic imaging at 4 to 6 months,7,8 whereas our mean age at the time of x-ray was 10 months. One study did have radiographs at 13-months; however, the study methods included randomization and interventions, and thus were very different from our study and other recent literature on radiographic imaging for breech infants.9
Similar to previous studies on this topic,7-9 this study was limited by a significant loss to follow up. Loss to follow up has been a limitation to many studies exploring hip development over time. This creates a potential for bias due to the possibility that the population lost to follow-up may be different at baseline than the population matriculated into the study.
Despite the limitations of our study, our results are still useful for helping to describe this at-risk population. Like previous studies and literature reviews on DDH in at-risk infants,12,13 we also contend that consistent diagnostic criteria need to be utilized for diagnosing DDH in order to make results comparable across studies. Finally, the late DDH cases in our population of breech infants with normal hip ultrasounds at birth suggests a need for follow up imaging for breech infants with initially normal ultrasounds. Studies that report follow up for these children would be helpful to show if this acetabular dysplasia remodels over time in order to offer clear guidelines for screening and follow-up of patients at risk for DDH.
Footnotes
Authors’ Note: This study has been carried out with approval from the Institutional Review Boards at Children’s Hospital Los Angeles and Boston Children’s Hospital.
Author Contributions: Antoniak K: data collection, study design, and macnuscipt writing. Lee C: data collection, and manuscript preparation. Goldstein R: manuscript review. Abousamra O: study design, and manuscript review.
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Goldstein AAOS—board member Pediatric Society of North America—board member.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs: Rachel Y. Goldstein  https://orcid.org/0000-0002-3691-7529
https://orcid.org/0000-0002-3691-7529
Oussama Abousamra
https://orcid.org/0000-0002-2815-4779
References
- 1.Sewell MD, Rosendahl K, Eastwood DM.Developmental dysplasia of the hip BMJ. 2009;339:b4454. [DOI] [PubMed] [Google Scholar]
- 2.Price KR, Dove R, Hunter JB.Current screening recommendations for developmental dysplasia of the hip may lead to an increase in open reduction. Bone Joint J. 2013;95-B(6):846-850. [DOI] [PubMed] [Google Scholar]
- 3.Committee on Quality Improvement, Subcommittee on Developmental Dysplasia of the Hip. Clinical practice guideline: early detection of developmental dysplasia of the hip. Pediatrics. 2000;105(4):896-905. [DOI] [PubMed] [Google Scholar]
- 4.Fitch RD.Ultrasound for screening and management of developmental dysplasia of the hip. N C Med J. 2014;75(2):142-145. [DOI] [PubMed] [Google Scholar]
- 5.Bache CE, Clegg J, Herron M.Risk factors for developmental dysplasia of the hip: ultrasonographic findings in the neonatal period. J Pediatr Orthop B. 2002;11(3):212-218. [DOI] [PubMed] [Google Scholar]
- 6.Barr LV, Rehm A.Should all twins and multiple births undergo ultrasound examination for developmental dysplasia of the hip? Bone Joint J. 2013;95-B(1):132-134. [DOI] [PubMed] [Google Scholar]
- 7.Imrie M, Scott V, Stearns P, Bastrom T, Mubarak SJ.Is ultrasound screening for DDH in babies born breech sufficient? J Child Orthop. 2010;4(1):3-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brusalis CM, Price CT, Sankar WN.Incidence of acetabular dysplasia in breech infants following initially normal ultrasound: the effect of variable diagnostic criteria. J Child Orthop. 2017;11(4):272-276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Morris AR, Thomas JMC, Reading IC, Clarke NMP. Does late hip dysplasia occur after normal ultrasound screening in breech babies? J Pediatr Orthop. 2019;39(4):187-192. [DOI] [PubMed] [Google Scholar]
- 10.Graf R.Fundamentals of sonographic diagnosis of infant hip dysplasia. J Pediatr Orthop. 1984;4(6):735-740. [DOI] [PubMed] [Google Scholar]
- 11.Tönnis D.Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop Relat Res. 1976;119:39-47. [PubMed] [Google Scholar]
- 12.Loder RT, Skopelja EN.The epidemiology and demographics of hip dysplasia. ISRN Orthop. 2011;2011:238607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bracken J, Tran T, Ditchfield M.Developmental dysplasia of the hip: controversies and current concepts. J Paediatr Child Health. 2012;48(11):963-973. [DOI] [PubMed] [Google Scholar]