

ABSTRACT
The emergence of the novel SARS-CoV-2 and COVID-19 has brought into sharp focus the need for a vaccine to prevent this disease. Vaccines have saved millions of lives since their introduction to the public over 200 years ago. The potential for vaccination reached new heights in the mid-20th century with the development of technologies that expanded the ability to create novel vaccines. Since then, there has been continued technological advancement in vaccine development. The resulting platforms provide the promise for solutions for many infectious diseases, including those that have been with us for decades as well as those just now emerging. Each vaccine platform represents a different technology with a unique set of advantages and challenges, especially when considering manufacturing. Therefore, it is essential to understand each platform as a separate product and process with its specific quality considerations. This review outlines the relevant platforms for developing a vaccine for SARS-CoV-2 and discusses the advantages and disadvantages of each.
KEYWORDS: COVID-19, manufacturing, platform development, vaccines
Introduction
The availability of vaccines, combined with the operational expertise and political commitment to administer them, is responsible for many of the most important achievements in public health in human history.1 A vaccine vanquished smallpox, the only human disease that has ever been eradicated.2 Polio, a scourge of children and parents in the early 20th century, is also on the verge of elimination because of vaccines.3 Another disease, measles, that primarily impacts children has been reduced to very low levels through effective vaccination campaigns. Vaccination against these three diseases saves ~8 million lives annually.1,4 Except maybe for clean drinking water, no other public health intervention saves as many lives as vaccinations do every year.5,6
The modern era of vaccination started in the late 18th century with Edward Jenner’s attempts to develop a smallpox vaccine.5 The “Golden Age” of vaccine development is more recent, however, beginning in the 1950s with the advent of virus propagation in cell culture.7 This technological breakthrough made vaccines such as Jonas Salk’s polio vaccine possible and has directly led to the diversity of vaccine development platforms today.8 To see this diversity on display, look no further than the variety of technologies being developed in the race to create a COVID-19 vaccine (Figure 1).
Figure 1.
Vaccine platforms being developed for COVID-19
The development of vaccines offers a unique set of challenges as compared to other drugs. Vaccines are usually administered to healthy people who may never have contracted the disease against which the vaccine offers protection. Therefore, vaccines have a higher bar for safety and tolerability than other drugs. While recipients might be willing to experience some discomfort at the injection site, severe reactions that occur with any sort of regularity will inhibit the use of the vaccine. Aversion to vaccines is a serious problem because a successful vaccination campaign requires a significant amount of compliance to achieve herd immunity, which is needed to stop the spread of the targeted disease.
Another problem is the fear of medical procedures involving injections. At over 12 billion injections per year, vaccinations are the most common painful medical procedures worldwide.9,10 It is not surprising then that a survey conducted in the United States (U.S.) for Target CVS Pharmacy in 2012 revealed that almost 15% of Americans avoid getting the flu vaccination because of a fear of needles.11 The survey results were consistent with estimates that needle phobia affects ~10% of the global population.10,12,13 Fear of needles is a significant contributor to vaccine hesitancy, a pressing public health concern worldwide.14,15 To fight noncompliance caused by needle fear, many vaccine manufacturers are developing a wide range of needle-free technologies that circumvent the problems associated with hypodermic injections.16
In addition to increasing compliance, needle-free technologies may also help reduce costs. A study by the Centers for Disease Control and Prevention (CDC), a federal agency in the United States (U.S.), found that administering a dose of measles vaccine with a patch instead of a typical needle injection would cut costs by almost 40% by reducing refrigeration costs and waste.17 These types of logistical issues are important to consider in carrying out a vaccination campaign. Vaccines are often administered in local clinics or by traveling health-care workers, and refrigeration can add to the challenge of mass immunization. Therefore, for any vaccine to impact a global pandemic like COVID-19, its development must consider issues of stability and affordability so that it can be administered throughout the world, especially in developing nations.
In addition to the innovative approaches for administering vaccines, there are also various novel platforms for manufacturing. These platforms have advantages and disadvantages, including differences in production, efficacy, safety profile, and immune response. Vaccine modalities include live, attenuated viruses, inactivated pathogens, protein subunit vaccines, polysaccharides, conjugate vaccines, DNA platforms, mRNA platforms, and viral vectors. The choice of platform for the vaccine plays a crucial role in both the elicited immune response and the duration of protection provided by the final product. Live, attenuated viral vaccines or virus-like particles can induce antibody responses that persist for several decades in the absence of subsequent antigen exposure and reactivation of immune memory. They also generate a T-cell response, which supports disease attenuation and protection against complications.
In contrast, the shortest immune responses are generally elicited by protein subunit antigens that primarily induce an antibody response to prevent infection. Vaccine protection can also be augmented by adding adjuvants, such as aluminum, to the final formulation to boost immunogenicity and modulate antibody persistence.18,19 An individual patient’s immune response to vaccination will depend on the vaccine platform and the adjuvant, among other factors.
For any vaccine technology platform to be viable, it must demonstrate that it can be efficacious. Determining vaccine efficacy requires the formal demonstration that vaccine-mediated protection is dependent on the presence of a given marker, such as an antibody titer, or several antigen-specific cells above a given threshold.20 For the most part, however, vaccine-mediated protection against certain infectious diseases is a complex challenge that has mostly been developed empirically. The efficacy of vaccines is primarily conferred by the induction of antigen-specific antibodies whose quality is determined by their avidity, specificity, and neutralizing capacity. Ideally, one would want vaccine-induced responses to be sufficiently broad to extend protection to nonvaccine strains of the same pathogen (e.g., influenza, rotavirus, Streptococcus pneumoniae, or human papilloma virus (HPV)) yet sufficiently restrained so as not to elicit cross-reactions to allergens and self-antigens or other undesirable nonspecific effects. Nonspecific effects of vaccinations have been reported and they can cause concern over immune overload and increased vulnerability to infections.21,22 These fears are not supported by any direct evidence, however.21,23
The COVID-19 pandemic has led to an increased interest in using many technology platforms to deliver suitable vaccines (Figure 1). This article will provide an overview of the various vaccine platforms being used for COVID-19 and discuss their advantages and disadvantages. Table 1 lists examples of vaccines under development using different platform technologies. The review also discusses the regulatory status of some of the vaccine products, with a specific focus on those currently in clinical trials. We recognize the complexity of global regulatory pathways; so to simplify this review, we predominantly reference the regulatory framework used in the U.S. as an example to illustrate how a vaccine may be approved for human use. Some of the vaccine products in development may not be approved and marketed in the U.S. but may be available in other countries. Regardless, the challenges and opportunities discussed herein are the same.
Table 1.
COVID-19 Vaccine Candidates in Development, Grouped by Platform
| Platform | Developer (Vaccine Name or Type and adjuvant, if reported) | Dosesa | Clinical Stageb |
|---|---|---|---|
| Inactivated Virus | Sinovac Research and Development Co., Ltd (CoronaVac) | 2 | EUAC |
| Sinopharm, China National Biotec Group Co., Wuhan Institute of Biological Products | 2 | EUAC | |
| Sinopharm, China National Biotec Group Co., Beijing Institute of Biological Products | 2 | EUAC | |
| Institute of Medical Biology, Chinese Academy of Medical Sciences | 2 | Phase 3 | |
| Research Institute for Biological Safety Problems, Rep of Kazakhstan (QazCovid-in®) | 2 | Phase 3 | |
| Bharat Biotech International Limited (BBV152) | 2 | Phase 3 | |
| Beijing Minhai Biotechnology Co. | 1–3 | Phase 2 | |
| Valneva, National Institute for Health Research, United Kingdom (VLA2001) | 2 | Phase 1/2 | |
| Erciyes University (ERUCOV-VAC) | 2 | Phase 1 | |
| Viral Vector | AstraZeneca, University of Oxford (ChAdOx1-S – (AZD1222), Covishield) | 1–2 | EUAEU |
| CanSino Biological Inc., Beijing Institute of Biotechnology (Adenovirus type 5 vector) | 1 | Phase 3 | |
| Gamaleya Research Institute, Health Ministry of the Russian Federation (Gam-COVID-Vac (rAd26-S+ rAd5-S)) | 2 | EUAR | |
| Janssen Pharmaceutical (Johnson & Johnson) (Ad26.COV2.S) | 1–2 | Phase 3US, EU | |
| ReiThera, Leukocare, Univercells (GRAd-COV2) | 1 | Phase 1 | |
| Vaxart (VXA-CoV2-1 Ad5 adjuvanted oral platform) | 2 | Phase 1 | |
| University of Munich (Ludwig-Maximilians) (MVA-SARS-2-S) | 2 | Phase 1 | |
| Merck & Co., Themis, Sharp & Dohme, Institute Pasteur, University of Pittsburgh (V591-001) | 1–2 | Development Halted | |
| University of Hong Kong, Xiamen University, Beijing Wantai Biological Pharmacy (DelNS1–2019-nCoV-RBD-OPT1) | 1 | Phase 2 | |
| Shenzhen Geno-Immune Medical Institute (Covid-19/aAPC) | 3 | Phase 1 | |
| Shenzhen Geno-Immune Medical Institute (LV-SMENP-DC) | 1 | Phase 1/2 | |
| ImmunityBio, Inc., NantKwest, Inc. (hAd5-S-Fusion+N-ETSD) | 1–2 | Phase 1 | |
| City of Hope Medical Center, National Cancer Institute (COH04S1 (MVA-SARS-2-S)) | 1–2 | Phase 1 | |
| Israel Institute for Biological Research (rVSV-SARS-CoV-2-S) | 1 | Phase 1/2 | |
| Aivita Biomedical, National Institute of Health Research and Development, Ministry of Health Republic of Indonesia (Dendritic cell vaccine AV-COVID-19) | 1 | Phase 1/2 | |
| Cellid Co., Ltd. (AdCLD-CoV19) | 1 | Phase 1/2 | |
| Altimmune, Inc. (AdCOVID) | 1–2 | Phase 1 | |
| VLP | Serum Institute of India, Accelagen Pty, SpyBiotech (RBD SARS-CoV-2 HBsAg) | 2 | Phase 1/2 |
| Medicago Inc. (CoVLP) | 2 | Phase 2/3 | |
| Subunit | Novavax (SARS-CoV-2 rS & Matrix M1 adjuvant) | 2 | Phase 3 |
| Anhui Zhifei Longcom Biopharmaceutical, Institute of Microbiology, Chinese Academy of Sciences | 2–3 | Phase 3 | |
| Kentucky Bioprocessing Inc. (KBP-COVID-1, receptor binding domain-based) | 2 | Phase 1/2 | |
| Sanofi Pasteur, GSK (spike protein formulation with adjuvant) | 2 | Phase 1/2 | |
| Clover Biopharmaceuticals Inc., GSK, Dynavax (SCB-2019 & AS03 or CpG 1018 and alum adjuvant) | 2 | Phase 2/3 | |
| Vaxine Pty Ltd. (COVAX-19® spike protein & adjuvant) | 1 | Phase 1 | |
| CSL Ltd. + Seqirus, University of Queensland (UQ-CSL V451 & MF59 adjuvant) | 2 | Development Halted | |
| Medigen Vaccine Biologics, Dynavax, National Institute of Allergy and Infectious Diseases (NIAID) (MVC-COV1901, S protein & CpG 1018 adjuvant) | 2 | Phase 2/3 | |
| Instituto Finlay de Vacunas (FINLAY-FR, receptor binding domain-based & adjuvant) | 2 | Phase 2 | |
| Federal Budgetary Research Institution State Research Center of Virology and Biotechnology “Vector” (EpiVacCorona peptide antigens) | 2 | Phase 1/2 | |
| West China Hospital, Sichuan University (receptor binding domain-based) | 2 | Phase 2 | |
| University Hospital Tuebingen (IMP CoVac-1, SARS-CoV-2 HLA-DR peptides) | 1 | Phase 1 | |
| COVAXX, United Biomedical, Inc. (UB-612 (spike protein & receptor binding domain-based) | 2 | Phase 2/3 | |
| Adimmune Corporation (AdimrSC-2f, receptor binding domain-based with and without aluminum) | Unknown | Phase 1 | |
| Center for Genetic Engineering and Biotechnology (CIGB) (CIGB-669, receptor binding domain-based & AgnHB) | 3 | Phase 1/2 | |
| Center for Genetic Engineering and Biotechnology (CIGB) (CIGB-66, receptor binding domain-based & aluminum hydroxide) | 3 | Phase 1/2 | |
| Biological ELimited (BECOV2) | 2 | Phase 1/2 | |
| Nanogen Pharmaceutical Biotechnology (S protein & aluminum adjuvant) | 2 | Phase 1/2 | |
| Shionogi (S-268019) | 2 | Phase 1/2 | |
| University Medical Center Groningen, Akston Biosciences Inc. (receptor binding domain-based Fc fusion protein) | Unknown | Phase 1/2 | |
| Vaccine and Infectious Disease Organization (VIDO), Seppic, Vaccine Formulation Institute (VFI) (COVAC-1/COVAC-2, spike protein & SWE adjuvant) | 2 | Phase 1/2 | |
| DNA | Inovio Pharmaceuticals + International Vaccine Institute, Advaccine (Suzhou) Biopharmaceutical Co., Ltd. (INO-4800 & electroporation) | 2 | Phase 2/3 |
| AnGes + Takara Bio, Osaka University (AG0301-COVID19) | 2 | Phase 2/3 | |
| Zydus Cadila (nCov vaccine) | 3 | Phase 3 | |
| Genexine Consortium (GX-19) | 2 | Phase 1/2 | |
| Entos Pharmaceuticals Inc. (Covigenix VAX-001) | 2 | Phase 1 | |
| Providence Health & Services (CORVax – S Protein Plasmid DNA Vaccine) | 2 | Phase 1 | |
| Symvivo Corporation (bacTRL-Spike oral DNA vaccine) | 1 | Phase 1 | |
| GeneOne Life Science, Inc. (GLS-5310) | 2 | Phase 1/2 | |
| RNA | Moderna + National Institute of Allergy and Infectious Diseases (NIAID) (mRNA −1273) | 2 | EUAUS |
| Pfizer/BioNTech, Fosun Pharma (BNT162, 3 LNP-mRNAs) | 2 | EUAUS, EU | |
| CureVac AG (CVnCoV) | 2 | Phase 3 | |
| Arcturus Therapeutics (ARCT-021) | Unknown | Phase 2 | |
| Imperial College London (LNP-nCoVsaRNA) | 2 | Phase 1 | |
| Academy of Military Science (AMS), Walvax Biotechnology and Suzhou Abogen Biosciences (ARCoV) | 2 | Phase 1 | |
| Chulalongkorn University (ChulaCov19) | 2 | Phase 1 | |
| Live, Attenuated | Codagenix/Serum Institute of India (COVI-VAC) | 1-2 | Phase 1 |
EUA, Emergency Use Authorization in; C, China, R, Russia; US, United States; EU, European Union & United Kingdom; note, these vaccines may also be approved for use in other countries.
aMost vaccine candidates will require two doses administered 14 to 56 days apart.
bClinical phase of development as reported by WHO on February 2, 2020 (DRAFT landscape of COVID-19 candidate vaccines). www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines.
Vaccine biology
Regardless of the manufacturing technology, a vaccine works by first stimulating an inflammatory reaction from cells in the innate immune system.24–26 The first step involves activating immature dendritic cells (DCs), a group of antigen-presenting cells (APCs) that patrol the body looking for foreign antigens. Following injection, the vaccine rapidly disseminates throughout the vascular network to reach the target tissues. This pattern is very similar to that occurring after a natural infection, including the initial mucosal replication stage for vaccines administered through the nasal and oral routes.21 When exposed to the vaccine antigen, DCs undergo maturation and modulate specific surface receptors. The DCs then migrate toward secondary lymph nodes, where they trigger B and T cells, lymphocytes equipped with surface receptors capable of binding to antigens.27,28
The interaction with the secondary lymph nodes induces a highly efficient B cell differentiation pathway through specific germinal centers (GCs). Antigen-specific B cells undergo massive clonal proliferation and become antibody-secreting plasma cells.29 A small subset of B cells experience extensive somatic hypermutation within the variable-region segments of their immunoglobulin (Ig) genes.30 The mutations increase the affinity of the surface IgGs for the antigen, allowing B cells to mediate protection by induction of highly specific serum antibodies. B cells also process vaccine antigens into small peptides that they display at their surface through major histocompatibility complex (MHC) class II molecules. MHC-peptide complexes thus become available for binding by the specific follicular T-helper (Tfh) cells, located in the lymph nodes that support potent B cell activation and differentiation into antibody-secreting-cells, and also mediate adjuvanticity.31–36
Given the significance of B cells, it is possible to underestimate the importance of T cell responses in vaccine efficacy. However, T cells play an essential role in the induction and persistence of high-affinity antibodies required for long-term protection. They also reduce, control, and clear extracellular and intracellular pathogens through cytokine-production. The T cell response is mediated by CD4 + T-helper (Th) lymphocytes. Th cells limit the spread of infectious agents by recognizing and killing infected cells or secreting specific antiviral cytokines such as interferon (IFN)-γ, tumor necrosis factor (TNF)-α/TNF-β, and interleukin 2 (IL-2) in response to viral infections.37,38 The generation of the CD4 + Th cell response begins when DCs capture an antigen in peripheral tissue and then migrate to draining lymph nodes, where T cell vaccine responses are elicited in parallel to B cell responses.
Much of the orthodoxy surrounding vaccine development assumes that individuals have unlimited repertoires of receptors for antigen recognition in their B cells and T cells. However, the actual repertoire diversity is probably less than optimal, and situations exist where few B or T cells can bind to a given antigen. The absence of diversity in these cases acts to limit vaccine efficacy. Therefore, evaluating a vaccine platform requires appraising how it elicits, supports, and maintains each cell type’s responses. Assuming that it is possible to predict the B and T cell response to a given immunogen, vaccine strategies could be optimized and personalized.39
COVID-19 biology and vaccine development
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2, Figure 2) that causes COVID-19 is an enveloped, positive-sense, single-stranded RNA virus.40 Through its trimeric spike (S) protein, it binds to angiotensin-converting enzyme 2 (ACE-2) on the surface of various human cells.41 The virus then fuses with the mammalian cell and localizes to the endoplasmic reticulum-Golgi, where it releases its nuclear material.42 The virus replicates and reforms as small vesicles that can be exported out of the cell by endocytosis.43
Figure 2.
SARS-CoV-2
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes the respiratory illness known as coronavirus disease 2019 (COVID-19). SARS-CoV-2 is an envelope virus 50–200 nanometers in diameter. It expresses several genes required for transmission and propagation, including those encoding spike (S) proteins  that allow the virus to attach to and fuse with the infected host’s cells. The RNA genome
that allow the virus to attach to and fuse with the infected host’s cells. The RNA genome  is organized and maintained within the envelope.
is organized and maintained within the envelope.
Under normal circumstances, a single vaccine platform usually becomes the de facto technology to address a specific pathogen. However, the COVID-19 pandemic has created a unique situation in which dozens of companies are racing to develop vaccines based on different platforms.44 Historically, four platforms (inactivated pathogen vaccines, recombinant subunit vaccines, conjugate vaccines and attenuated virus vaccines) have made up the bulk of vaccine products. Each of these platforms has unique advantages that provide significant public health benefits. Indeed, several COVID-19 vaccines are being developed that rely on inactivated SARS-CoV-2 virus (Table 1). These traditional platforms also pose specific challenges.
In response to COVID-19, manufacturers are also looking at newer technologies that seek to avoid the safety and efficacy concerns associated with some of the more traditional approaches to vaccine development. Many of these new platforms have not been widely used, but proof of concepts have been demonstrated for some of them.45 A few subunit and viral vector vaccines are already in use for other infections, and there are currently over a dozen of these vaccines for COVID-19 in clinical trials based on these platforms.46 On the other hand, all of the RNA and DNA vaccines being developed, including the ten vaccine candidates in clinical trials for COVID-19, are entirely new and have never been approved for use in humans.47 In this review, we highlight each vaccine platform’s key features and examine the advantages and challenges associated with each.
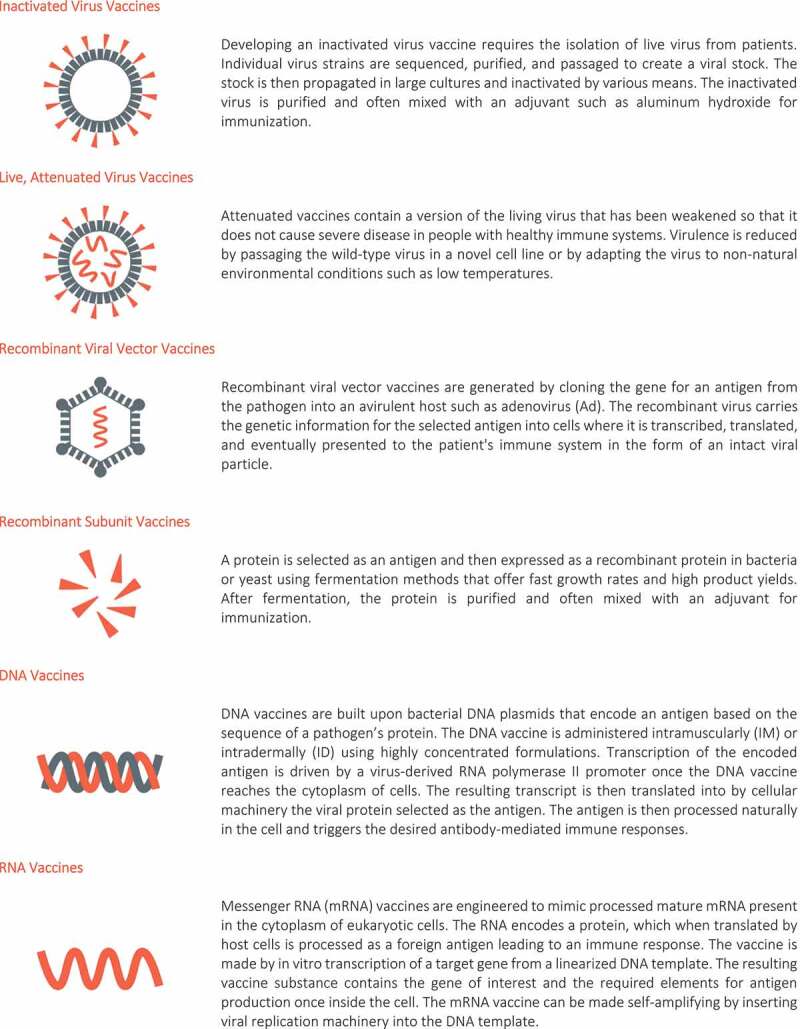
Inactivated pathogen vaccines
Some of the earliest vaccines were made by inactivating the pathogenic bacterium, parasite, or virus using various methods followed by administration of the inactive pathogen as the vaccine antigen. Today, the inactivation process is often carried out using radiation or a chemical agent. Inactivation prevents replication of the pathogen, so the vaccines based on this platform cannot cause disease and are usually considered safer than other platforms, such as live and attenuated virus vaccines.48
To make an inactivated viral vaccine, an individual viral strain is first isolated, sequenced, plaque purified, and passaged in a mammalian cell line to create a viral stock. The genetic stability of the virus is monitored through several more passages. The virus is then propagated in a multi-liter culture and inactivated by using a wide range of reagents or methods, including ascorbic acid, hydrogen peroxide, gamma irradiation, UV treatment, heat, formaldehyde, and β-Propiolactone (BPL).49–54 The inactivated virus is purified from cell culture using filtration and chromatography. Homogeneity is confirmed using cryo-electron microscopy and other release assays. The inactivated virus is often mixed with an adjuvant such as aluminum to enhance the immunogenicity of the final vaccine product. These procedures preserve the structure of the pathogen’s protective epitopes, but remove the pathogen’s ability to replicate or recover virulence, if performed correctly.
Inactivated vaccines, such as the polio vaccine, produce immune responses by stimulating not only humoral immunity featuring neutralizing antibodies but also promoting cellular immune responses similar to what would be seen for live viruses, through the preservation and cross-presentation of conserved internal viral epitopes to cytotoxic T cells (CTLs), through MHC class 1 pathway.7,48,55,56 Immunity is activated by recognizing the viral pathogen-associated molecular patterns (PAMPs), using innate immune cell receptors such as toll-like receptor (TLR) 7, which can induce T-cell-mediated immune responses.55,57
Due to the maintenance of the functional viral domains during inactivation, the immune response is similar to that which occurs in living viruses. First, viral degradation occurs in the endosome following the exogenous pathway or the cross-presentation pathway. Next, viral membrane fusion occurs following the endogenous pathway. The mentioned pathways, along with the recognition of viral PAMPs, using pattern recognition receptors (PRRs) such as TLR7 and RIG-1, and the production of cytokines such as IFN-1, can promote potent cellular-mediated immune responses.
Advantages
Inactivated vaccines have been used for over a century, and the pharmaceutical industry understands their production well.58 These vaccines have a better safety profile than live, attenuated vaccines, and immunosuppressed patients can generally use them because they do not cause the disease state. There are several inactivated vaccines currently licensed to protect against six different viral pathogens.59 The history of inactivated vaccine manufacturing, safety, and performance also facilitate acceptance by regulatory agencies.
Vaccine manufacturers can also take advantage of continuous cell lines to reduce production costs during scale-up.60 Inactivated vaccines also tend to be more stable than other platforms, making them less sensitive to cold chain disruptions. Therefore, storage conditions are not as critical. Finally, inactivated vaccines can also be administered using needle-free technology. For example, the inactivated influenza vaccine, Afluria (manufactured by bioCSL Pty Ltd.), is approved for use with a jet injector device, the PharmaJet Stratis Needle-free Injection System by PharmaJet Inc. for intramuscular injection.61 Another inactivated influenza vaccine, Fluzone Intradermal, manufactured by Sanofi Pasteur Inc., is approved for intradermal administration with its supplied microinjection system.62
Challenges
Inactivated vaccines tend to be less immunogenic than live, attenuated vaccines because the inability to replicate limits vaccine-induced activation of DCs. Inactivated vaccines can only activate innate responses at the injection site, making the site and administration route critical.21 Vaccination also generally requires multiple doses of the vaccine to achieve and maintain protective immunity.63 Therefore, a larger first dose, often followed by a booster dose, is usually needed to achieve the desired immunity.
Larger and repeat doses of inactivated vaccines generally require a lot of infectious material to be manufactured before inactivation, so the pathogen for use in inactivated vaccines must be amenable to being cultured in large quantities in various commercial production systems. Manufacturing systems include chicken eggs (for influenza vaccine), bacterial fermenters, or bioreactors using suspension cells. As with all vaccines, these approaches can be expensive and require significant commitments of time and facilities.20
Other limitations of inactivated vaccines include a lack of cross-protection due to the induction of strain-specific neutralizing antibody responses, inadequate responses to immunization among high-risk groups like the elderly, a long production period, and a high prevalence of antigenic changes in the target viruses.21,22 The inadequate response to immunization by inactivated virus may also be due to the choice of adjuvant, which needs to target the correct age group.24 A more significant issue is that killed vaccines offer limited protection against intracellular pathogens. Because the vaccine organism is dead, it cannot actively penetrate host cells. The processing of the organism’s antigens by the endogenous processing pathway and subsequent presentation on MHC class I are therefore limited. As a result, T cell activation and CTL generation by this vaccine platform do not occur. A DC that has phagocytosed the killed vaccine may cross-present peptides derived from the inactivated pathogen. Still, any generated levels of peptide-MHC class I activate only a limited number of T cells.
Live, attenuated vaccines
Live attenuated vaccines have been developed to protect against both viruses and bacteria.63 In contrast to other platforms, these vaccines contain a weakened version of the live virus or bacteria that does not cause severe disease in people with healthy immune systems. The reduced virulence of live, attenuated vaccines is often created by passaging the wild-type virus into a novel cell line or adapting the virus to non-natural environmental conditions such as low temperatures.64 Because live, attenuated vaccines are closest to a natural infection, they act as suitable primers for the immune system to develop protection against natural disease. Examples of live, attenuated vaccines include the measles, mumps, and rubella vaccine (MMR), varicella (chickenpox) vaccine, and cold-adapted influenza vaccine (Flumist®).
Since these vaccines can be designed to target various pathogens, they likely signal through several different TLRs, expressed by DCs.65,66 Several studies have examined the receptors that sense pathogens, but only a few have examined those that detect live attenuated vaccines.67 Even fewer studies have examined how these receptors influence the adaptive immune responses to the live vaccines. For example, the Bacillus Calmette-Guérin (BCG) vaccine for tuberculosis activates DCs via multiple TLRs, but it is unknown whether TLR signaling is required for adaptive immunity.68 The yellow fever vaccine, YF-17D, is also known to activate various TLRs (TLR2, TLR3, and TLR7-9).69 Signaling via particular combinations of TLRs results in synergistic activation of DCs.70 On the other hand, live, attenuated influenza vaccines, first introduced in the 1960s, seems to require only TLR7-mediated production of type I IFN by DCs for their immunogenicity.71,72 It is unknown whether the live, attenuated influenza vaccine triggers the same TLRs as the wild-type virus to activate antigen-specific antibodies and CD4+ and CD8 + T cell responses.57,73
Regardless, manufacturers have developed technologies to create live, attenuated influenza vaccines that confer long-term immunity.7 This is especially important when considering vaccines for vulnerable populations. For example, until recently, an inactivated influenza vaccine, rather than a live vaccine, was the standard for pediatric vaccination even though it did not provide lasting local or cellular immunity.74 A live, attenuated vaccine for flu was finally approved for children in 2004.75
Advantages
Live, attenuated vaccines can be very effective. Since a viable pathogen is used, a single dose is often enough to induce long-lasting immunity because the infectious agent can replicate in the host. Also, the innate immune system is triggered through pathogen-associated signals, such as viral RNA, allowing recognition by TLRs.69 The result is the secretion of cytokines that create a general inflammatory milieu against all potential antigens. For example, the BCG vaccine can be used as an immune therapy for bladder cancer because of its capacity to stimulate a localized immune response when administered directly to the bladder.76 The preservation of viral replication has another advantage: large quantities of the pathogen’s antigen are synthesized and accumulate in the host. Thus, only small amounts of the actual vaccines need to be administered, thereby maximizing cost-effectiveness.
The cost of vaccinations and single-dose courses are significant issues for vaccination in developing countries. Funding for vaccines in these countries is often constrained, and returning to an immunization clinic for a booster dose may present insurmountable logistical barriers.77,78 Finally, recent technological breakthroughs have begun to replace the need for needle injections. For example, the live attenuated influenza vaccine, Flumist®, can be administered as a nasal spray.61
Challenges
The principal risk with an attenuated vaccine is that it can sometimes recover its virulence.78 Under rare circumstances, one of the three attenuated viral strains comprising the Sabin oral polio vaccine can revert to virulence after passing through the human intestinal tract.77 Another concern is that live, attenuated vaccines are grown in large quantities in culture vessels. Other organisms may contaminate the culture during this process and become incorporated into the vaccine. These contaminants cannot be inactivated in downstream processes since the vaccine itself is not completely inactivated during manufacturing. The human oncogenic virus, SV40, a simian virus, was discovered as a contaminant in early preparations for the Sabin polio vaccine attenuated by passage through monkey kidney cells.79,80
Processes used to manufacture live vaccines can also introduce contaminants. A flawed manufacturing process led to contamination of a yellow fever vaccine with hepatitis B virus in Brazil from 1938 to 1940, and then again in 1942 among US military personnel.81,82 In both these situations, pooled human serum had been used as a vaccine stabilizer, but the serum had been contaminated with the hepatitis B virus.
Even when properly manufactured, however, live, attenuated vaccines can induce transient immunosuppression in healthy individuals. Therefore, the vaccinated person becomes vulnerable to natural infections that should be easily fended-off. For example, it was discovered that vaccination with a no longer attenuated strain of measles virus rendered patients unusually susceptible to pneumonia, diarrhea, and parasitic infections.77 Live, attenuated vaccines also cannot be safely administered to people with already weakened immune systems, like patients undergoing chemotherapy, since their immune systems may be overwhelmed even by the weakened pathogen.
Finally, storage conditions are critical for live, attenuated vaccines because they are composed of a living organism. The cold chain from manufacturer to site of injection must be maintained, which can be a significant challenge in many developing countries.78
Viral vectors
The use of attenuated viruses can be risky for pathogens such as HIV, Ebolavirus, Zika virus, and SARS-CoV-2 because of the risk that these highly pathogenic organisms may revert to their pathogenic form.23 For these viruses, a safer alternative is to develop a recombinant viral vector vaccine that mimics the natural pathogen but is not virulent. To make this type of vaccine, an antigen from the target pathogen is chosen and then cloned into an avirulent viral host.83,84 Several recombinant viral vectors derived from other viruses have emerged as gene delivery systems for therapeutic intervention and vaccination. All of them have shown advantages and limitations depending on the medical application.
Numerous clinical trials have been initiated with vectors from adenovirus (Ad), vesicular stomatitis virus (VSV), and cytomegalovirus (CMV).85,86 These host-virus genomes carry out all the viral transmission and amplification functions, including antigen production, to present the chosen antigen to the patient’s immune system. In particular, the Ad vectors have been extensively tested as vaccine delivery systems in several preclinical and clinical studies for various infectious diseases, including rabies, HIV-1, malaria, hepatitis C virus (HCV), and influenza.87–92
The most widely used method in viral vector development involves homologous recombination.93 In this system, the E1 transcription unit of the Ad virus is deleted to reduce the risk of generating a replication-competent virus.94 Deletion of the E1 does not mitigate all risk, however. These E1-deficient viral vectors are then propagated through mammalian cells, such as a modified human embryonic kidney cell line known as HEK 293, which can still result in a small amount of contamination with replication-competent adenovirus.95 This can create significant issues with quality control in preparing vaccines for human applications.96 To circumvent this issue, developers can use direct molecular cloning as an alternative strategy.97 Microcarrier bioreactor systems and suspension cell culture bioreactor systems are used for large-scale cultivation of various cell lines that support the growth of viral vectors.98 The bulk material is nuclease-treated, and a two-step process involving sequential chromatography or chromatography-tandem ultracentrifugation/filtration is then used to remove process-related impurities.99
Successful protection against a pathogen may require neutralizing antibodies, effective T cell responses, or both.100 In general, viral vectors induce the necessary strong antibody responses as well as a response from CTLs, including CD8 + T cells. The T cell response is critical in controlling intracellular pathogens but is not triggered by the traditionally purified inactivated or subunit vaccines.101 Ad vectors being developed as vaccines against HIV and malaria are among the most potent for inducing CD8 + T cell responses. These vaccine candidates engage in multiple redundant signaling pathways even though the specific TLRs involved remain to be identified.83
Advantages
The main advantage of viral vector-based vaccines is the ability to present protective antigen epitopes in the context of a live, replicating virus without concern about reversion to a pathogenic state. This presentation leads to a more robust immune response and allows for antigen sparing as the viral vectors have limited reproductive activity. The ability to scale-up and purify recombinant viral vectors for clinical studies has become a much more standardized practice due to the availability of quality-controlled production cell lines, which generate high titer viral batches.33 Furthermore, the cell lines can be grown in bioreactor systems used for large-scale cultivation to produce high cell densities of up to 5–10 × 106 cells per milliliter.30,34,35 The combination of increased cell density and high viral titers results in higher yields, making harvesting, downstream processing, quality assurance, and process control more efficient. The result is lower production costs per vial of vaccine.
Various chromatographic techniques can be used to purify the bulk vaccine substance, including affinity chromatography, anion-exchange chromatography, size-exclusion chromatography, and membrane chromatography.36–40 The use of highly scalable clinical-grade purification strategies allows for the generation of high purity and quality vaccine stocks without any adverse impact on the viral vector infectivity, yield, and purity.30,35 The entire process from the identification of the protective epitopes for the vaccine virus to formulation and filling takes approximately twelve weeks, which is crucial during a pandemic when large quantities of highly purified vaccine are needed quickly.31
Challenges
The immunogenic properties result from both the encoded antigen and the viral vector that carries the antigen recognized by the immune system. The addition of genetic material that encodes other viral proteins can lower or modify the vaccine’s efficacy by diverting immune responses away from the target antigens. Also, the antigen itself does not participate in any of the recombinant viruses’ functions. Because it is not essential, the replicating virus could jettison the antigen encoding sequences. If the virus loses the sequence encoding the antigen, the result will be an ineffective vaccine product. Therefore, it is vital to have the appropriate controls in place to ensure the stability of the intact construct vector and antigen.
Another issue is that many people have preexisting immunity to some viral vectors in development as vaccine platforms, including some of the adenovirus serotypes.102,103 This preexisting immunity can lead to a premature clearance of the vaccine before an immune response can be mounted to the antigen of interest carried by the vector. Furthermore, even if there is no large pool of preexisting immunity to a serotype, once a vaccine using that serotype is licensed and broadly administered, it may preclude that serotype from being used in subsequent vaccines.104 One possible solution to serotype immunity is the recent development of “cloaked” adeno-associated viral vectors. Cloaked AAV vectors inhibit the activation of the DNA-sensing Toll-like receptor 9 (TLR9) thereby hiding them from immune surveillance.105
Virus-like particles (VLPs)
Virus-like particles (VLPs) are similar to viral vector systems in that they present a protective antigen in the context of an intact viral particle but without any capacity to replicate. Some recombinant viral antigens can even spontaneously assemble in vivo or in vitro into VLPs or non-genetic multimeric nanoparticles without a viral genome.106,107 The assembled VLPs have a similar morphology to natural viruses.108 Therefore, VLPs can mimic the presentation of antigenic epitopes of the virus and achieve tissue-specific targeting and effective cell penetration.109 Unlike live, attenuated, or viral vector vaccines, VLPs cannot replicate, and the lack of replication adds an extra level of safety but requires higher doses of vaccine.110
VLPs have excellent immunogenicity because their size, usually 20–200 nm in diameter, is close to the optimal size recognized by immune cells.111 Their size, combined with highly ordered repeat epitopes, is ideal for cellular phagocytosis and antigen presentation to DCs. The VLPs are easily absorbed by DCs and transported to lymph nodes, stimulating the secretion of various cytokines.112 The result is the induction of a robust cellular and humoral immune response.113
Furthermore, the VLP shape and epitope structure allow it to activate B cells by cross-linking their receptors.114,115 In the absence of DCs, the B cells are sufficient to induce Tfh cell development.116 Moreover, activated B cells can promote CD4 + T cell proliferation and differentiation through homologous interactions or through TLR signals to regulate cytokine production and initiate a cellular response.116 VLPs can also be used to stimulate the immune system by engineering them to display antigenic epitopes or deliver small molecules.107
Advantages
The advantages of using VLPs as a vaccine delivery platform include efficient targeting and host cell penetration, as well as biocompatibility.117 Similar to natural viruses, receptors exposed to the surfaces of VLPs can mediate precise host cell targeting and aid in facilitating endocytosis to penetrate the host cells efficiently.118 Moreover, proteolytic mechanisms mean that VLPs can be degraded, and the degradative products are biocompatible. Therefore, VLPs can be used to envelop drugs, small molecules, and nucleic acids for targeted delivery and could be harnessed to develop gene therapy vectors. VLPs also present repetitive high-density displays of epitopes and exhibit excellent adjuvant properties capable of inducing strong immune responses, all without the potential for reversion to a pathogenic state.106,119
Challenges
There are still many technical challenges associated with manufacturing VLP-based vaccines. Among the concerns is the stability of VLPs. Although more stable than subunit vaccines, the absence of a viral genome within the particle can make it prone to disintegration during downstream processing.120 Variations in temperature, shear force, and chemical treatment can destroy the particle’s integrity and reduce the vaccine’s immunogenicity. Therefore, the design, purification, and storage of VLPs are critically important for their long-term stability.121
The expression level of viral proteins in different platforms can vary considerably, especially for secreted glycoproteins.122 The introduction of a signal peptide can improve secretion; however, extrinsic structural features can negatively impact the immunogenicity of the VLP.123 Even if the expression is optimized, purifying VLPs can be difficult. Numerous process-related contaminants, such as cell debris, host cell proteins, DNA, and lipids, must be removed. Stepwise purification methods, such as centrifugation, precipitation, ultrafiltration, and chromatography, are necessary to prepare VLPs.124
The purification strategy is highly dependent on the expression system used, requiring a de novo strategy for each vaccine candidate. For example, the baculovirus used for insect cell expression systems has similar biophysical features to some VLPs, including size and charge. Therefore, the similarity between the target product and parts of the expression system can complicate downstream processes. Baculoviruses can have adjuvant activity and cause undesirable synergistic effects if not removed or inactivated during the production process.125 Furthermore, since VLPs are non-replicating, they lack the antigen sparing attribute found in attenuated viruses and viral vectors; therefore, they require higher doses to be administered.
Subunit vaccines
Like inactivated vaccines or VLPs, subunit vaccines do not contain any live components of the pathogen. Instead, as the name suggests, they contain an antigenic subunit of the pathogen meant to induce a protective immune response. They differ from inactivated vaccines in that they include only the parts of the virus or bacteria necessary to elicit a protective immune response. Therefore, side effects are less common because subunit vaccines contain only the antigen and no other pathogen molecules. This precision comes at the cost of robust immunogenicity, however.
Subunit vaccine developers must invest significant effort to examine the various potential subunits of a pathogen to determine which combinations will produce an effective protective immune response within the correct pathway. Even when an antigen that elicits an immune response is found, there is no guarantee that immunological memory will be formed. Therefore, subunit vaccines often require the use of an adjuvant to properly engage the immune system and induce a robust immune response.
There are currently various recombinant proteins being used as vaccine antigens, such as the Epstein-Barr virus envelope glycoprotein (gp350) and nuclear antigen 1 (EBNA1), the human enterovirus 71 capsid protein VP1, the P1 polypeptide, and 3CD protease, hepatitis B virus surface antigen (HBsAg), and diphtheria and tetanus toxoids.63,126–131 Heterologous expression in bacteria (Escherichia coli) or yeast (Saccharomyces cerevisiae and Pichia pastoris) is the most common approaches for expressing these proteins because these organisms are conducive to fermentation methods that offer fast growth rates and high product yields.127 Expression of recombinant proteins in E. coli is economical; however, it lacks post-translational modifications (PTMs) that can be critical for biological activity.132 While PTMs are essential, yeast can be used due to their ability to express recombinant proteins with proper folding and modifications.133,134 Insect and mammalian cells and transgenic animals or plants can also be used to produce recombinant proteins as vaccine antigens when more authentic PTMs are required.127,135,136
Subunit vaccines often require adjuvants to enhance their immune response. The immunogenicity of Shingrix, a subunit vaccine for herpes zoster, is boosted with AS01B, a suspension composed of 3-O-desacyl-4ʹ-monophosphoryl lipid A (MPL) from Salmonella minnesota and a saponin molecule (QS-21) purified from the bark of the Quillaja saponaria tree.137,138 Another subunit vaccine, Heplisav-B for adult hepatitis B, uses a synthetic DNA sequence encoding a TLR agonist, CpG 1018, as an adjuvant to enhance the immune response.139,140
Advantages
Recombinant protein subunit vaccines are composed of a small number of well-defined components that have been produced in heterologous expression systems and are selected to induce a protective immune response against the pathogen.20,141 Compared to other platforms, subunit vaccines only contain the specified recombinant proteins or synthetic peptides.142 Therefore, subunit vaccines usually do not induce side effects at the injection site because they do not contain any of the potentially harmful components of an infectious pathogen.141 They are also unlikely to elicit eosinophilic immunopathology or antibody-mediated disease enhancement and appear safe to use in immunosuppressed patients. These features have made subunit vaccines attractive candidates for several pathogens.143
The manufacture, purification, and characterization of the antigenic subunits can be more efficient and be less expensive than alternative platforms.144 Subunit vaccines require large amounts of antigens for the final formulation. However, recombinant DNA technology makes it possible to engineer high yields for many antigens.145,146 It is also believed that subunit vaccines induce more potent cross-neutralizing antibody responses.147 Finally, subunit vaccines can be delivered through a variety of administration routes, including intramuscular, subcutaneous, mucosal, or intradermal delivery using highly concentrated formulations.148
Challenges
Subunit vaccines can contain as many as 20 separate antigens. Identifying which antigens best stimulate the immune system to develop protection against the pathogen can be challenging and time-consuming.149 Smaller subunit components also usually lack the signals that are critical for stimulating an immune response. The result is that subunit vaccine preparations can be poorly immunogenic by themselves. An adjuvant is often added along with the antigens in the vaccine carrier to augment the immune response. The purified recombinant protein can be mixed with aluminum hydroxide, aluminum phosphate, alum (potassium aluminum sulfate), or mixed aluminum salts, which are the most commonly used adjuvants. Other adjuvants, especially TLR ligands, are increasingly being used in vaccine design, however.150,151
Developing a recombinant protein subunit vaccine that is effective first requires knowing which antigens induce protective immunity in response to infection.67 Once chosen, the antigen must be manufactured, purified, and characterized while maintaining the correct tertiary structure required to induce a protective immune response.152 Another significant challenge is the low production levels of the antigen when using non-bacterial heterologous expression systems.127,135,136 The selection of a proper antigen expression system is crucial for demonstrating the feasibility of scale-up with process development at acceptable yields, purity, and stability.147 The particle size component of vaccine formulations has also been recognized as a crucial factor that affects vaccine performance. Many recent vaccine development approaches aim to mimic the size of the native pathogen in their preparation, which subunit vaccines cannot do.153
DNA vaccines
DNA vaccines are bacterial plasmids that encode a vaccine antigen driven by a viral-derived RNA polymerase II promoter, such as the CMV or SV40 promoters.154 Like subunit vaccines, DNA vaccines can be injected through intramuscular, subcutaneous, mucosal, or intradermal delivery using highly concentrated formulations.148 Unlike recombinant protein antigens, the DNA vaccine must gain entry into the cytoplasm of cells to be effective.154 When DNA vaccines are administered by localized injection with a needle and syringe, the plasmid DNA is taken up by a limited number of cells at the injection site. The injected DNA is then transcribed into mRNA and translated into the antigen of interest intracellularly.148 Locally transfected DCs traffic to the regional lymph node to initiate the immune response.155,156 Translated antigen is also shed exogenously, and some drains to regional lymph nodes and extracellular spaces. Other DCs pick up the rest of the antigen for cross-presentation. The local tissue becomes a protein factory for the presentation of antigen on MHC I or MHC II molecules for re-expansion of primed CD4+ and CD8 + T cells.79
An alternative to conventional needle delivery of DNA vaccines is a transdermal patch. The potential benefits of transdermal delivery systems for DNA vaccines have been actively investigated by research communities, as the skin layer that lies beneath the stratum corneum is supported by a densely connected network of immune-response modulating antigen-presenting cells, most significantly represented by dermal DCs in the epidermis and dermis of the skin.157 Microneedle delivery, one of the systems that have been developed for transdermal administration, are micron-sized needles that are constituted with appropriate drug formulations and directly penetrate the stratum corneum. The application of microneedles in vaccine delivery provides many clinical and logistical advantages. Most notably, the micron-scale dimensions of the microneedle shaft allow for direct and straightforward injection into the skin without requiring professional training or the use of full-size needles.158
DNA vaccines are experiencing rapid growth for various disease modalities, as demonstrated by the increasing number of clinical trials for both animal and human products.148 Nearly 100 clinical trials are ongoing in humans for a wide range of diseases, and there is an extensive pipeline of preclinical projects. Several DNA vaccine clinical trials have been recently completed or are currently ongoing. Inovio Pharmaceuticals and AstraZeneca have a vaccine (MEDI0457) targeting the human papillomavirus using the antigens HPV-16 and HPV-18 E6/E7 in clinical trials.159 Eisai Pharmaceuticals also has a microencapsulated DNA vaccine, encoding multiple HPV-16 E7-specific CTL epitopes, that was well tolerated in two different Phase I clinical trials.160,161
Advantages
DNA platforms provide greater control over vaccine design and can be manufactured quickly. The vaccine antigen can be designed from any available DNA sequences of a pathogen target protein and then synthesized. The synthetic approach allows flexibility and speed in preclinical testing with a rapid translation to clinical scale-up. More recently, the development of minicircle DNA using site-specific recombination enables manufacturers to remove bacterial elements that pose safety issues.162
Plasmid DNA is stable at room temperature, and DNA vaccine products do not require freezing during storage and transport because they are more durable than traditional vaccines.163 DNA vaccines appear to be safe and well tolerated based on limited clinical trial experience. Several DNA vaccines have already been approved for use in animals, including in fish (infectious hematopoietic necrosis virus), dogs (melanoma), swine (growth hormone-releasing hormone), and horses (West Nile virus).79
DNA vaccines are also antigen sparing since the antigen of interest is produced by endogenous cellular machinery.164 When directly targeted to immunogenic DCs with microneedle systems such as the Biojector®, an intradermal injection device that is well tolerated and allows dose-sparing, DNA vaccines can produce higher immune responses than conventional injection.158 Microinjection procedures also do not produce hazardous sharps waste like conventional needles and syringes, allowing minimally trained personnel to administer the vaccine. The result is lower costs and an expansion of vaccination campaigns into developing areas.165,166
Challenges
There are currently no licensed human vaccines that use this platform; however, many studies are underway to develop DNA vaccines for prophylactic applications. Several challenges pose significant barriers to development, however. DNA plasmids need to enter host cells where they are transcribed into RNA and translated into the corresponding protein to generate an immune response. Unfortunately, developing strategies for consistent cellular entry has been challenging. Various electroporation technologies have been investigated to facilitate the entry of DNA vaccines into cells. However, the process still requires additional steps and equipment compared to other approaches and different vaccine platforms.163
Other issues remain after the cellular uptake problem is solved. Once in the cell, the plasmids used to develop the vaccine can mutate, resulting in the incorrect protein antigen being expressed and a suboptimal immune response. DNA plasmids can also persist and integrate into tissues, creating concerns regarding tumorigenesis if insertion reduces the activity of a tumor suppressor or increases oncogenic activity.167,168 DNA integration may also result in chromosomal instability through the induction of chromosomal breaks or rearrangements. New formulations have improved nucleic acid performance in humans, but the DNA vaccines tested to date have demonstrated sub-optimal immunogenicity compared to more traditional vaccine approaches.154,169 A putative solution to low immunogenicity is to use the DNA vaccine as a primary immunization followed by a boost with a protein subunit vaccine.170
Furthermore, regulatory agencies require a description of the plasmid construction, all recombinant DNA cloning procedures, and the entire plasmid sequence in the Master Cell Bank (MCB).171 Regulators also require quantitative potency assays to evaluate the relevant biological activity. These assays must include both in vitro measures of transfection efficiency that monitor the transcription of the encoded genes, and in vivo assays of DNA vaccine immunogenicity.172 Local tissue distribution studies are also necessary for DNA vaccines utilizing novel vectors, new formulations, delivery methods or routes of administration, and other modifications expected to impact cellular uptake significantly. This means that DNA vaccines can have very high development and production costs compared with other vaccine platforms.163
RNA vaccines
Messenger RNA (mRNA) vaccines are a newer technology engineered to mimic processed, mature nucleic acid transcripts present in the cytoplasm of eukaryotic cells. The vaccine drug substance is made by in vitro transcription of a target gene from a linearized DNA template. The resulting vaccine contains the mRNA for the gene of interest and the required regulatory elements for translating the gene of interest, including untranslated regions, a 5ʹ cap, and the poly(A) tail.173 Furthermore, the mRNA vaccine can be made self-amplifying by inserting viral replication machinery into the DNA template.174 The addition of self-replication permits lower quantities of a vaccine to be administered per dose. Lowering dose requirements can be an important determinant in choosing a platform when there is a need to vaccinate many people in a short time frame, such as during a pandemic.
Once the encoded protein has been translated, it undergoes post-translational modification, the nature of which depends on the properties of the host cell. The translated protein can act in the cell in which it has been generated, or it can be secreted to act via autocrine, paracrine, or endocrine mechanisms. The protein product needs to be directed to MHC class II loading compartments to get cognate T cell help for a more robust and sustainable immune response. This can be accomplished by incorporating routing signals into the mRNA. Moreover, exogenous antigens taken up by DCs are also processed and loaded onto MHC class I molecules by a mechanism known as cross-priming. The resultant protein-derived epitopes can then be presented on the cell surface by both MHC class I and MHC class II molecules.175
Advantages
Messenger RNA is a noninfectious, non-integrating technology with no potential to cause infections or insertional mutagenesis.176 mRNA is also easily degraded, and its half-life can be regulated through modifications to the template or delivery method. Because mRNA is the minimal genetic vector, there is also no anti-vector immune response. The high yields attainable with in vitro transcription reactions allow vaccine manufacturing to be scaled-up rapidly to make many vaccine doses at low costs with smaller manufacturing footprints.173 The strong immune-stimulatory effect and intrinsic adjuvant activity of in vitro transcribed mRNA are added benefits and lead to potent antigen-specific cellular and humoral immune responses.177–180
Until recently, the production of clinical-grade mRNA vaccines posed a significant challenge due to issues with instability, delivery, and adverse events. The use of modified nucleosides combined with codon optimization has dramatically improved the stability of the mRNA.181,182 Formulation with ionizable lipid nanoparticles (LNPs) to encapsulate the anionic mRNA not only protects it from degradation by RNAse but has also demonstrated itself to be the most efficient method for in vivo delivery.183,184 Finally, purification protocols to remove double-stranded RNA (dsRNA), a typical process-related impurity, mute the innate immune response to the vaccine, reducing toxicity.185
The platform enables a large amount of antigen production from a minimal vaccine dose because the mRNA can replicate intracellularly. This self-replication within the vaccinated subjects also reduces the size of the dose required. An early study reported that immunization with as little as 10 µg of naked vaccine encoding RSV fusion (F), influenza virus hemagglutinin (HA), or pre-membrane and envelope (prM-E) proteins resulted in antibody responses and partial protection from lethal viral challenges in mice.173,174 The low dosage takes the strain off of a manufacturing process that is already easier to set up since the actual process is sequence-independent, and mRNA is relatively easy to produce as compared with recombinant protein, and live, attenuated virus vaccines. For example, Moderna’s Phase I clinical trial for its mRNA vaccine for COVID-19, mRNA-1273, used doses between 25 and 250 µg for each patient. In contrast, other vaccine platforms may require milligram amounts of vaccine antigen per dose.
The manufacturing process for mRNA vaccines can also be standardized to produce many encoded protein immunogens, making it the preferred platform for rapid response during a pandemic. All the ingredients to produce mRNA vaccines can be obtained from commercial suppliers as either synthesized chemicals or as bacterially expressed, animal-free reagents to circumvent safety issues associated with cell-culture use. This allows developers to leverage contract manufacturers’ existing expertise and resources to produce millions of vaccine doses in very short time frames with minimal manufacturing footprint.186
Challenges
Before BioNTech’s and Moderna’s vaccines, there were no mRNA vaccines licensed for use in humans. Even these vaccines are only approved under emergency use authorizations, and regulatory agencies, including the U.S. Food and Drug Administration (FDA) or the European Medicines Agency (EMA), have offered little official guidance for this platform. This a barrier for manufacturers because the number of precedents is limited, and the diversity of mRNA-based applications is broad. Therefore, a company cannot predict how regulators will review vaccines based on in vitro transcribed (IVT) mRNA.182 Most of the clinical trials using IVT mRNA have been initiated by European teams and have been performed in Europe. The lack of harmonization across multiple global regions is likely to be a barrier for manufacturers developing vaccines globally.
In addition to regulatory uncertainty, many manufacturing challenges must be tamed. For example, enzymatically synthesized mRNA preparations can contain double-stranded RNA (dsRNA) contaminants, a potent PAMP sensed by receptors in multiple cellular compartments.173 The amount of dsRNA contaminant is a significant determinant of the deleterious immunogenic profile of mRNA, but it can be removed by using standard chromatographic methods.185
Vaccines produced on this platform may not be useful in all populations. Some mRNA vaccines can induce potent type I INF reactions, and it is essential to identify patients at an increased risk of autoimmune responses before vaccination. Thus, mRNA vaccines may require a companion diagnostic assay that provides information necessary for this biological product’s safe and effective use. The requirement for a companion diagnostic tool brings many of the challenges associated with precision medicine tests.187,188
Other concerns include the proper packaging of mRNA into LNP since extracellular RNA can induce thrombosis.189,190 Although more than 95% of LNPs are endocytosed by cells, only a small fraction escapes the endosomes to reach the cytosol.191 mRNA is also inherently unstable, usually requiring storage temperatures of at least −20°C and possibly as low as −70°C. This requirement can add significant challenges to the cold chain, even for highly developed countries because few points of care have ready access to ultralow temperature freezers.
Support for vaccine development
The importance of vaccine development and the necessity for strong cross-sector partnerships have been recognized at the highest government levels. In the U.S., the federal government invested heavily over the last decade in four sprawling facilities to rapidly produce vaccines for infectious disease outbreaks.192 However, the COVID-19 pandemic has demonstrated that these facilities cannot manufacture large-scale batches of a vaccine. It is now clear that real solutions to public health threats require a multi-stakeholder approach.
Vaccines are complex products, and the development process requires perspectives, resources, and skills that are unique and complementary.1 So, even though an innovative vaccine platform may begin in an academic institution, it requires industry expertise to develop and manufacture a final product. The importance of the final stages of development has spurred many governmental efforts to create and expand expertise in disciplines that underlie product development and finished vaccine distribution.193,194 An example of such a government initiative is Operation Warp Speed (OWS), which was established to accelerate the development of vaccines for COVID-19. This public–private partnership brings together different agencies to oversee everything from basic research to licensure and program implementation, including the CDC, FDA, National Institutes of Health (NIH), Biomedical Advanced Research and Development Authority (BARDA), U.S. Department of Defense (DoD), U.S. Department of Agriculture, U.S. Department of Energy (DOE), and the U.S. Department of Veterans Affairs with pharmaceutical companies to coordinate existing Health and Human Services-wide efforts, including the ACTIV partnership for vaccine and therapeutic development, the Rapid Acceleration of Diagnostics (RADx) initiative for diagnostic development, and other work by BARDA.195
OWS has helped vaccine developers overcome several challenges that, so far, have resulted in the production and release of almost 64 million doses to the U.S. within 9 months.196 To accomplish this feat, OWS first worked with manufacturers to develop a list of critical supplies and then invoked the Defense Production Act on multiple occasions to expedite delivery.197 Next, OWS officials helped developers by scaling up manufacturing, including mediating disputes over intellectual property, shifting capacity to account for already in-use production facilities, and finding more fill-finish capacity.198 For example, BARDA, helped find a manufacturing partner for a vaccine developer and the Army Corps of Engineers has helped construct additional vaccine manufacturing suites while overseeing multiple agreements to expand manufacturing capacity for cell culture media and glass vials.197,198
Scaling up of manufacturing, however, created its own set of unique issues that OWS has helped resolve. New facilities require workers with technical expertise as well as managers with manufacturing experience.198 To address this issue, OWS worked with the U.S. Department of State to expedite visa approvals for engineers and other experts in drug manufacturing, and when hiring did not occur fast enough, they sent workers from the U.S. Department of Defense to fill positions.198
There are also several international efforts that have been put together to deal with the pandemic. The WHO already works with countries and international partners to improve global vaccination coverage by funding immunization campaigns and programs that ensure safe and reliable vaccine supply systems. In response to COVID-19, the WHO has implemented additional programs, including the Access to COVID-19 Tools (ACT) Accelerator.199 Launched in April 2020, the ACT Accelerator is a ground-breaking global collaboration bringing together multiple stakeholders, including the Bill & Melinda Gates Foundation, Coalition for Epidemic Preparedness Innovations (CEPI), Gavi, the Vaccine Alliance, the Global Fund, and the World Bank, to accelerate development, production, and access to COVID-19 tests, treatments, and vaccines.200 These organizations have joined forces to speed up the development and equitable distribution of vaccines to control COVID-19.201
The ACT Accelerator has four pillars: diagnostics, treatment, vaccines, and health system strengthening. The vaccines pillar, or COVAX, convened by CEPI, Gavi, and WHO, will speed up the search for an effective vaccine for all countries. In parallel, it supports the building of manufacturing infrastructure. COVAX is also buying supplies ahead of time so that two billion doses of vaccine can be fairly distributed by the end of 2021, with the aim of protecting high-risk and vulnerable people as well as frontline health-care workers.199 As such, COVAX is the only effort to ensure that people worldwide will have access to COVID-19 vaccines once they are available, regardless of their wealth.202 Available doses are expected to be allocated to all participating countries at the same rate, proportional to their total population size, once a vaccine is proven to be both safe and effective and has received regulatory approval.202
In addition to specific programs, the WHO and global pharmacopoeias provide compendial standards to support control strategies for vaccine products. An essential element of these tools are physical reference materials that play an indispensable role as calibrators of assays and comparators for potency assignment, as system suitability standards for assay performance monitoring, and to validate the quality of raw materials. There is also an active program at the WHO to develop international reference standards that support potency assessment for COVID-19 vaccines. The National Institute of Biological Standards and Control (NIBSC) is one of the WHO collaborative centers working with global laboratories on developing international standards for vaccines and is also the custodian of several standards to support vaccines’ potency and quality.203 The WHO Expert Committee on Biological Standardization (ECBS) has already established two standards to address some of the challenges associated with the safety and efficacy of COVI-19 vaccines: the First WHO International Standard for SARS-CoV-2 RNA nucleic acids-based assays and the First WHO International Standard for anti-SARS-CoV-2 antibodies.204 These reference materials will be used to standardize diagnostic assays and assays used to measure antibody responses to vaccination, as well as to support clinical outcomes of the vaccines under development.
Support for vaccine regulation
Vaccines are biological products whose regulations are codified in various national laws supplemented by national and international guidelines. These documents provide manufacturers with best practices while allowing scientific approaches to evolve so that regulators can still consider them with appropriate justification. In the U.S., national requirements are in the Public Health Service Act (42 U.S.C.), including section 351 (42 U.S.C. 262) and the Code of Federal Regulations Title 21 (21 CFR), including sections 200, 600, and 610. Additional recommendations are available in FDA Guidance documents, which are produced and revised as scientific and regulatory understanding advances (see Appendix).205 In Europe, the EMA has produced similar guidelines for vaccine manufacturers intending to market in the European Union (E.U.). The EMA expectations for a vaccine active substance and final product can be accessed via numerous guidelines on the EMA websites.206,207
Unfortunately, there is not a single international regulatory standard, and not all international regulatory bodies coordinate their responses with the U.S. and the E.U. The result is an overly complicated process at a global level, and not surprisingly, the current rollout of COVID-19 vaccines is a patchwork of regulatory decisions. For example, months after being approved in over several non-E.U. nations, an application for authorization of the Russian made Sputnik V COVID-19 vaccine had still not been received by the EMA, even though the manufacturer had believed the process to have been initiated.208 The confusion was caused by the incorrect usage of a submission portal for individual member states rather than the centralized application route for pan-E.U. approval. This global disparity in regulatory requirements and standards across countries poses significant challenges, no more so than during a pandemic where a coordinated global response is needed.
Uncoordinated regulatory responses create barriers to vaccine development. For example, companies seeking to participate in global markets must submit multiple approval applications for a single product. This process can require additional clinical trials or animal studies, which increases the cost and the time to bring the product to market. The lack of harmonization also puts a lot of the onus on regulatory agencies in developing countries with limited resources and which may lack the necessary expertise to stay abreast of the rapid advances in new treatments and manufacturing technologies.209 The result can be an inequitable distribution of vaccines and vaccine hesitancy if a drug’s approval is not perceived to have been legitimately vetted.
To align expectations and decrease differing requirements for global registrations, regulators and industry from multiple regions have collaborated to develop harmonized documents via the International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use (ICH) and the WHO.210 ICH’s Quality (Q) series of guidelines apply to many vaccine types, particularly those using recombinant DNA approaches to produce protein antigens; however, some of the newer platforms are not covered. Also, current good manufacturing practices (cGMPs), first implemented and required in the U.S. and E.U., are gradually being implemented for vaccine manufacturing in other countries. In addition, the WHO publishes its Technical Report Series to provide overarching guidance to vaccine manufacturers and more specific guidance for particular vaccine products. These documents serve as a roadmap for global manufacturers seeking approval and market distribution via WHO’s vaccine prequalification (PQ) program.
The COVID-19 pandemic has also spurred additional efforts. The WHO has been working with researchers from hundreds of institutions to develop and test vaccines, standardize assays, standardize regulatory approaches on innovative trial designs, and prioritize vaccine candidates’ criteria.211 The pandemic has spurred enormous activity and has fostered unparalleled global cooperation, bringing together the development and manufacturing activities of thousands of facilities in more than 150 countries.212 This effort will continue to require harmonization of pharmaceutical regulation with visible global coordination of responses among all regulatory authorities. Ultimately, each country would need to continue to make its own decision, but the harmonization of regulations between countries would bring transparency and alignment across all nations.
The United States Pharmacopoeia (USP)
As a global pharmacopoeia, USP is committed to guiding manufacturers of vaccines with technical assistance in applying existing standards in their development programs and collaborating with stakeholders on the development of new standards to support quality assessment of vaccines developed using the platforms described herein. The USP-National Formulary (USP-NF) book of standards contains a comprehensive set of documentary standards that describe best practices, analytical procedures applicable to the manufacturing and quality testing of vaccines.213 These standards are vetted by independent scientific experts through a public and transparent process and are complementary to those available from global pharmacopoeias and the WHO. Additionally, the USP book of standards contains validated test procedures that apply to adjuvants, excipients, and other components used to manufacture and formulate vaccines. Such test methods help to save time and resources, allowing manufacturers to devote more effort to controlling areas not covered in the compendium. Pharmacopoeial standards such as USP’s are recognized globally, and they often align with guidelines from the ICH helping to enable developers to achieve global regulatory predictability.
In the areas of RNA-based standards, USP is currently exploring the development of analytical methods and associated reference standards for mRNA size, content, and purity. For example, reference standards for dsRNA combined with documentary standards that provide guidance on methods and analysis may be useful to manufacturers in developing methods for ensuring the clearance of dsRNA contaminants. There are also existing standards that support general requirements for quality, e.g., sterility assurance and endotoxins testing, and standards that support qualification of some of the raw materials used in manufacturing. For instance, USP General Chapter <85> Bacterial Endotoxins Test is used to help ensure the quality of drugs, raw materials, excipients, water for injection, pharmaceutical ingredients, and biologics, including vaccines.
Other USP standards are applicable to nucleic acid-based, subunit protein-based, and other classes of vaccines, including some of the platforms being used for COVID-19 vaccines (Table 2). Regardless of the platform used, the potency of the vaccine is a critical quality attribute that must be measured and comply with regulator-approved thresholds for activity before licensure. USP also provides a comprehensive set of best practices and guidance to help manufacturers develop and implement the biological assays or bioassays used to perform potency testing (Table 2).
Table 2.
USP-NF general chapters for best practices
| To control the quantity and size of residual host cell DNA and host cell proteins |
| <1130> Nucleic Acid-Based Techniques – Approaches for Detecting Trace Nucleic Acids |
| <1132> Residual Host Cell Protein Measurement in Biopharmaceuticals |
| For different classes of vaccines |
| <1234> Vaccines for Human Use – Polysaccharide and Glycoconjugate Vaccines |
| <1235> Vaccines for Human Use – General Considerations |
| <1238> Vaccines for Human Use – Bacterial Vaccines |
| <1239> Vaccines for Human Use – Viral Vaccines |
| For biological assays |
| <1032> Design and Development of Biological Assays |
| <1033> Biological Assay Validation |
| <1034> Analysis of Biological Assays |
Conclusion
The public health crisis and economic disruption caused by the COVID-19 pandemic have brought vaccines into sharp focus. The consensus is that a return to some kind of “normal” can only occur once effective vaccines are widely available.214,215 Unfortunately, vaccine development is fraught with many challenges that limit our ability to do more than make educated guesses as to how many vaccines we will eventually have and when their supply will be sufficient to vaccinate the majority of the population.216 One of the biggest hurdles for companies is deciding which vaccine platform to pursue or to pivot an existing platform to target SARS-CoV-2. There is no precedent for what will work against a novel coronavirus, so nearly every vaccine platform is being explored as COVID-19 vaccines. Some strategies, like inactivated-viruses, attenuated viruses, and subunit vaccines, are strategies with long histories of success against other infections. Newer strategies like viral vectors and nucleic acid vaccines have little to no track record but offer some distinct advantages over more tried-and-true systems.
The rapid development timeline for a COVID-19 vaccine raises some important questions around equal access. On average, the typical development of a vaccine takes almost a decade. A lot of that time is spent running large clinical trials that consider how a vaccine performs in diverse populations. The 12- to 18-month timeline discussed for a COVID-19 vaccine comes at the cost of demonstrating safety and effectiveness in every demographic category, regardless of age, race, ethnicity, or gender. The data needed to ensure a vaccine meets everyone’s needs, irrespective of their demographic, is challenging to obtain when starting development from scratch, such as with SARS-CoV-2. What makes this situation even more worrisome is that COVID-19 impacts some of the most vulnerable populations, i.e., those who may be at the most significant risk from dangerous vaccine side effects.217–220 Even though companies can rely on a deep well of knowledge from other vaccine development experiences, including the seasonal influenza vaccine, there will undoubtedly be some gaps in the understanding that precludes equal access to protection from COVID-19.
Serendipitously, the industry’s multiple platform approach may help to curb some of the inequity. A vaccine based on a particular platform may work better for certain groups because of its safety profile, delivery method, stability during transport, or it just may be faster to produce and require smaller manufacturing footprints. The latter point is especially critical, given that the demand for approved COVID-19 vaccines is very high. Further complicating the process are the recent reports of SARS-CoV-2 variants that may not be as well recognized by the current crop of COVID-19 vaccines, possibly requiring development of modified follow-up vaccines.221 Fortunately, some of the vaccine platforms already being used are agile enough to allow for rapid redevelopment of better vaccines.
Regardless of the specific virus or variant, companies will still need to consider how to ramp up their manufacturing to an unprecedented speed while controlling cost, safety, and immunogenicity. They will also need to commit to robust post-marketing pharmacovigilance to identify rare side effects that may have been discovered during clinical trials for a more traditional vaccine development program. Each of these factors will play a role in determining which vaccines are used in populations throughout the world. Therefore, multiple vaccine options based on various platforms will be necessary to achieve the goal of protecting the world’s population from COVID-19. Increased transparency in the supply chain and raw materials used in manufacturing and clinical studies will enhance trust in the vaccines produced using the different platforms and allow them to deliver on their promise. As a global community, it is important to leverage the lessons learned from the COVID-19 pandemic, create new approaches to partnerships, and set the appropriate framework for developing treatments and vaccines to tackle future pandemics.
Appendix. Selected Regulatory Documents
21 CFR 201.
21 CFR 299.
21 CFR 600.
21 CFR 610.
Section 351 of the Public Health Service Act (42 U.S.C. 262).
Center for Biologics Evaluation and Research (CBER), U.S. Food and Drug Administration (FDA). Guidance for Industry – Emergency Use Authorization for Vaccines to Prevent COVID-19 (October 2020). https://www.fda.gov/media/142749/download
Center for Biologics Evaluation and Research (CBER), U.S. Food and Drug Administration (FDA). Guidance for Industry – Development and Licensure of Vaccines to Prevent COVID-19 (June 2020). https://www.fda.gov/media/139638/download
Center for Biologics Evaluation and Research (CBER), U.S. Food and Drug Administration (FDA). Guidance for Industry – Considerations for Plasmid DNA Vaccines for Infectious Disease Indications (November 2007). https://www.fda.gov/media/73667/download
Center for Biologics Evaluation and Research (CBER), U.S. Food and Drug Administration (FDA). Guidance for Industry – General Principles for the Development of Vaccines to Protect Against Global Infectious Diseases (December 2011). https://www.fda.gov/media/82306/download
Center for Biologics Evaluation and Research (CBER), U.S. Food and Drug Administration (FDA). Guidance for Industry – Content and Format of Chemistry, Manufacturing and Controls Information and Establishment Description Information for a Vaccine or Related Product (January 1999). https://www.fda.gov/media/73614/download
Center for Biologics Evaluation and Research (CBER), U.S. Food and Drug Administration (FDA). Guidance on Alternatives to Lot Release for Licensed Biological Products. Federal Register 1993;58(137): 38771–38773. http://www.fda.gov
Center for Biologics Evaluation and Research (CBER), U.S. Food and Drug Administration (FDA). Guidance for Industry – Characterization and Qualification of Cell Substrates and Other Biological Starting Materials Used in the Production of Viral Vaccines for the Prevention and Treatment of Infectious Diseases (September 2006). http://www.fda.gov
International Conference on Harmonization (ICH). Q2(R1). Validation of Analytical Procedures: Text and Methodology (November 2005). http://www.ich.org
International Conference on Harmonization (ICH). Q5A(R1). Viral Safety Evaluation of Biotechnology Products Derived from Cell Lines of Human or Animal Origin (September 1999). http://www.ich.org
International Conference on Harmonization (ICH). Q5B. Analysis of the Expression Construct in Cells Used for Production of r-DNA Derived Protein Products (November 1995). http://www.ich.org
International Conference on Harmonization (ICH). Q5C. Stability Testing of Biotechnological/Biological Products (November 1995). http://www.ich.org
International Conference on Harmonization (ICH). Q5D. Derivation and Characterization of Cell Substrates Used for Production of Biotechnological/Biological Products (July 1997). http://www.ich.org
International Conference on Harmonization (ICH). Q5E. Comparability of Biotechnological/Biological Products Subject to Changes in Their Manufacturing Process (November 2004). http://www.ich.org
International Conference on Harmonization (ICH). Q6B. Specifications: Test Procedures and Acceptance Criteria for Biotechnological/Biological Products (March 1999). http://www.ich.org
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
References
- 1.Folkers GK, Fauci AS.. The role of US government agencies in vaccine research and development. Nat Med. 1998May;4(5 Suppl):491–94. doi: 10.1038/nm0598supp-491. [DOI] [PubMed] [Google Scholar]
- 2.Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and its eradication. Geneva (CH): World Health Organization; 1988. [Google Scholar]
- 3.Morales M, Tangermann RH, Wassilak SG. Progress toward polio eradication - worldwide, 2015-2016. MMWR Morb Mortal Wkly Rep. 2016May13;65(18):470–73. doi: 10.15585/mmwr.mm6518a4. [DOI] [PubMed] [Google Scholar]
- 4.Orenstein WA, Ahmed R. Simply put: vaccination saves lives. Proc Natl Acad Sci U S A. 2017Apr18;114(16):4031–33. doi: 10.1073/pnas.1704507114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Plotkin SL, Plotkin SA. A short history of vaccination. In: Plotkin SA, Orenstein WA, Offit PA, Edwards KM, editors. Plotkin’s Vaccines. 7thed. Philadelphia (PA): Elsevier; 2018. p. 1–15. [Google Scholar]
- 6.Andre FE, Booy R, Bock HL, Clemens J, Datta SK, John TJ, Lee BW, Lolekha S, Peltola H, Ruff TA, et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Vol. 86.Bulletin of the World Health Organization; Geneva (CH): World Health Organization; 2008 February. p. 81–160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Plotkin SA, Orenstein WA, Plotkin SA, Orenstein WA, Offit PA, Edwards KM. Plotkin’s vaccines. 7th ed. Philadelphia (PA): Elsevier; 2018. [Google Scholar]
- 8.Salk JE, Krech U, Youngner JS, Bennett BL, Lewis LJ, Bazeley PL. Formaldehyde treatment and safety testing of experimental poliomyelitis vaccines. Am J Public Health Nations Health. 1954May;44(5):563–70. doi: 10.2105/ajph.44.5.563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Miller MA, Pisani E. The cost of unsafe injections. Bull World Health Organ. 1999;77:808–11. [PMC free article] [PubMed] [Google Scholar]
- 10.McMurtry CM, Noel M, Taddio A, Antony, M.M., Asmundson, G.J., Riddell, R.P., Chambers, C.T. and Shah, V. Interventions for individuals with high levels of needle fear: systematic review of randomized controlled trials and quasi-randomized controlled trials. Clin J Pain. 2015Oct;31(10 Suppl):S109–23. doi: 10.1097/ajp.0000000000000273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Betz K. Target survey shows adult Americans may avoid the flu shot due to fear of needles; 2012. [accessed 2012 Aug 14]. https://corporate.target.com/press/releases/2012/08/target-survey-shows-adult-americans-237507
- 12.Deacon B, Abramowitz J. Fear of needles and vasovagal reactions among phlebotomy patients. J Anxiety Disord. 2006;20(7):946–60. doi: 10.1016/j.janxdis.2006.01.004. [DOI] [PubMed] [Google Scholar]
- 13.Cox AC, Fallowfield LJ. After going through chemotherapy I can’t see another needle. Eur J Oncol Nurs. 2007Feb;11(1):43–48. doi: 10.1016/j.ejon.2006.04.035. [DOI] [PubMed] [Google Scholar]
- 14.Taddio A, Ipp M, Thivakaran S, Jamal A, Parikh C, Smart S, Sovran J, Stephens D, Katz J. Survey of the prevalence of immunization non-compliance due to needle fears in children and adults. Vaccine. 2012Jul6;30(32):4807–12. doi: 10.1016/j.vaccine.2012.05.011. [DOI] [PubMed] [Google Scholar]
- 15.Report of the SAGE working group on vaccine hesitancy; 2014. p. 1–64. [accessed 2014 Nov 12]. https://www.who.int/immunization/sage/meetings/2014/october/SAGE_working_group_revised_report_vaccine_hesitancy.pdf
- 16.Ravi AD, Sadhna D, Nagpaal D, Chawla L. Needle free injection technology: a complete insight. Int J Pharm Investig. 2015Oct-Dec;5(4):192–99. doi: 10.4103/2230-973x.167662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Adhikari BB, Goodson JL, Chu SY, Rota PA, Meltzer MI. Assessing the potential cost-effectiveness of microneedle patches in childhood measles vaccination programs: the case for further research and development. Drugs R D. 2016;16(4):327–38. doi: 10.1007/s40268-016-0144-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kasturi SP, Skountzou I, Albrecht RA, Koutsonanos D, Hua T, Nakaya HI, Ravindran R, Stewart S, Alam M, Kwissa M, et al. Programming the magnitude and persistence of antibody responses with innate immunity. Nature. 2011Feb24;470(7335):543–47. doi: 10.1038/nature09737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Einstein MH, Takacs P, Chatterjee A, Sperling RS, Chakhtoura N, Blatter MM, Lalezari J, David M-P, Lin L, Struyf F, et al. Comparison of long-term immunogenicity and safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine and HPV-6/11/16/18 vaccine in healthy women aged 18-45 years: end-of-study analysis of a phase III randomized trial. Hum Vaccin Immunother. 2014;10(12):3435–45. doi: 10.4161/hv.36121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Plotkin S, Robinson JM, Cunningham G, Iqbal R, Larsen S. The complexity and cost of vaccine manufacturing - an overview. Vaccine. 2017Jul24;35(33):4064–71. doi: 10.1016/j.vaccine.2017.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Siegrist C-A. Vaccine immunology. In: Plotkin SA, Orenstein WA, Offit PA, Edwards KM, editors. Plotkin’s vaccines. 7thed. Philadelphia (PA): Elsevier, Inc; 2018. p. 2. [Google Scholar]
- 22.Fine PE. Non-specific “non-effects” of vaccination. Bmj. 2004Dec4;329(7478):1297–98. doi: 10.1136/bmj.329.7478.1297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stowe J, Andrews N, Taylor B, Miller E. No evidence of an increase of bacterial and viral infections following measles, mumps and rubella vaccine. Vaccine. 2009Feb25;27(9):1422–25. doi: 10.1016/j.vaccine.2008.12.038. [DOI] [PubMed] [Google Scholar]
- 24.Coffman RL, Sher A, Seder RA. Vaccine adjuvants: putting innate immunity to work. Immunity. 2010Oct29;33(4):492–503. doi: 10.1016/j.immuni.2010.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lee S, Nguyen MT. Recent advances of vaccine adjuvants for infectious diseases. Immune Netw. 2015Apr;15(2):51–57. doi: 10.4110/in.2015.15.2.51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.O’Hagan DT, Fox CB. New generation adjuvants–from empiricism to rational design. Vaccine. 2015Jun8;33(Suppl 2):B14–20. doi: 10.1016/j.vaccine.2015.01.088. [DOI] [PubMed] [Google Scholar]
- 27.Cooper NR, Nemerow GR. The role of antibody and complement in the control of viral infections. J Invest Dermatol. 1984Jul;83(1 Suppl):121s–127s. doi: 10.1111/1523-1747.ep12281847. [DOI] [PubMed] [Google Scholar]
- 28.Pierce SK, Liu W. The tipping points in the initiation of B cell signalling: how small changes make big differences. Nat Rev Immunol. 2010Nov;10(11):767–77. doi: 10.1038/nri2853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tarlinton D, Good-Jacobson K. Diversity among memory B cells: origin, consequences, and utility. Science. 2013Sep13;341(6151):1205–11. doi: 10.1126/science.1241146. [DOI] [PubMed] [Google Scholar]
- 30.Goodnow CC, Vinuesa CG, Randall KL, Mackay F, Brink R. Control systems and decision making for antibody production. Nat Immunol. 2010Aug;11(8):681–88. doi: 10.1038/ni.1900. [DOI] [PubMed] [Google Scholar]
- 31.Crotty S. A brief history of T cell help to B cells. Nat Rev Immunol. 2015Mar;15(3):185–89. doi: 10.1038/nri3803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Bentebibel S-E, Lopez S, Obermoser G, Schmitt N, Mueller C, Harrod C, Flano E, Mejias A, Albrecht RA, Blankenship D, et al. Induction of ICOS+CXCR3+CXCR5+ TH cells correlates with antibody responses to influenza vaccination. Sci Transl Med. 2013Mar13;5(176):176ra32. doi: 10.1126/scitranslmed.3005191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Spensieri F, Borgogni E, Zedda L, Bardelli M, Buricchi F, Volpini G, Fragapane E, Tavarini S, Finco O, Rappuoli R, et al. Human circulating influenza-CD4+ ICOS1+IL-21+ T cells expand after vaccination, exert helper function, and predict antibody responses. Proc Natl Acad Sci U S A. 2013Aug27;110(35):14330–35. doi: 10.1073/pnas.1311998110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Mastelic Gavillet B, Eberhardt CS, Auderset F, Seubert A, Tregoning JS, Lambert, PH, de Gregorio E, Del Giudice G, Siegrist, CA. MF59 mediates its B cell adjuvanticity by promoting T follicular helper cells and thus germinal center responses in adult and early life. J Immunol. 2015May15;194(10):4836–45. doi: 10.4049/jimmunol.1402071. [DOI] [PubMed] [Google Scholar]
- 35.Linterman MA, Vinuesa CG. T follicular helper cells during immunity and tolerance. Prog Mol Biol Transl Sci. 2010;92:207–48. doi: 10.1016/s1877-1173(10)92009-7. [DOI] [PubMed] [Google Scholar]
- 36.Crotty S. Follicular helper CD4 T cells (T FH). Annu Rev Immunol. 2011;29(1):621–63. doi: 10.1146/annurev-immunol-031210-101400. [DOI] [PubMed] [Google Scholar]
- 37.Geginat J, Paroni M, Maglie S, Alfen JS, Kastirr I, Gruarin P, De Simone M, Pagani M, Abrignani S. Plasticity of human CD4 T cell subsets. Front Immunol. 2014;5:630. doi: 10.3389/fimmu.2014.00630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Igietseme JU, Eko FO, He Q, Black CM. Antibody regulation of Tcell immunity: implications for vaccine strategies against intracellular pathogens. Expert Rev Vaccines. 2004Feb;3(1):23–34. doi: 10.1586/14760584.3.1.23. [DOI] [PubMed] [Google Scholar]
- 39.Fink FK. Can we improve vaccine efficacy by targeting T and B cell repertoire convergence? Front Immunol. 2019;10:110. doi: 10.3389/fimmu.2019.00110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Gorbalenya AE, Baker SC, Baric RS, de Groot RJ, Drosten C, Gulyaeva AA, Haagmans BL, Lauber C, Leontovich AM, Neuman BW. The species severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020Apr;5(4):536–44. doi: 10.1038/s41564-020-0695-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Rabi FA, Al Zoubi MS, Kasasbeh GA, Salameh DM, Al-Nasser AD. SARS-CoV-2 and coronavirus disease 2019: what we know so far. Pathogens. 2020Mar20;9(3):231. doi: 10.3390/pathogens9030231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Novoa RR, Calderita G, Arranz R, Fontana J, Granzow H, Risco C. Virus factories: associations of cell organelles for viral replication and morphogenesis. Biol Cell. 2005Feb;97(2):147–72. doi: 10.1042/bc20040058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Fehr AR, Perlman S. Coronaviruses: an overview of their replication and pathogenesis. In: Maier HJ, Bickerton E, Britton P, editors. Coronaviruses: methods and protocols. New York (NY): Springer; 2015. p. 1–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mullard A. COVID-19 vaccine development pipeline gears up. The Lancet. 2020;395(10239):1751–52. doi: 10.1016/s0140-6736(20)31252-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Rauch S, Jasny E, Schmidt KE, Petsch B. New vaccine technologies to combat outbreak situations. Front Immunol. 2018;9:1963. doi: 10.3389/fimmu.2018.01963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Garde D. STAT: COVID-19 drugs & vaccines tracker. STAT. [accessed 2020 Sept 29]. https://www.statnews.com/feature/coronavirus/drugs-vaccines-tracker/?utm_campaign=cv_landing#vaccines
- 47.Vaccines . Milken institute; 2020. [accessed 2020 Sept 29]. https://covid-19tracker.milkeninstitute.org/#vaccines_intro
- 48.Barrett PN, Terpening SJ, Snow D, Cobb RR, Kistner O. Vero cell technology for rapid development of inactivated whole virus vaccines for emerging viral diseases. Expert Rev Vaccines. 2017Sep;16(9):883–94. doi: 10.1080/14760584.2017.1357471. [DOI] [PubMed] [Google Scholar]
- 49.Madhusudana SN, Shamsundar R, Seetharaman S. In vitro inactivation of the rabies virus by ascorbic acid. Int J Infect Dis. 2004Jan;8(1):21–25. doi: 10.1016/j.ijid.2003.09.002. [DOI] [PubMed] [Google Scholar]
- 50.Amanna IJ, Raué HP, Slifka MK. Development of a new hydrogen peroxide–based vaccine platform. Nat Med 2012Jun;18(6):974–79. doi: 10.1038/nm.2763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Martin SS, Bakken RR, Lind CM, Garcia P, Jenkins E, Glass PJ, Parker MD, Hart MK, Fine DL. Comparison of the immunological responses and efficacy of gamma-irradiated V3526 vaccine formulations against subcutaneous and aerosol challenge with Venezuelan equine encephalitis virus subtype IAB. Vaccine. 2010Jan22;28(4):1031–40. doi: 10.1016/j.vaccine.2009.10.126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Budowsky EI, Bresler SE, Friedman EA, Zheleznova NV. Principles of selective inactivation of viral genome. I. UV-induced inactivation of influenza virus. Arch Virol. 1981;68(3–4):239–47. doi: 10.1007/bf01314577. [DOI] [PubMed] [Google Scholar]
- 53.Nims RW, Plavsic M. Polyomavirus inactivation - a review. Biologicals. 2013Mar;41(2):63–70. doi: 10.1016/j.biologicals.2012.09.011. [DOI] [PubMed] [Google Scholar]
- 54.Stauffer F, El-Bacha T, Da Poian AT. Advances in the development of inactivated virus vaccines. Recent Pat Antiinfect Drug Discov. 2006Nov;1(3):291–96. doi: 10.2174/157489106778777673. [DOI] [PubMed] [Google Scholar]
- 55.Sabbaghi A, Miri SM, Keshavarz M, Zargar M, Ghaemi A. Inactivation methods for whole influenza vaccine production. Rev Med Virol. 2019Nov;29(6):e2074. doi: 10.1002/rmv.2074. [DOI] [PubMed] [Google Scholar]
- 56.Budimir N, Huckriede A, Meijerhof T, Boon L, Gostick E, Price DA, Wilschut J, De Haan A. Induction of heterosubtypic cross-protection against influenza by a whole inactivated virus vaccine: the role of viral membrane fusion activity. PLoS ONE. 2012;7(1):e30898. doi: 10.1371/journal.pone.0030898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Geeraedts F, Goutagny N, Hornung V, Severa M, De Haan A, Pool J, Wilschut J, Fitzgerald KA, Huckriede A. Superior immunogenicity of inactivated whole virus H5N1 influenza vaccine is primarily controlled by toll-like receptor signalling. PLoS Pathog. 2008Aug29;4(8):e1000138. doi: 10.1371/journal.ppat.1000138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Sanders B, Koldijk M, Schuitemaker H. Inactivated Viral Vaccines. In: Nunnally BK, Turula VE, Sitrin RD, editors. Vaccine analysis: strategies, principles, and control. Berlin Heidelberg: Springer; 2015. p. 45–80. [Google Scholar]
- 59.Sanders B, Koldijk M, Schuitemaker H. Inactivated viral vaccines. Berlin Heidelberg: Springer; 2015. p. 45–80. [Google Scholar]
- 60.Barrett PN, Mundt W, Kistner O, Howard MK. Vero cell platform in vaccine production: moving towards cell culture-based viral vaccines. Expert Rev Vacc. 2009May;8(5):607–18. doi: 10.1586/erv.09.19. [DOI] [PubMed] [Google Scholar]
- 61.FDA . FDA updated communication on use of jet injectors with inactivated influenza vaccines. U.S. food and drug administration. [accessed 2020 Sept 4]. https://www.fda.gov/vaccines-blood-biologics/vaccines/fda-updated-communication-use-jet-injectors-inactivated-influenza-vaccines
- 62.Bragazzi NL, Orsi A, Ansaldi F, Gasparini R, Icardi G. Fluzone® intra-dermal (Intanza®/Istivac® Intra-dermal): an updated overview. Hum Vaccin Immunother. 2016;12(10):2616–27. doi: 10.1080/21645515.2016.1187343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.CDC . Understanding how vaccines work; 2018.
- 64.Bull JJ, Nuismer SL, Antia R, Müller V. Recombinant vector vaccine evolution. PLoS Comput Biol. 2019Jul;15(7):e1006857. doi: 10.1371/journal.pcbi.1006857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Iwasaki A, Medzhitov R. Regulation of adaptive immunity by the innate immune system. Science. 2010Jan15;327(5963):291–95. doi: 10.1126/science.1183021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Kawai T, Akira S. The role of pattern-recognition receptors in innate immunity: update on toll-like receptors. Nat Immunol. 2010May;11(5):373–84. doi: 10.1038/ni.1863. [DOI] [PubMed] [Google Scholar]
- 67.Pulendran B, Ahmed R. Immunological mechanisms of vaccination. Nat Immunol. 2011Jun;12(6):509–17. doi: 10.1038/ni.2039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Tsuji S, Matsumoto M, Takeuchi O, Akira S, Azuma I, Hayashi A, Toyoshima K, Seya T. Maturation of human dendritic cells by cell wall skeleton of Mycobacterium bovis bacillus Calmette-Guerin: involvement of toll-like receptors. Infect Immun. 2000Dec;68(12):6883–90. doi: 10.1128/iai.68.12.6883-6890.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Querec T, Bennouna S, Alkan S, Laouar Y, Gorden K, Flavell R, Akira S, Ahmed R, Pulendran B. Yellow fever vaccine YF-17D activates multiple dendritic cell subsets via TLR2, 7, 8, and 9 to stimulate polyvalent immunity. J Exp Med. 2006Feb20;203(2):413–24. doi: 10.1084/jem.20051720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Napolitani G, Rinaldi A, Bertoni F, Sallusto F, Lanzavecchia A. Selected toll-like receptor agonist combinations synergistically trigger a T helper type 1-polarizing program in dendritic cells. Nat Immunol. 2005Aug;6(8):769–76. doi: 10.1038/ni1223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Minor TE, Dick EC, Dick CR, Inhorn SL. Attenuated influenza A vaccine (Alice) in an adult population: vaccine-related illness, serum and nasal antibody production, and intrafamily transmission. J Clin Microbiol. 1975Nov;2(5):403–09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Hall CB, Douglas G Jr., Fralonardo SA. Live attenuated influenza virus vaccine trial in children. Pediatrics. 1975Dec;56(6):991–98. [PubMed] [Google Scholar]
- 73.Koyama S, Aoshi T, Tanimoto T, Kumagai Y, Kobiyama K, Tougan T, Sakurai K, Coban C, Horii T, Akira S, Ishii, KJ. Plasmacytoid dendritic cells delineate immunogenicity of influenza vaccine subtypes. Sci Transl Med. 2010Mar31;2(25):25ra24. doi: 10.1126/scitranslmed.3000759. [DOI] [PubMed] [Google Scholar]
- 74.Gouglas D, Christodoulou M, Plotkin SA, Hatchett R. CEPI: driving progress toward epidemic preparedness and response. Epidemiol Rev. 2019Jan31;41(1):28–33. doi: 10.1093/epirev/mxz012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Plotkin S. History of vaccination. Proc Natl Acad Sci U S A. 2014Aug26;111(34):12283–87. doi: 10.1073/pnas.1400472111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Fuge O, Vasdev N, Allchorne P, Green JS. Immunotherapy for bladder cancer. Res Rep Urol. 2015;7:65–79. doi: 10.2147/RRU.S63447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Mak TW, Saunders ME, Jett BD. Primer to the immune response (Second Edition). Academic Cell; 2014. p. vii–viii. [Google Scholar]
- 78.Mak TW, Saunders ME. 23 - vaccines and clinical immunization. In: Mak TW, Saunders ME, editors. The immune response. Burlington (MA): Academic Press; 2006. p. 695–749. [Google Scholar]
- 79.Kutzler MA, Weiner DB. DNA vaccines: ready for prime time? Nat Rev Genet. 2008Oct;9(10):776–88. doi: 10.1038/nrg2432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Garcea RL, Imperiale MJ. Simian virus 40 infection of humans. J Virol. 2003May;77(9):5039–45. doi: 10.1128/jvi.77.9.5039-5045.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Thomas RE, Lorenzetti DL, Spragins W. Mortality and morbidity among military personnel and civilians during the 1930s and World War II from transmission of hepatitis during yellow fever vaccination: systematic review. Am J Public Health. 2013Mar;103(3):e16–29. doi: 10.2105/ajph.2012.301158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Marr JS, Cathey JT. The yellow fever vaccine misadventure of 1942. J Public Health Manage Pract. 2017;23(6):6. doi: 10.1097/PHH.0000000000000565. [DOI] [PubMed] [Google Scholar]
- 83.Kallel H, Kamen AA. Large-scale adenovirus and poxvirus-vectored vaccine manufacturing to enable clinical trials. Biotechnol J. 2015May;10(5):741–47. doi: 10.1002/biot.201400390. [DOI] [PubMed] [Google Scholar]
- 84.Liu MA. Immunologic basis of vaccine vectors. Immunity. 2010Oct29;33(4):504–15. doi: 10.1016/j.immuni.2010.10.004. [DOI] [PubMed] [Google Scholar]
- 85.Condit RC, Williamson A-L, Sheets R, Seligman SJ, Monath TP, Excler J-L, Gurwith M, Bok K, Robertson JS, Kim D, et al. Unique safety issues associated with virus-vectored vaccines: potential for and theoretical consequences of recombination with wild type virus strains. Vaccine. 2016Dec12;34(51):6610–16. doi: 10.1016/j.vaccine.2016.04.060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Kochhar S, Excler J-L, Bok K, Gurwith M, McNeil MM, Seligman SJ, Khuri-Bulos N, Klug B, Laderoute M, Robertson JS, et al. Defining the interval for monitoring potential adverse events following immunization (AEFIs) after receipt of live viral vectored vaccines. Vaccine. 2019Sep10;37(38):5796–802. doi: 10.1016/j.vaccine.2018.08.085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Xiang ZQ, Greenberg L, Ertl HC, Rupprecht CE. Protection of non-human primates against rabies with an adenovirus recombinant vaccine. Virology. 2014Feb;450-451:243–49. doi: 10.1016/j.virol.2013.12.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Shen CF, Lanthier S, Jacob D, Montes J, Beath A, Beresford A, Kamen A. Process optimization and scale-up for production of rabies vaccine live adenovirus vector (AdRG1.3). Vaccine. 2012Jan5;30(2):300–06. doi: 10.1016/j.vaccine.2011.10.095. [DOI] [PubMed] [Google Scholar]
- 89.Ondondo BO. The influence of delivery vectors on HIV vaccine efficacy. Front Microbiol. 2014;5:439. doi: 10.3389/fmicb.2014.00439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Schuldt NJ, Amalfitano A. Malaria vaccines: focus on adenovirus based vectors. Vaccine. 2012Jul27;30(35):5191–98. doi: 10.1016/j.vaccine.2012.05.048. [DOI] [PubMed] [Google Scholar]
- 91.Swadling L, Capone S, Antrobus RD, Brown A, Richardson R, Newell EW, Halliday J, Kelly C, Bowen D, Fergusson J, et al. A human vaccine strategy based on chimpanzee adenoviral and MVA vectors that primes, boosts, and sustains functional HCV-specific T cell memory. Sci Transl Med. 2014Nov5;6(261):261ra153. doi: 10.1126/scitranslmed.3009185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Tripp RA, Tompkins SM. Virus-vectored influenza virus vaccines. Viruses. 2014Aug7;6(8):3055–79. doi: 10.3390/v6083055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Zhang W, Fu J, Ehrhardt A. Novel vector construction based on alternative adenovirus types via homologous recombination. Hum Gene Ther Methods. 2018Jun;29(3):124–34. doi: 10.1089/hgtb.2018.044. [DOI] [PubMed] [Google Scholar]
- 94.Ng P, Graham FL. Construction of first-generation adenoviral vectors. Meth Mol Med. 2002;69:389–414. doi: 10.1385/1-59259-141-8:389. [DOI] [PubMed] [Google Scholar]
- 95.Kovesdi I, Hedley SJ. Adenoviral producer cells. Viruses. 2010Aug;2(8):1681–703. doi: 10.3390/v2081681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Murakami P, Pungor E, Files J, Do L, Van Rijnsoever R, Vogels R, Bout A, McCaman M. A single short stretch of homology between adenoviral vector and packaging cell line can give rise to cytopathic effect-inducing, helper-dependent E1-positive particles. Hum Gene Ther. 2002May20;13(8):909–20. doi: 10.1089/10430340252939023. [DOI] [PubMed] [Google Scholar]
- 97.Afkhami S, Yao Y, Xing Z. Methods and clinical development of adenovirus-vectored vaccines against mucosal pathogens. Mol Ther Methods Clin Dev. 2016;3:16030. doi: 10.1038/mtm.2016.30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Vemula SV, Mittal SK. Production of adenovirus vectors and their use as a delivery system for influenza vaccines. Expert Opin Biol Ther. 2010Oct;10(10):1469–87. doi: 10.1517/14712598.2010.519332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Morenweiser R. Downstream processing of viral vectors and vaccines. Gene Ther. 2005Oct;12(Suppl 1):S103–10. doi: 10.1038/sj.gt.3302624. [DOI] [PubMed] [Google Scholar]
- 100.Nabel GJ. Designing tomorrow’s vaccines. N Engl J Med. 2013Feb7;368(6):551–60. doi: 10.1056/NEJMra1204186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Rollier CS, Reyes-Sandoval A, Cottingham MG, Ewer K, Hill AV. Viral vectors as vaccine platforms: deployment in sight. Curr Opin Immunol. 2011Jun;23(3):377–82. doi: 10.1016/j.coi.2011.03.006. [DOI] [PubMed] [Google Scholar]
- 102.Fausther-Bovendo H, Kobinger GP. Pre-existing immunity against Ad vectors: humoral, cellular, and innate response, what’s important? Hum Vaccin Immunother. 2014;10(10):2875–84. doi: 10.4161/hv.29594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Mennechet FJD, Paris O, Ouoba AR, Salazar Arenas S, Sirima SB, Takoudjou Dzomo GR, Diarra A, Traore IT, Kania D, Eichholz K, et al. A review of 65 years of human adenovirus seroprevalence. Expert Rev Vacc. 2019Jun;18(6):597–613. doi: 10.1080/14760584.2019.1588113. [DOI] [PubMed] [Google Scholar]
- 104.Seregin SS, Amalfitano A. Overcoming pre-existing adenovirus immunity by genetic engineering of adenovirus-based vectors. Expert Opin Biol Ther. 2009Dec;9(12):1521–31. doi: 10.1517/14712590903307388. [DOI] [PubMed] [Google Scholar]
- 105.Chan YK, Wang SK, Chu CJ, Copland DA, Letizia AJ, Costa Verdera H, Chiang JJ, Sethi M, Wang MK, Neidermyer WJ, et al. Engineering adeno-associated viral vectors to evade innate immune and inflammatory responses. Sci. Transl. Med. 2021;13(580):eabd3438. doi: 10.1126/scitranslmed.abd3438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Roldao A, Mellado MC, Castilho LR, Carrondo MJ, Alves PM. Virus-like particles in vaccine development. Expert Rev Vacc. 2010Oct;9(10):1149–76. doi: 10.1586/erv.10.115. [DOI] [PubMed] [Google Scholar]
- 107.Qian C, Liu X, Xu Q, Wang Z, Chen J, Li T, Zheng Q, Yu H, Gu Y, Li S, et al. Recent progress on the versatility of virus-like particles. Vaccines (Basel). 2020Mar20;8(1): doi: 10.3390/vaccines8010139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Dong H, Guo HC, Sun SQ. Virus-like particles in picornavirus vaccine development. Appl Microbiol Biotechnol. 2014May;98(10):4321–29. doi: 10.1007/s00253-014-5639-1. [DOI] [PubMed] [Google Scholar]
- 109.Deschuyteneer M, Elouahabi A, Plainchamp D, Plisnier M, Soete D, Corazza Y, Lockman L, Giannini S, Deschamps M. Molecular and structural characterization of the L1 virus-like particles that are used as vaccine antigens in Cervarix, the AS04-adjuvanted HPV-16 and −18 cervical cancer vaccine. Hum Vaccin. 2010May;6(5):407–19. doi: 10.4161/hv.6.5.11023. [DOI] [PubMed] [Google Scholar]
- 110.Metz SW, Thomas A, White L, Stoops M, Corten M, Hannemann H, de Silva AM. Dengue virus-like particles mimic the antigenic properties of the infectious dengue virus envelope. Virol J. 2018Apr2;15(1):60. doi: 10.1186/s12985-018-0970-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Mohsen MO, Gomes AC, Vogel M, Bachmann MF. Interaction of viral capsid-derived Virus-Like Particles (VLPs) with the innate immune system. Vaccines (Basel). 2018Jul2;6(3). doi: 10.3390/vaccines6030037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Cinamon G, Zachariah MA, Lam OM, Foss FW Jr., Cyster JG. Follicular shuttling of marginal zone B cells facilitates antigen transport. Nat Immunol. 2008Jan;9(1):54–62. doi: 10.1038/ni1542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Zabel F, Kundig TM, Bachmann MF. Virus-induced humoral immunity: on how B cell responses are initiated. Curr Opin Virol. 2013Jun;3(3):357–62. doi: 10.1016/j.coviro.2013.05.004. [DOI] [PubMed] [Google Scholar]
- 114.Zabel F, Mohanan D, Bessa J, Link A, Fettelschoss A, Saudan P, Kündig TM, Bachmann MF. Viral particles drive rapid differentiation of memory B cells into secondary plasma cells producing increased levels of antibodies. J Immunol. 2014Jun15;192(12):5499–508. doi: 10.4049/jimmunol.1400065. [DOI] [PubMed] [Google Scholar]
- 115.Cimica V, Galarza JM. Adjuvant formulations for virus-like particle (VLP) based vaccines. Clin Immunol. 2017Oct;183:99–108. doi: 10.1016/j.clim.2017.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Hong S, Zhang Z, Liu H, Tian M, Zhu X, Zhang Z, Wang W, Zhou X, Zhang F, Ge Q, et al. B cells are the dominant antigen-presenting cells that activate naive CD4+ T cells upon immunization with a virus-derived nanoparticle antigen. Immunity. 2018Oct16;49(4):695–708.e4. doi: 10.1016/j.immuni.2018.08.012. [DOI] [PubMed] [Google Scholar]
- 117.Steinmetz NF. Viral nanoparticles as platforms for next-generation therapeutics and imaging devices. Nanomedicine. 2010Oct;6(5):634–41. doi: 10.1016/j.nano.2010.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Seow Y, Wood MJ. Biological gene delivery vehicles: beyond viral vectors. Mol Ther. 2009May;17(5):767–77. doi: 10.1038/mt.2009.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Chackerian B, Lenz P, Lowy DR, Schiller JT. Determinants of autoantibody induction by conjugated papillomavirus virus-like particles. J Immunol. 2002Dec1;169(11):6120–26. doi: 10.4049/jimmunol.169.11.6120. [DOI] [PubMed] [Google Scholar]
- 120.Vicente T, Roldao A, Peixoto C, Carrondo MJ, Alves PM. Large-scale production and purification of VLP-based vaccines. J Invertebr Pathol. 2011Jul;107(Suppl):S42–8. doi: 10.1016/j.jip.2011.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Dai S, Wang H, Deng F. Advances and challenges in enveloped virus-like particle (VLP)-based vaccines. J Immunol Sci. 2018;2(2):36–41. doi: 10.29245/2578-3009/2018/2.1118. [DOI] [Google Scholar]
- 122.Chang GJ, Hunt AR, Holmes DA, Springfield T, Chiueh T-S, Roehrig JT, Gubler DJ. Enhancing biosynthesis and secretion of premembrane and envelope proteins by the chimeric plasmid of dengue virus type 2 and Japanese encephalitis virus. Virology. 2003Feb1;306(1):170–80. doi: 10.1016/s0042-6822(02)00028-4. [DOI] [PubMed] [Google Scholar]
- 123.Zhang S, Liang M, Gu W, Li C, Miao F, Wang X, Jin C, Zhang L, Zhang F, Zhang Q, et al. Vaccination with dengue virus-like particles induces humoral and cellular immune responses in mice. Virol J. 2011Jun30;8(1):333. doi: 10.1186/1743-422x-8-333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Peixoto C, Sousa MF, Silva AC, Carrondo MJ, Alves PM. Downstream processing of triple layered rotavirus like particles. J Biotechnol. 2007Jan10;127(3):452–61. doi: 10.1016/j.jbiotec.2006.08.002. [DOI] [PubMed] [Google Scholar]
- 125.van Oers MM. Opportunities and challenges for the baculovirus expression system. J Invertebr Pathol. 2011Jul;107(Suppl):S3–15. doi: 10.1016/j.jip.2011.05.001. [DOI] [PubMed] [Google Scholar]
- 126.Demain AL, Vaishnav P. Production of recombinant proteins by microbes and higher organisms. Biotechnol Adv. 2009May-Jun;27(3):297–306. doi: 10.1016/j.biotechadv.2009.01.008. [DOI] [PubMed] [Google Scholar]
- 127.Tripathi NK, Shrivastava A. Recent developments in recombinant protein-based dengue vaccines. Front Immunol. 2018;9:1919. doi: 10.3389/fimmu.2018.01919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Tripathi NK, Karothia D, Shrivastava A, Banger S, Kumar JS. Enhanced production and immunological characterization of recombinant West Nile virus envelope domain III protein. N Biotechnol. 2018Nov25;46:7–13. doi: 10.1016/j.nbt.2018.05.002. [DOI] [PubMed] [Google Scholar]
- 129.Wang M, Jiang S, Wang Y. Recent advances in the production of recombinant subunit vaccines in Pichia pastoris. Bioengineered. 2016Apr;7(3):155–65. doi: 10.1080/21655979.2016.1191707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Wang M, Jiang S, Han Z, Zhao B, Wang L, Zhou Z, Wang Y. Expression and immunogenic characterization of recombinant gp350 for developing a subunit vaccine against Epstein-Barr virus. Appl Microbiol Biotechnol. 2016Feb;100(3):1221–30. doi: 10.1007/s00253-015-7027-x. [DOI] [PubMed] [Google Scholar]
- 131.Wang M, Jiang S, Wang Y. Recombinant VP1 protein expressed in Pichia pastoris induces protective immune responses against EV71 in mice. Biochem Biophys Res Commun. 2013Jan4;430(1):387–93. doi: 10.1016/j.bbrc.2012.11.035. [DOI] [PubMed] [Google Scholar]
- 132.Baeshen MN, Al-Hejin AM, Bora RS, Ahmed MMM, Ramadan HAI, Saini KS, Baeshen NA, Redwan EM. Production of biopharmaceuticals in E. coli: current scenario and future perspectives. J Microbiol Biotechnol. 2015Jul;25(7):953–62. doi: 10.4014/jmb.1412.12079. [DOI] [PubMed] [Google Scholar]
- 133.Ahmad M, Hirz M, Pichler H, Schwab H. Protein expression in Pichia pastoris: recent achievements and perspectives for heterologous protein production. Appl Microbiol Biotechnol. 2014Jun;98(12):5301–17. doi: 10.1007/s00253-014-5732-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Porro D, Gasser B, Fossati T, Maurer M, Branduardi P, Sauer M, Mattanovich D. Production of recombinant proteins and metabolites in yeasts: when are these systems better than bacterial production systems? Appl Microbiol Biotechnol. 2011Feb;89(4):939–48. doi: 10.1007/s00253-010-3019-z. [DOI] [PubMed] [Google Scholar]
- 135.Tan LC, Chua AJ, Goh LS, Pua SM, Cheong YK, Ng ML. Rapid purification of recombinant dengue and West Nile virus envelope Domain III proteins by metal affinity membrane chromatography. Protein Expr Purif. 2010Nov;74(1):129–37. doi: 10.1016/j.pep.2010.06.015. [DOI] [PubMed] [Google Scholar]
- 136.Yap YK, Smith DR. Strategies for the plant-based expression of dengue subunit vaccines. Biotechnol Appl Biochem. 2010Oct;57(2):47–53. doi: 10.1042/ba20100248. [DOI] [PubMed] [Google Scholar]
- 137.FDA . Common ingredients in U.S. licensed vaccines. Food and Drug Administration; 2020. [accessed 2020 July 27]. https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/common-ingredients-us-licensed-vaccines
- 138.Grupping K, Campora L, Douha M, Heineman TC, Klein NP, Lal H, Peterson J, Vastiau I, Oostvogels L. Immunogenicity and safety of the HZ/su adjuvanted Herpes Zoster subunit vaccine in adults previously vaccinated with a live attenuated Herpes Zoster vaccine. J Infect Dis. 2017Dec12;216(11):1343–51. doi: 10.1093/infdis/jix482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Bode C, Zhao G, Steinhagen F, Kinjo T, Klinman DM. CpG DNA as a vaccine adjuvant. Expert Rev Vaccines. 2011;10(4):499–511. doi: 10.1586/erv.10.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Cooper C, Mackie D. Hepatitis B surface antigen-1018 ISS adjuvant-containing vaccine: a review of HEPLISAV™ safety and efficacy. Expert Rev Vaccines. 2011Apr;10(4):417–27. doi: 10.1586/erv.10.162. [DOI] [PubMed] [Google Scholar]
- 141.Wang M, Jiang S, Wang Y. Recent advances in the production of recombinant subunit vaccines in Pichia pastoris. Bioengineered. 2016;7(3):155–65. doi: 10.1080/21655979.2016.1191707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Zhang N, Jiang S, Du L. Current advancements and potential strategies in the development of MERS-CoV vaccines. Expert Rev Vaccines. 2014Jun;13(6):761–74. doi: 10.1586/14760584.2014.912134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Oyston P, Robinson K. The current challenges for vaccine development. J Med Microbiol. 2012Jul;61(Pt 7):889–94. doi: 10.1099/jmm.0.039180-0. [DOI] [PubMed] [Google Scholar]
- 144.Moyle PM, Toth I. Modern subunit vaccines: development, components, and research opportunities. ChemMedChem. 2013Mar;8(3):360–76. doi: 10.1002/cmdc.201200487. [DOI] [PubMed] [Google Scholar]
- 145.Trumpfheller C, Longhi MP, Caskey M, Idoyaga J, Bozzacco L, Keler T, Schlesinger SJ, Steinman RM. Dendritic cell-targeted protein vaccines: a novel approach to induce T-cell immunity. J Intern Med. 2012Feb;271(2):183–92. doi: 10.1111/j.1365-2796.2011.02496.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Cox MM. Recombinant protein vaccines produced in insect cells. Vaccine. 2012Feb27;30(10):1759–66. doi: 10.1016/j.vaccine.2012.01.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Jiang S, Bottazzi ME, Du L, Lustigman S, Tseng CTK, Curti E, Jones K, Zhan B, Hotez PJ. Roadmap to developing a recombinant coronavirus S protein receptor-binding domain vaccine for severe acute respiratory syndrome. Expert Rev Vaccines. 2012Dec;11(12):1405–13. doi: 10.1586/erv.12.126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Gary EN, Weiner DB. DNA vaccines: prime time is now. Curr Opin Immunol. 2020Apr4;65:21–27. doi: 10.1016/j.coi.2020.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Pathak A. Global markets for vaccine technologies; 2018April.
- 150.Alexopoulou L, Holt AC, Medzhitov R, Flavell RA. Recognition of double-stranded RNA and activation of NF-kappaB by toll-like receptor 3. Nature. 2001Oct18;413(6857):732–38. doi: 10.1038/35099560. [DOI] [PubMed] [Google Scholar]
- 151.Janeway CA Jr., Medzhitov R. Innate immune recognition. Annu Rev Immunol. 2002;20(1):197–216. doi: 10.1146/annurev.immunol.20.083001.084359. [DOI] [PubMed] [Google Scholar]
- 152.Black M, Trent A, Tirrell M, Olive C. Advances in the design and delivery of peptide subunit vaccines with a focus on toll-like receptor agonists. Expert Rev Vaccines. 2010Feb;9(2):157–73. doi: 10.1586/erv.09.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Depelsenaire ACI, Kendall MAF, Young PR, Muller DA. Chapter three - introduction to vaccines and vaccination. In: Skwarczynski M, Toth I, editors. Micro and nanotechnology in vaccine development. Cambridge (MA): William Andrew Publishing; 2017. p. 47–62. [Google Scholar]
- 154.Li L, Petrovsky N. Molecular mechanisms for enhanced DNA vaccine immunogenicity. Expert Rev Vaccines. 2016;15(3):313–29. doi: 10.1586/14760584.2016.1124762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Akbari O, Panjwani N, Garcia S, Tascon R, Lowrie D, Stockinger B. DNA vaccination: transfection and activation of dendritic cells as key events for immunity. J Exp Med. 1999Jan4;189(1):169–78. doi: 10.1084/jem.189.1.169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Chattergoon MA, Robinson TM, Boyer JD, Weiner DB. Specific immune induction following DNA-based immunization through in vivo transfection and activation of macrophages/antigen-presenting cells. J Immunol. 1998Jun15;160(12):5707–18. [PubMed] [Google Scholar]
- 157.Kim YC, Park JH, Prausnitz MR. Microneedles for drug and vaccine delivery. Adv Drug Deliv Rev. 2012Nov;64(14):1547–68. doi: 10.1016/j.addr.2012.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Suh H, Shin J, Kim YC. Microneedle patches for vaccine delivery. Clin Exp Vaccine Res. 2014Jan;3(1):42–49. doi: 10.7774/cevr.2014.3.1.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.DNA Medicines Pipeline . Inovio pharmaceuticals. [accessed 2020 Aug 10]. https://www.inovio.com/dna-medicines-pipeline
- 160.Sheets EE, Urban RG, Crum CP, Hedley ML, Politch JA, Gold MA, Muderspach LI, Cole GA, Crowley-Nowick PA. Immunotherapy of human cervical high-grade cervical intraepithelial neoplasia with microparticle-delivered human papillomavirus 16 E7 plasmid DNA. Am J Obstet Gynecol. 2003Apr;188(4):916–26. doi: 10.1067/mob.2003.256. [DOI] [PubMed] [Google Scholar]
- 161.Klencke B, Matijevic M, Urban RG, Lathey JL, Hedley ML, Berry M, Thatcher J, Weinberg V, Wilson J, Darragh T, et al. Encapsulated plasmid DNA treatment for human papillomavirus 16-associated anal dysplasia: a Phase I study of ZYC101. Clin Cancer Res. 2002May;8(5): 1028–37. [PubMed] [Google Scholar]
- 162.Jechlinger W, Azimpour Tabrizi C, Lubitz W, Mayrhofer P. Minicircle DNA immobilized in bacterial ghosts: in vivo production of safe non-viral DNA delivery vehicles. J Mol Microbiol Biotechnol. 2004;8(4):222–31. doi: 10.1159/000086703. [DOI] [PubMed] [Google Scholar]
- 163.Vartak A, Sucheck SJ. Recent advances in subunit vaccine carriers. Vaccines. 2016;4(2):12. doi: 10.3390/vaccines4020012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Liu MA. DNA vaccines: an historical perspective and view to the future. Immunol Rev. 2011Jan;239(1):62–84. doi: 10.1111/j.1600-065X.2010.00980.x. [DOI] [PubMed] [Google Scholar]
- 165.Rodgers AM, Cordeiro AS, Donnelly RF. Technology update: dissolvable microneedle patches for vaccine delivery. Med Devices (Auckl). 2019;12:379–98. doi: 10.2147/MDER.S198220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Graham BS, Enama ME, Nason MC, Gordon IJ, Peel SA, Ledgerwood JE, Plummer SA, Mascola JR, Bailer RT, Roederer M, et al. DNA vaccine delivered by a needle-free injection device improves potency of priming for antibody and CD8+ T-cell responses after rAd5 boost in a randomized clinical trial. PLoS ONE. 2013;8(4):e59340–e59340. doi: 10.1371/journal.pone.0059340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167.Ledwith BJ, Manam S, Troilo PJ, Barnum AB, Pauley CJ, Griffiths II TG, Harper LB, Beare CM, Bagdon WJ, Nichols WW, et al. Plasmid DNA vaccines: investigation of integration into host cellular DNA following intramuscular injection in mice. Intervirology. 2000;43(4–6):258–72. doi: 10.1159/000053993. [DOI] [PubMed] [Google Scholar]
- 168.Vahedi F, Nazari N, Arbabi S, Peymanfar Y. Investigation of DNA integration into reproductive organs following intramuscular injection of DNA in mice. Rep Biochem Mol Biol. 2012Oct;1(1):21–24. [PMC free article] [PubMed] [Google Scholar]
- 169.Chen WH, Strych U, Hotez PJ, Bottazzi ME. The SARS-CoV-2 vaccine pipeline: an overview. Curr Trop Med Rep. 2020Mar3;1–4. doi: 10.1007/s40475-020-00201-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170.Liu F, Wang X, Zheng M, Xiong F, Liu X, Zhou L, Tan W, Chen Z. Immunization with DNA prime-subunit protein boost strategy based on influenza H9N2 virus conserved matrix protein M1 and its epitope screening. Sci Rep. 2020Mar5;10(1):4144. doi: 10.1038/s41598-020-60783-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.FDA . Points to consider in the characterization of cell lines used to produce biologicals; 1993.[accessed 2020 Dec 3]. https://www.fda.gov/media/76255/download
- 172.FDA . Considerations for Plasmid DNA Vaccines for Infectious Disease Indications. Guidance for Industry; 2007.
- 173.Pardi N, Hogan MJ, Porter FW, Weissman D. mRNA vaccines - a new era in vaccinology. Nat Rev Drug Discov. 2018Apr;17(4):261–79. doi: 10.1038/nrd.2017.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174.Fleeton MN, Chen M, Berglund P, Rhodes G, Parker SE, Murphy M, Atkins GJ, Liljestrom P. Self-replicative RNA vaccines elicit protection against influenza A virus, respiratory syncytial virus, and a tickborne encephalitis virus. J Infect Dis. 2001May1;183(9):1395–98. doi: 10.1086/319857. [DOI] [PubMed] [Google Scholar]
- 175.Bevan MJ. Cross-priming. Nat Immunol. 2006Apr;7(4):363–65. doi: 10.1038/ni0406-363. [DOI] [PubMed] [Google Scholar]
- 176.Jackson NAC, Kester KE, Casimiro D, Gurunathan S, DeRosa F. The promise of mRNA vaccines: a biotech and industrial perspective. NPJ Vaccines. 2020;5(1):11. doi: 10.1038/s41541-020-0159-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Hoerr I, Obst R, Rammensee HG, Jung G. In vivo application of RNA leads to induction of specific cytotoxic T lymphocytes and antibodies. Eur J Immunol. 2000Jan;30(1):1–7. doi:. [DOI] [PubMed] [Google Scholar]
- 178.Bourquin C, Schmidt L, Hornung V, Wurzenberger C, Anz D, Sandholzer N, Schreiber S, Voelkl A, Hartmann G, Endres S, et al. Immunostimulatory RNA oligonucleotides trigger an antigen-specific cytotoxic T-cell and IgG2a response. Blood. 2007Apr1;109(7):2953–60. doi: 10.1182/blood-2006-07-033258. [DOI] [PubMed] [Google Scholar]
- 179.Sander LE, Davis MJ, Boekschoten MV, Amsen D, Dascher CC, Ryffel B, Swanson JA, Müller M, Blander JM. Detection of prokaryotic mRNA signifies microbial viability and promotes immunity. Nature. 2011May22;474(7351):385–89. doi: 10.1038/nature10072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 180.Weissman D, Ni H, Scales D, Dude A, Capodici J, McGibney K, Abdool A, Isaacs SN, Cannon G, Karikó K, et al. HIV gag mRNA transfection of dendritic cells (DC) delivers encoded antigen to MHC class I and II molecules, causes DC maturation, and induces a potent human in vitro primary immune response. J Immunol. 2000Oct15;165(8):4710–17. doi: 10.4049/jimmunol.165.8.4710. [DOI] [PubMed] [Google Scholar]
- 181.Kariko K, Buckstein M, Ni H, Weissman D. Suppression of RNA recognition by toll-like receptors: the impact of nucleoside modification and the evolutionary origin of RNA. Immunity. 2005Aug;23(2):165–75. doi: 10.1016/j.immuni.2005.06.008. [DOI] [PubMed] [Google Scholar]
- 182.Sahin U, Kariko K, Tureci O. mRNA-based therapeutics–developing a new class of drugs. Nat Rev Drug Discov. 2014Oct;13(10):759–80. doi: 10.1038/nrd4278. [DOI] [PubMed] [Google Scholar]
- 183.Semple SC, Akinc A, Chen J, Sandhu AP, Mui BL, Cho CK, Sah DWY, Stebbing D, Crosley EJ, Yaworski E, et al. Rational design of cationic lipids for siRNA delivery. Nat Biotechnol. 2010Feb;28(2):172–76. doi: 10.1038/nbt.1602. [DOI] [PubMed] [Google Scholar]
- 184.Pardi N, Tuyishime S, Muramatsu H, Kariko K, Mui BL, Tam YK, Madden TD, Hope MJ, Weissman D. Expression kinetics of nucleoside-modified mRNA delivered in lipid nanoparticles to mice by various routes. J Control Release. 2015Nov10;217:345–51. doi: 10.1016/j.jconrel.2015.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 185.Kariko K, Muramatsu H, Ludwig J, Weissman D. Generating the optimal mRNA for therapy: HPLC purification eliminates immune activation and improves translation of nucleoside-modified, protein-encoding mRNA. Nucleic Acids Res. 2011Nov;39(21):e142. doi: 10.1093/nar/gkr695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 186.Moderna and Lonza announce worldwide strategic collaboration to manufacture Moderna’s vaccine (mRNA-1273) against novel Coronavirus. Moderna, Inc. May2020;1:2020. [Google Scholar]
- 187.Theofilopoulos AN, Baccala R, Beutler B, Kono DH. Type I interferons (alpha/beta) in immunity and autoimmunity. Annu Rev Immunol. 2005;23:307–36. doi: 10.1146/annurev.immunol.23.021704.115843. [DOI] [PubMed] [Google Scholar]
- 188.Nestle FO, Conrad C, Tun-Kyi A, Homey B, Gombert M, Boyman O, Burg G, Liu Y-J, Gilliet M. Plasmacytoid predendritic cells initiate psoriasis through interferon-α production. J Exp Med. 2005;202(1):135–43. doi: 10.1084/jem.20050500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 189.Fischer S, Gerriets T, Wessels C, Walberer M, Kostin S, Stolz E, Zheleva K, Hocke A, Hippenstiel S, Preer KT, et al. Extracellular RNA mediates endothelial-cell permeability via vascular endothelial growth factor. Blood. 2007Oct1;110(7):2457–65. doi: 10.1182/blood-2006-08-040691. [DOI] [PubMed] [Google Scholar]
- 190.Kannemeier C, Shibamiya A, Nakazawa F, Trusheim H, Ruppert C, Markart P, Song Y, Tzima E, Kennerknecht E, Niepmann M, et al. Extracellular RNA constitutes a natural procoagulant cofactor in blood coagulation. Proc Natl Acad Sci U S A. 2007;104(15):6388–93. doi: 10.1073/pnas.0608647104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 191.Maugeri M, Nawaz M, Papadimitriou A, Angerfors A, Camponeschi A, Na M, Hölttä M, Skantze P, Johansson S, Sundqvist M, et al. Linkage between endosomal escape of LNP-mRNA and loading into EVs for transport to other cells. Nat Commun. 2019Sep24;10(1):4333. doi: 10.1038/s41467-019-12275-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192.Willman D. Federal vaccine development sites ill-suited to counter covid-19 epidemic. The Washington Post. [accessed 2020 Mar 15].
- 193.Bloom BR. The United States needs a national vaccine authority. Science. 1994Sep2;265(5177):1378–80. doi: 10.1126/science.8073275. [DOI] [PubMed] [Google Scholar]
- 194.Douglas RG. Fostering partnerships for vaccine development: a delicate fabric. Bull N Y Acad Med Summer. 1996;73:113–23. [PMC free article] [PubMed] [Google Scholar]
- 195.Trump Administration Announces Framework and Leadership for ‘Operation Warp Speed’ . United States department of health and human services. [accessed 2020 Oct 2]. https://www.hhs.gov/about/news/2020/05/15/trump-administration-announces-framework-and-leadership-for-operation-warp-speed.html
- 196.Howard KL, Wright CN. Operation warp speed: accelerated COVID-19 vaccine development status and efforts to address manufacturing challenges. Report to Congressional Addresses; 2021February.
- 197.Russell WWDEFENSE PRODUCTION ACT: opportunities exist to increase transparency and identify future actions to mitigate medical supply chain issues. Report to Congressional Committees. 2020Nov.
- 198.Cox B. How operation warp speed helps clear obstacles to COVID-19 vaccine production. informa pharma intelligence. [accessed 2021 Feb 15]. https://pink.pharmaintelligence.informa.com/PS143777/How-Operation-Warp-Speed-Helps-Clear-Obstacles-To-COVID-19-Vaccine-Production?vid=Pharma&processId=cfd18ede-9413-4c6b-a0c6-83de4f8744fd
- 199.The Access to COVID-19 Tools (ACT) Accelerator . World Health Organization. [accessed 2020 Oct 2]. https://www.who.int/initiatives/act-accelerator
- 200.Status report & plan. ACT accelerator: access to COVID-19 tools; 2020Sept. p. 1–36.
- 201.An economic investment case & financing requirements. ACT accelerator: access to COVID-19 tools; 2020Sept25.
- 202.Berkley S. COVAX explained. GAVI. [accessed 2020 Oct 2]. https://www.gavi.org/vaccineswork/covax-explained
- 203.Biological reference materials . The National Institute for Biological Standards and Control (NIBSC). [accessed 2021 Feb 9]. https://www.nibsc.org/products/brm_product_catalogue.aspx
- 204.Main outcomes of the meeting of the WHO expert committee on biological standardization held from 9 to 10 December 2020. World Health Organization. [accessed 2021 Mar 3]. https://www.who.int/publications/m/item/ECBS-Executive-Summary.IF.IK.TW-15_Dec_2020
- 205.Vaccine and Related Biological Product Guidances . U.S. food and drug administration. [accessed 2021 Feb 8]. https://www.fda.gov/vaccines-blood-biologics/biologics-guidances/vaccine-and-related-biological-product-guidances
- 206.Biologicals: active substance . European Medicines Agency. [accessed 2021 Feb 8]. https://www.ema.europa.eu/en/human-regulatory/research-development/scientific-guidelines/biologicals/biologicals-active-substance
- 207.Biologicals: finished product . European medicines agency. [accessed 2021 Feb 8]. https://www.ema.europa.eu/en/human-regulatory/research-development/scientific-guidelines/biologicals/biologicals-finished-product
- 208.Schofield I. EMA: no application received for Sputnik V vaccine. Informa Pharma Intelligence. [accessed 2021 Feb 15]. https://pink.pharmaintelligence.informa.com/PS143771/EMA-No-Application-Received-For-Sputnik-V-Vaccine
- 209.Zerhouni E, Hamburg M. The need for global regulatory harmonization: a public health imperative. Sci Transl Med. 2016;8(338):338ed6–338ed6. doi: 10.1126/scitranslmed.aaf1396. [DOI] [PubMed] [Google Scholar]
- 210.Health product and policy standards. World Health Organization; 2021Feb8. [Google Scholar]
- 211.Coronavirus disease (COVID-19): vaccine access and allocation. World Health Organization. [accessed 2021 Dec 12]. https://www.who.int/news-room/q-a-detail/coronavirus-disease-(covid-19)-vaccine-access-and-allocation
- 212.Patrick SM, Wright JA. Designing a global coalition of medicines regulators; 2014.
- 213.Atouf F, Venema J. Do standards matter? What is their value? J Pharm Sci. 2020May1;109(8):2387–92. doi: 10.1016/j.xphs.2020.04.017. [DOI] [PubMed] [Google Scholar]
- 214.Lichfield G. This is what it will take to get us back outside. MIT Technology Review. Massachusetts Institute of Technology; 2020. [Google Scholar]
- 215.Thomson-Deveaux A, Paine N. Even with a vaccine, the economy could take many months to return to normal. ABC News. [accessed 2020 Sept 7]. https://fivethirtyeight.com/features/even-with-a-vaccine-the-economy-could-take-many-months-to-return-to-normal
- 216.Zhang S. A vaccine reality check. The Altantic. Washington DC: Romer, Hayley; 2020. [Google Scholar]
- 217.CDC . Health equity considerations and racial and ethnic minority groups. Centers for Disease Control and Prevention. [accessed 2020 Sept 7]. https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html
- 218.AMA . Impact of COVID-19 on minoritized and marginalized communities. American Medical Association. [accessed 2020 Sept 7]. https://www.ama-assn.org/delivering-care/health-equity/impact-covid-19-minoritized-and-marginalized-communities
- 219.Artiga S, Orgera K, Pham O, Corallo B. Growing data underscore that communities of color are being harder hit by COVID-19. Policy Watch. [accessed 2020 Apr 12]. https://www.kff.org/policy-watch/growing-data-underscore-communities-color-harder-hit-covid-19/
- 220.Laurencin CT, McClinton A. The COVID-19 pandemic: a call to action to identify and address racial and ethnic disparities. J Racial Ethn Health Disparities. 2020;7(3):398–402. doi: 10.1007/s40615-020-00756-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 221.Koyama T, Weeraratne D, Snowdon JL, Parida L. Emergence of drift variants that may affect COVID-19 vaccine development and antibody treatment. Pathogens. 2020;9(5):324. doi: 10.3390/pathogens9050324. [DOI] [PMC free article] [PubMed] [Google Scholar]