

Abstract
Objective:
To analyze variations in palatal morphology in subjects presenting unilaterally impacted maxillary permanent central incisors compared with a control group of subjects without eruption anomalies using a three-dimensional (3D) analysis.
Materials and Methods:
Twenty-six white subjects (10 girls and 16 boys; mean age 9.5 ± 1.5 years) with unilaterally impacted maxillary permanent central incisors (impacted incisor group [IIG]) were compared with a control group (CG) of 26 subjects (14 girls and 12 boys, mean age 8.7 ± 1.6 years) presenting no eruption disorders. For each subject, dental casts were taken and the upper arch was scanned using a 3D laser scanner. To study the entirety of the shape of the palate in any point of the surface, 3D geometric morphometrics was applied.
Results:
Subjects with impacted maxillary incisors showed skeletal adaptations of the maxilla. In the IIG, both the superior palatal region and lateral palatal surface showed significantly different morphology when compared with CG, with a narrower and higher palatal vault.
Conclusion:
The absence of maxillary central incisors over the physiological age of eruption influenced the development of the palatal morphology compared with subjects without eruption anomalies.
Keywords: Impacted incisors, Palatal morphology, Three-dimensional analysis
INTRODUCTION
Failure of eruption of permanent upper incisors is an infrequent observation in dental practice, but its treatment is essential because of the keen importance of these teeth in the smile's esthetics. This pathologic condition of the early mixed dentition phase occurs in 0.2% to 1.0% of the population.1
Supernumerary teeth and odontomas are the most common cause of failure of eruption. Other factors that can lead to the failure of maxillary incisors eruption are dilacerated teeth, tooth malposition, abnormal inclination and crowding, persistent primary maxillary incisors, trauma leading to dilacerations and developmental displacement, dense mucoperisteum, follicular cysts, and nonvital primary teeth.2,3
During normal eruption, the two permanent central incisors emerge within the arch almost concomitantly. In the presence of only one fully erupted central incisor, the practitioner should examine the potential causes of the contralateral incisor's delayed eruption.4 Early diagnosis is very important, and interceptive orthodontic treatment could not only improve skeletal relationship and eliminate functional interferences but also may correct disturbances during the eruption.5
Geometric morphometrics has been proposed in the literature6 as an original method of visualization of shape changes. It can show three-dimensional (3D) morphological changes in their complexity, in a more effective way than traditional bidimensional measurements used for morphometric analyses. Geometric morphometrics is also used to address an increasingly varied range of questions about evolution and development of organisms.7
No data are available in the literature with regard to morphological changes in the maxilla produced by failure of eruption of a permanent incisor, as assessed with a 3D morphometric analysis. The aim of this study was to analyze the morphological characteristics of the palatal vault, comparing subjects with a unilaterally impacted maxillary central incisor and a control group of subjects without eruption anomalies by using 3D geometric morphometrics. The purpose was to understand if the effects of eruption disorders of upper central incisors may influence the development of the palate.
MATERIALS AND METHODS
For the present study, ethical approval was obtained from the Ethical Committee of the University of Rome Tor Vergata, and informed consent was obtained from the subjects' parents before inclusion.
Twenty-six white subjects (10 girls, 16 boys) with unilaterally impacted maxillary permanent central incisors who sought orthodontic treatment at the Department of Orthodontics at the University of Rome Tor Vergata were selected. The mean age of the subjects was 9.5 years (SD = 1.5 years).
The additional inclusion criteria for the enrollment of the subjects in the impacted incisor group (IIG) were white ancestry, eruption of the contralateral incisor at least 6 months earlier or deviation from the normal sequence of eruption (lateral incisor erupted prior to the central incisor), no posterior or anterior crossbite, normal overjet and overbite values, intermediate mixed dentition (first permanent molars and incisors erupted), mixed dentition with a Class I or edge-to-edge molar relationship (46.2% Class I, 53.8% end-to-end molar relationship), skeletal Class I relationships, prepubertal stage of cervical vertebral maturation as assessed on lateral cephalograms (CS1, CS2),8 absence of previous orthodontic treatment or tooth extraction, and the absence of sucking habits, craniofacial syndromes, cysts, cleft lip and/or palate, or multiple and/or advanced caries. A panoramic radiograph and cephalometric radiograph were taken for all subjects at the time of initial observation to confirm the diagnosis of incisors' impaction and planned a treatment.
This group was compared with a control group (CG) of 26 prepubertal subjects (14 girls, 12 boys) with no eruption disorders in the permanent incisors and a mean age of 8.7 years (SD = 1.6 years). All were in intermediate mixed dentition with a Class I or end-to-end molar relationship (50% Class I, 50% end-to-end molar relationship). The CG group matched the IIG in terms of dentition stage, skeletal relationship, and skeletal maturation.
To analyze the palate's shape, study casts of the maxillary arches of all subjects were scanned using an intraoral scanner (Carestream 3500) with a reported accuracy of 30 μm. The scanning of the maxillary dental casts with the intraoral scanner was done by using a predetermined order. It started with the most distal tooth in the first quadrant continuing to the anterior teeth and then to the second quadrant. Each tooth was scanned from its buccal and lingual sides (placing the camera at an angle of less than 45° to the tooth axis). After that, the palate vault was scanned starting on the right side and ending on the left side first of the premaxillary region and then of the maxillary posterior region.
All models were exported in a Standard Tesselation Language format (.stl digital file). To study the entirety of the shape of the palate at any point of the surface, 3D geometric morphometrics (GMM) analysis was used.9–12
A template for data set/collection of homologous landmarks describing a palate was created with Viewbox (dHAL software, Kifissia, Greece) and used to digitize each upper maxillary digital cast of all subjects.
The boundaries of the palate were defined as a midline passing on the raphe medianus, a perimeter line passing apical to the gingival sulci of each tooth, and a posterior line passing from distal of the first molars. Sliding semi-landmarks were evenly distributed on the surface defined by boundaries.13 A total of 240 points were registered for each palate (Figure 1).
Figure 1.

The template of 240 landmarks and semi-landmarks used to study the palatal shape.
The average of the data set was calculated and used as a fixed reference to allow all sliding landmarks of each palate to slide on the surface and become more and more homologous from subject to subject. The procedure was repeated three times. The average palatal template of the IIG and the CG was then calculated.
An ideal palatal surface was then warped (adapted) to the average data set of both IIG and CG.14,15 The two palates' average shapes were superimposed through Viewbox with an iterative closest point procedure. This procedure allows easy visualization of differences between the average of each group. Distances between the average palate of the IIG and CG were also measured with a color map tool that was built into the software.
Statistical Analysis
Generalized partial least square Procustes superimposition was used to extract Procrustes coordinates for shape description. Principal component analysis (PCA) was performed on the Procrustes coordinates to reveal the main patterns of shape variation. The calculations were carried out using Viewbox 4 software.6
Method error was assessed by repeated digitization of 20 randomly selected study casts by the same investigator after a period of 10 days.
RESULTS
Method Error
The average Procrustes distance between repeated digitization of 20 study casts was 6.41% (SD = 2.27%) of the total variance of the sample.
Procrustes Superimposition and PCA
Figures 2 and 3 show for the two groups a cluster distribution of the palatal shape space after Procustes superimposition. A statistically significant shape difference between the palate's shape of IIG and CG was found (10,000 permutations, P < .01).
Figure 2.
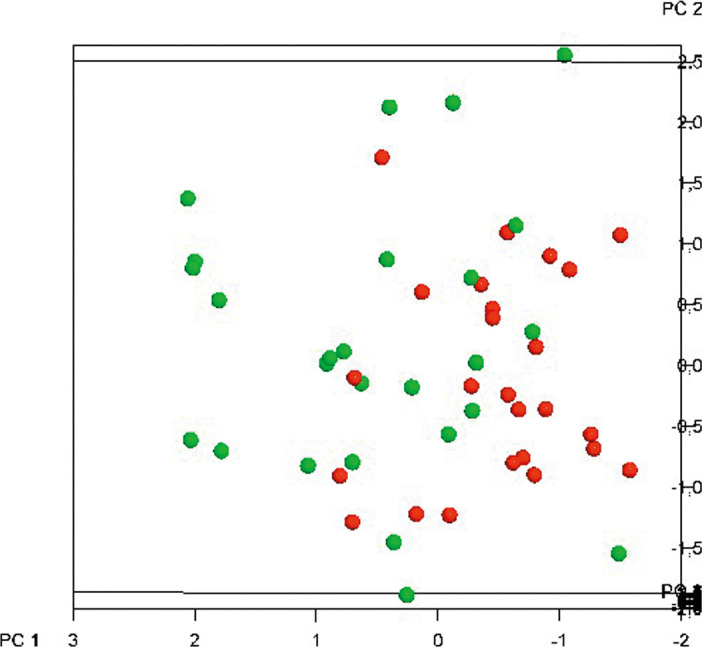
Plot of the sample individual distribution. Red spheres: GC; green spheres: IIG.
Figure 3.
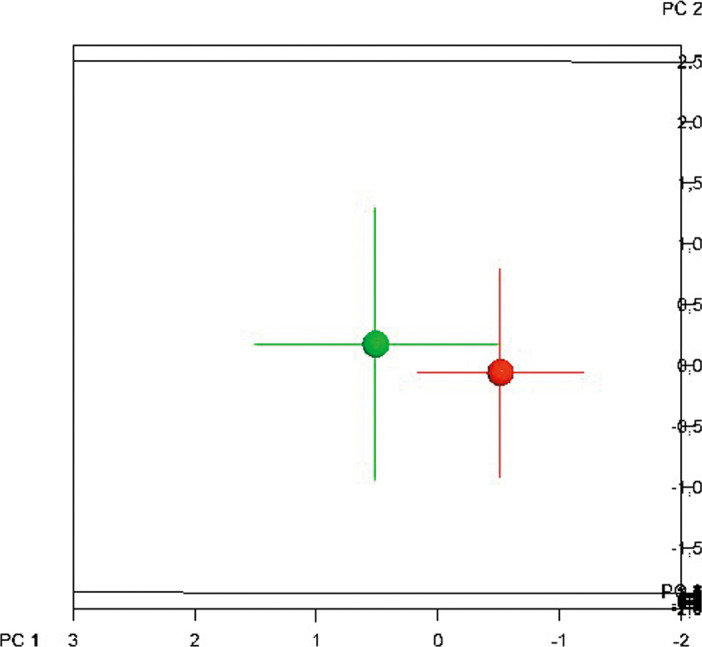
Plot of the sample average distribution. Red sphere: GC; green sphere: IIG.
The first three principal components were considered to be meaningful as they explain about 70% of total shape variance. PC1, explaining 46.7% of the total differences, shows shape differences in all three dimensions: variability is shown in terms of palatal width, height, and length differences (Figure 4). PC2 and PC3 were mostly associated with vertical dimension and palatal height variations.
Figure 4.

Graphic depictions (palate) of the first principal component. (a) Transverse view. (b) Sagittal view. (c) Posterior view. (d) Global view from above.
When comparing the IIG and CG samples in the frontal and lateral views (Figure 4a,b), significant palatal shape changes were found, with the greatest deformation located in the lateral and superior region.
This deformation could be described as a simultaneous vertical extension in the entire palatal vault and horizontal compression in the lateral region of the palate in the IIG (blue points) vs the control group (red points); that is, the palate is narrower, longer, and higher in the IIG compared with the CG. The vertical extension of the palatal vault is also evident in the hard palate area, as shown in the posterior view (Figure 4c).
A mesh was adapted through warping to the average palates both for IIG and CG samples. A colorimetric map was used to visually present differences between the two shapes: green represents virtually no changes, whereas blue represents a positive (outer surface) distance and red represents a negative (inner surface) distance of one surface compared with the other (Figure 5).
Figure 5.

Colorimetric maps showing the differences in shape between the palates of IIG vs CG. (a) Global vision from above. (b) Sagittal vision.
DISCUSSION
This study aimed to analyze the anatomical characteristics of the palatal vault, comparing subjects with a unilaterally impacted maxillary central incisor and a CG of subjects without eruption anomalies by using 3D analysis of digital dental casts. The primary objective was to visualize the effects of eruption disorders on the development of the anterior maxillary arch.
No data are reported in the literature about the influence of the teeth eruption disorders on the development of maxillary complex. A previous study16 identified 23 subjects with impacted maxillary incisors. Diagnostic casts served to measure both intermolar and intercanine widths. The authors concluded that subjects with impacted maxillary incisors exhibit transverse maxillary deficiency in the anterior and posterior portion of the dental arch. Furthermore, the analysis of the palatal morphology and of the maxillary dimension has been evaluated usually by 2D transverse dental measurements on dental casts, giving only incomplete information about the morphology of the palatal vault.17 To overcome this limitation, an evaluation of 3D characteristics of the palatal vault by means of 3D technology has been used.18 GMM analysis showed that maxillary shape changes could be recorded in the cross-sectional comparison between the IIG and CG.
Data from the current study indicate that subjects with impacted maxillary incisors show a transverse maxillary deficiency compared with the CG. In particular, the superior palatal region and the lateral maxillary surface were different between the two groups. As shown in Figures 4 and 5, the absence of maxillary central incisors over the physiological age of eruption influenced the development of a different maxillary morphology with a narrower and higher palatal vault compared with subjects without eruption anomalies.
The overall growth maxillary changes are the result of both a downward and forward translation of the maxilla and a simultaneous surface remodeling.19 As reported by Enlow and Hans,20 the maxillary growth is mainly determined by both a downward and forward translation of the maxilla and a simultaneous surface remodeling especially during certain stages of dental development such as during complete eruption of the maxillary incisors. The teeth actively drift inferiorly at the same time, by remodeling growth within the alveolar sockets. In growing children, the development of the palatal vault is influenced by local factors, so when incisors do not erupt, the remodeling of the anterior surface of maxilla does not take place.
The IIG displayed a reduction in the transversal dimension of the premaxillary area, especially between the two central incisors and in the canine region (Figure 5a). The loss of space in the anterior region accounts for many of the cases that failed to show spontaneous eruption of delayed incisors.21
In these cases, the clinician must choose a therapeutic protocol to correct the anterior space deficiency and to improve the intraosseous positions of the impacted teeth.22
Pavoni et al.22 supported the use of rapid maxillary expansion (RME) to decrease the incidence of impacted incisors. The use of RME in early mixed dentition increases the anterior segment of the maxillary arch,23 allowing an improvement of incisor intraosseous vertical and angular position and a recovery of space in the upper arch.24
When the central incisors erupt, the sagittal dimension of the maxillary arch should be controlled. The absence of a permanent incisor is usually accompanied by a shift of the adjacent teeth, so the improvement in the perimeter of the upper arch facilitated by cervical pull headgear can help to prevent the mesial movement of the distal segment of the upper dental arch.25
CONCLUSIONS
GMM can be a useful tool for describing the 3D shape changes of maxillary surfaces in children with impacted incisors.
Children with unilaterally impacted maxillary permanent central incisors showed a narrower and higher palatal vault when compared with a control group of subjects without impaction.
REFERENCES
- 1.Kurol J. Early treatment of tooth eruption disturbances. Am J Orthod Dentofacial Orthop. 2002;121:588–591. doi: 10.1067/mod.2002.124173. [DOI] [PubMed] [Google Scholar]
- 2.Kolokitha OE, Papadopoulou AK. Impaction and apical root angulation of the maxillary central incisors due to supernumerary teeth: combined surgical and orthodontic treatment case report. Am J Orthod Dentofacial Orthop. 2008;134:153–160. doi: 10.1016/j.ajodo.2006.08.020. [DOI] [PubMed] [Google Scholar]
- 3.Betts A, Camilleri GE. A review of 47 cases of unerupted maxillary incisors. Int J Paediatr Dent. 1999;9:285–292. doi: 10.1111/j.1365-263x.1999.00147.x. [DOI] [PubMed] [Google Scholar]
- 4.Chokron A, Reveret S, Salmon B, et al. Strategies for treating an impacted maxillary central incisor. Int Orthod. 2010;8:152–176. doi: 10.1016/j.ortho.2010.03.001. [DOI] [PubMed] [Google Scholar]
- 5.Cozza P, Marino A, Laganà G. Interceptive management of eruption disturbances: case report. J Clin Pediatr Dent. 2004;29:1–4. doi: 10.17796/jcpd.29.1.82827t4j53t83758. [DOI] [PubMed] [Google Scholar]
- 6.Papagiannis A, Halazonetis DJ. Shape variation and covariation of upper and lower dental arches of an orthodontic population. Eur J Orthod. 2015. pp. 1–10. [DOI] [PMC free article] [PubMed]
- 7.Klingenberg CP. Evolution and development of shape: integrating quantitative approaches. Nat Rev Genet. 2010;11:623–635. doi: 10.1038/nrg2829. [DOI] [PubMed] [Google Scholar]
- 8.Baccetti T, Franchi L, McNamara JA., Jr The cervical vertebral maturation (CMV) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod. 2005;11:119–129. [Google Scholar]
- 9.Mitteroecker P, Gunz P. Advances in geometric morphometrics. Evol Biol. 2009;36:235–247. [Google Scholar]
- 10.Klingenberg CP. Visualizations in geometric morphometrics: how to read and how to make graphs showing shape changes. Hystrix. 2013;24(1):1–10. [Google Scholar]
- 11.Polychronis G, Halazonetis DJ. Shape covariation between the craniofacial complex and first molars in humans. J Anat. 2014;225:220–231. doi: 10.1111/joa.12202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gunz P, Mitteroecker P, Bookstein FL. Semilandmarks in 3D. In: Slice DE, editor. Modern Morphometrics in Physical Anthropology Developments in Primatology: Progress and Prospects. New York: Kluwer Academic Publishers-Plenum Publishers;; 2005. pp. 73–98. [Google Scholar]
- 13.Adams DC, Rohlf FJ, Slice DE. A field comes of age: geometric morphometrics in the 21st century. It J Mamm. 2013. pp. 1–8.
- 14.Glasbey CA, Mardia KV. A review of image-warping methods. J Appl Stat. 1998;25:155–171. [Google Scholar]
- 15.Huanca Ghislanzoni L, De Simone M, Rosati R, Bottino A, Sforza C. A new 3-dimensional method for the construction of an average dental arch. J World Fed Orthod. 2014;3:2–6. [Google Scholar]
- 16.Pavoni C, Franchi L, Buongiorno M, Cozza P. Evaluation of maxillary arch morphology in children with unilaterally impacted incisors via three-dimensional analysis of digital dental casts: a controlled study. J Orofac Orthop. 2016;77:16–21. doi: 10.1007/s00056-015-0003-3. [DOI] [PubMed] [Google Scholar]
- 17.Lione R, Buongiorno M, Franchi L, Cozza P. Evaluation of maxillary arch dimensions and palatal morphology in mouth-breathing children by using digital dental casts. Int J Pediatr Otorhinolaryngol. 2014;78:91–95. doi: 10.1016/j.ijporl.2013.09.028. [DOI] [PubMed] [Google Scholar]
- 18.Gracco A, Malaguti A, Lombardo L, Mazzoli A, Raffaeli R. Palatal volume following rapid maxillary expansion in mixed dentition. Angle Orthod. 2009;80:153–119. doi: 10.2319/010407-7.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Proffit WR, Fields HW, Sarver DM. Contemporary Orthodontics. Amsterdam, The Netherlands: Elsevier; 2013. 5th ed. [Google Scholar]
- 20.Enlow DH, Hans MG. Essentials of Facial Growth. Philadelphia: WB Saunders;; 1996. [Google Scholar]
- 21.Pavoni C, Franchi L, Laganà G, et al. Management of impacted incisors following surgery to remove obstacles to eruption: a prospective clinical trial. Pediatr Dent. 2013;35:364–368. [PubMed] [Google Scholar]
- 22.Pavoni C, Franchi L, Laganà G, Cozza P. Radiographic assessment of maxillary incisor position after rapid maxillary expansion in children with clinical signs of eruption disorder. J Orofac Orthop. 2013;74:468–479. doi: 10.1007/s00056-013-0180-x. [DOI] [PubMed] [Google Scholar]
- 23.Lione R, Pavoni C, Laganà G, et al. Rapid maxillary expansion: effects on palatal area investigated by computed tomography in growing subjects. Eur J Paediatr Dent. 2012;13:215–218. [PubMed] [Google Scholar]
- 24.Baccetti T, Mucedero M, Leonardi M, Cozza P. Interceptive treatment of palatal impaction of maxillary canines with rapid maxillary expansion: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2009;136:657–661. doi: 10.1016/j.ajodo.2008.03.019. [DOI] [PubMed] [Google Scholar]
- 25.Armi P, Cozza P, Baccetti T. Effect of RME and headgear treatment on the eruption of palatally displaced canines: a randomized clinical study. Angle Orthod. 2011;81:370–374. doi: 10.2319/062210-339.1. [DOI] [PMC free article] [PubMed] [Google Scholar]