

Abstract
Patient: Female, 24-year-old
Final Diagnosis: Primary infertility • yolk sac tumor
Symptoms: Abdomen distension • infertility
Medication: —
Clinical Procedure: Salpingo-oophorectomy
Specialty: Obstetrics and Gynecology • Oncology • Pathology
Objective:
Unusual setting of medical care
Background:
A yolk sac tumor (YST) is a rare, malignant tumor of cells that line the yolk sac of the embryo. It most frequently occurs in the ovary (ovarian yolk sac tumor: OYST) in children and adolescents. Thus, fertility-preservation treatment is a concern.
Case Report:
A 24-year-old nulliparous woman visited us for infertility treatment and then right OYST was detected. A uni-lateral right salpingo-oophorectomy, infra-colic omentectomy, ipsilateral lymph node dissection, and peritoneal biopsies were performed. Histological examination confirmed the diagnosis of a stage IC OYST. Six cycles of bleomycin-etoposide-cisplatin chemotherapy were performed. She had no recurrence over the next 16 months. She conceived by in-vitro fertilization, and abdominally gave birth to a term infant. Both mother and baby had a smooth recovery.
Conclusions:
This case adds further evidence to the 5-year survival and progression-free survival following surgery and chemotherapy in OYSTs, while preserving fertility.
Keywords: Germ Cells, Pregnancy, Yolk Sac
Background
Malignant ovarian germ cell tumors account for 2–3% of all ovarian tumors. There are 2 types: germinomatous and nongerminomatous [1].
Ovarian yolk-sac tumors (OYSTs), also known as endodermal sinus tumors, are the second most common malignant germ cell tumors of the ovaries after dysgerminomas [2]. They represent 20% of germinal tumors of the ovary. Most of these tumors tend to occur in women around the age of 35 years, which encompasses the prime reproductive years [3].
Due to their rarity, OYSTs are usually referred to a gynecological oncologist for further management [4].
A combination of fertility-sparing surgical strategies and chemotherapy have been proven to preserve fertility, with a 94% 5-year survival rate when patients are treated with bleomycin, etoposide, and cisplatin (BEP) chemotherapy [5].
The earlier chemotherapy is administered, and the younger the woman, the better is the outcome. In a study of 52 patients, 97% of affected women resumed menstruation, with a fertility rate of 75% among those contemplating conception [6]. On the other hand, a survey of the long-term effect of chemotherapy showed that a small percentage of women had menstrual irregularities and subfertility [7].
Recently, there has been a renewed interest in the fertility-preserving approach for younger women with OYSTs, in the form of unilateral salpingo-oophorectomy and omentectomy, with uterine preservation [8].
In contrast to reproductive-age women, those who have completed childbearing and postmenopausal women should rather undergo radical surgery [9].
Case Report
In 2013, a 24-year-old nulliparous Mediterranean woman presented to the assisted conception unit with a 2-year history of primary subfertility due to oligozoospermia. She reported occasional abdominal distension, with no weight loss or ascites. Pelvic ultrasound and MRI revealed the presence of a right ovarian complex cystic mass with a diameter of 15×15 cm. Laboratory results revealed an AFP level of 28 000 ng/ml (normal <10 ng/ml), with normal levels of other tumor markers. Surgery was scheduled due to concern for the possible presence of a malignant germ cell tumor (yolk sac tumor).
Due to the patient’s age and desire for future childbearing, a fertility-sparing surgical strategy was chosen. A unilateral right salpingo-oophorectomy was performed through an abdominal midline incision. Infra-colic omentectomy, ipsilateral lymph node dissection, and peritoneal biopsies were performed. There was no gross disease of the left ovary, uterus, and fallopian tube, and they were left in situ. On pathological examination, the cut surface of the tumor showed alternating white, brown, and hemorrhagic areas. Histopathology confirmed a malignant yolk sac tumor (Figures 1, 2). The cytology of the peritoneal washing was positive for malignancy. A stage IC tumor was designated, according to the International Federation of Gynecology and Obstetrics classification (FIGO).
Figure 1.
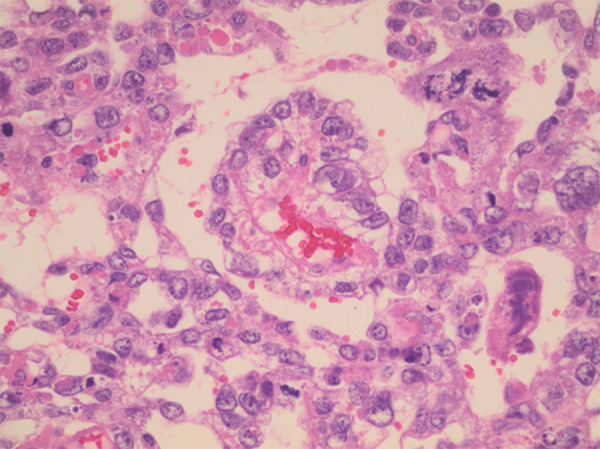
A tubulopapillary sinusoidal structure with central vascular core and cuboidal to columnar epithelial-like cell lining (Schiller-Duval body).
Figure 2.
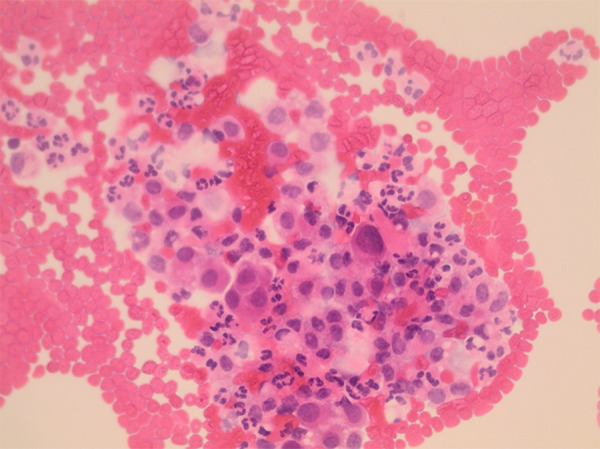
Cytospin preparation shows clusters of atypical large cells with high N/C ratio.
Postoperative chemotherapy was started in the form of bleomycin-etoposide-cisplatin (BEP), with 6 cycles over 12 months.
Following surgery, the AFP levels dropped to 3898 ng/ml, as measured prior to commencing chemotherapy. Subsequent AFP levels decreased to 2 ng/ml. Follow-up by CT imaging and tumor markers over the following 16 months were in the normal range, after which she was lost to follow-up.
Following that, the patient underwent 2 attempts at in-vitro fertilization by intra-cytoplasmic sperm injection, the indication being oligozoospermia, at a private assisted reproduction clinic. The first attempt ended in failure, but the second one was a success.
The antenatal period at our hospital was uneventful, except for the finding of intrauterine fetal growth restriction. All other clinical, hematological, and ultra-sonographic investigations were normal. At the 37 weeks of gestation, the patient underwent an elective cesarean section. A live male baby, weighing 2200 g, with an Apgar score of 8 at 1 min and 9 at 5 min, was delivered.
At the cesarean section, gross inspection and palpation revealed no signs of tumor recurrence, and the left ovary and fallopian tube were healthy.
Discussion
Yolk sac tumors are considered rare in both sexes [10]. They commonly arise in the gonads but sometimes can occur outside and are called gonadal germ cell tumors. Abdominal pain and distension may be the only clinical presentation, which is usually that of any highly malignant tumor of the ovaries. Endocrine manifestations are extremely rare, as only 3 cases have been reported [11].
Various diagnostic modalities can aid the diagnosis of YSTs, such as US, CT, MRI and histopathological analysis [12]. On CT and MRI studies an OYST appears as an enhancing large solid cystic mass with intra-tumoral hemorrhage [13], and on histo-pathology they display a focal papillary pattern with Schiller-Duval bodies (Figure 1).
It has been suggested that AFP can be applied as a tumor marker as its level is elevated in about 90% of cases [14]. In our case, the AFP level was elevated to 28 000 ng/ml. The plan was to follow up by alpha-feto-protein every 3 months, with yearly CT scan for 2 years.
The diagnosis and prognosis of patients can be monitored by AFP levels post-operatively and during chemotherapy. This is supported by several studies showing that a lower level of postoperative serum AFP is a useful marker for eliciting any residual cancer cells [15].
However, it has been suggested that an increase in the levels of AFP is more sensitive than specific [16]. Therefore, a slight increase may not be considered a sole criterion for decision-making during chemotherapy.
Without any treatment, YSTs are almost universally fatal [17]. The standard approach to OYSTs is debulking surgery, followed by adjuvant chemotherapy. Most cases are expected to be cured with conservative surgery and BEP chemotherapy [5]. It has been found that the overall 5-year disease-free survival rates with stage I/II and stage III/IV OYSTs were 94% and 90%, respectively [18].
There is a risk of damage to the gonads as a sequelae of chemotherapy. Studies reveal that most women revert to normal menstruation and reproductive function after treatment; thus, fertility could be preserved [19]. Fertility-preservation treatment is usually considered and actually performed in patients with OYST; we herein reconfirm its importance.
Conclusions
This case report adds further evidence to the 5-year survival and progression-free survival following surgery and chemo-therapy in OYSTs, while preserving fertility. In addition, it highlights the need for a multidisciplinary approach involving gynecological oncologists, general oncologists, and radiologists in the management of women with OYSTs.
Acknowledgments
Many thanks to Jordan University of Science and Technology/ King Abdullah University Hospital.
Footnotes
Declaration of Figures Authenticity
All figures submitted have been created by the authors who confirm that the images are original with no duplication and have not been previously published in whole or in part.
References:
- 1.Euscher ED. Germ cell tumors of the female genital tract. Surg Pathol Clin. 2019;12(2):621–49. doi: 10.1016/j.path.2019.01.005. [DOI] [PubMed] [Google Scholar]
- 2.de La Motte Rouge T, Pautier P, et al. Prognostic factors in women treated for ovarian yolk sac tumour: A retrospective analysis of 84 cases. Eur J Cancer. 2011;47(2):175–82. doi: 10.1016/j.ejca.2010.08.012. [DOI] [PubMed] [Google Scholar]
- 3.Aviki EM, Abu-Rustum NR. A call to standardize our approach to fertility-sparing surgery in patients with gynecologic cancers. Gynecol Oncol. 2017;147(3):491–92. doi: 10.1016/j.ygyno.2017.11.001. [DOI] [PubMed] [Google Scholar]
- 4.Hodroj K, Stevovic A, Attidnon V, et al. Molecular charactarization of ovarian yolk sac tumor (OYST) Cancers (Basel) 2021;13(2):E220. doi: 10.3390/cancers13020220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Even C, Lhommé C, Duvillard P, et al. [Ovarian yolk sac tumour: General review] Bull Cancer. 2011;98(8):963–75. doi: 10.1684/bdc.2011.1387. [in French] [DOI] [PubMed] [Google Scholar]
- 6.Nasioudis D, Chapman-Davis E, Frey MK, et al. Management and prognosis of ovarian yolk sac tumors; An analysis of the National Cancer Data Base. Gynecol Oncol. 2017;147(2):296–301. doi: 10.1016/j.ygyno.2017.08.013. [DOI] [PubMed] [Google Scholar]
- 7.Wang PH, Chao HT, Chao KC. Chemotherapy-induced gonadotoxicity. Taiwan J Obstet Gynecol. 2010;49(1):1–2. doi: 10.1016/S1028-4559(10)60001-0. [DOI] [PubMed] [Google Scholar]
- 8.Nasioudis D, Frey MK, Chapman-Davis E, et al. Fertility-preserving surgery for advanced stage ovarian germ cell tumors. Gynecol Oncol. 2017;147(3):493–96. doi: 10.1016/j.ygyno.2017.10.010. [DOI] [PubMed] [Google Scholar]
- 9.de La Motte Rouge T, Pautier P, Duvillard P, et al. Survival and reproductive function of 52 women treated with surgery and bleomycin, etopo-side, cisplatin (BEP) chemotherapy for ovarian yolk sac tumor. Ann Oncol. 2008;19(8):1435–41. doi: 10.1093/annonc/mdn162. [DOI] [PubMed] [Google Scholar]
- 10.Maizlin II, Dellinger M, Gow KW, et al. Testicular tumors in prepubescent patients. J Pediatr Surg. 2018;53(9):1748–52. doi: 10.1016/j.jpedsurg.2017.09.020. [DOI] [PubMed] [Google Scholar]
- 11.Safdar NS, Stall JN, Young RH. Malignant mixed germ cell tumors of the ovary: An Analysis of 100 cases emphasizing the frequency and interrelationships of their tumor types. Am J Surg Pathol. 2021;45(6):727–41. doi: 10.1097/PAS.0000000000001625. [DOI] [PubMed] [Google Scholar]
- 12.Eddaoualline H, Sami H, Rais H, et al. Ovarian Yolk sac tumor: A case report and literature review. Clin Case Rep Int. 2018;2:1057. [Google Scholar]
- 13.Li Y, Zheng Y, Lin J, et al. Radiological-pathological correlation of yolk sac tumor in 20 patients. Acta Radiol. 2016;57(1):98–106. doi: 10.1177/0284185114561916. [DOI] [PubMed] [Google Scholar]
- 14.Khan IU, Jose J, Fawazy T, et al. Testicular yolk sac tumor in an eight-month-old child: A case report. Gulf Med. J. 2012;1:37–40. [Google Scholar]
- 15.Sell A, Sogaard H, Norgaard-Pedersen B. Serum alpha-fetoprotein as a marker for the effect of post-operative radiation therapy and/or chemo-therapy in eight cases of ovarian endodermal sinus tumour. Int J Cancer. 1976;18(5):574–80. doi: 10.1002/ijc.2910180505. [DOI] [PubMed] [Google Scholar]
- 16.Albany C, Einhorn L. Pitfalls in management of patients with germ cell tumors and slight elevation of serum α-fetoprotein. J Clin Oncol. 2014;32(19):2114–15. doi: 10.1200/JCO.2014.56.0607. [DOI] [PubMed] [Google Scholar]
- 17.Zhang GY, Zhang R, Wu LY, et al. Neoadjuvant bleomycin, etoposide, and cisplatin (BEP) chemotherapy in the treatment of extensively advanced yolk sac tumors: A single center experience. Int J Gynecol Cancer. 2018;28(4):713–20. doi: 10.1097/IGC.0000000000001209. [DOI] [PubMed] [Google Scholar]
- 18.de La Motte Rouge T, Pautier P, Duvillard P, et al. Survival and reproductive function of 52 women treated with surgery and bleomycin, etopo-side, cisplatin (BEP) chemotherapy for ovarian yolk sac tumor. Ann Oncol. 2008;19(8):1435–41. doi: 10.1093/annonc/mdn162. [DOI] [PubMed] [Google Scholar]
- 19.Zanetta G, Bonazzi C, Cantù MG, et al. Survival and reproductive function after treatment of malignant germ cell ovarian tumors. J Clin Oncol. 2001;19(4):1015–20. doi: 10.1200/JCO.2001.19.4.1015. [DOI] [PubMed] [Google Scholar]