

Abstract
Objective:
To compare the treatment effects of mini-implants as anchor units with conventional methods of anchorage reinforcement in maxillary dentoalveolar protrusion patients in terms of skeletal, dental, and soft tissue changes.
Materials and Methods:
We searched the databases of the Cochrane Library, PubMed, OVIDSP, CBM, VIP, WanFang Data, and CNKI covering December 1966 to March 2016 for randomized controlled trials (RCTs) and clinical controlled trials that compared the treatment effects of mini-implants with conventional anchorage reinforcement in maxillary dentoalveolar protrusion patients. Literature filtering, data extraction, and methodological quality evaluation were finished independently by two researchers and disagreements were solved by discussion. Meta-analysis was performed when possible; otherwise descriptive assessment was done.
Results:
Through a predefined search strategy, we finally included 14 eligible studies. Eight outcomes were evaluated in this study: maxillary incisor retraction, maxillary molar movement, U1-SN, SNA, SN-MP, UL-E Plane, NLA and G-Sn-Pg.
Conclusions:
Mini-implant anchorage was more effective in retracting the anterior teeth, produced less anchorage loss, and had a greater effect on SN-MP for the high-angle patients than did traditional anchorage. Both mini-implants and traditional anchorage underwent decreases in on U1-SN and SNA. More qualified RCTs are required to make reliable recommendations about the anchorage capacity of mini-implant and traditional anchorage in patients with maxillary dentoalveolar protrusion, especially on the UL-E plane, NLA, and G-Sn-Pg.
Keywords: Systematic review, Implant, Traditional anchorage, Protrusion
INTRODUCTION
Anchorage control in treating severe maxillary dentoalveolar protrusion patients is a difficult problem.1 Treatment of this malocclusion often includes extraction of maxillary (or bimaxillary) first or second premolars and maximum anchorage.2 To reinforce anchorage, various auxiliaries can be used, including a Nance holding arch, headgear, transpalatal arch,3 and others. However, all these methods have inherent disadvantages, such as complicated designs, need for exceptional patient cooperation, and elaborate wire bending.4 Thus, some anchorage loss or mesial movement of the maxillary molars is usually observed.
In recent years, the mini-implant has gained enormous popularity in the orthodontic community.5 Mini-implant is used herein as a generic term for all temporary bone-anchored devices. It can provide stable bony anchorage and overcome problems of anchorage loss during extraction space closure, which usually occurs with traditional methods of anchorage preparation.6 However, there is little accurate scientific evidence pertaining to the superiority of the mini-implant anchorage system over traditional anchorage technique in patients with maxillary dentoalveolar protrusion, with the few published studies demonstrating conflicting results. Upadhyay1 found intrusion and distalization of maxillary molars using mini-implants as anchorage in patients with dentoalveolar protrusion. However, Lai et al.7 found that mini-implant anchorage afforded greater anterior tooth retraction and less maxillary molar mesialization than did the headgear.
In clinical practice, orthodontists' concern is which anchorage type—traditional anchorage or the implant—would be more effective.8 The aim of this review is to compare the treatment effects with mini-implants in maxillary dental protrusion patients with conventional methods of anchorage reinforcement in terms of dentoskeletal and soft-tissue changes.
MATERIALS AND METHODS
Search Strategy
An electronic literature search was carried out using PubMed, OVIDSP, the Cochrane Library, CBM, VIP, WanFang Data, and CNKI. Terms used in the search included mini-implant, orthodontic anchorage, and protrusion. In order to improve the search, the Related Articles tool was used in the PubMed search.
Inclusion Criteria
Studies were selected if they satisfied all the following inclusion criteria:
Publication date from December 1966 to March 2016
Original studies based on humans
Randomized controlled trials (RCTs) or clinical controlled trials (CCTs); prospective or retrospective controlled studies
Age of patients over 14 years
Studies conducted on patients with maxillary or bimaxillary dental protrusion, patients whose orthodontic treatment called for extraction of maxillary or bimaxillary premolars, and maximum anchorage during anterior segment retraction
The experimental group and control group used mini-implants and conventional anchorage as anchorage reinforcement
Mini-implants were screwed into the buccal alveolar bone between the maxillary second premolars and first molars
Lateral cephalometric analysis that assessed dental and skeletal movements
Exclusion Criteria
Trials evaluating only the effects of implant or conventional anchorage
Studies exploring measurement methods
Studies concerning other anchorage situations, such as molar distalization
Case reports, reviews, or letters
Data Extraction and Quality Analysis
Data were extracted and recorded independently by two reviewers, and in duplicate using a customized data collection form, on the following items: author and year of publication, study design, number, gender, type of malocclusion, anchorage devices, and reported outcomes.
A quality evaluation of the methodological soundness of RCT articles was performed according to the standards described in the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0).9 Meanwhile, a quality score was calculated by a modified version of the method described by Jadad.10 Otherwise, a methodological quality assessment of the methodological soundness and quality score of CCT articles was performed according to the standards described in the Cochrane Handbook.9 The methods and results sections of each article were read and scored by two independent, blind readers. The evaluators discussed their findings, and when disagreement occurred, it was resolved through further discussion and rereading.
Data Analysis
In this systematic review, evaluation of anchorage effects mainly includes eight aspects, as follows:
maxillary incisor retraction
maxillary molar movement
axial inclination of the maxillary central incisor to the SN plane (U1-SN)
angle between the SN plane and the NA plane (SNA)
inclination of the mandibular plane to the cranial base (SN-MP)
upper lip to E-plane (UL-E pane, mm)
nasolabial angle (NLA)
facial convexity (G-Sn-Pg)
Original outcome data, if possible, underwent statistical pooling through fixed or random effects models by using Review Manager 5.3. Statistical analysis was assessed by a statistician, especially regarding the choice between fixed and random-effect models.11
RESULTS
Description of Studies
Finally, we selected 14 studies,1,4,12–23 including 8 RCTs1,12–18 and 6 CCTs.4,19–23 Summary details of included studies are given in Table 1. Flow of the selection process is demonstrated in Figure 1.
Table 1.
Characteristics of Included Studies
|
Study ID: Author and Year |
Design Study |
Interventions |
Malocclusion |
Loading Force |
Rate of Mini-implant (%) |
|
|
Mini-implant Anchorage |
Traditional Anchorage |
|||||
| Yu et al. 2011 12 | RCT | Maxillary mini-implant (n = 16) | Headgear (n = 16) | Class I or II | 100–150 g | 100 |
| Huang et al. 200713 | RCT | Maxillary mini-implant (n = 10) | Headgear (n = 10) | Class I | 150 g | 100 |
| Wei et al. 2011 14 | RCT | Maxillary mini-implant (n = 10) | Headgear (n = 10) | Class I or II | 1.96 N | 90 |
| Su et al. 2009 15 | RCT | Maxillary mini-implant (n = 15) | Headgear (n = 15) | Class I or II | 100−150 g | 80 |
| Upadhyay et al. 2008 1 | RCT | Maxillary and mandibular mini- implant (n = 20) | Headgear or TPAa (n = 20) | Class I | 150 g | 90 |
| Al-Sibaie et al. 201416 | RCT | Maxillary mini-implant (n = 28) | TPA (n = 28) | Class II Division 1 | 150 g | 100 |
| Liu et al. 2009 17 | RCT | Maxillary mini-implant (n = 17) | TPA (n = 17) | Class I or II | – | – |
| Ma et al. 2008 18 | RCT | Maxillary and mandibular mini- implant (n = 15) | Headgear (n = 15) | Class I or II | 100 g | – |
| Park et al. 2008 19 | CCT | Maxillary and mandibular mini- implant (n = 16) | Headgear (n = 14) | Class I or II | 150-200 g | 100 |
| Upadhyay et al. 2008 4 | CCT | Maxillary and mandibular mini- implant (n = 15) | Choose to use as needed (n = 15) | Class I or II | 150 g | 100 |
| Yao et al. 2008 20 | CCT | Maxillary mini-implant (n = 25) | Headgear plus TPA (n = 22) | Class I or II | – | 100 |
| Chen et al. 2015 21 | CCT | Maxillary mini-implant (n = 15) | Headgear (n = 16) | Class I or II | – | – |
| Koyama et al. 2011 22 | CCT | Maxillary mini-implant (n = 14) | Headgear (n = 14) | Class I | 200 g | – |
| Kuroda et al. 2009 23 | CCT | Maxillary mini-implant (n = 11) | Headgear plus TPA (n = 11) | Class II Division 1 | 100 g | 80–95 |
TPA indicates transpalatal arch.
Figure 1.

Flow chart summarizing literature search.
Methodological Quality of Included Studies
Of the 14 included studies, the 8 RCTs1,12–18 were of high quality, and the 6 CCTs4,19–23 were grade B (quality score, 6–9). The methodological quality for RCT and CCT trials are presented in Tables 2 and 3, respectively.
Table 2.
Methodological Qualitya of Selected RCT Trials
|
Study |
Random Sequence Generation |
Allocation Concealment |
Blinding |
Incomplete Outcome Date |
Selective Reporting |
Other Bias |
Jadad Score |
Quality |
| Yu et al. 2011 12 | Yes | Unclear | Unclear | Yes | Yes | Yes | 4 | High |
| Huang et al. 200713 | Yes | Unclear | Unclear | Yes | Yes | Yes | 4 | High |
| Wei et al. 2011 14 | Yes | Unclear | Unclear | Yes | Yes | Yes | 4 | High |
| Su et al. 2009 15 | Yes | Unclear | Unclear | Yes | Yes | Yes | 5 | High |
| Upadhyay et al. 2008 1 | Yes | Yes | Unclear | Yes | Yes | Yes | 5 | High |
| Al-Sibaie et al. 201416 | Yes | Yes | Unclear | Yes | Yes | Yes | 4 | High |
| Liu et al. 2009 17 | Yes | Unclear | Unclear | Yes | Yes | Yes | 4 | High |
| Ma et al. 2008 18 | Yes | Unclear | Unclear | Yes | Yes | Yes | 4 | High |
Quality was categorized as low (1–3 Jadad scores) or high (4–7 Jadad scores).
Table 3.
Methodological Qualitya of Selected CCT Trials
|
Study |
Diagnostic Criteria |
Grouping Method |
Blinding |
Baseline Consistency |
Confounder Control |
Lost to Treatment |
Score |
Grade |
| Park et al. 2008 19 | Clinical diagnosis | Not mentioned | Not mentioned | Good | Better | No | 6 | B |
| Upadhyay et al. 2008 4 | Clinical diagnosis | Not mentioned | Not mentioned | Better | Better | No | 8 | B |
| Yao et al. 2008 20 | Clinical diagnosis | Not mentioned | Not mentioned | Better | Better | No | 7 | B |
| Chen et al. 2015 21 | Clinical diagnosis | Not mentioned | Not mentioned | Better | Good | No | 6 | B |
| Koyama et al. 2011 22 | Clinical diagnosis | Not mentioned | Not mentioned | Better | Better | No | 7 | B |
| Kuroda et al. 2009 23 | Clinical diagnosis | Not mentioned | Not mentioned | Better | Better | No | 6 | B |
Quality was categorized as grade A (10–12 score), B (6–9 score), or C (0–5 score).
Effects of Interventions
The cephalometric variables investigated in this review are shown in Table 4.
Table 4.
Cephalometric Variables Investigated in This Review
|
Measurements |
WMD (95% CI) |
P value |
| SNA (°) | −0.03 (−0.19, 0.13) | .71 |
| SN-MP (°) | −1.12 (−2.21, −0.03) | .04* |
| Maxillary incisor retraction (mm) | −1.50 (−1.84, −1.17) | .00* |
| Maxillary molar movement (mm) | −2.01 (−2.45, −1.58) | .00* |
| U1-SN (°) | 0.61 (−0.84, 2.05) | .41 |
| UL-E plane (mm) | −0.73 (−1.17, 0.28) | .001* |
| NLA (°) | 3.52 (1.17, 5.87) | .003* |
| G-Sn-Pg (°) | −0.77 (−1.55, −0.02) | .06 |
P <.05.
Skeletal Effects
SNA.
Eleven articles1,12,15–23 reported the SNA. A forest plot is demonstrated in Figure 2, showing that there was no significant difference between the mini-implant and the traditional anchorage technique (P = .71) and that the weighted mean difference (WMD) 95% confidence interval (95% CI) was −0.03° (−0.19°, 0.13°).
Figure 2.
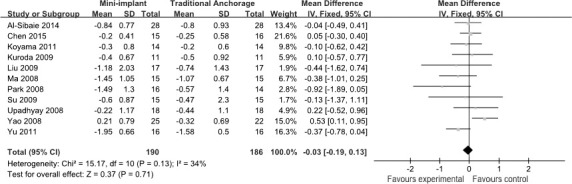
Meta-analysis of SNA.
SN-MP.
Six studies1,16,17,20–22 investigated this outcome. Because of existing heterogeneity, a random-effect model was adopted. As presented in Figure 3, the WMD (95% CI) between the two groups was −1.12° (−2.21°, −0.03°), with a significant difference (P = .04).
Figure 3.
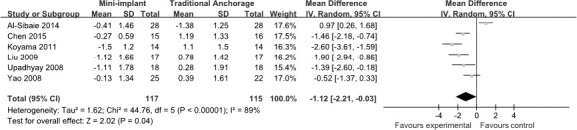
Meta-analysis of SN-MP.
Dental Effects
Maxillary incisor retraction.
Thirteen articles1,4,13–23 were categorized into this study. The forest plot is shown in Figure 4. The WMD (95% CI) was −1.50 mm (−1.84 mm, −1.17 mm), with a significant difference between the two groups (P < .00001).
Figure 4.
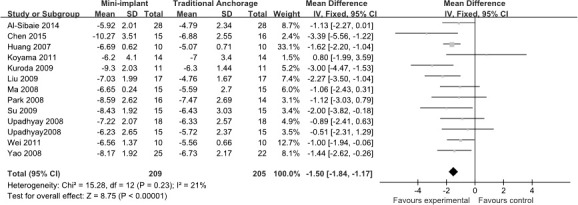
Meta-analysis of maxillary incisor retraction.
Maxillary molar movement.
Thirteen articles1,4,12–17,19–23 were categorized into this study. A meta-analysis was done (Figure 5). Because of existing heterogeneity (I2 = 80%), a random-effect model was adopted. The WMD (95% CI) between the mini-implant and traditional anchorage was −2.01 mm (−2.45 mm, −1.58 mm), and there was a significant difference between the two groups (P < .00001).
Figure 5.
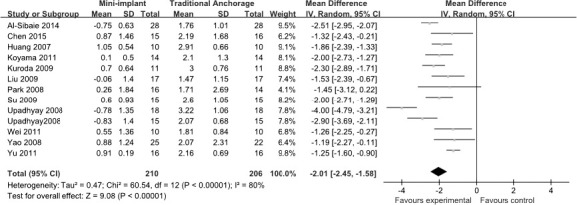
Meta-analysis of maxillary molar movement.
U1-SN.
Twelve articles1,4,12–14,16–22 reported U1-SN. A forest plot is demonstrated in Figure 6. Results of the meta-analysis show significant heterogeneity among these 12 trials (I2 = 76%), so a random-effect model was adopted. As shown in Figure 6, the WMD (95% CI) was 0.61° (−0.84°, 2.05°), and results from the two groups showed no statistical significance (P = .41).
Figure 6.
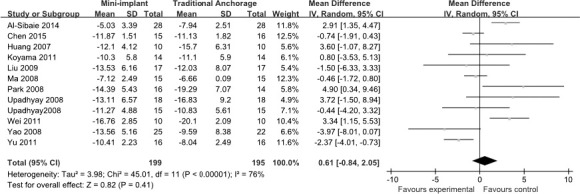
Meta-analysis of U1-SN.
Soft Tissue Effects
UL-E plane (mm).
Five articles1,16,17,19,23 were categorized into this study. A meta-analysis was done; the forest plot is shown in Figure 7. It indicates that there was a significant difference between the mini-implant and the traditional anchorage technique on the UL-E plane (P = .001); the WMD (95% CI) was −0.73 mm (−1.17 mm, 0.28 mm).
Figure 7.
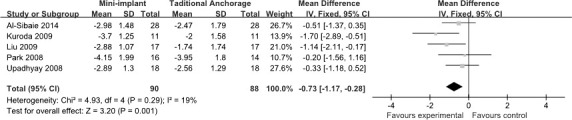
Meta-analysis of UL-E plane.
NLA. Four articles1,16,17,23 reported the nasolabial angle. A forest plot is demonstrated in Figure 8. Heterogeneity was detected, so a random-effect model was adopted. The meta-analysis indicates that there was a significant difference between the mini-implant and traditional anchorage technique (P = .003); the WMD (95% CI) was 3.52° (1.17°, 5.87°).
Figure 8.

Meta-analysis of NLA.
G-Sn-Pg.
Three articles1,17,23 were categorized into this study. The meta-analysis is shown in Figure 9. The result was that the WMD (95% CI) between the two groups was −0.77° (−1.55°, −0.02°), and there was no statistical significance (P = .06).
Figure 9.

Meta-analysis of G-Sn-Pg.
DISCUSSION
Skeletal Effects of Intervention
SNA.
Results showed that both groups underwent decreases in SNA. This indicates that point A moved back during retraction of the maxillary incisor. Moreover, the meta-analysis showed that there was no significant difference. Therefore, both anchorage methods produced significant basal bone changes.
SN-MP.
Results showed that there was a significant difference between the two groups, the WMD (95% CI) was −1.12° (−2.21°, −0.03°), although it could not be considered clinically significant. We cannot suggest that mini-implant anchorage would be more effective than the traditional anchorage technique for high-angle patients.
Dental Effects of Intervention
Maxillary incisor retraction.
The WMD (95% CI) between the two groups regarding accumulative distance moved was −1.50 mm (−1.84 mm, −1.17 mm), with a significant difference, namely, that more maxillary incisor retraction occurred in the mini-implant group than in the traditional anchorage group.
Maxillary molar movement.
Results showed that there was a significant difference between the two groups, namely, that the mini-implant group experienced less movement of the maxillary molars and less anchorage loss compared with the traditional anchorage group; the WMD (95% CI) being −2.01 mm (−2.45 mm, −1.58 mm). Maxillary molar movement was also an important factor in the treatment quality of the maxillary dental protrusion patients. In the clinical situation, 1 mm of maxillary molar distal movement has a negative effect on treatment. Therefore, we suggest the use of the much stronger anchorage capacity of mini-implants.
U1-SN.
The result of meta-analysis showed that the WMD (95% CI) between the two groups was 0.61° (−0.84°, 2.05°), but there was no statistical significance in U1-SN.
Soft Tissue Effects of Intervention
UL-E plane (mm).
The results showed that there was a significant difference between the two groups. However, soft tissue changes are affected by many factors. Oliver24 found that patients with a high lip or thin-lip strain exhibited a significant correlation between incisor retraction and lip retraction, but those having a low lip or a thick-lip strain showed no such correlation. Therefore, in clinical practice, to predict lip morphology, orthodontists need to consider not only the inclination of the maxillary incisors, but also the lip muscle structure and other factors.
NLA.
Results of the meta-analysis showed a statistically significant difference between the two groups. However, in view of the small number of high-quality studies, we cannot determine whether the mini-implant is more effective than traditional anchorage in reducing NLA.
G-Sn-Pg.
Only three studies were included in this systematic review. Kuroda et al.23 showed that facial convexity was significantly improved in both groups, but there was no statistical significance. However, Upadhyay et al.1 revealed that there was a greater change in the soft tissue profile in the mini-implant anchorage group, with statistical significance. In the third study,17 mini-implant anchorage produced greater improvement than did traditional anchorage, with no significant difference. Therefore, because of unreliable methodology and results, we cannot determine the effectiveness of mini-implant vs traditional anchorage technique. To investigate the effect of the two anchorage types, more RCTs are needed.
Meta-analysis Limitations
This meta-analysis may have some limitations. First, the included studies have a risk of bias. The absence of information on method error analysis and blind measurements were examples of failures that may have affected the results across studies. Moreover, baseline differences existed mainly in the types of interventions and outcomes. For instance, most studies reported the amount of maxillary molar movement, but cephalometric measurements were based on different reference planes—the FH plane and the PP plane—resulting in evaluating quality and control of bias of the included eight RCTs1,12–18 as high quality and the six CCTs4,19–23 as grade B (Tables 2 and 3). Otherwise, the internal validity of a meta-analysis can only be as good as the quality of the studies reviewed. Thus, quality-related differences in the treatment effect should be treated as hypothesis-generating observations.
CONCLUSIONS
Mini-implant anchorage was more effect in retracting the anterior teeth and had less anchorage loss.
Both mini-implants and traditional anchorage were equally effective on U1-SN and SNA.
More qualified RCTs are required to make reliable recommendations about the anchorage capacity of mini-implant vs traditional anchorage on patients with maxillary dentoalveolar protrusion, especially in SN-MP and soft tissue effects.
ACKNOWLEDGMENT
Supported by the National Natural Science Foundation of China (81260162).
REFERENCES
- 1.Upadhyay M, Yadav S, Nagaraj K, Patil S. Treatment effects of mini implants for en-masse retraction of anterior teeth in bialveolar dental protrusion patients: a randomized controlled trial. Am J Orthod Dentofacial Orthop. 2008;134:18–29. doi: 10.1016/j.ajodo.2007.03.025. [DOI] [PubMed] [Google Scholar]
- 2.Melsen B, Bosch C. Different approaches to anchorage: a survey and an evaluation. Angle Orthod. 1997;67:23–30. doi: 10.1043/0003-3219(1997)067<0023:DATAAS>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Proffit WR. The second stage of comprehensive treatment: correction of molar relationship and space closure. In: Proffit WR, Fields HW Jr, editors. Contemporary orthodontics. 3rd ed. St. Louis: Mosby-Yearbook; 1997. pp. 573–577. [Google Scholar]
- 4.Upadhyay M, Yadav S, Patil S. Mini-implant anchorage for en-masse retraction of maxillary anterior teeth: a clinical cephalometric study. Am J Orthod Dentofacial Orthop. 2008;134:803–810. doi: 10.1016/j.ajodo.2006.10.025. [DOI] [PubMed] [Google Scholar]
- 5.Costa A, Raffaini M, Melsen B. Miniscrews as orthodontic anchorage: a preliminary report. Int J Adult Orthod Orthognath Surg. 1998;13:201–229. [PubMed] [Google Scholar]
- 6.Pandurangan H. Clinical information in using mini-screws in orthodontics. Int J orthod. 2013;4:19–24. [PubMed] [Google Scholar]
- 7.Lai EH, Yao CC, Chang JZ, Chen I, Chen YJ. Three dimensional dental model analysis of treatment outcomes for protrusive maxillary dentition: comparison of headgear, mini-screw, and miniplate skeletal anchorage. Am J Orthod Dentofacial Orthop. 2008;134:636–645. doi: 10.1016/j.ajodo.2007.05.017. [DOI] [PubMed] [Google Scholar]
- 8.Li F, Hu HK, Chen JW, et al. Comparison of anchorage capacity between implant and headgear during anterior segment retraction. Angle Orthod. 2011;81:915–922. doi: 10.2319/101410-603.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [Updated March 2011]. The Cochrane Collaboration. 2011. Available at: www.cochrane-handbook.org.
- 10.Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled Clin Trials. 1996;17:1–12. doi: 10.1016/0197-2456(95)00134-4. [DOI] [PubMed] [Google Scholar]
- 11.Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to Meta-Analysis. John Wiley Sons. 2009. Chapter 13.
- 12.Yu SD, Hong XC, Yao QH, et al. Clinical comparison between micro-screw implant and headgear used for anchorage control. J Dent Prev Treat. 2011;19(8):414–416. [Google Scholar]
- 13.Huang XF, Han PY. Comparison of clinical effects between screw-implant and extra-force as anchorage. Beijing J Stomatol. 2007;15:213–215. [Google Scholar]
- 14.Wei MG, Lu DZ, Wang GS. Comparison of micro-implant anchorage with headgear anchorage in treatment of maxillary dentoalveolar protrusion. J Tong Ji University. 2011;32:52–56. [Google Scholar]
- 15.Su QZ, Yan Y, Yan HY. Comparison of clinical effects between microscrew implant and headgear in control. Chin J Orthod. 2009;16:140–143. [Google Scholar]
- 16.Al-Sibaie S, Hajeer MY. Randomized controlled trial assessment of changes following en-masse retraction with mini-implants anchorage compared to two-step retraction with conventional anchorage in patients with Class II Division 1 malocclusion: a randomized controlled trial. Eur J Orthod. 2014;36:275–283. doi: 10.1093/ejo/cjt046. [DOI] [PubMed] [Google Scholar]
- 17.Liu YH, Ding WH, Liu J. Comparison of the differences in cephalometric parameters after active orthodontic treatment applying mini-screw implants or transpalatal arches in adult patients with bialveolar dental protrusion. J Oral Rehabil. 2009;36:687–695. doi: 10.1111/j.1365-2842.2009.01976.x. [DOI] [PubMed] [Google Scholar]
- 18.Ma J, Wang L, Zhang W, et al. Comparative evaluation of micro-implant and headgear anchorage used with a pre-adjusted appliance system. Eur J Orthod. 2008;30:283–287. doi: 10.1093/ejo/cjm128. [DOI] [PubMed] [Google Scholar]
- 19.Park HS, Yoon DY, Park CS, et al. Treatment effects and anchorage potential of sliding mechanics with titanium screws compared with the Tweed-Merrifield technique. Am J Orthod Dentofacial Orthop. 2008;133:593–600. doi: 10.1016/j.ajodo.2006.02.041. [DOI] [PubMed] [Google Scholar]
- 20.Yao CC, Lai EH, Chang JZ, et al. Comparison of treatment outcomes between skeletal anchorage and extraoral anchorage in adults with maxillary dentoalveolar protrusion. Am J Orthod Dentofacial Orthop. 2008;134:615–624. doi: 10.1016/j.ajodo.2006.12.022. [DOI] [PubMed] [Google Scholar]
- 21.Chen M, Li Z M, Liu X, et al. Differences of treatment outcomes between self-ligating brackets with microimplant and headgear anchorages in adults with bimaxillary protrusion. Am J Orthod Dentofacial Orthop. 2015;147:465–471. doi: 10.1016/j.ajodo.2014.11.029. [DOI] [PubMed] [Google Scholar]
- 22.Koyama I, Iino S, Abe Y, et al. Difference between sliding mechanics with implant anchorage and straight-pull headgear and intermaxillary elastics in adults with bimaxillary protrusion. Eur J Orthod. 2011;33:126–131. doi: 10.1093/ejo/cjq047. [DOI] [PubMed] [Google Scholar]
- 23.Kuroda S, Yamada K, Deguchi T, et al. Class II malocclusion treated with miniscrew anchorage: comparison with traditional orthodontic mechanics outcomes. Am J Orthod Dentofacial Orthop. 2009;135:302–309. doi: 10.1016/j.ajodo.2007.03.038. [DOI] [PubMed] [Google Scholar]
- 24.Oliver BM. The influence of lip thickness and strain on upper lip response to incisor retraction. Am J Orthod. 1982;82:141–149. doi: 10.1016/0002-9416(82)90492-4. [DOI] [PubMed] [Google Scholar]