

Abstract
Study Design:
This is a correlation study.
Objective:
The objective was to obtain normative values from modified Hertel exophthalmometer, to compare difference in values between modified and standard Hertel exophthalmometer and to statistically analyze for correlation.
Methods:
The study to validate the modification done to Hertel exophthalmometer was performed at the Department of Oral and Maxillofacial Surgery at our institute. Informed consent was obtained from patients; measurement in 100 volunteers was made with Hertel and modified Hertel exophthalmometer by a single observer, and the measurements taken by the 2 devices were tabulated along with variables such as age and gender. Data were collected and statistical analysis was performed to compare and correlate the values between standard and modified exophthalmometer. Differences of ocular protrusion values in gender and age were also calculated.
Results:
There has been no statistically significant difference in the normative data between standard Hertel and modified Hertel exophthalmometer and in relation to age and gender.
Conclusions:
The modification of the Hertel exophthalmometer is validated and can also be used for relative exophthalmometry to assess the need for treatment and to evaluate the globe position and orbital volume intraoperatively. The proposed modification of the instrument allows it to be used in cases when one of the lateral orbital walls is fractured or displaced due to trauma.
Keywords: exophthalmometry, Hertel exophthalmometer
Introduction
Ocular protrusion measurement is usually done in ophthalmology or endocrinology, for diagnosis of orbital diseases.1 Differences in degree of ocular protrusion manifest as exophthalmos or enophthalmos. In maxillofacial surgery, studies have shown that ocular protrusion measurement is an important aspect in planning of exophthalmos or enophthalmos correction, arising primarily or secondarily from trauma or in syndromes.
Exophthalmometry has been used as a tool for measurement of corneal position in relation to the bony orbit. Over the years, there have been many devices that were developed for measuring ocular protrusion. It started with the design of an instrument to measure ocular protrusion by Cohn2 and many exophthalmometers were devised following his invention. Each tried to overcome the drawbacks of the other. Hertel had introduced his device in 1905 which was considered to be an exophthalmometer that produced reliable and reproducible results.3 As with any other exophthalmometer, this device had also many drawbacks and was modified by many to suit their purposes and overcome the shortcomings.
One of the drawback of the instrument was that the readings in Hertel exophthalmometer (Figure 1) may vary if too much pressure was applied on the orbital rims while seating of the footplates, parallax errors may arise, the instrument relied on intact orbital rims for its placement and rotation of the instrument can occur at the horizontal axis.4
Figure 1.

Hertel exophthalmometer.
The zygomatic bone being a part of the lateral wall of orbit causes changes in the orbital volume when displaced by a fracture. One of the accepted ways to ensure adequate reduction of the complex zygomatic bone is restoration of orbital volume. It has been agreed by Choi et al that post-traumatic enophthalmos is increased in proportion to the orbital volume.5 Enophthalmos occurs with an increase in volume of the bony orbit with consequent posterior displacement of the globe.5 An increase in orbital volume is noted in orbital wall fractures which can manifest as enophthalmos. Moreover, most studies have presented that an enophthalmos of greater than 2 mm is an indication for orbital wall surgery.6 Secondary post-traumatic deformities of orbit are difficult to correct than those corrected primarily.7 Hence, this situation warrants an adequate and proper assessment of intraoperative reduction of zygomatic complex fractures.
Modalities of checking adequate reduction of zygomatic and orbital fractures and restoration of orbital volume intraoperatively include the use of ultrasonography (USG), mobile spiral computed tomography (CT), C-arm fluoroscopy, and C-arm cone-beam CT.8 These methods may not be suitable at all times. We thus hypothesized that Hertel instrument may be used for this purpose. But the design of Hertel exophthalmometer is such that it requires to be rested on intact lateral orbital rims and this will not be suitable in zygomatic or orbital fractures. So we modified the Hertel exophthalmometer by adding a 3-dimensional (3D) spirit level, which helped to position the instrument in a reproducible way (Figure 2).
Figure 2.

Modified Hertel exophthalmometer.
Aim
The aim of the study was to validate our modification of Hertel exophthalmometer.
Objectives
The objective was to obtain normative values from modified Hertel exophthalmometer, to compare difference in values between modified and standard Hertel exophthalmometer and to statistically analyze for correlation.
Methodology
The study to validate the modification done to Hertel exophthalmometer was performed at the Department of Oral and Maxillofacial Surgery at our institute. The Institutional Ethics Committee permission was obtained for descriptive study on normal individuals. Informed consent was obtained from patients; measurement in 100 volunteers was made with Hertel and modified Hertel exophthalmometer by a single observer, and the measurements taken by the 2 devices were tabulated along with variables such as age and gender. Data collected was statistically analysed to compare and correlate the values between standard and modified exophthalmometer. Differences of ocular protrusion values in gender and age were also calculated.
Inclusion Criteria
The inclusion criteria includes patients of age 18 to 50 years, willing to participate in the study.
Exclusion Criteria
Patients with ptosis/pseudoptosis, periorbital edema, inability to open eye, craniofacial syndrome, orbital trauma, and refractive errors were excluded from the study.
Plan for Statistics
The analysis was performed using SPSS version 20. Statistical analyses such as analysis of variance (ANOVA) and correlation were performed to compare the differences in standard and modified Hertel instrument.
Instrument Design
In this modification, a 3D spirit level (Figure 3) is mounted in the center of the Hertel exophthalmometer scale. This will help us to parallel the device and provide a stable reference point for the user to measure the corneal projection. The 3D spirit level can be paralleled in anteroposterior, horizontal, and vertical axes. Hence, the level of paralleling of the instrument can be changed according to the patient’s position with the help of the 3D spirit level. In examining a patient sitting in an upright position or in a supine position, the horizontal and anteroposterior axes can be paralleled. Thus, the anteroposterior position of the affected orbit with the opposite rim as landmark was assessed and had overcome the limitation of Hertel usage in lateral orbital rim fractures. Also, this position is reproducible and helps us to obtain repeatable values.
Figure 3.
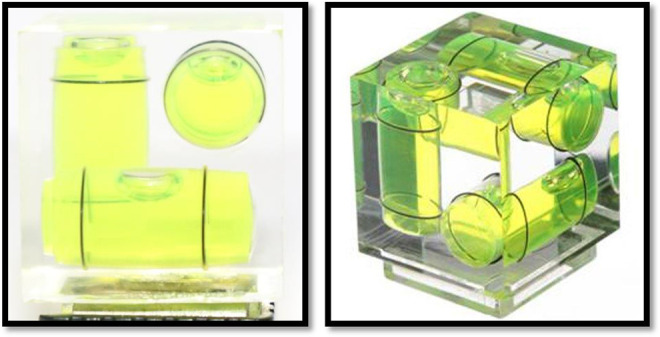
Three-dimensional spirit level.
Measurement of Values
The patient is seated in an upright position on a chair.
Readings with standard Hertel exophthalmometer are taken by resting the instrument on both the lateral orbital rims of the patient and measuring the corneal projection values of the globes, which are reflected in the millimeter scale and are recorded in the case sheet.
To avoid parallax errors, lines on the prism are placed into position by moving the examiner’s viewpoint; they are made to coincide before determining the measurement.
These readings are repeated in the modified instrument on the same patient by paralleling the Hertel exophthalmometer in at least 2 planes (anteroposterior and horizontal) with the aid of the attached spirit level and the readings are recorded.
For the modified Hertel, the footplate is rested on one of the rims and the 3D spirit level is used to make it parallel to the horizontal and anteroposterior plane. This is a highly reproducible position and the readings are done in a similar manner in the other side.
Results
A total of 100 patients were involved in the study. There were 53 female and 47 male. The gender and age distribution is shown in Table 1 and Figure 4.
Table 1.
Descriptive Data: Gender and Age.
| Age | Male | Female | Total |
|---|---|---|---|
| <25 | 8 | 10 | 18 |
| 25-30 | 12 | 14 | 26 |
| 31-35 | 5 | 3 | 8 |
| 36-40 | 6 | 6 | 12 |
| 41-45 | 2 | 6 | 8 |
| 46-50 | 3 | 7 | 10 |
| >50 | 11 | 7 | 18 |
| Total | 47 | 53 | 100 |
Figure 4.

Distribution of age.
The descriptive statistics of the 100 exophthalmometer readings are given in Table 2. The minimum reading observed by both standard Hertel and modified Hertel exophthalmometer was 17 for right and left eyes. The maximum reading observed by both standard Hertel and modified Hertel exophthalmometer was 25 on the right eye and 24 on the left eye in our study. The mean reading of standard Hertel on the right eye is 21.1 ± 1.5. The mean reading of standard Hertel on the left eye is 19.8 ± 1.6. The mean reading of modified Hertel on the right eye is 20.9 ± 1.5. The mean reading of modified Hertel on the left eye is 19.6 ± 1.8.
Table 2.
Descriptive Statistics.
| Exophthalmometer reading | Mean ± standard deviation (in mm) | Minimum (in mm) | Maximum (in mm) | |
|---|---|---|---|---|
| Right eye | Standard Hertel | 21.1 ± 1.5 | 17 | 25 |
| Modified Hertel | 20.9 ± 1.5 | 17 | 25 | |
| Left eye | Standard Hertel | 19.8 ± 1.6 | 17 | 24 |
| Modified Hertel | 19.6 ± 1.8 | 17 | 24 | |
The findings of correlation analysis by Pearson coefficient are presented in Table 3. The correlation coefficient between standard Hertel and modified Hertel exophthalmometer in the right eye is .933 with a value of P < .001. The correlation coefficient between standard Hertel and modified Hertel exophthalmometer in the left eye is .919 with a value of P < .001.
Table 3.
Pearson Correlation Coefficient With Right and Left Eye In Between Standard Hertel Readings and Modified Hertel Readings.
| Correlation | Pearson correlation coefficient | P value |
|---|---|---|
| Between right eye standard and modified Hertel | .933 | <.001 |
| Between left eye standard and modified Hertel | .919 | <.001 |
The scatterplot showing correlation between standard and modified Hertel instrument is presented in Figures 5 and 6.
Figure 5.
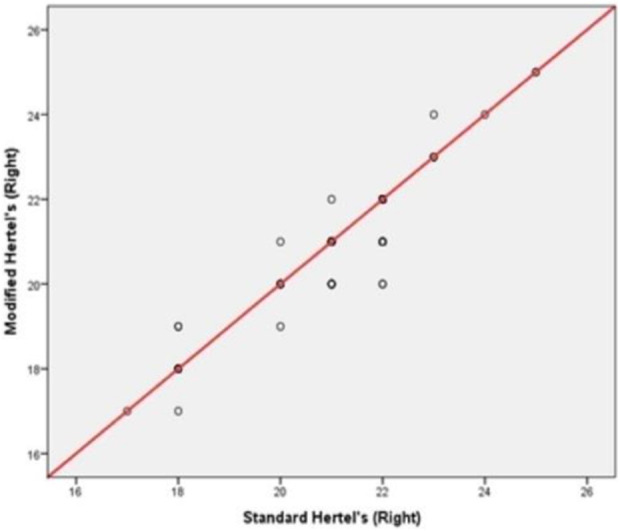
Correlation between standard Hertel readings and modified Hertel readings in the right eye. The correlation between standard and modified Hertel readings in the right eye showed a Pearson coefficient of r = .933.
Figure 6.

Correlation between standard Hertel readings and modified Hertel readings in the left eye. The correlation between standard and modified Hertel readings in the left eye showed a Pearson coefficient of r = .919.
This shows a largely positive correlation between these 2 values. The positive correlation shows that when the values of standard Hertel exophthalmometer increase, the values in modified Hertel exophthalmometer will also increase.
The mean values of each age group in each category are described in Table 4. The mean values obtained in the right eye for our study population was 20.68 for the age group below 30 years, 21.13 for age group from 31 to 50 years, and 21.89 for ages above 50 as measured by Hertel exophthalmometer. The mean values obtained in the left eye for our study population was 19.75 for the age group below 30 years, 19.29 for age group from 31 to 50 years, and 20.89 for ages above 50 as measured by Hertel exophthalmometer. The mean of modified Hertel values obtained in the right eye for patients of age below 30 was 20.50, of age from 31 to 50 was 20.89, and greater than 50 was 21.83. The mean of modified Hertel values obtained in the left eye for patients of age below 30 was 19.45, of age from 31 to 50 was 19.24, and greater than 50 was 20.94.
Table 4.
Mean of Age.
| Instrument | Side | Age category | Mean | SD |
|---|---|---|---|---|
| Hertel values | Right eye | <30 years (n = 44) | 20.68 | 1.736 |
| 31-50 years (n = 38) | 21.13 | 1.018 | ||
| >50 years (n = 18) | 21.89 | 1.231 | ||
| Left eye | <30 years (n = 44) | 19.75 | 1.527 | |
| 31-50 years (n = 38) | 19.29 | 1.675 | ||
| >50 years (n = 18) | 20.89 | 1.367 | ||
| Modified Hertel values | Right eye | <30 years (n = 44) | 20.50 | 1.691 |
| 31-50 years (n = 38) | 20.89 | 1.008 | ||
| >50 years (n = 18) | 21.83 | 1.383 | ||
| Left eye | <30 years (n = 44) | 19.45 | 1.649 | |
| 31-50 years (n = 38) | 19.24 | 1.715 | ||
| >50 years (n = 18) | 20.94 | 1.626 |
Abbreviation: SD, standard deviation.
One-way ANOVA test was performed to check the correlation between exophthalmometry values and age of both exophthalmometers. The F and P values for Hertel right eye was 4.719 and .011 and for left eye was 6.440 and .002, respectively. The F and P values for modified Hertel right eye was 5.705 and .005 and for left eye was 6.865 and .002, respectively (Table 5). The table shows an increase in exophthalmometric values with age which is statistically significant.
Table 5.
One-Way ANOVA Test for Correlation With Age.
| One-way ANOVA test | Sum of squares | df | Mean square | F | Sig. | ||
|---|---|---|---|---|---|---|---|
| Hertel | Right eye | Between groups | 18.845 | 2 | 9.422 | 4.719 | .011 |
| Within groups | 193.665 | 97 | 1.997 | ||||
| Total | 212.510 | 99 | |||||
| Left eye | Between groups | 31.316 | 2 | 15.658 | 6.440 | .002 | |
| Within groups | 235.844 | 97 | 2.431 | ||||
| Total | 267.160 | 99 | |||||
| Modified Hertel | Right eye | Between groups | 22.711 | 2 | 11.356 | 5.705 | .005 |
| Within groups | 193.079 | 97 | 1.991 | ||||
| Total | 215.790 | 99 | |||||
| Left eye | Between groups | 38.318 | 2 | 19.159 | 6.865 | .002 | |
| Within groups | 270.722 | 97 | 2.791 | ||||
| Total | 309.040 | 99 | |||||
Abbreviation: ANOVA, analysis of variance.
The Hertel and modified Hertel instrument readings correlated positively as an increase in age for right eye Hertel with a Pearson correlation coefficient of .271 (P = .006), for left eye with a Pearson correlation coefficient of .211 (P = .036), for right eye modified Hertel with a Pearson correlation coefficient of .301 (P = .002) and left eye modified Hertel with a Pearson correlation coefficient of .265 (P = .008). There has been an increase in exophthalmometry values with age in Hertel and modified Hertel exophthalmometer. Both Hertel readings and modified Hertel readings are positively correlated with age and all these correlations are statistically significant (Table 6).
Table 6.
Pearson Correlation Coefficient With Age.
| Instrument | Side | Pearson correlation coefficient | P value |
|---|---|---|---|
| Hertel | Right eye | .271 | .006 |
| Left eye | .211 | .036 | |
| Modified HERTEL | Right eye | .301 | .002 |
| Left eye | .265 | .008 |
The mean values between male and female were also calculated in the study. It was found that the mean of Hertel exophthalmometer value in our study population in male was 21.3 ± 1.3 mm for the right eye and 19.9 ± 1.6 mm for the left eye. In female, it was 20.9 ± 1.6 mm for the right eye and 19.8±1.7 mm for the left eye. In modified Hertel exophthalmometer, the mean value of ocular protrusion in male was 21.0 ± 1.4 mm for the right eye and 19.6 ± 1.7 mm for the left eye. In female, it was 20.8 ± 1.5 mm for the left eye and 19.7 ± 1.8 mm for the right eye (Table 7). There was no statistically significant difference in the values of male and female in both modified and standard Hertel exophthalmometer.
Table 7.
Mean of Gender.
| Instrument | Side | Gender | Mean ± SD | Mean difference | T statistics | P value |
|---|---|---|---|---|---|---|
| Hertel | Right eye | Male | 21.3 ± 1.3 | 0.43 | 1.473 | .144 |
| Female | 20.9 ± 1.6 | |||||
| Left eye | Male | 19.9 ± 1.6 | 0.17 | 0.527 | .599 | |
| Female | 19.8 ± 1.7 | |||||
| Modified Hertel | Right eye | Male | 21.0 ± 1.4 | 0.29 | 0.973 | .333 |
| Female | 20.8 ± 1.5 | |||||
| Left eye | Male | 19.6 ± 1.7 | 0.12 | −0.348 | .729 | |
| Female | 19.7 ± 1.8 |
Abbreviation: SD, standard deviation.
Discussion
Birch-Hirschfield defines absolute exophthalmos as “the difference between the level of the cornea and a point on the orbital rim.”9 Enophthalmos is defined as retrodisplacement of globe within the bony confines of the orbit.10
The Hertel exophthalmometer is the most widely used instrument for the measurement of globe position and is a reliable method for measuring the ocular protrusion.3 Hertel exophthalmometer involves measuring the distance between the corneal apex and lateral orbital rim and noting the position of this alignment on the millimeter scale. The measurement obtained on the scale can be taken as the ex- or enophthalmos. Relative exophthalmometry can also be done by using Hertel exopthalmometer.11
But there are 3 major disadvantages of the Hertel instrument as described by Ameri and Fenton:
The resting of the footplate on the lateral orbital rim may be unreliable if too much pressure is applied or if the instrument is not placed properly.
There can be possible rotation of the instrument at the horizontal plane.
Since it has 2 prisms that reflects the cornea, there can be parallax error while the measurement is recorded.4
Also, the application of the Hertel exophthalmometer mainly relied on orbital rims that were intact. Following the development of Hertel exophthalmometer, many people had attempted to modify his instrument to suit various applications and purposes.
The exophthalmometer has found its use in oral and maxillofacial surgery as an instrument to measure restoration of orbital volume, which indirectly results in adequate reduction of zygomatic fractures and prevents postoperative complications like enophthalmos.
Yeatts et al in the year 1992 modified the Hertel exophthalmometer by using the external auditory canal as a reference point in case of fractured orbital rims. They showed no statistical difference between the 2 methods.12
Kratky and Hurwitz in the year 1993 developed a fixation adapter that attaches to a standard Hertel instrument and transfers fixation to the forehead and nasion from the lateral orbit. As concluded by this study, the new fixation adapter applied to the Hertel instrument may be useful in assessing trauma and surgical cases where the lateral orbital rim has been damaged.13
The purpose of our study was to validate the modified instrument to measure adequate restoration of orbital volume after reduction of zygomatic fractures. It has been already agreed that Hertel exophthalmometer is a reliable method for measuring orbital volume.3 The anteroposterior displacement caused by orbital trauma can be assessed by Hertel exophthalmometer. The drawback of this instrument that prevented us from using in zygomatic fractures is that it used the lateral orbital rims as a stable point. The lateral orbital rim was often displaced in fractures of zygoma and orbit. The challenge was to modify the instrument to create a stable reference point using the unaffected lateral orbital rim. The solution was in the form of a 3D spirit level incorporated in the horizontal beam of the Hertel instrument. This 3D spirit level allows repeated positioning of the instrument by placing the footplate on the unaffected side and paralleling the spirit level in the X (horizontal) and Y (anteroposterior) axes (Figure 7). Validation of the modified Hertel instrument was done in normal individuals is essential for future use in ensuring adequate reduction in zygomatic fractures, which was done in our study.
Figure 7.

Positioning the modified Hertel exophthalmometer on an individual.
An increase in orbital volume is noted in orbital wall fractures which can manifest as enophthalmos.14 Significant correlation was observed between the degree of enophthalmos and the volume of herniated orbital contents.15 The mechanism for traumatic enophthalmos can be due to enlargement of the bony orbit due to bone loss, loss of ligament support (Lockwood’s ligament), post-traumatic fat atrophy, fat displacement, fat contracture, or neurogenic causes.16 Enophthalmos usually correlates with orbital volume and height of retrobulbar portion of orbit.17 Post-traumatic enophthalmos is increased in proportion to the orbital volume.15
According to a study by Nasir et al, the most important factor to predict a post-traumatic enophthalmos in the acute phase was the fracture size. It is 3 times more likely to be observed in pure orbital blowout fracture in patients with a floor defect size of more than 150 mm2.18 Preoperative measurements of orbital volume can be used as quantitative values to predict the final degree of enophthalmos in pure blowout fractures.5
Any abnormal relationship between the globe and bony orbit can manifest clinically as exophthalmos or enophthalmos.19 Displacement of one or more walls of orbit by fracture causes change in orbital volume. For 3 mm of displacement of either the inferior or medial wall, orbital volume will change from 7% to 12%.20 Studies reveal that area of fractures greater than 1.9 cm2 and volume of herniated tissue more than 0.9 ml causes a change in the degree of enophthalmos. Enophthalmos becomes clinically evident when the relative exophthalmometric value of affected side lies between 3 mm and 4 mm or more.21 Late enophthalmos of 2 to 3 mm caused by an unrepaired zygomatic or orbital blowout fracture can cause aesthetic and functional impairment.22 A difference of at least 3 to 4 mm in exophthalmometric measurements is necessary to establish pathology.23 Usually, 2 mm of enophthalmos corresponds to a bone defect area of approximately 2.75 cm2 in patients with medial orbital wall fracture.24
A perfect secondary correction of enophthalmos is not easily achieved.25 The outcome is better when appropriate fracture reduction and fixation occurs at the first surgery.26 The results that are obtained after secondary deformity correction are never as good as obtained in primary repair.7 Enophthalmos can be reversed by early or late bone reconstruction which restore the position and shape of the orbital soft tissue by correcting the volume and shape of the bony orbit.16 The objective of surgery for correction of enophthalmos in patients with a volume discrepancy should be to decrease the volume of the bony orbit and to increase the anterior projection of the globe.6 This can be achieved if intraoperative assessment of globe projection is done after reduction of fractures.
There is no simple and reliable method to assess proper reduction of zygomatic fractures. Various methods like USG,27 CT,28 and C-arm29 had been used in attempt to check proper reduction and restoration of orbital volume. But there are practical difficulties in these methods. Ramli et al found that measurement taken in CT and Hertel exophthalmometry should not be used interchangeably as it will lead to errors in clinical interpretation. Proptosis measures show a lower value in CT scans than in exophthalmometers.28 Ocular protrusion values of CT scan showed only intermediate accuracy with the Hertel exophthalmometer.30 Nkenke et al did a study on differences in globe position using Hertel exophthalmometry, optical 3D imaging, and CT.11 They found that Hertel exophthalmometry can lead to errors in reading when surrounding soft tissue edema or displaced lateral rims is present. Our modification can overcome this issue as the footplate lies only on the unaffected rim.
Normative data in standard and in modified Hertel exophthalmometer in normal individuals were obtained in our study, and values between the 2 instruments were compared. Included in the study were normal adult individuals of age 18 to 50 without any obvious pathology. Children were also excluded from the study as there seems to be an increase in Hertel value in adults as compared to children.31 Hyperopic individuals were also excluded as it was found that people with refractive errors may have a false increase in values.32
There is a possibility of parallax errors while measuring in Hertel exophthalmometer as it is a 2-mirror instrument. By aligning the reference line properly with no-parallax-alignment-line given in the reflecting side, this problem can be avoided. The patient should be consistently positioned as far from the reflecting surface of the instrument as possible. These measures were described by Frueh in 2007 and were employed in our study.33 The same instrument was used in this study to avoid inter-instrument bias.34
Correlation of age and gender of the patients with exophthalmometry values of standard Hertel and modified exophthalmometer was also done in our study. There was a significant difference, an increasing trend of exophthalmometric values between younger and older adults showing a positive correlation. This was found to be in accordance with many studies.31,35 Hertel exophthalmometry values of 20.5 to 21 mm can be pathological if there is no excessive myopia.31 He also added that whenever there is a suspicion of exophthalmos, many factors must be taken into consideration, such as history, race, sex, age, physical type, stature, state of nutrition, cranial form or refraction before establishing diagnosis.36,37
In a study to determine normative exophthalmometric data in white and black adults, it was found that the normal protrusion in white men was 16.5 mm, white women was 15.4 mm, black men was 18.5 mm, and black women was 17.8.38 In another study, the mean protrusion value for black men and women was found to be 24.12 and 22.74, respectively.32 In our study, for modified Hertel exophthalmometer, the mean value of ocular protrusion in male was 21.0 ± 1.4 mm for the right eye and 19.6 ± 1.7 mm for the left eye. In female, it was 20.8 ± 1.5 mm for the left eye and 19.7 ± 1.8 mm for the right eye (P > .05). There was no statistically significant difference in gender as obtained in our study as proved by many other studies in the literature.35,37
Another aspect that should have been dealt with in this study is inter- and intra-observer variance and reliability. Various studies have shown with the Hertel exophthalmometer there is some unavoidable and negligible inter- and intra-observer variance in readings done with the Hertel exophthalmometer.3,39,40,41 This was not done in this study to exclude chances of confusion and risk of false values during statistical analysis. However, we plan to implement this topic exclusively in another study.
By comparing these parameters, we could prove that there has been no statistically significant difference in the normative data between standard Hertel and modified Hertel exophthalmometer. Hence, our instrument can be used in cases of zygomatic fractures for assessment of pre- and postoperative ocular protrusion values, intraoperative assessment for orbital volume restoration after reduction.
Conclusion
Therefore, the modification of the Hertel exophthalmometer is validated and can also be used for relative exophthalmometry to assess the need for treatment and to evaluate the globe position and orbital volume intraoperatively. The proposed modification of the instrument allows it to be used in cases when one of the lateral orbital walls is fractured or displaced due to trauma.
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iD: Rizwana Fathima Jamal, MDS  https://orcid.org/0000-0002-1786-7968
https://orcid.org/0000-0002-1786-7968
References
- 1.Foster OA. Differential diagnosis of the causes of exophthalmos. Br J Ophthalmol. 1938;22(6):364–375.18169543 [Google Scholar]
- 2.Cohn HL. Messungen Der Prominenz Der AugenmittelsteinesneuenInstrumentes Des Exophtalmometers. 1868. [Google Scholar]
- 3.Kashkouli MB, Beigi B, Noorani MM, Nojoomi M. Hertel exophthalmometry: reliability and interobserver variation. Orbit. 2003;22(4):239–245. [DOI] [PubMed] [Google Scholar]
- 4.Ameri H, Fenton S. Comparison of unilateral and simultaneous bilateral measurement of the globe position, using the Hertel exophthalmometer. Ophthalmic Plast Reconstr Surg. 2004;20(6):448–451. [DOI] [PubMed] [Google Scholar]
- 5.Choi SH, Kang DH, Gu JH. The correlation between the orbital volume ratio and enophthalmos in unoperated blowout fractures. Arch Plast Surg. 2016;43(6):518–522. doi:10.5999/aps.2016.43.6.518 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Catone GA, Morrissette MP, Carlson ER. A retrospective study of untreated orbital blow-out fractures. J Oral Maxillofac Surg. 1988;46(12):1033–1037. [DOI] [PubMed] [Google Scholar]
- 7.Hammer B, Prein J. Correction of post-traumatic orbital deformities: operative techniques and review of 26 patients. J Craniomaxillofac Surg. 1995;23(2):81–90. [DOI] [PubMed] [Google Scholar]
- 8.Van Hout WM, Van Cann EM, Muradin MS, Frank MH, Koole R. Intraoperative imaging for the repair of zygomaticomaxillary complex fractures: a comprehensive review of the literature. J Craniomaxillofac Surg. 2014;42(8):1918–1923. [DOI] [PubMed] [Google Scholar]
- 9.Drews LC. Exophthalmometry and a new exophthalmometer. Trans Am Ophthalmol Soc. 1956;54(1):215. [PMC free article] [PubMed] [Google Scholar]
- 10.Chane RA, Rootman J. Enophthalmos: a clinical review. Ophthalmology. 1984;91(3):229–237. [DOI] [PubMed] [Google Scholar]
- 11.Nkenke E, Benz M, Maier T, et al. Relative en- and exophthalmometry in zygomatic fractures comparing optical non-contact, non-ionizing 3D imaging to the Hertel instrument and computed tomography. J Craniomaxillofacial Surg. 2003;31(6):362–368. [DOI] [PubMed] [Google Scholar]
- 12.Yeatts RP, van Rens E, Taylor CL. Measurement of globe position in complex orbital fractures. I. A modification of Hertel’s exophthalmometer, using the external auditory canal as a reference point. Ophthalmic Plast Reconstr Surg. 1992;8(2):114–118. [DOI] [PubMed] [Google Scholar]
- 13.Kratky V, Hurwitz JJ. Hertel exophthalmometry without orbital rim contact. Ophthalmology. 1994;101(5):931–937. [DOI] [PubMed] [Google Scholar]
- 14.Stasior OG, Roen JL. Traumatic enophthalmos. Ophthalmology. 1982;89(11):1267–1273. [DOI] [PubMed] [Google Scholar]
- 15.Jin HR, Shin SO, Choo MJ, Choi YS. Relationship between the extent of fracture and the degree of enophthalmos in isolated blowout fractures of the medial orbital wall. J Oral Maxillofac Surg. 2000;58(6):617–620. [DOI] [PubMed] [Google Scholar]
- 16.Manson PN, Grivas A, Rosenbaum A, Vannier M, Zinreich J, Iliff N. Studies on enophthalmos: II. The measurement of orbital injuries and their treatment by quantitative computed tomography. Plast Reconstr Surg. 1986;77(2):203–214. [PubMed] [Google Scholar]
- 17.Ramieri G, Spada MC, Bianchi SD, Berrone S. Dimensions and volumes of the orbit and orbital fat in posttraumatic enophthalmos. Dentomaxillofac Radiol. 2000;29(5):302–311. [DOI] [PubMed] [Google Scholar]
- 18.Nasir SA, Ramli R, Jabar NA. Predictors of enophthalmos among adult patients with pure orbital blowout fractures. PloS One. 2018;13(10):e0204946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Goldberg RA, Relan A, Hoenig J. Relationship of the eye to the bony orbit, with clinical correlations. Aust N Z J Ophthalmol. 1999;27(6):398–403. [DOI] [PubMed] [Google Scholar]
- 20.Parsons GS, Mathog RH. Orbital wall and volume relationships. Arch Otolaryngol Head Neck Surg. 1988;114(7):743–747. [DOI] [PubMed] [Google Scholar]
- 21.Koo L, Hatton MP, Rubin PA. When is enophthalmos “significant”? Ophthalmic Plast Reconstr Surg. 2006;22(1):274–277. [DOI] [PubMed] [Google Scholar]
- 22.Forrest CR. Secondary management of posttraumatic craniofacial deformities. In: Jeffrey W, ed. Plastic Surgery Secrets Plus. 2nd ed. Mosby Elsevier; 2010:330–339. [Google Scholar]
- 23.Bogren HG, Franti CE, Wilmarth SS. Normal variations of the position of the eye in the orbit. Ophthalmology. 1986;93(8):1072–1077. [DOI] [PubMed] [Google Scholar]
- 24.Sung YS, Chung CM, Hong IP. The correlation between the degree of enophthalmos and the extent of fracture in medial orbital wall fracture left untreated for over six months: a retrospective analysis of 81 cases at a single institution. Arch Plast Surg. 2013;40(4):335–340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Clauser L, Galie M, Pagliaro F, Tieghi R. Posttraumatic enophthalmos: etiology, principles of reconstruction, and correction. J Craniofac Surg. 2008;19(2):351–359. [DOI] [PubMed] [Google Scholar]
- 26.Gaziri DA, Omizollo G, Luchi GH, de Oliveira MG, Heitz C. Assessment for treatment of tripod fractures of the zygoma with microcompressive screws. J Oral Maxillofac Surg. 2012;70(6):e378–e388. [DOI] [PubMed] [Google Scholar]
- 27.Ogunmuyiwa SA, Fatusi OA, Ugboko VI, Ayoola OO, Maaji SM. The validity of ultrasonography in the diagnosis of zygomaticomaxillary complex fractures. Int J Oral Maxillofac Surg. 2012;41(4):500–505. [DOI] [PubMed] [Google Scholar]
- 28.Ramli N, Kala S, Samsudin A, Rahmat K, Zainal Abidin Z. Proptosis—correlation and agreement between Hertel exophthalmometry and computed tomography. Orbit. 2015;34(5):257–262. [DOI] [PubMed] [Google Scholar]
- 29.Maheedhar A, Ravindran C, Azariah ED. Use of C-arm to assess reduction of zygomatic complex fractures: a comparative study. Craniomaxillofac Trauma Reconstr. 2017;10(1):35–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Delmas J, Loustau JM, Martin S, Bourmault L, Adenis JP, Robert PY. Comparative study of 3 exophthalmometers and computed tomographic biometry. Eur J Ophthalmol. 2018;28(2):144–149. [DOI] [PubMed] [Google Scholar]
- 31.Dohvoma VA, Epée E, Mvogo SR, Lietcheu NS, Mvogo CE. Correlation between Hertel exophthalmometric value and refraction in young Cameroonian adults aged 20 to 40 years. Clin Ophthalmol. 2016;10:1447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Dunsky IL. Normative data for Hertel exophthalmometry in a normal adult black population. Optom Vis Sci. 1992;69(7):562–564. [DOI] [PubMed] [Google Scholar]
- 33.Frueh WT, Frueh BR. Errors of single-mirror or prism Hertel exophthalmometers and recommendations for minimizing the errors. Ophthalmic Plast Reconstr Surg. 2007;23(3):197–201. [DOI] [PubMed] [Google Scholar]
- 34.Sleep TJ, Manners RM. Interinstrument variability in Hertel-type exophthalmometers. Ophthalmic Plast Reconstr Surg. 2002;18(4):254–257. [DOI] [PubMed] [Google Scholar]
- 35.Kumari Sodhi P, Gupta VP, Pandey RM. Exophthalmometric values in a normal Indian population. Orbit. 2001;20(1):1–9. [DOI] [PubMed] [Google Scholar]
- 36.Knudtzon K. On exophthalmometry: the result of 724 measurements with the Hertel exophthalmometer on normal adult individuals. Acta Psychiatr Scand. 1949;24(3-4):523. [PubMed] [Google Scholar]
- 37.Omer K, Ozlem BS, Karahan E, Mehmet OZ, Murat U. The effect of age, gender, refractive status and axial length on the measurements of Hertel exophthalmometry. Open Ophthalmol J. 2015;9:113–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Migliori ME, Gladstone GJ. Determination of the normal range of exophthalmometric values for black and white adults. Am J Ophthalmol. 1984;98(4):438–442. [DOI] [PubMed] [Google Scholar]
- 39.Lam AK, Lam CF, Leung WK, Hung PK. Intra-observer and inter-observer variation of Hertel exophthalmometry. Ophthalmic Physiol Opt. 2009;29(4):472–476. doi:10.1111/j.1475-1313.2008.00617.x [DOI] [PubMed] [Google Scholar]
- 40.Karwoski BA, Killian FA, Rosenberg C, Glavas YP. Inter-observer variability of Hertel exophthalmometry stratified by training experience. Invest Ophthalmol Vis Sci. 2009;50(13):4038. [Google Scholar]
- 41.Musch DC, Frueh BR, Landis JR. The reliability of Hertel exophthalmometry: observer variation between physician and lay readers. Ophthalmology. 1985;92(9):1177–1180. [DOI] [PubMed] [Google Scholar]