

Abstract
This study aimed to examine in a longitudinal cohort design whether social media use among adolescents is related to symptoms of social anxiety, depressed mood, and physical symptoms of anxiety over time. As part of the LIFECOURSE study of risk and protective factors for healthy adolescent development, three waves of school-based surveys of adolescents born in Iceland in 2004 were analyzed. Of the 3914 eligible adolescents, 2378 gave informed consent. Complete responses for this study were collected from 2211 students at the first wave, with 2052 responding roughly 12 months later, and 2097 responding in year 3. Linear mixed-effects models were used to analyze time spent on social media in relation to psychological distress over time. More time spent on social media was weakly but significantly associated with increased symptoms of depressed mood, social anxiety and symptoms of physical anxiety over time. However, the effect size of these relationships suggest they may not be of clinical relevance. The relationship between time spent on social media and symptoms of depressed mood and physical symptoms of anxiety grew stronger over time, although it is not known if this relationship is causal. The relationship between time spent on social media and all outcomes of psychological distress were stronger for girls than boys and increased social media use had a positive relationship with symptoms of depressed mood over time. The relationships found in this study were relatively small and future studies need to focus on the clinical and public health significance of these effects.
Keywords: Adolescents, symptoms of anxiety, longitudinal studies, social media use, symptoms of depressed mood
1. Introduction
The simultaneous increase in social media use and worsening self-reported mental health among adolescents has motivated researchers to investigate the relationship between social media use and adolescent mental health (Heffer et al. 2019; Jensen et al. 2019; Keles et al. 2019; McCrae et al. 2017; Orben and Przybylski 2019; Riehm et al. 2019; Seabrook et al. 2016; Twenge et al. 2018). As with in-person social interactions, social media experiences can be positive, negative, neutral, or mixed. Positive aspects include connecting with friends, increased social support, and greater levels of self-expression (Anderson and Jiang 2018; Seabrook et al. 2016; Thorisdottir et al. 2019). However, possible negative aspects of social media may include upward social comparisons, cyberbullying, fewer in-person interactions (Anderson and Jiang 2018; Thorisdottir et al. 2019), less family time, and more conflicts with parents (Williams and Merten 2011).
Social media plays a role in adolescent social life and explaining how social media use can possibly influence something as complex as mental health requires a holistic theoretical framework. The transformation framework (Nesi et al. 2018a, 2018b) proposes that the unique context of social media fundamentally transforms adolescents' peer experiences across multiple domains. For example, through what is referred to as asynchronicity or the time that passes between responses in a dialogue online, adolescents can carefully select their words and engage in many conversations at the same time, as well as decide how to present themselves. Furthermore, this ongoing dialogue may contribute to feelings of pressure to be constantly online (Calancie et al. 2017). Peer experiences are prospectively associated with mental health symptoms (Landstedt and Almquist 2019; Modin et al. 2011); thus, understanding whether social media plays a role in adolescent mental health is important.
Some studies have concluded that social media use contributes to lower psychological well-being and increases symptoms of depression, anxiety, and psychological distress among children and adolescents (Keles et al. 2019; McCrae et al. 2017), although the associations are weak. Others maintain that there is little or no relationship between youth social media use and symptoms of depression (Heffer et al. 2019) and psychological distress (Jensen et al. 2019). Several systematic reviews and meta-analysis on the topic have observed contradictory evidence of mixed, null, and positive associations. However, the nature of the relationship between social media use and psychological distress is not clear. This could be due to the high reliance on cross-sectional studies and lack of mediating and moderating variables (Huang 2017; Keles et al. 2019; McCrae et al. 2017; Seabrook et al. 2016). Another potential explanation for the disparate findings is that the concept itself is broad, often vague, and measured differently. Some studies use well-being scales (Booker et al. 2018; Orben et al. 2019), while others use general distress scales (Jensen et al. 2019) or examine symptoms of internalizing problems (Riehm et al. 2019), such as anxiety and depression (Boers et al. 2019; Coyne et al. 2020; Heffer et al. 2019; Vannucci and McCauley Ohannessian 2019).
The few longitudinal studies on the topic have reported mixed findings. Some find that social media use predicts higher depressive symptoms (Boers et al. 2019; Vannucci and McCauley Ohannessian 2019), panic disorder symptoms (Vannucci and McCauley Ohannessian 2019), greater internalizing problems (Boers et al. 2019; Riehm et al. 2019) and worse well-being (Booker et al. 2018). However, others have found that frequency of social media use does not predict later mental health outcomes (Coyne et al. 2020; Jensen et al. 2019).
The role of gender in social media and mental health relationship has also been inconclusive (McCrae et al. 2017). Where there are gender differences, the relationship between social media and worse mental health has either been stronger for girls than boys (Frison and Eggermont 2016; Thorisdottir et al. 2019) or only exist for girls (Devine and Lloyd 2012). A study on the relationship between social media and life satisfaction measured within six domains (i.e., friends, family, appearance, life, school work, and school) found that gender was important; within-person models were significant for two out of six domains for boys and five out of six domains for girls (Orben and Przybylski 2019). However, two longitudinal studies found no gender differences in social media use and internalizing symptoms (Riehm et al. 2019; Vannucci and McCauley Ohannessian 2019). Given these inconsistent findings, some have called for analyses to be stratified by gender or tested for gender interactions (Booker et al. 2018).
This study sought to examine, over a three-year period, the relationships between time spent on social media and symptoms of depressed mood, social anxiety, and physical symptoms of anxiety among Icelandic adolescents. While other studies have typically focused on more general concepts, such as well-being (Booker et al. 2018; Orben et al. 2019) and overall distress (Jensen et al. 2019; Riehm et al. 2019), we specifically examined symptoms of depressed mood, differentiating physical and social symptoms of anxiety (Coyne et al. 2020; Vannucci and McCauley Ohannessian 2019). Our study addresses several shortcomings of previous work. First, because social media is rapidly evolving in the way it alters how adolescents interact with their peers, the recency of our data affords an advantage over older data by providing a current analysis of the relationship between use and mental health over time. Second, given the high prevalence of anxiety among girls in Western economies (Bor et al. 2014), we examined whether gender plays a role in the relationship between social media use and mental health over time. Third, there is a lack of empirical evidence on the effects of social media use on adolescents since the majority of studies have focused on young children or adults (Odgers and Jensen 2020). Finally, because of the compelling evidence showing the deleterious impact of divorce and family disruptions on children and adolescents (Amato 2000; Behere et al. 2017), we controlled for parental support and family structure (Hall-Lande et al. 2007; Stadler et al. 2010). The reason being that adolescent social media use has been associated with less family time and more conflicts with parents (Williams and Merten 2011), as well as children from single-parent households having more screen time daily (Wartella et al. 2013).
We hypothesized that: 1) there is a positive relationship between social media use and symptoms of depressed mood, symptoms of social anxiety and physical symptoms of anxiety; 2) the relationship between social media use and symptoms of depressed mood, symptoms of social anxiety and physical symptoms of anxiety increases over time; and 3) the observed relationships between social media use and symptoms of depressed mood, symptoms of social anxiety and physical symptoms of anxiety will be stronger for girls than boys.
2. Methods
This study was approved by the National Bioethics Committee of Iceland and registered with the Icelandic Data Protection Authority.
3. Sample and participants
Our data come from three waves of school-based surveys from the LIFECOURSE study of risk and protective factors for healthy adolescent development (Sigfusdottir et al. 2017). Fig. 1 shows participant enrollment and participation. In this study, only students that answered a question regarding their gender at baseline were included in the sample, N = 2211. No one withdrew from the study, and those lost at follow up are students that were not present in school on the day of the survey.
Fig. 1.
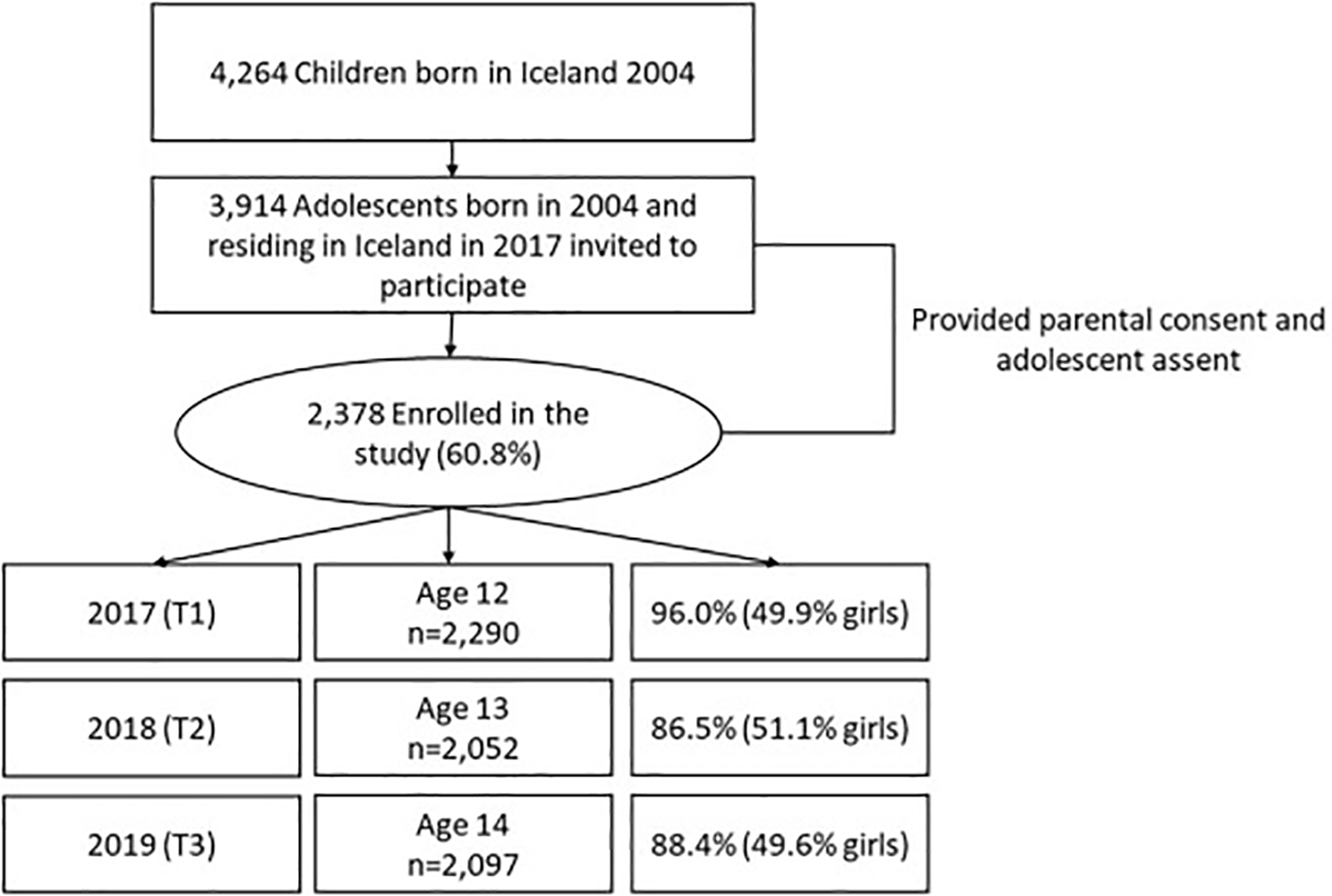
Enrollment, participation and participation rates in the LIFECOURSE study. Of the 3914 eligible adolescents, 60.8% (N = 2378) provided parental consent and adolescent assent, with 2290 responding to the first survey wave when they were 12 years old, with 2052 responding roughly 12 months later when they were 13-years old, and 2097 responding in year 3 when they were 14 years old. (Participation rate 2017: 96.0% [49.9% girls], 2018: 86.5% [51.1% girls], and 2019: 88.4% [49.6% girls].) In this study, only students that answered a question regarding their gender at baseline were included in the sample, N = 2211. No one withdrew from the study and those lost at follow up are students that were not present in school on the day of the survey.
4. Procedure
All surveys were conducted by the Icelandic Center for Social Research and Analysis (ICSRA) in February in 2017, 2018 and 2019 in all secondary schools in Iceland using procedures developed by ICSRA, in collaboration with the Icelandic Ministry of Education, Science and Culture. First, the sample contact information was acquired through Statistics Iceland, the national statistical bureau. A non-traceable, unique research identification number was created for each participant. For each wave of data collection, teachers at individual school sites supervised participation of students in the classroom and administered the survey questionnaire using a double-envelope system to identify students while distributing the surveys in classroom settings, omitting their identification post-survey completion. Students were instructed not to write their names or other identifying information anywhere on the questionnaire and were asked to place their completed survey questionnaire in a nondescript, pre-sealed envelope provided to them before returning it to the supervising teacher.
5. Measures
Study variables included time spent on social media, symptoms of physical anxiety, social anxiety, and depressed mood. Three control variables were employed: Gender, family structure, and parental support. Full details of the measures are in the published supplementary file.
Time on social media was assessed at all three time points with one question: “On average, how much time do you spend on social media each day (e.g., Facebook, Snapchat, Twitter, and Instagram)?” This scale is comparable with similar measures in other studies examining how much time adolescents spend on social media (Twenge et al. 2018).
Physical symptoms of anxiety were measured at all three time points with the 12-item physical symptoms Multidimensional Anxiety Scale for Children (MASC), translated and adapted for Icelandic youth (Olason et al. 2004). The scale has demonstrated good reliability and validity in a sample of Icelandic adolescents (Olason et al. 2004). In this sample, Cronbach's alpha was 0.886 (T1), 0.912 (T2), and 0.919 (T3).
Symptoms of social anxiety were measured at all three time points with the 9-item social anxiety scale from the Icelandic version of MASC (Olason et al. 2004). The scale has demonstrated good reliability and validity in a sample of Icelandic adolescents (Olason et al. 2004). In this sample, Cronbach's alpha was 0.896 (T1), 0.915 (T2), and 0.920 (T3).
Depressed mood was measured at all three time points with nine items from the depression dimension scale of the Original Symptom Checklist (Derogatis and Unger 2010). The scale demonstrates good internal consistency and test-retest reliability (Derogatis and Unger 2010). In this sample, Cronbach's alpha was 0.900 (T1), 0.906 (T2), and 0.920 (T3).
Gender was a binary variable asking participants to indicate whether they were a boy (=1) or a girl (=2) at baseline.
Family structure was assessed by asking adolescents at baseline who they currently live with. For the purpose of this analysis, the variable was coded into a binary variable, participants living with both biological parents (=1) and participants living in other arrangements (=2).
Parental support was measured at all three time points with the five-item Perceived Parental Support Scale (PPS), measured on a 4-point scale, asking how adolescents perceive general support from parents. The scale has been validated in a multi-country sample and shown good internal consistency and convergent validity (Kristjansson et al. 2011). In this sample, Cronbach's alpha was 0.821 (T1), 0.872 (T2), and 0.899 (T3).
6. Statistical analysis and handling of missing data
All analyses were conducted using SPSS v.26. Missing values within individual variables ranged from 1.7% to 5.8% and are treated with pairwise deletion unless otherwise specified. All scale variables were treated as continuous and described using means and standard deviations. Gender and family structure were treated as categorical and described using valid percentages. Distributional properties were assessed for the scale variables, and skew and kurtosis determined to be around the common threshold of 1.0 or less in all instances, except the PPS scale where skew was 1.6 and kurtosis 3.0. Alpha was set to 0.05 for all analyses.
Linear mixed-effects models were the primary tool of analysis for the main outcomes of psychological distress over time, using a long format (three rows per person, one row for each time point). These models are designed to model correlations among observations on subjects (over time and/or within groups), and they are valid in the presence of missing at random data (Verbeke and Molenberghs 2000, p. 568). Various covariance models were compared using Akaike's Information Criterion to determine the best fit to the data (Gurka 2006), taking into account correlations between observations over time. The best-fitting structure included unstructured covariance matrix. The tests of hypotheses involved the fixed effects (FE) portion of the model, namely the association between social media use (time-varying) and symptoms of depressed mood, and physical and social anxiety. Control variables in each of these models were gender and family structure (both time-invariant), and parental support (time-varying). Time was treated continuously. The model allows us to control for mental health at baseline (intercept), changes in mental health over time (the time effect), after accounting for control variables, to see if there is an average social media effect on mental health (main effect of social media). Next, we tested the addition of two interaction terms; time spent on social media by time was assessed to identify if the relationship between time spent on social media and the three outcomes increases as participants grow older, and time spent on social media by gender was tested to assess if the over-time relationship between time on social media and the three outcomes may be different between girls and boys. In the interaction effect models, time spent on social media was grand-mean centered. Accurate model parameter estimations were ensured by use of the residual maximum likelihood approach with the Kenward and Roger, 1997 approximation of degrees of freedom. Sensitivity analysis was conducted using OLS regression end-point analysis to determine model effect sizes (R-square values). Additionally, identical linear mixed models were conducted on the standardized dependent and independent variables to produce standardized parameter estimates for the model.
7. Results
Table 1 shows descriptive statistics for all study variables. Symptoms of depressed mood, symptoms of social anxiety, physical symptoms of anxiety, and time spent on social media increased over the three waves of the study, and parental support decreased. Tables 2 to 4 show the results for all linear mixed-effects models. For all three psychological distress outcome variables, symptoms were lowest for those who reported greater parental support, living with both parents and of male gender.
Table 1.
Descriptive statistics.
| Categorical variable (%) | Time 1–12 years old (N = 2211) |
Time 2–13 years old (N = 2052) |
Time 3–14 years old (N = 2097) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Girls | Boys | Total | Girls | Boys | Total | Girls | Boys | |
|
| |||||||||
| Gender | 49.9 | 50.1 | n/a | n/a | n/a | n/a | n/a | n/a | |
| Family structure – both biological parents | 74.0 | 75.3 | 72.7 | n/a | n/a | n/a | n/a | n/a | n/a |
| Continuous variables, Mean (SD) | |||||||||
| Symptoms of depressed mood | 1.64 (0.68) |
1.70 (0.72) |
1.59 (0.63) |
1.73 (0.73) |
1.86 (0.77) |
1.59 (0.63) |
1.81 (0.79) |
2.02 (0.83) |
1.58 (0.68) |
| Symptoms of social anxiety | 1.75 (0.70) |
1.90 (0.74) |
1.60 (0.64) |
1.88 (0.77) |
2.10 (0.78) |
1.63 (0.67) |
1.96 (0.81) |
2.26 (0.79) |
1.64 (0.69) |
| Physical symptoms of anxiety | 1.67 (0.60) |
1.76 (0.63) |
1.57 (0.55) |
1.76 (0.67) |
1.92 (0.69) |
1.56 (0.59 |
1.84 (0.70) |
2.08 (0.70) |
1.56 (0.60) |
| Time spent on social media | 2.82 (1.64) |
3.06 (1.65) |
2.57 (1.60) |
3.51 (1.78) |
3.87 (1.73) |
3.15 (1.76) |
3.82 (1.84) |
4.28 (1.77) |
3.37 (1.78) |
| Parental support | 3.64 (0.45) |
3.70 (0.72) |
3.59 (0.63) |
3.58 (0.54) |
3.62 (0.52) |
3.56 (0.55) |
3.57 (0.58) |
3.59 (0.55) |
3.56 (0.60) |
Table 2.
Mixed model analysis with depressed mood as the dependent variable, unstructured model with repeated effects of time.
| Model 1. No interactions |
Model 2. With interactions |
|||||||
|---|---|---|---|---|---|---|---|---|
| Fixed effects (SE) | P | 95% CI | Standardized effects (SE) | Fixed effects (SE) | P | 95% CI | Standardized effects (SE) | |
|
| ||||||||
| Intercept | 3.06 (0.07) | <0.001 | [2.92. 3.20] | 0.25 (0.03) | 3.09 (0.08) | <0.001 | [2.93, 3.25] | 0.23 (0.04) |
| Male gender | −0.23 (0.02) | <0.001 | [−0.28, −0.29] | −0.32 (0.03) | −0.24 (0.02) | <0.001 | [−0.28, −0.19] | −0.32 (0.03) |
| Family structure | −0.08 (0.03) | 0.002 | [−0.14, −0.03] | −0.12 (0.04) | −0.28 (0.03) | 0.002 | [−0.14, −0.03] | −0.11 (0.04) |
| Parental support | −0.39 (0.02) | <0.001 | [−0.43, −0.36] | −0.28 (0.01) | −0.39 (0.02) | <0.001 | [−0.43, −0.36] | −0.28 (0.01) |
| Social media time | 0.05 (0.01) | <0.001 | [0.04, 0.06] | 0.13 (0.01) | 0.04 (0.01) | 0.002 | [0.01, 0.06] | 0.19 (0.02) |
| Time | 0.04 (0.01) | <0.001 | [0.03, 0.06] | 0.05 (0.01) | 0.04 (0.01) | <0.001 | [0.03, 0.06] | 0.05 (0.01) |
| Time × Social media time | 0.02 (0.01) | <0.001 | [0.01, 0.03] | 0.04 (0.01) | ||||
| Gender × Social media time | −0.05 (0.01) | <0.001 | [−0.07, −0.03] | −0.12 (0.02) | ||||
Table 4.
Mixed model analysis with symptoms of social anxiety as the dependent variable, unstructured model with repeated effects of time.
| Model 1. No interactions |
Model 2. With interactions |
|||||||
|---|---|---|---|---|---|---|---|---|
| Fixed effects (SE) | P | 95% CI | Standardized effects (SE) | Fixed effects (SE) | P | 95% CI | Standardized effects (SE) | |
|
| ||||||||
| Intercept | 3.06 (0.08) | <0.001 | [2.91, 3.21] | 0.34 (0.04) | 3.02 (0.08) | <0.001 | [2.85, 3.18] | 0.33 (0.04) |
| Male gender | −0.43 (0.03) | <0.001 | [−0.48, −0.38] | −0.56 (0.03) | −0.43 (0.03) | <0.001 | [−0.48, −0.38] | −0.57 (0.03) |
| Family structure | −0.07 (0.03) | 0.015 | [−0.13, −0.01] | −0.09 (0.04) | −0.07 (0.03) | 0.016 | [−0.13, −0.01] | −0.09 (0.04) |
| Parental support | −0.34 (0.02) | <0.001 | [−0.37, −0.30] | −0.23 (0.01) | −0.33 (0.02) | <0.001 | [−0.27, −0.30] | −023 (0.01) |
| Social media time | 0.04 (0.01) | <0.001 | [0.03, 0.05] | 0.09 (0.01) | 0.05 (0.01) | <0.001 | [0.02, 0.07] | 0.14 (0.02) |
| Time | 0.07 (0.01) | <0.001 | [0.05, 0.09] | 0.08 (0.01) | 0.07 (0.01) | <0.001 | [0.05, 0.09] | 0.07 (0.01) |
| Time × Social media time | 0.01 (0.01) | 0.130 | [0.00, 0.02] | 0.02 (0.01) | ||||
| Gender × Social media time | −0.05 (0.01) | <0.001 | [−0.07, −0.03] | −0.11 (0.02) | ||||
Hypothesis 1.
After controlling for time and other covariates, time spent on social media was significantly positively associated with depressed mood (FE = 0.04, SE = 0.01, p = 0.002), physical symptoms of anxiety (FE = 0.04, SE = 0.01, p = 0.001) and symptoms of social anxiety (FE = 0.05, SE = 0.01, p < 0.001). A significant main effect of time indicates that symptoms increase between data collection waves 1, 2 and 3, after taking into account other variables.
Hypothesis 2.
There was a significant interaction between time and time spent on social media on symptoms of depressed mood (FE = 0.02, SE = 0.01, p < 0.001) and physical symptoms of anxiety (FE = 0.01, SE = 0.005, p = 0.002), but not on symptoms of social anxiety. This partially supports hypothesis two. The significant social media by time interaction suggests that the impact of social media increases as participants grow older.
Hypothesis 3.
There was a significant interaction between time spent on social media and gender for symptoms of depressed mood (FE = 0.05, SE = 0.01, p < 0.001), symptoms of social anxiety (FE = -0.05, SE = 0.01, p < 0.001) and physical symptoms of anxiety (FE = -0.05, SE = 0.01, p < 0.001). The gender by time spent on social media interaction suggests that the relationship between social media and symptoms of depressed mood, symptoms of social anxiety, and physical symptoms of anxiety is stronger for girls than boys.
The sensitivity analysis for the end-point OLS regression R-squared values for symptoms of depressed mood, symptoms of physical anxiety, and social anxiety symptoms were 0.299, 0.326, and 0.374, respectively.
8. Discussion
Consistent with some previous work (Boers et al. 2019; Riehm et al. 2019; Vannucci and McCauley Ohannessian 2019), we found a relationship between time spent on social media and symptoms of psychological distress, although in our study this relationship was negligible. Other researchers (Vannucci and McCauley Ohannessian 2019) that have examined social media use by subgroups found that adolescents who use social media excessively and across multiple platforms reported higher levels of depressive symptoms and panic disorder over six months than adolescents who used only Instagram and Snapchat and compared with adolescents who used little social media. Moreover, in that work, different types of social media use did not predict symptoms of generalized anxiety disorder, separation anxiety disorder or social anxiety disorder.
These findings are similar to those reported here, where we found evidence of time spent on social media being positively associated with both physical symptoms of anxiety and symptoms of social anxiety; this relationship strengthened over time with physical symptoms of anxiety but not with social anxiety. It is possible that the non-significant relationship for social anxiety is because those individuals who suffer from social anxiety do not feel good in certain social circumstances. Social media, where they have a platform to engage absent real-life social situations, thus provide a buffer. Different dimensions of psychological distress in relation to social media use nevertheless should receive further exploration and examination using other measures, such as social anxiety among social media users.
Previous studies have shown that as adolescents move from pre-teen to teen years, identity exploration increases and the need for peer acceptance becomes more important (Gerwin et al. 2018). The transformational framework (Nesi et al. 2018a, 2018b) proposes that the nature of social media context—frequent contact with peers, the constant feedback, public display of the self—possibly amplifies identity and peer acceptance concerns, which in turn may plausibly explain worsening adolescent mental health (Gerwin et al. 2018; Nesi et al. 2018a) through mechanisms such as upward social comparison, negative self-evaluation and decreased perceived support from friends (Nesi et al. 2018b).
Girls in our study reported more psychological distress than boys; the relationship between social media use and all three outcomes was significantly stronger for girls compared to boys, although the interaction effect is very weak and may not be of clinical importance. Longitudinal studies have reported mixed findings on the role of gender (Booker et al. 2018; Heffer et al. 2019; Vannucci and McCauley Ohannessian 2019), with some studies finding that the relationship is stronger or only exists for girls (Booker et al. 2018) or that there is no gender difference (Riehm et al. 2019; Vannucci and McCauley Ohannessian 2019).
In this study, there were positive relationships between social media use and different psychological distress symptoms, although, in all instances, the effects were small and may not be meaningful as an assessment for change despite the statistical significance. Furthermore, it could be that the change in this direction is a reflection of increased age and older adolescents are more prone to emotional difficulties. To date there is no clear consensus in the literature on whether or not there is a relationship between social media and well-being (Orben et al. 2019; Orben and Przybylski 2019; Twenge 2019; Twenge and Campbell 2019). This could be due to lack of consensus on what measures to use (those examining positive or negative aspects of mental health with varying specificity) and how to analyze time spent on social media. In this study, time was treated as a continuous linear variable, comparable to some studies (Boers et al. 2019; Twenge et al. 2018) but others have chosen to compare subgroups of low and heavy users (Kelly et al. 2018; Riehm et al. 2019) or different forms of use (Vannucci and McCauley Ohannessian 2019). The former approach assumes similar effects of time across the spectrum of social media use, while the latter endorses that only heavy use has an impact on psychological distress. Perhaps the better question is whether social media meaningfully contributes to the mental health of young people. This is a topic of significant debate, as Twenge (2019) has found a comparable relationship and concluded that using the medium may have harmful effects. On the other hand, others have argued that the impact of social media is generally limited and other factors may play a larger role in the development of mental health among youth (Orben et al. 2019; Orben and Przybylski 2019). Thus, we sought to identify the unique relationships of social media with mental health by including control variables, especially parental support, whose protective effects have been widely established (Hall-Lande et al. 2007; Stadler et al. 2010). Our findings suggest that the relationship between social media and symptoms of depressed mood and physical symptoms of anxiety increases as participants grow older. However, the parameter estimates are low and should be interpreted cautiously, where some have suggested using a cutoff of β = 0.2 for interpretation of clinical significance (Ferguson 2009), while others have suggested associations of r = 0.1 for a practically significant interpretation (Orben and Przybylski 2019). Furthermore, it is also very possible that adolescents that have poorer mental health turn to social media to feel better.
There is a lack of consensus in the literature on the role of social media in mental health. We believe that in order to reach a better understanding of how and if social media is related to mental health the focus needs to be on the different aspects of social media and potential positive as well as negative effects. For example, one important distinction is whether youth use social media actively (chatting with friends and posting content) or passively (scrolling, looking at content from others). A recent cross-sectional study of Icelandic adolescents found that using social media passively was positively associated with symptoms of emotional distress, while active social media use did not relate to emotional distress (Thorisdottir et al. 2019). Until the mechanisms are better understood, a careful presentation of the narrative is needed.
There are several limitations. First, we used a single question to examine average social media use and did not include measures on different platforms or different types of social media use, such as active or passive use, which along with time spent on social media, has been shown to be significantly associated with increased psychological distress (Thorisdottir et al. 2019). Self-report measures might not accurately reflect the time that adolescents spend on social media and this area of inquiry would benefit from designing multi-report studies that include ecological momentary assessment as well as reporting from parents. Second, social media use was treated as a continuous variable instead of looking at different categories of high versus low social media use, thus diminishing comparability with some other studies. Third, we did not test for possible pathways between social media use and mental health such as cyberbullying, sleep, body image or self-esteem (Kelly et al. 2018). Finally, we did not test for the directionality of effects. Recent studies have begun to do so with one longitudinal study finding that social media use did not predict later depressive symptoms, but rather that greater depressive symptoms predicted more frequent social media use (Heffer et al. 2019). Contrary to these findings, an experimental study found that limiting social media use to 30 min a day for three days resulted in decreased loneliness and reduced depressive symptoms (Hunt et al. 2018). Understanding the bi-directionality of these complex relationships will be required to disentangle if these small associations that have been found between social media use and psychological distress are meaningful or not. The phenomena of social media as well as mental health is fraught with complexity and a number of unmeasured third-factor variables have yet to be identified and understood.
Despite these limitations, our study has notable strengths. We used a within-person approach to examine the relationship between social media and symptoms of psychological distress among a birth cohort over three time points. Our study also benefited from a large sample and high participant retention across each of the three time points. Finally, the questionnaires were empirically supported with high reliability and we included validated measures on different types of anxiety over three years, the first study to do so.
In conclusion, although adolescent use of social media appears to confer some benefits (Anderson and Jiang 2018; Seabrook et al. 2016; Thorisdottir et al. 2019), it is also a relatively new and prevalent factor in the lives of adolescents that our data show is positively related to increased levels of psychological distress, although the effects were weak to small. However, the effect of social media on psychological distress is most likely multifactorial and a better understanding of the mechanisms involved is required before we can warrant major concerns about the longitudinal impact of social media on adolescent mental health.
Supplementary Material
Table 3.
Mixed model analysis with physical symptoms of anxiety as the dependent variable, unstructured model with repeated effects of time.
| Model 1. No interactions |
Model 2. With interactions |
|||||||
|---|---|---|---|---|---|---|---|---|
| Fixed effects (SE) | P | 95% CI | Standardized effects (SE) | Fixed effects (SE) | P | 95% CI | Standardized effects (SE) | |
|
| ||||||||
| Intercept | 2.84 (0.07) | <0.001 | [2.71. 2.97] | 0.29 (0.04) | 2.84 (0.08) | <0.001 | [2.69, 2.99] | 0.28 (0.04) |
| Male gender | −0.31 (0.02) | <0.001 | [−0.35, −0.37] | −0.47 (0.03) | −0.32 (0.02) | <0.001 | [−0.36, −0.37] | −0.48 (0.03) |
| Family structure | −0.05 (0.02) | 0.023 | [−0.10, −0.01] | −0.09 (0.04) | −0.05 (0.02) | 0.028 | [−0.10, −0.01] | −0.08 (0.04) |
| Parental support | −0.32 (0.02) | <0.001 | [−0.35, −0.28] | −0.35 (0.01) | −0.31 (0.02) | <0.001 | [−0.35, −0.28] | −0.25 (0.01) |
| Social media time | 0.05 (0.0005) | <0.001 | [0.04, 0.06] | 0.13 (0.01) | 0.04 (0.01) | 0.001 | [0.02, 0.06) | 0.19 (0.02) |
| Time | 0.04 (0.01) | <0.001 | [0.03, 0.06] | 0.05 (0.01) | 0.04 (0.01) | <0.001 | [0.03, 0.06] | 0.05 (0.01) |
| Time × Social media time | 0.01 (0.005) | 0.002 | [0.01, 0.02] | 0.03 (0.01) | ||||
| Gender × Social media time | −0.05 (0.01) | <0.001 | [−0.06, −0.03] | −0.13 (0.03) | ||||
Funding
The European Research Council (ERC) award ERC-CoG-2014-647860 supported this work and I.E.T was funded by a PhD research grant awarded by the Icelandic Centre for Research (No. 174030-051). The content is solely the responsibility of the authors and does not necessarily represent the official views of the ERC or Icelandic Centre for Research or other entities with which the authors are affiliated.
Footnotes
Declaration of Competing Interest
The authors declare no conflicts of interest.
References
- Amato PR, 2000. The consequences of divorce for adults and children. J. Marriage Fam. 62, 1269–1287. 10.1111/j.1741-3737.2000.01269.x. [DOI] [Google Scholar]
- Anderson M, Jiang J, 2018. Teens, Social Media & Technology 2018. Pew Research Centre. [Google Scholar]
- Behere AP, Basnet P, Campbell P, 2017. Effects of family structure on mental health of children: a preliminary study. Indian J. Psychol. Med. 39, 457–463. 10.4103/0253-7176.211767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boers E, Afzali MH, Newton N, Conrod P, 2019. Association of screen time and depression in adolescence. JAMA Pediatr. 173, 853–859. 10.1001/jamapediatrics.2019.1759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Booker CL, Kelly YJ, Sacker A, 2018. Gender differences in the associations between age trends of social media interaction and well-being among 10–15 year olds in the UK. BMC Public Health 18, 321. 10.1186/s12889-018-5220-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bor W, Dean AJ, Najman J, Hayatbakhsh R, 2014. Are child and adolescent mental health problems increasing in the 21st century? A systematic review. Aust. N. Z. J. Psychiatr. 48, 606–616. 10.1177/0004867414533834. [DOI] [PubMed] [Google Scholar]
- Calancie O, Ewing L, Narducci LD, Horgan S, Khalid-Khan S, 2017. Exploring how social networking sites impact youth with anxiety: a qualitative study of Facebook stressors among adolescents with an anxiety disorder diagnosis. Cyberpsychology J. Psychosocial Res. Cyberspace 11. 10.5817/CP2017-4-2. [DOI] [Google Scholar]
- Coyne SM, Rogers AA, Zurcher JD, Stockdale L, Booth M, 2020. Does time spent using social media impact mental health?: an eight year longitudinal study. Comput. Hum. Behav. 104, 106160. 10.1016/j.chb.2019.106160. [DOI] [Google Scholar]
- Derogatis LR, Unger R, 2010. Symptom checklist-90-revised. In: The Corsini Encyclopedia of Psychology. American Cancer Society, pp. 1–2. 10.1002/9780470479216.corpsy0970. [DOI] [Google Scholar]
- Devine P, Lloyd K, 2012. Internet use and psychological well-being among 10-year-old and 11-year-old children. Child Care Pract. 18, 5–22. 10.1080/13575279.2011.621888. [DOI] [Google Scholar]
- Ferguson CJ, 2009. An effect size primer: a guide for clinicians and researchers. Prof. Psychol. Res. Pract. 40, 532–538. 10.1037/a0015808. [DOI] [Google Scholar]
- Frison E, Eggermont S, 2016. Gender and Facebook motives as predictors of specific types of Facebook use: A latent growth curve analysis in adolescence. J. Adolesc. 52, 182–190. 10.1016/j.adolescence.2016.08.008. [DOI] [PubMed] [Google Scholar]
- Gerwin RL, Kaliebe K, Daigle M, 2018. The interplay between digital media use and development. Child Adolesc. Psychiatr. Clin. N. Am. 27, 345–355. 10.1016/j.chc.2017.11.002. [DOI] [PubMed] [Google Scholar]
- Gurka MJ, 2006. Selecting the best linear mixed model under REML. Am. Stat. 60, 19–26. 10.1198/000313006X90396. [DOI] [Google Scholar]
- Hall-Lande JA, Eisenberg ME, Christenson SL, Neumark-Sztainer D, 2007. Social isolation, psychological health, and protective factors in adolescence. Adolescence 42, 265–286. [PubMed] [Google Scholar]
- Heffer T, Good M, Daly O, MacDonell E, Willoughby T, 2019. The longitudinal association between social-media use and depressive symptoms among adolescents and young adults: an empirical reply to Twenge et al. (2018). Clin. Psychol. Sci. 7, 462–470. 10.1177/2167702618812727. [DOI] [Google Scholar]
- Huang C, 2017. Time spent on social network sites and psychological well-being: a meta-analysis. Cyberpsychol. Behav. Soc. Netw. 20, 346–354. 10.1089/cyber.2016.0758. [DOI] [PubMed] [Google Scholar]
- Hunt MG, Marx R, Lipson C, Young J, 2018. No more FOMO: limiting social media decreases loneliness and depression. J. Soc. Clin. Psychol. 751–768. 10.1521/jscp.2018.37.10.751. [DOI] [Google Scholar]
- Jensen M, George MJ, Russell M, Odgers CL, 2019. Young Adolescents' Digital Technology Use and Mental Health Symptoms: Little Evidence of Longitudinal or Daily Linkages. 10.1177/2167702619859336. [DOI] [PMC free article] [PubMed]
- Keles B, McCrae N, Grealish A, 2019. A systematic review: the influence of social media on depression, anxiety and psychological distress in adolescents. Int. J. Adolesc. Youth 0, 1–15. 10.1080/02673843.2019.1590851. [DOI] [Google Scholar]
- Kelly Y, Zilanawala A, Booker C, Sacker A, 2018. Social Media Use and Adolescent Mental Health: Findings From the UK Millennium Cohort Study. EClinical Med. 6, 59–68. 10.1016/j.eclinm.2018.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kenward MG, Roger JH, 1997. Small sample inference for fixed effects from restricted maximum Likelihood. Biometrics 53, 983–997. 10.2307/2533558. [DOI] [PubMed] [Google Scholar]
- Kristjansson AL, Sigfusdottir ID, Karlsson T, Allegrante JP, 2011. The perceived parental support (PPS) Scale: validity and reliability in the 2006 youth in Europe substance use prevention survey. Child Indic. Res. 4, 515–528. 10.1007/s12187-010-9095-x. [DOI] [Google Scholar]
- Landstedt E, Almquist YB, 2019. Intergenerational patterns of mental health problems: the role of childhood peer status position. BMC Psychiatry 19, 286. 10.1186/s12888-019-2278-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrae N, Gettings S, Purssell E, 2017. Social media and depressive symptoms in childhood and adolescence: a systematic review. Adolescent Res Rev 2, 315–330. 10.1007/s40894-017-0053-4. [DOI] [Google Scholar]
- Modin B, Östberg V, Almquist Y, 2011. Childhood peer status and adult susceptibility to anxiety and depression. a 30-year hospital follow-up. J. Abnorm. Child Psychol. 39, 187–199. 10.1007/s10802-010-9462-6. [DOI] [PubMed] [Google Scholar]
- Nesi J, Choukas-Bradley S, Prinstein MJ, 2018a. Transformation of adolescent peer relations in the social media context: part 1-a theoretical framework and application to dyadic peer relationships. Clin. Child Fam. Psychol. Rev. 21, 267–294. 10.1007/s10567-018-0261-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nesi J, Choukas-Bradley S, Prinstein MJ, 2018b. Transformation of adolescent peer relations in the social media context: part 2-application to peer group processes and future directions for research. Clin. Child Fam. Psychol. Rev. 21, 295–319. 10.1007/s10567-018-0262-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odgers CL, Jensen MR, 2020. Annual research review: adolescent mental health in the digital age: facts, fears, and future directions. J. Child Psychol. Psychiatry 61, 336–348. 10.1111/jcpp.13190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olason DT, Sighvatsson MB, Smári J, 2004. Psychometric properties of the multidimensional anxiety scale for children (MASC) among Icelandic schoolchildren. Scand. J. Psychol. 45, 429–436. 10.1111/j.1467-9450.2004.00424.x. [DOI] [PubMed] [Google Scholar]
- Orben A, Przybylski AK, 2019. Screens, teens, and psychological well-being: evidence from three time-use-diary studies. Psychol. Sci. 30, 682–696. 10.1177/0956797619830329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orben A, Dienlin T, Przybylski AK, 2019. Social media's enduring effect on adolescent life satisfaction. Proc. Natl. Acad. Sci. 116, 10226–10228. 10.1073/pnas.1902058116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riehm KE, Feder KA, Tormohlen KN, Crum RM, Young AS, Green KM, Pacek LR., La Flair LN., Mojtabai R., 2019. Associations between time spent using social media and internalizing and externalizing problems among US youth. JAMA Psychiat. 1–9. 10.1001/jamapsychiatry.2019.2325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seabrook EM, Kern ML, Rickard NS, 2016. Social networking sites, depression, and anxiety: a systematic review. JMIR Ment. Health 3. 10.2196/mental.5842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sigfusdottir ID, Kristjansson AL, Thorlindsson T, Allegrante JP, 2017. Stress and adolescent well-being: the need for an interdisciplinary framework. Health Promot. Int. 32, 1081–1090. 10.1093/heapro/daw038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stadler C, Feifel J, Rohrmann S, Vermeiren R, Poustka F, 2010. Peer-victimization and mental health problems in adolescents: are parental and school support protective? Child Psychiatry Hum. Dev. 41, 371–386. 10.1007/s10578-010-0174-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thorisdottir IE, Sigurvinsdottir R, Asgeirsdottir BB, Allegrante JP, Sigfusdottir ID, 2019. Active and passive social media use and symptoms of anxiety and depressed mood among Icelandic adolescents. Cyberpsychol. Behav. Soc. Netw. 22, 535–542. 10.1089/cyber.2019.0079. [DOI] [PubMed] [Google Scholar]
- Twenge JM, 2019. More time on technology, less happiness? Associations between digital-media use and psychological well-being. Curr. Dir. Psychol. Sci. 28, 372–379. 10.1177/0963721419838244. [DOI] [Google Scholar]
- Twenge JM, Campbell WK, 2019. Media use is linked to lower psychological well-being: evidence from three datasets. Psychiatry Q. 90, 311–331. 10.1007/s11126-019-09630-7. [DOI] [PubMed] [Google Scholar]
- Twenge JM, Martin GN, Campbell WK, 2018. Decreases in psychological well-being among American adolescents after 2012 and links to screen time during the rise of smartphone technology. Emotion 18, 765–780. 10.1037/emo0000403. [DOI] [PubMed] [Google Scholar]
- Vannucci A, McCauley Ohannessian C, 2019. Social media use subgroups differentially predict psychosocial well-being during early adolescence. J. Youth Adolesc. 48, 1469–1493. 10.1007/s10964-019-01060-9. [DOI] [PubMed] [Google Scholar]
- Verbeke G, Molenberghs G, 2000. Linear Mixed Models for Longitudinal Data. In: Springer Series in Statistics. Springer-Verlag, New York. 10.1007/978-1-4419-0300-6. [DOI] [Google Scholar]
- Wartella E, Rideout V, Lauricella AR, Connell S, 2013. Parenting in the age of digital technology: a national survey. In: Report for the center on media and Human development school of communication Northwestern University. [Google Scholar]
- Williams AL, Merten MJ, 2011. iFamily: internet and social media technology in the family context. Fam. Consum. Sci. Res. J. 40, 150–170. 10.1111/j.1552-3934.2011.02101.x. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.