

Abstract
Background
Many face-to-face and digital therapeutic supports are designed for adolescents experiencing high levels of psychological distress. However, promoting psychological well-being among adolescents is often neglected despite significant short-term and long-term benefits.
Objective
This research has 3 main objectives: (1) to assess the acceptability of Match Emoji, a casual video game with psychological well-being concepts among 13-15-year-old students in a New Zealand secondary school; (2) to identify the feasibility of the research process; and (3) to explore the preliminary well-being and therapeutic potential of Match Emoji.
Methods
Approximately 40 participants aged 13-15 years from a local secondary college in Wellington, New Zealand, will be invited to download and play Match Emoji 3-4 times a week for 5-15 minutes over a 2-week period. Participants will complete 4 assessments at baseline, postintervention, and 3 weeks later to assess psychological well-being and therapeutic changes. Statistical analysis will be used to synthesize data from interviews and triangulated with assessment changes and game analytics. This synthesis will help to assess the acceptability and feasibility of the Match Emoji.
Results
The key outputs from the project will include the acceptability, feasibility, and therapeutic potential of Match Emoji. It is anticipated that participants will have finished playing the recommended game play regimen by August 2021 with analysis of results completed by October 2021.
Conclusions
Data from the study are expected to inform future research on Match Emoji including a randomized controlled trial and further adjustments to the design and development of the game.
International Registered Report Identifier (IRRID)
PRR1-10.2196/31588
Keywords: digital mental health tools, casual video games, young people
Introduction
In New Zealand, an increasing number of young people experience elevated levels of psychological distress and low well-being [1]. Although treatments such as cognitive behavioral therapy exist and have shown promise for reducing clinical levels of psychological distress [2,3], supports for promoting psychological well-being are often underutilized despite their therapeutic potential [4-6].
Young adolescents, aged between 13 and 15 years, are particularly vulnerable to experiencing elevated levels of psychological distress and low well-being [7,8]. This is in part due to the additional external and internal demands placed on young adolescents from navigating puberty to the formation of gender norms and health and well-being attitudes [9,10]. To compound rapid developmental changes, young adolescents enter a more complex educational environment while forging new relationships with peers and family members. As approximately half of all mental ill-health starts by age 15 years and 75% develops by age 18 years [7], it is vital to create interventions that will promote psychological well-being skills among young adolescents.
Young adolescents in New Zealand who have access to the curriculum are provided with opportunities to learn mental health and well-being skills such as stress management and resilience skills [11,12]. Although education through the curriculum is a promising preventive measure [12,13], longitudinal research suggests more targeted supports are required to promote psychological well-being among young adolescents [14].
Given the popularity of digital technologies, a plethora of digital mental health interventions (DMHIs) have been created and shown promise for alleviating psychological distress and promoting psychological well-being in trials [15-17]. This scalable and low-cost approach is promising for young people, considering the potential to bypass traditional barriers such as stigma and time [18-20]. Recent systematic reviews and meta-analyses, however, report DMHIs are yet to reach their full engagement potential, with low real-world use of many popular mental health apps [17,21].
A growing amount of research has attempted to identify ways in which to increase adherence to DMHIs among young people [17,22]. One promising approach is using microinterventions. The goal of microinterventions is to enable users to work towards a highly focused goal with support from in-the-moment elements such as reminders and nudges [23].
A popular activity among many young people that utilizes similar underlying mechanics of microinterventions are casual video games (CVGs). Globally, CVGs such as “Bejewelled” and “Angry Birds” are played by millions of people in short bursts of time [24]. According to a recent systematic review of the literature, CVGs may also hold promising therapeutic mood enhancing and brief releases from unpleasant experiences [25]. Previous research with young adolescents suggests CVGs are a popular approach among this age group who commonly play these games to distract and “calm a busy mind” [26].
Based upon a systematic review of the literature and research with young adolescents, we created Match Emoji, a CVG with psychological well-being concepts for young adolescents. Although it is important to evaluate core psychotherapeutic components of interventions to understand how specific elements guide the design of the intervention as a whole [27], it is more useful to investigate the potential for real-world usage in naturalistic settings [21,28], As such, the aim of the current protocol is: (1) to assess the acceptability of Match Emoji among 13-15-year old students in a New Zealand secondary school, (2) to identify the feasibility of the research process, and (3) to explore the preliminary well-being and therapeutic potential of Match Emoji.
Methods
Research Strategy
This study will employ a mixed methods design to assess the acceptability, feasibility, and therapeutic potential of a CVG with psychological well-being concepts among 13-15-year-old students.
Study Design
The study will involve 3 phases. First, we will recruit 13-15-year-old students from 2-4 classrooms in a local secondary school within the Wellington region of New Zealand. Once participants have returned their consent and assent forms, they will be asked to download Match Emoji onto their phone or digital device. During the second phase, participants will be encouraged to play the game 3-4 times a week for 5-15 minutes for a 2-week period. Game play time and sessions will be collected through the Unity platform to help inform the feasibility and acceptability of the recommended game play. During the third phase, researchers will follow up 2 weeks after the recommended regimen of Match Emoji and collect secondary outcomes measures (from the Child and Adolescent Mindfulness Measure [CAMM], General Help-Seeking Questionnaire [GHSQ], Flourishing Scale [FS], and Revised Children's Anxiety and Depression Scale [RCADS]), followed by short interviews with participants about their experience.
Study Population
Approximately 40 students from a local secondary school in Wellington, New Zealand, will take part in playing Match Emoji 3-4 times a week for 5-15 minutes over a 2-week period. Participants will be invited from year 9 and 10 classrooms and are typically between 13 and 15 years of age. As this is an acceptability and feasibility study, a total of 40 participants will provide a large enough sample size to show a meaningful difference in the primary and secondary outcomes between baseline, postintervention, and a 3-week follow-up.
Inclusion Criteria
Young people will be included in the study if they are between the ages of 13 and 15 years, have provided written consent from a parent or caregiver, and are able to understand and sign the assent form.
Exclusion and Safety Criteria
Young people will be excluded from participation if they do not meet the inclusion criteria. The appropriate personnel within the secondary school will be engaged if a participant self-reports a high level of mental health need. This will be determined through the 4 questionnaires. Those participants who are engaged with existing therapeutic support are able to participate in the research study if consent has been obtained from the young person.
Intervention
Match Emoji is a match-3 CVG with psychological well-being concepts designed for young adolescents. The aim of Match Emoji is to match similar colored emojis together to earn points and progress through the game. There is a total of 6 different colored and shaped emojis that represent a unique digital expression such as an emotion, idea, or personality. When the user has successfully matched the required number of emojis with a fixed number of moves or time frame, a micromessage appears on the screen. Each micromessage consists of a short psychological well-being concept such as “notice what is going on around you” or “sometimes talking to a friend can help” and is delivered via a dynamic messaging loading system that identifies the “optimal” time to display the message. Hints are used throughout the game if players get stuck. For example, if the player waits too long before making a move, Match Emoji identifies a potential combination of similar colored emojis by moving a successful sequence of items back and forth to capture the user's attention. An example of the game can be seen in Figure 1.
Figure 1.
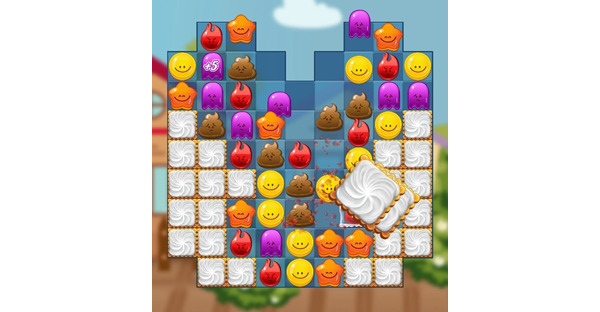
Image of the Match Emoji game.
Outcome Measures
The primary outcomes of the study are (1) acceptability of Match Emoji (ie, is Match Emoji acceptable among young adolescents), as assessed via a short semistructured intervention with participants after the recommended regime of game play and game analytics including the number of sessions and minutes played recorded via the Unity platform, and (2) feasibility of Match Emoji (ie, is it easy to complete the study with young adolescents within a secondary school context) as measured by the number of students interested in participating in completing the 4 questionnaires, playing the recommended regimen of Match Emoji, and attending the follow-up interview.
The secondary outcome (measured at baseline before accessing Match Emoji, on completing the 2 weeks of recommended game play, and at the 3-week follow-up) is efficacy (ie, does Match Emoji promote psychological well-being skills). This will be assessed by measuring changes over time in the CAMM, GHSQ, FS, and RCADS. It is estimated to take participants approximately 10-15 minutes to complete all questionnaires.
The CAMM is a 10-item measure of mindfulness for use with children and adolescents and has been reported to have good internal consistency and significant correlations between CAMM scores and measures of psychological functioning and distress [29]. The GHSQ is a 1-page questionnaire with 2 sets of questions that examine the respondent’s likelihood of seeking help for a specific issue such as psychological distress. The GHSQ has been reported to have good reliability and validity and appears to be a flexible measure of help-seeking intentions that can be applied to different contexts and age groups including young people [30].
The 8-item FS is a valid and reliable brief summary measure of psychological well-being suited for young people [31,32]. The scale provides a single psychological well-being score derived from the 8 questions and has been used as an effective measure to access adolescents’ psychological well-being in the New Zealand secondary school context [33]. The RCADS is a youth self-report questionnaire with 6 subscales including separation anxiety disorder and low mood. The RCADS has good reliability on subscales and total scale [34], internal consistency, and good convergent validity [35]. The RCADS has been used as an appropriate and easy-to-administer assessment tool of anxiety and depressive symptoms in several populations within New Zealand [35,36].
Interviews lasting approximately 30 minutes will take place with no more than 6 participants at one time to understand experiences with playing Match Emoji. Interviews will be conducted by the first author (RP) at the local school in a setting familiar to the participants. Responses will be recorded in a paper-based format. Questions will involve (1) What parts of the game did you like? (2) What parts of the game could be improved? (3) What did you learn from playing the game? (4) Did you try and use any of the ideas from the game and if so, which ones? (5) Do you think you will continue to play Match Emoji? Interviews will not involve more than 6 participants at a time. At the end of the interview, participants will be able to read and correct answers.
Statistical Analysis
Quantitative data from the 4 assessments and game play usage will be analyzed using Microsoft Excel, SPSS version 26, and the metrics recorded from the Unity platform including number of sessions and minutes played [37,38]. Analyses will include descriptive statistics (eg, number of sessions completed, number of minutes played, changes in assessment scores, and sociodemographic characteristics of the participants).
As this is an acceptability and feasibility study, a sample size of 40 participants will be a large enough sample to show a meaningful difference in primary and secondary outcomes between baseline and the end of the interview. Chi-square tests and t tests will be used to assess the statistical significance of changes in the 4 assessment scores over time. A P value <.05 will be used at the 95% confidence level to determine the therapeutic potential of any difference between pre- and postmeasures. NVivo will be used to store and code qualitative data from the interviews with participants. A general inductive approach will be used by researchers to identify and analyze emerging themes [39].
Ethics and Consent
This study received ethics approval from the New Zealand Health and Disability Ethics Committee (21/NTA/34) on May 28, 2021. After the college principal or senior management staff member has understood and approved the research, participants will be provided with information about the study. Students will be provided with time to ask questions before deciding to provide informed decision about their voluntary participation through an assent form. A consent form will also be required from the parent or guardian.
All the project data and materials sent for publication will be de-identified by removing statements identifying participants. Participants who disclose mental health needs that meet the threshold for a clinical diagnosis will be handled by appropriate school personnel such as a school counsellor. The data will be stored securely in a password-protected computer accessible only to the research team. The de-identifiable findings will be included in the first author’s (RP) doctoral thesis as well as being disseminated through peer-reviewed academic journals, national and international conferences, and public events. If parents ask for their child’s individual results such as game analytics, we will seek permission from the child first.
Results
Recruitment of participants started in June 2021, with completion anticipated to be completed by July 2021. It is anticipated that participants will have finished playing the recommended game play regimen by August 2021 with analysis of results completed by October 2021. The key outputs from the game will inform future design and iterations of the game. In addition, a larger and more robust methodological approach such as a randomized controlled trial may be created to fully understand the therapeutic effects of Match Emoji.
Discussion
Promoting psychological well-being among young adolescents may support overall health and improve disease-specific outcomes later in life [40-42]. Given the potential benefits of promoting psychological well-being coupled with a heightened risk of experiencing elevated levels of psychological distress, it is crucial to explore engaging, preventive tools for young adolescents [43]. This is particularly important in New Zealand where a growing number of young people have reported experiencing psychological distress [14].
The current acceptability and feasibility study aims to assess the acceptability of Match Emoji among 13-15-year-old students in a New Zealand secondary school, identify the feasibility of the research process, and examine the psychological well-being and therapeutic potential of the game. The primary outcomes of the study will help to shape the iterative design process of Match Emoji and understand if the game is worthy of more rigorous testing in a randomized controlled trial. The secondary outcomes will examine the psychological well-being and therapeutic potential of Match Emoji. If Match Emoji is shown in subsequent studies to be acceptable and useful for young adolescents in its final form, it is hoped that the game may be promoted and available free of charge to young people in New Zealand on Google Play and App Store.
Abbreviations
- CAMM
Child and Adolescent Mindfulness Measure
- CVG
casual video game
- DMHI
digital mental health intervention
- FS
Flourishing Scale
- GHSQ
General Help-Seeking Questionnaire
- RCADS
Revised Children's Anxiety and Depression Scale
Appendix
Original peer-review report from the funding agency (Health and Disability Ethics Committees, Ministry of Health, New Zealand).
Peer review from academic.
Footnotes
Conflicts of Interest: TF is a co-developer of SPARX, a computerized CBT program for adolescent depression. The Intellectual Property for SPARX is owned by Uniservices at the University of Auckland and co-developers can benefit financially from licensing of SPARX outside of New Zealand.
References
- 1.Every-Palmer S, Jenkins M, Gendall P, Hoek J, Beaglehole B, Bell C, Williman J, Rapsey C, Stanley J. Psychological distress, anxiety, family violence, suicidality, and wellbeing in New Zealand during the COVID-19 lockdown: A cross-sectional study. PLoS One. 2020 Nov 4;15(11):e0241658. doi: 10.1371/journal.pone.0241658. https://dx.plos.org/10.1371/journal.pone.0241658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Andrews G, Bell C, Boyce P, Gale C, Lampe L, Marwat O, Rapee R, Wilkins G. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of panic disorder, social anxiety disorder and generalised anxiety disorder. Aust N Z J Psychiatry. 2018 Nov 30;52(12):1109–1172. doi: 10.1177/0004867418799453. [DOI] [Google Scholar]
- 3.Nixon RDV. CBT for anxiety disorders: A practitioner book. Clinical Psychologist. 2020 Nov 09;18(2):98–98. doi: 10.1111/cp.12042. [DOI] [Google Scholar]
- 4.Funmi T, Modupe T, Oluwasegun O. Promoting Psychological Wellbeing across the Life Span: Prospects and Challenges in Nigeria. JPBR. 2020 May 08;2(1):p43. doi: 10.22158/jpbr.v2n1p43. [DOI] [Google Scholar]
- 5.Ruini C, Ottolini F, Tomba E, Belaise C, Albieri E, Visani D, Offidani E, Caffo E, Fava GA. School intervention for promoting psychological well-being in adolescence. J Behav Ther Exp Psychiatry. 2009 Dec;40(4):522–32. doi: 10.1016/j.jbtep.2009.07.002. [DOI] [PubMed] [Google Scholar]
- 6.Boehm JK, Trudel-Fitzgerald C, Kivimaki M, Kubzansky LD. The prospective association between positive psychological well-being and diabetes. Health Psychol. 2015 Oct;34(10):1013–21. doi: 10.1037/hea0000200. http://europepmc.org/abstract/MED/25603420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005 Jun;62(6):593–602. doi: 10.1001/archpsyc.62.6.593. [DOI] [PubMed] [Google Scholar]
- 8.Loewen OK, Maximova K, Ekwaru JP, Faught EL, Asbridge M, Ohinmaa A, Veugelers PJ. Lifestyle Behavior and Mental Health in Early Adolescence. Pediatrics. 2019 May 19;143(5):e20183307. doi: 10.1542/peds.2018-3307. http://pediatrics.aappublications.org/cgi/pmidlookup?view=long&pmid=31004047. [DOI] [PubMed] [Google Scholar]
- 9.Kågesten A, Gibbs S, Blum RW, Moreau C, Chandra-Mouli V, Herbert A, Amin A. Understanding Factors that Shape Gender Attitudes in Early Adolescence Globally: A Mixed-Methods Systematic Review. PLoS One. 2016 Jun 24;11(6):e0157805. doi: 10.1371/journal.pone.0157805. https://dx.plos.org/10.1371/journal.pone.0157805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lane C, Brundage CL, Kreinin T. Why We Must Invest in Early Adolescence: Early Intervention, Lasting Impact. J Adolesc Health. 2017 Oct;61(4 Suppl):S10–S11. doi: 10.1016/j.jadohealth.2017.07.011. https://linkinghub.elsevier.com/retrieve/pii/S1054-139X(17)30357-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ministry of Education The New Zealand Curriculum for English-Medium Teaching and Learning in Years 1-13. 2007. [2021-07-26]. https://www.academia.edu/24415300/The_New_Zealand_Curriculum_for_English-medium_teaching_and_learning_in_years_1_13.
- 12.Fitzpatrick KM, Harris C, Drawve G. How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide Life Threat Behav. 2020 Dec;50(6):1241–1249. doi: 10.1111/sltb.12655. http://europepmc.org/abstract/MED/32589799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kutcher S, Wei Y, Coniglio C. Mental Health Literacy: Past, Present, and Future. Can J Psychiatry. 2016 Mar 03;61(3):154–8. doi: 10.1177/0706743715616609. http://europepmc.org/abstract/MED/27254090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Clark T, Fleming T, Bullen P, Crengle S, Denny S, Dyson B, Peiris-John R, Robinson E, Rossen F, Sheridan J, Teevale T, Utter J, Lewycka S. Health and well-being of secondary school students in New Zealand: trends between 2001, 2007 and 2012. J Paediatr Child Health. 2013 Nov 07;49(11):925–934. doi: 10.1111/jpc.12427. doi: 10.1111/jpc.12427. [DOI] [PubMed] [Google Scholar]
- 15.Armaou M, Konstantinidis S, Blake H. The Effectiveness of Digital Interventions for Psychological Well-Being in the Workplace: A Systematic Review Protocol. Int J Environ Res Public Health. 2019 Dec 30;17(1):255. doi: 10.3390/ijerph17010255. https://www.mdpi.com/resolver?pii=ijerph17010255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lehtimaki S, Martic J, Wahl B, Foster KT, Schwalbe N. Evidence on Digital Mental Health Interventions for Adolescents and Young People: Systematic Overview. JMIR Ment Health. 2021 Apr 29;8(4):e25847. doi: 10.2196/25847. https://mental.jmir.org/2021/4/e25847/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Garrido S, Millington C, Cheers D, Boydell K, Schubert E, Meade T, Nguyen QV. What Works and What Doesn't Work? A Systematic Review of Digital Mental Health Interventions for Depression and Anxiety in Young People. Front Psychiatry. 2019 Nov 13;10:759. doi: 10.3389/fpsyt.2019.00759. doi: 10.3389/fpsyt.2019.00759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Renton T, Tang H, Ennis N, Cusimano MD, Bhalerao S, Schweizer TA, Topolovec-Vranic J. Web-based intervention programs for depression: a scoping review and evaluation. J Med Internet Res. 2014 Sep 23;16(9):e209. doi: 10.2196/jmir.3147. https://www.jmir.org/2014/9/e209/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kass AE, Balantekin KN, Fitzsimmons-Craft EE, Jacobi C, Wilfley DE, Taylor CB. The economic case for digital interventions for eating disorders among United States college students. Int J Eat Disord. 2017 Mar;50(3):250–258. doi: 10.1002/eat.22680. http://europepmc.org/abstract/MED/28152203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lattie EG, Adkins EC, Winquist N, Stiles-Shields C, Wafford QE, Graham AK. Digital Mental Health Interventions for Depression, Anxiety, and Enhancement of Psychological Well-Being Among College Students: Systematic Review. J Med Internet Res. 2019 Jul 22;21(7):e12869. doi: 10.2196/12869. https://www.jmir.org/2019/7/e12869/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fleming T, Bavin L, Lucassen M, Stasiak K, Hopkins S, Merry S. Beyond the Trial: Systematic Review of Real-World Uptake and Engagement With Digital Self-Help Interventions for Depression, Low Mood, or Anxiety. J Med Internet Res. 2018 Jun 06;20(6):e199. doi: 10.2196/jmir.9275. https://www.jmir.org/2018/6/e199/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Liverpool S, Mota CP, Sales CMD, Čuš A, Carletto S, Hancheva C, Sousa S, Cerón SC, Moreno-Peral P, Pietrabissa G, Moltrecht B, Ulberg R, Ferreira N, Edbrooke-Childs J. Engaging Children and Young People in Digital Mental Health Interventions: Systematic Review of Modes of Delivery, Facilitators, and Barriers. J Med Internet Res. 2020 Jun 23;22(6):e16317. doi: 10.2196/16317. https://www.jmir.org/2020/6/e16317/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Baumel A, Fleming T, Schueller SM. Digital Micro Interventions for Behavioral and Mental Health Gains: Core Components and Conceptualization of Digital Micro Intervention Care. J Med Internet Res. 2020 Oct 29;22(10):e20631. doi: 10.2196/20631. https://www.jmir.org/2020/10/e20631/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Clement J. Share of casual video gamers worldwide as of 2019, by age. Statista. 2021. Feb 08, [2021-07-26]. https://www.statista.com/statistics/1128710/casual-video-gamers-age/
- 25.Pine R, Fleming T, McCallum S, Sutcliffe K. The Effects of Casual Videogames on Anxiety, Depression, Stress, and Low Mood: A Systematic Review. Games Health J. 2020 Aug;9(4):255–264. doi: 10.1089/g4h.2019.0132. [DOI] [PubMed] [Google Scholar]
- 26.Pine R, Sutcliffe K, McCallum S, Fleming T. Young adolescents' interest in a mental health casual video game. Digit Health. 2020 Aug 30;6:2055207620949391. doi: 10.1177/2055207620949391. https://journals.sagepub.com/doi/10.1177/2055207620949391?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Meinlschmidt G, Lee J, Stalujanis E, Belardi A, Oh M, Jung EK, Kim H, Alfano J, Yoo S, Tegethoff M. Smartphone-Based Psychotherapeutic Micro-Interventions to Improve Mood in a Real-World Setting. Front Psychol. 2016 Jul 28;7:1112. doi: 10.3389/fpsyg.2016.01112. doi: 10.3389/fpsyg.2016.01112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bidargaddi N, Schrader G, Klasnja P, Licinio J, Murphy S. Designing m-Health interventions for precision mental health support. Transl Psychiatry. 2020 Jul 07;10(1):222. doi: 10.1038/s41398-020-00895-2. doi: 10.1038/s41398-020-00895-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kuby AK, McLean N, Allen K. Validation of the Child and Adolescent Mindfulness Measure (CAMM) with Non-Clinical Adolescents. Mindfulness. 2015 May 22;6(6):1448–1455. doi: 10.1007/s12671-015-0418-3. [DOI] [Google Scholar]
- 30.Olivari C, Guzmán-González M. Validación del cuestionario general de búsqueda de ayuda para problemas de salud mental en adolescentes. Rev. chil. pediatr. 2017 Jun;88(3):324–331. doi: 10.4067/s0370-41062017000300003. [DOI] [PubMed] [Google Scholar]
- 31.Diener E, Wirtz D, Tov W, Kim-Prieto C, Choi D, Oishi S, Biswas-Diener R. New Well-being Measures: Short Scales to Assess Flourishing and Positive and Negative Feelings. Soc Indic Res. 2009 May 28;97(2):143–156. doi: 10.1007/s11205-009-9493-y. [DOI] [Google Scholar]
- 32.Schotanus-Dijkstra M, Ten Klooster PM, Drossaert CHC, Pieterse ME, Bolier L, Walburg JA, Bohlmeijer ET. Validation of the Flourishing Scale in a sample of people with suboptimal levels of mental well-being. BMC Psychol. 2016 Mar 17;4(1):12. doi: 10.1186/s40359-016-0116-5. https://bmcpsychology.biomedcentral.com/articles/10.1186/s40359-016-0116-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hone LC, Jarden A, Schofield G, Duncan S. Measuring flourishing: The impact of operational definitions on the prevalence of high levels of wellbeing. Intnl. J. Wellbeing. 2014 Jun 04;4(1):62–90. doi: 10.5502/ijw.v4i1.4. [DOI] [Google Scholar]
- 34.Chorpita BF, Moffitt CE, Gray J. Psychometric properties of the Revised Child Anxiety and Depression Scale in a clinical sample. Behav Res Ther. 2005 Mar;43(3):309–22. doi: 10.1016/j.brat.2004.02.004. [DOI] [PubMed] [Google Scholar]
- 35.Esbjørn BH, Sømhovd MJ, Turnstedt C, Reinholdt-Dunne ML. Assessing the Revised Child Anxiety and Depression Scale (RCADS) in a national sample of Danish youth aged 8-16 years. PLoS One. 2012 May 23;7(5):e37339. doi: 10.1371/journal.pone.0037339. https://dx.plos.org/10.1371/journal.pone.0037339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Radez J, Waite P, Chorpita B, Creswell C, Orchard F, Percy R, Spence SH, Reardon T. Using the 11-item Version of the RCADS to Identify Anxiety and Depressive Disorders in Adolescents. Res Child Adolesc Psychopathol. 2021 Apr 01;:2020. doi: 10.1007/s10802-021-00817-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.SPSS software. IBM. [2021-07-26]. https://www.ibm.com/analytics/spss-statistics-software.
- 38.Unity. [2021-07-26]. https://unity.com/
- 39.Thomas DR. A General Inductive Approach for Analyzing Qualitative Evaluation Data. American Journal of Evaluation. 2016 Jun 30;27(2):237–246. doi: 10.1177/1098214005283748. [DOI] [Google Scholar]
- 40.Ong AD, Mroczek DK, Riffin C. The Health Significance of Positive Emotions in Adulthood and Later Life. Soc Personal Psychol Compass. 2011 Aug 01;5(8):538–551. doi: 10.1111/j.1751-9004.2011.00370.x. http://europepmc.org/abstract/MED/21927620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Diener E, Chan MY. Happy People Live Longerubjective Well-Being Contributes to Health and Longevity. Applied Psychology: Health and Well-Being. 2011;3(1):1–43. doi: 10.1111/j.1758-0854.2010.01045.x. [DOI] [Google Scholar]
- 42.DeSteno D, Gross JJ, Kubzansky L. Affective science and health: the importance of emotion and emotion regulation. Health Psychol. 2013 May;32(5):474–86. doi: 10.1037/a0030259. [DOI] [PubMed] [Google Scholar]
- 43.Tang Y, Tang R, Gross JJ. Promoting Psychological Well-Being Through an Evidence-Based Mindfulness Training Program. Front Hum Neurosci. 2019 Jul 10;13:237. doi: 10.3389/fnhum.2019.00237. doi: 10.3389/fnhum.2019.00237. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Original peer-review report from the funding agency (Health and Disability Ethics Committees, Ministry of Health, New Zealand).
Peer review from academic.