

Summary
Burn injury is still a global health problem due to its high incidence. Healing of burn wounds requires an optimal state of the body that is characterized by serum albumin level, especially in the category of patients that require skin graft to cover the wound caused by the deep burn. This study investigates the relationship between albumin levels and the outcome of split-thickness skin graft (STSG) and obtains a tolerance limit for albumin levels that can be successful in STSG. This was a prospective cohort study at our Plastic Surgery Center in Bandung, West Java, Indonesia from June 2019 to November 2020. Fortyseven burn injury patients who had undergone STSG qualified as the study subjects based on the criteria set. Of these patients, 85.11% were male and 68.08% were in the productive age. Preoperative albumin level has no significant correlation with graft outcome (P>0.05). Area Under the Curve (AUC) is 0.758; (95% CI: 0.605, 0.910). The optimal cut-off point for albumin levels is 2.175 (sensitivity of 0.78 and a specificity of 0.714). In our study, graft healing has no significant correlation with albumin levels. Further study is needed to assess the relationship between serum albumin levels (preoperative and postoperative) with outcome of the graft, and assess infection status.
Keywords: serum albumin, skin graft, burn injury
Abstract
En raison d’une incidence restant élevée, les brûlures demeurent un problème de santé publique. Leur guérison nécessite une optimisation de l’état général, reflété par l’albuminémie, en particulier chez les patients ayant besoin de greffes. Cette étude évalue la corrélation entre l’albuminémie et l’intégration des Greffes de Peau Mince (GPM), en recherchant un seuil bas d’albuminémie avant GPM. Elle a été conduite dans le service de chirurgie plastique de l’hôpital de Bandung, dans l’ouest de l’île de Java, entre juin 2019 et novembre 2020, auprès de 47 patients brûlés ayant besoin d’une GPM (85,11% d’hommes dont 68,08% en âge de travailler). Nous n’avons pas trouvé de relation significative entre l’albuminémie préopératoire et l’intégration des greffes (p > 0,05 ; aire sous courbe ROC 0,758 ; IC95 0,605 à 0,910). La limite optimale de l’albuminémie est de 21,75 g/L, amenant une sensibilité de 0,78 et une spécificité de 0,714. Devant cette absence de significativité, il est nécessaire de prolonger les études à la recherche d’une albuminémie (pré- et post- opératoire) permettant d’améliorer l’intégration des greffes et de réduire l’incidence des infections.
Introduction
High mortality rate due to complications of burn means burn injury is considered a global health problem. An estimated 180,000 deaths worldwide every year is due to burns. Most of these cases occur in countries with low-moderate income, and almost two-thirds of the cases are in African and Southeast Asian countries.1 Surviving burn patients also face morbidity, such as contractures and keloids, the number of which is still high.2,3 Morbidity remains a problem that needs to be resolved.
Proper burn wound management requires an optimal state of the body that is supported by laboratory results, such as hemoglobin (Hb) levels above 10 g/dL and albumin levels above 2.5 gr%. An adequate amount of hemoglobin is vital in any wound healing process. The oxygen that the hemoglobin distributes has a crucial role, such as supplying energy, catalyzing reactive oxygen species, and as a fibroblast signaling molecule in the composition and deposition of collagen. Oxygen supply to the wound tissue becomes a parameter that determines wound healing rates.4
Albumin is just as important as it is a source of amino acids required for wound healing. Amino acids play a role in the wound healing process, especially glutamine and arginine. Glutamine is a metabolic fuel in the process of cell proliferation, while arginine is a component needed for collagen synthesis. Several studies further show that supplementation of arginine, both orally and parenterally, can increase collagen accumulation and increase the activity of leukocyte mitogenesis in peripheral blood circulation. Besides being a proline precursor, arginine is also the only metabolic substrate for the synthesis of nitrite oxide (NO). NO is important for collagen formation in wound tissue.5
The treatment of burn wounds is important in optimizing wound healing. Nearly 90% of burns treated at Hasan Sadikin Hospital require surgery such as debridement, tangential excision, and skin grafting. Out of this percentage, most patients require wound closure by skin graft technique because of the depth of the burn. The rate of wound healing from split-thickness skin graft (STSG) surgery is influenced by serum albumin levels.6
However, there are no studies that mention tolerance levels of albumin in the body that contribute to the success of STSG surgery on burns.6 Albumin levels are still the gold standard in the world, including Indonesia, for surgery such as STSG. On the other hand, for patients with extensive and deep burns, albumin levels are usually low or decreasing.7 In albumin-depleted conditions, interventions are necessary to achieve albumin levels of 2.5 gr% or higher. There are methods to increase albumin level, such as prescribing a long-term high protein diet or albumin infusion.7 However, both methods are considered quite costly. Most cases in Hasan Sadikin Hospital require a long period of time to reach an albumin level of more than 2.5 gr% necessary for surgery. For this reason, it becomes a question for this study to obtain a lower tolerance limit for albumin levels that can still result in a successful STSG. This study seeks to find out the relationship between albumin levels and the outcome of STSG.
Methods
This was a prospective cohort study that took place at the plastic surgery center of Hasan Sadikin Hospital in Bandung, West Java, Indonesia from June 2019 to November 2020. All family or patients were informed about the research project at their first encounter at the surgery department and written consent was obtained. A total of 52 samples from grade 2B and grade 3 burn patients with total body surface area (TBSA) >2% were taken by consecutive sampling technique. The diagnosis of grade 2B and grade 3 burns was based on the classification of burn degrees.8 Inclusion criteria in this study were patients with grade 2B and grade 3 burns with >2% TBSA, aged 14-69 years old, with hemoglobin levels before surgery of >10 g%, and there were no comorbidities and complications.
The patients’ serum albumin levels (gr/dl) were measured before STSG surgery. All study subjects underwent STSG surgery with the same procedure. The skin graft was taken using a humby knife. Donor skin graft was taken from the thigh. After suturing the skin graft at the recipient’s location, the surface area of the transplanted skin graft is drawn on the sterile mica that has been sterilized using a sterile marker. After surgery, an assessment of the graft in the recipient location was carried out on the 7th day post STSG surgery. Review of the result of STSG was carried out on the 7th day after surgery. The surgery is considered as a success if at least 90% of the graft tissue is “taken” from the entire operated tissue. Measurement of the surface area of the graft tissue that “takes” / “does not take” is used measuring mica with units of cm.
Data were analyzed using SPSS ver. 20.0. The normality test was performed using the Saphiro-Wilk test. Data correlation was obtained using Chi Square test. A p-value of <0.05 was regarded as statistically significant. The optimal cut off points for albumin levels that can be successful in STSG surgery on burns were generated by the receiver operating characteristic curve (ROC).
Results
Forty-eight patients with burn injury were enrolled as study subjects. One patient was excluded due to death before the 7th day after surgery. In this study, complete take rate of graft is considered if 90% or more of the graft was successfully taken. Concerning healing of the grafts, 70.21% (33 subjects) of the patients showed complete take rate of the graft, while only 29.79% (14 subjects) of the patients showed incomplete take. The study subjects comprised of 40 male patients (85.11%) and 7 female patients (14.89%) with the characteristics shown in Table I. The etiology of burn included burn from electrical accidents in 21 patients (44.68%), direct flame in 16 patients (34.04%), scald in 7 patients (14.89%), chemical in 2 patients (4.26%) and friction in 1 patient (2.13%) (Table I). Table I shows the mean of variable collected data. Table II shows the relation between serum albumin levels with skin graft take. There was no significant correlation between serum albumin level preoperative and the outcome of graft (p value >0.05). Table III shows the relation between outcome of graft and type of STSG. Fig. 1 shows the age distribution of burn injury patients with low serum albumin level. Fig. 2 shows the age distribution of burn injury patients with normal serum albumin level. Younger patients have normal preoperative albumin. Table IV shows the correlation between serum albumin levels with the percentage of TBSA. There was a significant correlation between preoperative serum albumin level and the percentage of TBSA (p-value <0.05).
Table I. Characteristics of the patients.

Table II. Relation between outcome of graft and preoperative albumin level (N=47).
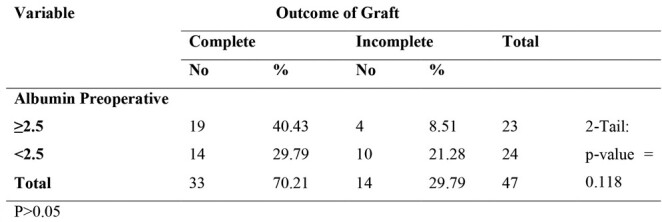
Table III. Relation between outcome of graft and type of STSG (N=47).
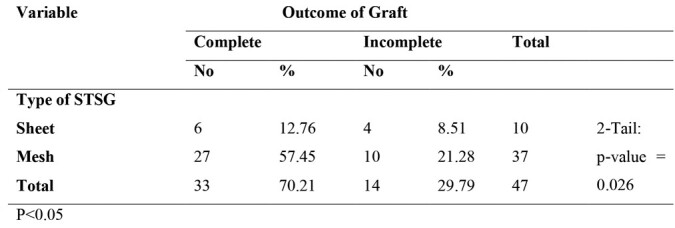
Fig. 1. Age distribution of burn injury patients with preoperative albumin below 2.5 gr/dl.

Fig. 2. Age distribution of burn injury patients with preoperative albumin more than 2.5 gr/dl.
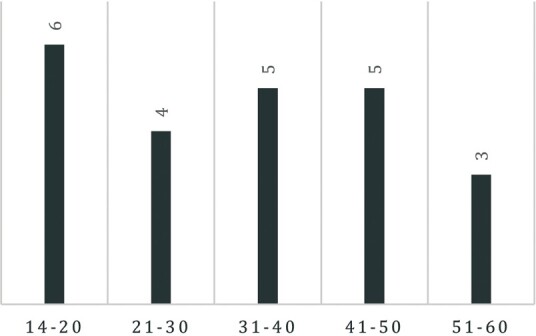
Table IV. Correlation of serum albumin level with percentage of TBSA.

The receiver operating characteristic curve (ROC) for serum albumin levels that marks the success in STSG surgery on burns is shown in Fig. 3.
Fig. 3. ROC curve.
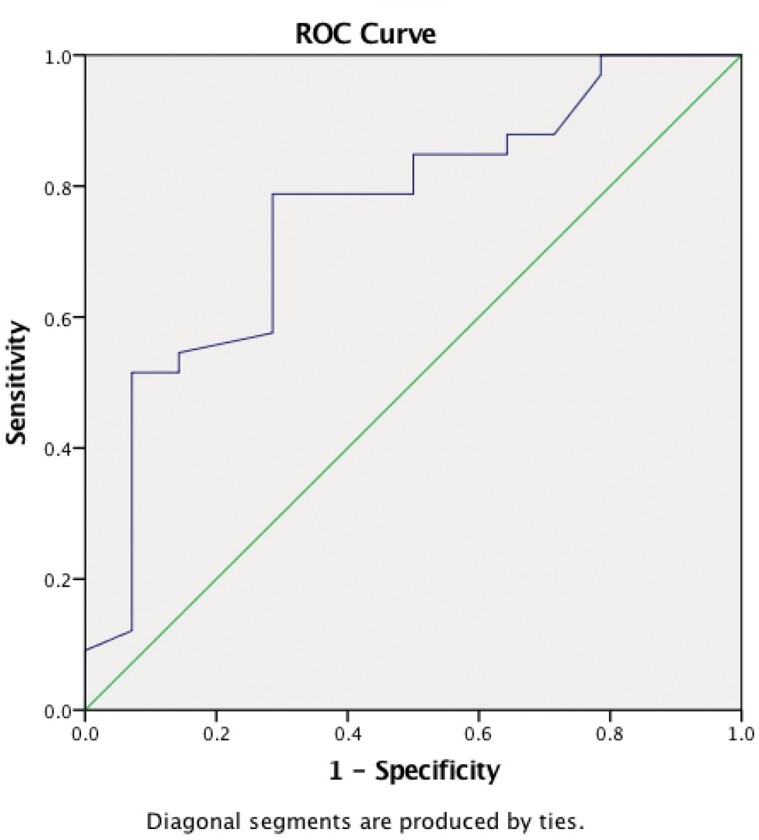
The accuracy of serum albumin level is assessed by the area under the curve (AUC). AUC for preoperative albumin was 0.758; (95% CI: 0.605, 0.910). The optimal cut-off point for albumin levels that can be successful in STSG surgery on burns is 2.175, provided a sensitivity measure of 0.78 and a specificity measure of 0.714 (Table V).
Table V. Sensitivity and specificity of serum albumin.

Discussion
The aim of this study is to assess the relationship between albumin levels with the outcome of STSG and to obtain a cut off point for a tolerance limit for albumin levels that can be successful in STSG surgery on burns. The demographic data show that most of the subjects in this study were male and in the productive age. Studies showed that burn injury patients in Indonesia’s national referral burn center ratio of 1.22:1 between males and females.9 The higher risk for males is associated with open fire cooking while selling food, inherently unsafe cooking stoves, or electrical repair.
In this study, there was no significant correlation of probability of graft “take” with preoperative serum albumin (Tables II-III). This is different from several studies that have been previously conducted. Moghazy et al. confirmed complete graft healing was found in 93.8% of patients with normal preoperative albumin levels (>3.5 gr%) as compared with 44.4% of those with low preoperative albumin levels, who also had longer hospital stays and increased mortality and morbidity, especially in terms of recovery from sepsis.6 Other studies showed albumin correlates with wound healing. Burn injury was related to increasing vascular permeability and hypermetabolism, all of which acts to decrease serum albumin levels.10 While some studies showed preoperative serum albumin level is associated with take rate of graft, it is in fact the preoperative albumin level that is used as a sensitive tool in predicting graft take in burned patients, when all other conditions are optimized and favorable. In this study, preoperative albumin has a significant correlation with age (P = 0.0122). Serum albumin levels are highest in younger patients due to their high nutritional reserve and regeneration capacity, which decreases with age, while levels significantly decrease in patients with chronic disease.11
Serum albumin has various important physiological functions, such as maintenance of colloid osmotic pressure, anticoagulant effects, free radical scavenging, and altering capillary membrane permeability. In addition, hypoalbuminemia results in reduced collagen synthesis and granuloma formation, which impairs the innate immune response. Thus, wound healing is slowed down and the systemic immune status is predisposed to infection.12
While identifying the correlation between preoperative albumin levels and outcome of the graft, the following facts were observed. There were 14 patients out of 47 (29.79%) with low serum preoperative albumin levels who had complete take rate of graft. After a meticulous study while taking the data of these patients, it was found that the patients had a clean wound, which contributed to the increase of graft take rate. From the normal serum preoperative albumin levels, we found 4 of the patients had infection. On the other hand, 10 patients (21.28%) out of 24 with low preoperative albumin serum levels had incomplete take rate of graft. The patients had a burn in different areas. Upon studying the incomplete graft take cases, we found that all these patients suffered from small-sized raw areas. In the case of the other patients, the graft loss was also attributed to a local factor. We also found that low post operative serum albumin might have contributed to the graft loss.
Another possible cause is the use of mesh grafts instead of sheets in some of the patients, particularly those with large surface areas and/or clinically and bacteriological infected wounds. We found that the use of mesh grafts in burns had a better outcome regardless of serum albumin preoperative levels. Successful treatment of wounds relies on precise control and continuous monitoring of the wound-healing process, in this case graft take.13 Table IV shows that there is a significant correlation between the percentage of TBSA and serum preoperative albumin levels. This might guide us to conclude that the preoperative albumin serum level is less sensitive, hence, in some cases, less reliable as a graft-healing indicator. In this study, we found that there is a tolerance limit for albumin levels that can be successful in STSG, which is 2.175, provided a sensitivity of 0.78 and a specificity of 0.714 (Table V). In this study, outcome of the graft did not correlate significantly with albumin levels.
Conclusion
Normal preoperative albumin level is a sensitive means to predict outcome of graft in cases of burns. Nevertheless, local factors should be optimized, such as area to be measured and wound hygiene. Factors leading to normalizing the preoperative albumin level in burned patients should be carefully studied and implemented to assure the most optimum circumstances for graft take.
Further study is needed to assess the relationship between serum albumin level (preoperative and postoperative) with outcome of the graft by assessing the infection status.
References
- 1.Burns. WHO. 2018 Available from: https://www.who.int/news-room/factsheets/detail/burns . [Google Scholar]
- 2.Buja Z, Arifi H, Hoxha E, Duqi S. Surgical treatment of burns sequelae. Our experience in the Department of Plastic and Reconstructive Surgery, Pristina, Kosovo. Ann Burns Fire Disasters. 2015;28(3):205–205. [PMC free article] [PubMed] [Google Scholar]
- 3.Goel A, Shrivastava P. Post-burn scars and scar contractures. Ind J Plast Surg. 2010;43(Suppl):S63–S63. doi: 10.4103/0970-0358.70724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Xie P, Jia S, Tye R, Chavez-Munoz C. Systemic administration of hemoglobin improves ischemic wound healing. J Surg Res. 2015;194(2):696–705. doi: 10.1016/j.jss.2014.10.050. [DOI] [PubMed] [Google Scholar]
- 5.Chow O, Barbul A. Immunonutrition: role in wound healing and tissue regeneration. Adv Wound Care. 2014;3(1):46–53. doi: 10.1089/wound.2012.0415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Moghazy A, Adly O, Abbas A, Moati T. Assessment of the relation between prealbumin serum level and healing of skingrafted burn wounds. Burns. 2010;36(4):495–500. doi: 10.1016/j.burns.2009.05.014. [DOI] [PubMed] [Google Scholar]
- 7.Pérez-Guisado J, de Haro-Padilla JM, Rioja LF, DeRosier LC, de la Torre JI. Serum albumin levels in burn people are associated to the total body surface burned and the length of hospital stay but not to the initiation of the oral/enteral nutrition. Int J Burn Trauma. 2013;3(3):159–159. [PMC free article] [PubMed] [Google Scholar]
- 8.Evers LH, Bhavsar D, Mailänder P. The biology of burn injury. Exp Dermatol. 2010;19(9):777–783. doi: 10.1111/j.1600-0625.2010.01105.x. [DOI] [PubMed] [Google Scholar]
- 9.Wardhana A, Basuki A, Prameswara ADH. The epidemiology of burns in Indonesia’s national referral burn center from 2013 to 2015. Burns Open. 2017;1(2):67–73. [Google Scholar]
- 10.Ishida S, Hashimoto I, Seike T, Abe Y. Serum albumin levels correlate with inflammation rather than nutrition supply in burns patients: a retrospective study. J Med Invest. 2014;61(3.4):361–368. doi: 10.2152/jmi.61.361. [DOI] [PubMed] [Google Scholar]
- 11.Abu-Sittah G, Chahine F, Janom H. Management of burns in the elderly. Ann Burns Fire Disasters. 2016;29(4):249–249. [PMC free article] [PubMed] [Google Scholar]
- 12.Odunayo A. Albumin and colloid osmotic pressure. Monitoring and intervention for the critically ill small animal. 2017;2017:43–53. [Google Scholar]
- 13.Junker JP, Kamel RA, Caterson E, Eriksson E. Clinical impact upon wound healing and inflammation in moist, wet, and dry environments. Adv Wound Care. 2013;2(7):348–356. doi: 10.1089/wound.2012.0412. [DOI] [PMC free article] [PubMed] [Google Scholar]