

Abstract
Background
Women with ST‐segment–elevation myocardial infarction experience delays in reperfusion compared with men with little data on each time component from symptom onset to reperfusion. This study analyzed sex discrepancies in patient delays, prehospital system delays, and hospital delays.
Methods and Results
Consecutive patients with ST‐segment–elevation myocardial infarction treated with percutaneous coronary intervention across 30 hospitals in the Victorian Cardiac Outcomes Registry (2013–2018) were analyzed. Data from the Ambulance Victoria Data warehouse were used to perform linkage to the Victorian Cardiac Outcomes Registry for all patients transported via emergency medical services (EMS). The primary end point was EMS call‐to‐door time (prehospital system delay). Secondary end points included symptom‐to‐EMS call time (patient delay), door‐to‐device time (hospital delay), 30‐day mortality, major adverse cardiovascular events, and major bleeding. End points were analyzed according to sex and adjusted for age, comorbidities, cardiogenic shock, cardiac arrest, and symptom onset time. A total of 6330 (21% women) patients with ST‐segment–elevation myocardial infarction were transported by EMS. Compared with men, women had longer adjusted geometric mean symptom‐to‐EMS call times (47.0 versus 44.0 minutes; P<0.001), EMS call‐to‐door times (58.1 versus 55.7 minutes; P<0.001), and door‐to‐device times (58.5 versus 54.9 minutes; P=0.006). Compared with men, women had higher 30‐day mortality (odds ratio [OR], 1.38; 95% CI, 1.06–1.79; P=0.02) and major bleeding (OR, 1.54; 95% CI, 1.08–2.20; P=0.02).
Conclusions
Female patients with ST‐segment–elevation myocardial infarction experienced excess delays in patient delays, prehospital system delays, and hospital delays, even after adjustment for confounders. Prehospital system and hospital delays resulted in an adjusted excess delay of 10 minutes compared with men.
Keywords: first medical contact, ischemic time, prehospital delay, sex discrepancies, ST‐segment–elevation myocardial infarction
Subject Categories: Mortality/Survival, Quality and Outcomes, Health Services
Nonstandard Abbreviations and Acronyms
- DTD
door‐to‐device
- FMC
first medical contact
- VCOR
Victorian Cardiac Outcomes Registry
Clinical Perspective
What Is New?
Female patients with ST‐segment–elevation myocardial infarction (STEMI) transported to a hospital via emergency medical services have longer patient delays, prehospital healthcare delays, hospital delays, and total healthcare delays (the sum of prehospital healthcare and hospital delays) compared with male patients with STEMI.
Two thirds of the total delay in women result from healthcare delays with female patients with STEMI experiencing an adjusted excess healthcare system delay of 10 minutes compared with men.
This delay likely represents a complex construct of differences in presentation as well as patient and professional bias.
What Are the Clinical Implications?
Specific strategies are needed to address delays in STEMI care for female patients.
Female patients' awareness of their risk of cardiovascular disease and heart attack symptoms should continue to be targeted with public health campaigns.
Education of healthcare professionals on the potential role of sex bias should include all providers involved in STEMI care, from the provider receiving the emergency call to the ambulance officers and interventional cardiologist.
Timely revascularization with percutaneous coronary intervention (PCI) is a critical component of improving outcomes in ST‐segment–elevation myocardial infarction (STEMI).1, 2, 3, 4 During the past decades, major improvements in reperfusion times have been achieved.5, 6 However, healthcare services have focused on improving door‐to‐device (DTD) times, with little impact on system delays that occur before a patient arrives at the hospital.7, 8, 9 The latter can be substantial and is often difficult to assess because of multiple time components.10 Of particular concern has been the finding that women with STEMI have significantly longer ischemic times with delays in reperfusion.11, 12 These delays have been related to both hospital and prehospital delays.13, 14, 15, 16 Prehospital delays consist of the time from STEMI symptom onset to arrival at the door of a PCI‐capable hospital. They consist of a patient's delay from symptom onset until first medical contact (FMC) and a prehospital healthcare delay from FMC until arrival at a hospital. In particular, patient delays for women have been targeted by public awareness campaigns to increase women's early recognition of myocardial infarction symptoms and the need to activate emergency services.15, 17 In patients with STEMI who travel via emergency medical services (EMS), the prehospital healthcare times are made up of multiple components, including EMS call to arrival time and ECG acquisition, scene time, and scene‐to‐door time.8 Delays at each point can result in reperfusion delays and longer ischemic times. Sex differences in each component of the symptom‐to‐door time have not been well studied.
We therefore aimed to assess sex differences in prehospital delays in patients with STEMI transported by EMS and their impact on clinical outcomes. This is of critical importance as we need to identify the reasons for delays still observed in women with STEMI to design and implement strategies to overcome them.
Methods
Data Availability Statement
Because of the sensitive nature of the data collected for this study, requests to access the data set from qualified researchers trained in human subject confidentiality protocols may be sent to the VCOR (Victorian Cardiac Outcomes Registry) Data Access, Research and Publications Committee at vcor@monash.edu.
Study Design and Patient Population
From 2013 to 2018, consecutive patients treated with PCI for STEMI were prospectively enrolled into the VCOR. VCOR is an Australian, state‐based clinical quality registry designed to monitor the performance and outcomes of PCI in Victoria. VCOR was established in 2012 and is engaged at 30 Victorian hospitals (13 public [ie, government funded] and 17 private) with all patients undergoing successful or attempted PCI entered into the registry.18 VCOR collects baseline demographic, procedural characteristics, in‐hospital, and 30‐day outcomes on all patients who undergo PCI at a given facility through a secure web‐based data collection system.19 Data integrity is ensured with regular audit activities conducted by the central registry. VCOR is funded by the Victorian Department of Health and Human Services.
Data from the Ambulance Victoria Data warehouse were used to perform data set linkage to VCOR for all patients with STEMI. Ambulance Victoria is the statewide EMS in Victoria, Australia, covering 227 000 km2 with a population of >6.3 million residents. Paramedics in Victoria complete an electronic patient care record at the conclusion of each case, including timestamps from receipt of the phone call to the Triple Zero (000) emergency number until off stretcher at the hospital. Data from these records and the computer‐aided dispatch system are uploaded into a data warehouse.20 Most Ambulance Victoria paramedics are trained to the advanced life support level. Mobile intensive care ambulance paramedics have a higher clinical skill set and provide advanced management of cardiac conditions. Until 2016, only mobile intensive care ambulance EMS were equipped with monitors capable of 12‐lead ECGs, and all other advanced life support paramedics carried monitors capable of 3‐lead ECGs. In 2016, all paramedics in Victoria were equipped with monitors capable of 12‐lead ECGs and wireless transmission technology.
To obtain patient socioeconomic status, residential postcodes recorded in VCOR were linked with the Index of Relative Socioeconomic Disadvantage developed by the Australian Bureau of Statistics from data collected in the national census in 2016. Each postcode is allocated an Index of Relative Socioeconomic Disadvantage score based on a weighted combination of factors including household income, unemployment rate, and home and vehicle ownership, with a low score indicating high socioeconomic disadvantage. All postcodes in the state of Victoria are ranked according to Index of Relative Socioeconomic Disadvantage score and classified by deciles.21, 22
The study was approved by the Institutional Human Research Ethics Committee with an opt‐out consent.
Inclusion and Exclusion Criteria
Consecutive patients who were transported to a hospital by Ambulance Victoria and received successful or attempted PCI for a STEMI were included. At the time of entering the patient into the VCOR database, STEMI was defined as elevated biomarkers and new or presumed new ST‐segment elevation in ≥2 contiguous leads. The clinical definition was based on the Fourth Universal Definition of Myocardial Infarction.23 Preprocedural creatinine was collected up to 60 days before the PCI, and the Cockcroft‐Gault formula was used to determine estimated glomerular filtration rate. Left ventricular ejection fraction (LVEF) was collected during the index admission. Normal LVEF was defined as LVEF>50%, moderate dysfunction as LVEF 35% to 44%, and severe dysfunction as LVEF<35%. New heart failure was defined as LVEF<45% with clinical evidence of heart failure. Complex lesions included type B2 and C lesions according to the American College of Cardiology/American Heart Association classification guidelines.
Only patients in whom VCOR and Ambulance Victoria data linkage was performed were included. Patients were excluded if they had (1) missing time data, (2) symptom onset while already admitted to hospital, (3) presented after 12 hours from symptom onset, (4) underwent thrombolysis before PCI, or (5) were transported by Ambulance Victoria after the PCI (and not before). Specifically, for the analysis of DTD time, patients were excluded if they were transferred to a non–PCI‐capable hospital and thereafter underwent interhospital transfer (Figure 1).
Figure 1. Inclusion and exclusion criteria.
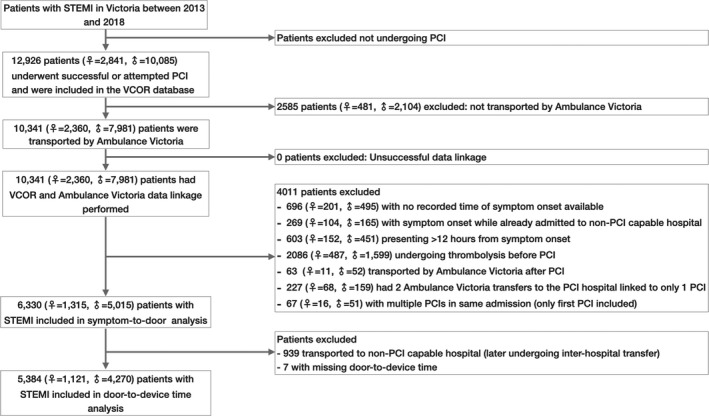
Overview of the patients included. A total of 6330 patients (21% women) were included in the final analysis for baseline criteria, outcomes, and symptom‐to‐door time; 5384 patients were included for door‐to‐device time analysis. PCI indicates percutaneous coronary intervention; STEMI, ST‐segment–elevation myocardial infarction; and VCOR, Victorian Cardiac Outcome Registry.
Definition of Time Intervals
Figure 2 gives an overview of the ischemic time spans and delays assessed.
Figure 2. Overview of time intervals from symptom onset to reperfusion.
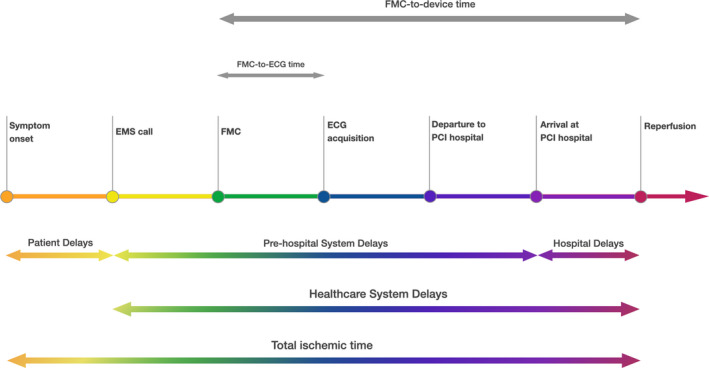
Overview of the ischemic time spans and delays assessed. The primary end point was EMS call‐to‐door time (prehospital EMS‐related system delay). Secondary end points included each component of the prehospital system delay as well as the patient, hospital, and healthcare delays. EMS indicates emergency medical services; FMC, first medical contact; and PCI, percutaneous coronary intervention.
Time Spans
Symptom‐to‐EMS call time was defined as time from STEMI symptom onset recorded in the medical records to the time when Ambulance Victoria received the first call, which was recorded in the computer‐aided dispatch system. Ambulance arrival at scene was used as FMC. EMS call‐to‐FMC time was defined as the time interval between Ambulance Victoria receiving the first phone call until arrival of the first team at the scene. FMC‐to‐ECG time was defined as time interval from arrival of the first team at the scene to acquisition of a 12‐lead ECG. The time of ECG acquisition was used as time of STEMI diagnosis. ECG‐to‐departure time was defined as time from acquisition of a 12‐lead ECG to departure from the scene. Scene time was defined as the entire time spent with the patient at their pick‐up location, from FMC to departure time of the transporting team. Departure‐to‐door time was defined as time from departure from the scene to arrival at the PCI‐capable hospital. DTD time was defined as time from arrival at the PCI‐capable hospital to time of reperfusion of the culprit coronary artery. Total ischemic time was defined as time from symptom onset to reperfusion of the culprit artery.
Time Delays
Patient delay was defined as symptom‐to‐EMS call time. Prehospital system delays were defined as the timespan between the phone call to Ambulance Victoria until arrival at the PCI‐capable hospital (EMS call‐to‐door time). Hospital delay was defined as DTD time. Healthcare delay was the sum of prehospital system delay and hospital delay.
Guideline‐Recommended Times
The FMC‐to‐device time was defined as time from EMS arrival at the scene until reperfusion of the culprit artery.4 The FMC‐to‐ECG time was defined as time from EMS arrival at the scene until acquisition of an ECG.2
Primary and Secondary Outcomes
The primary end point was EMS call‐to‐door time (prehospital EMS‐related system delay). Secondary end points included each component of the prehospital system delay as well as the patient, hospital system, and healthcare delays (Figure 2). Secondary outcomes included 30‐day all‐cause mortality, major adverse cardiovascular events (consisting of all‐cause death, new or recurrent myocardial infarction, stent thrombosis, or target vessel revascularization), major adverse cardiovascular and cerebrovascular events (consisting of major adverse cardiovascular events and stroke), major bleeding (consisting of types 3 and 5 according to the Bleeding Academic Research Consortium definition),24 recurrent myocardial infarction, new heart failure (defined according to clinical signs), and new renal impairment.
According to the American College of Cardiology/American Heart Association guidelines, the percentage of patients who were transported to a PCI‐capable facility achieving an FMC‐to‐device time of ≤90 minutes was calculated and compared between sexes.4 According to the European Society of Cardiology guidelines, the percentage of patients achieving an FMC‐to‐ECG time of ≤10 minutes was compared between sexes.2
Statistical Analysis
VCOR and Ambulance Victoria data linkage was performed with prehospital care records captured electronically by Ambulance Victoria using identifier variables (names, date of birth, date of hospital arrival). Match scores >0.75 were assumed to be true. Associations in categorical variables were analyzed with chi‐square or Fisher exact tests as appropriate and expressed as number and percentage. Continuous variables were analyzed with t tests and expressed as mean and standard deviation. Univariable and multivariable associations with sex were determined by logistic regression. Because the distributions of times were highly skewed, their data were log‐transformed for analysis and then back‐transformed to determine an estimated geometric mean. The geometric mean was adjusted for age, diabetes mellitus, estimated glomerular filtration rate, previous PCI and/or coronary artery bypass grafting, history of peripheral vascular disease and cerebrovascular disease, LVEF, cardiogenic shock, out‐of‐hospital cardiac arrest requiring intubation, and time of symptom onset (night versus day). The same variables were determined a priori to be included in the multivariable models. The variables forced into and retained in the models were determined based on prior literature and experience that these factors are known to influence major adverse cardiovascular events and all‐cause mortality. Statistical analyses were performed using Stata version 16 with P<0.05 considered statistically significant.
Results
Baseline, Procedural, and Discharge Data
A total of 12 926 patients with STEMI underwent successful or attempted PCI and were included in the VCOR database. Of these, 10 341 patients (23% female) were transported by Ambulance Victoria and were successfully linked with Ambulance Victoria data. Figure 1 gives an overview of the patients: 6330 patients (21% female) were included in the final analysis for baseline criteria, outcomes, and symptom‐to‐door time; 5384 patients were included for DTD time analysis. Table 1 shows baseline, procedural, and discharge characteristics. Female patients were significantly older and had more comorbidities than male patients. There was no sex difference in socioeconomic status. Radial access was used significantly less often in female than male patients. Female patients received significantly lower rates of secondary prevention medications compared with male patients.
Table 1.
Baseline and Discharge Characteristics According to Sex
| Total Patients With STEMI, n=6330 | Female Patients, n=1315 | Male Patients, n=5015 | P Value | |
|---|---|---|---|---|
| Age, y | 62.9±12.8 | 68.4±13.3 | 61.5±12.3 | <0.001 |
| Low socioeconomic status | 1207 (19.4) | 273 (21.0) | 934 (19.0) | 0.09 |
| BMI, kg/m2 | 27.5 (24.7–30.8) | 27.1 (23.5–31.1) | 27.7 (24.9–30.6) | <0.001 |
| Diabetes mellitus | 1002 (15.8) | 236 (17.9) | 766 (15.3) | 0.02 |
| eGFR ≤45 mL/min | 493 (7.8) | 239 (18.2) | 254 (5.1) | <0.001 |
| Moderate–severe LVEF impairment | 1720 (29.1) | 332 (27.3) | 1388 (29.5) | 0.13 |
| Previous CABG and/or PCI | 820 (13.0) | 123 (9.4) | 697 (13.9) | <0.001 |
| Cerebrovascular disease | 223 (3.5) | 65 (4.9) | 158 (3.2) | 0.002 |
| Peripheral vascular disease | 139 (2.2) | 34 (2.6) | 105 (2.1) | 0.28 |
| Oral anticoagulant therapy | 173 (2.7) | 49 (3.7) | 124 (2.5) | 0.01 |
| Onset of symptoms 7 am to 8 pm | 4128 (65.2) | 836 (63.6) | 3292 (65.6) | 0.16 |
| Cardiogenic shock or cardiac arrest requiring intubation | 758 (12.0) | 150 (11.4) | 608 (12.1) | 0.48 |
| Radial access | 3506 (55.4) | 640 (48.7) | 2866 (57.1) | <0.001 |
| PCI success | 5958 (94.1) | 1229 (93.5) | 4729 (94.3) | 0.25 |
| Glycoprotein IIb/IIIa inhibitor | 2374 (37.5) | 425 (32.3) | 1949 (38.9) | <0.001 |
| Mechanical ventricular support | 191 (3.0) | 19 (1.4) | 172 (3.4) | <0.001 |
| Referral to cardiac rehabilitation | 4987 (78.8) | 995 (75.7) | 3992 (79.6) | 0.002 |
| Discharge medication | ||||
| Aspirin | 5784 (98.1) | 1171 (97.8) | 4613 (98.2) | 0.41 |
| Thienopyridine | 1554 (26.4) | 355 (29.7) | 1199 (25.5) | 0.004 |
| Ticagrelor | 4219 (71.6) | 811 (67.9) | 3408 (72.6) | 0.001 |
| β‐blockers | 5132 (87.2) | 1014 (84.9) | 4118 (87.8) | 0.008 |
| ACEI/ARB | 4956 (84.2) | 977 (81.8) | 3979 (84.9) | 0.010 |
| Statin | 5702 (96.8) | 1128 (94.4) | 4574 (97.4) | <0.001 |
Data are presented as number (percentage), mean±SD, or median (interquartile range). LVEF data were available in 93% of cases. ACEI indicates angiotensin‐converting enzyme inhibitor; ARB, angiotensin receptor blockers; BMI, body mass index; CABG, coronary artery bypass grafting; eGFR, estimated glomerular filtration rate; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; and STEMI, ST‐segment–elevation myocardial infarction.
EMS Data
Ambulance Victoria use rates were 83% in female patients and 79% in male patients in the entire VCOR cohort (before database matching; odds ratio [OR], 1.29; 95% CI, 1.16–1.44; P<0.001; not shown in tables). Ambulance Victoria data including prehospital ECG notification, proportion with transport to a non–PCI‐capable hospital, and unit skill set are displayed in Table 2. Prehospital ECG notification was performed in 61.9% of female patients compared with 65.1% of male patients (P=0.032).
Table 2.
Ambulance Data According to Sex
| Total Patients, n=6330 | Female Patients, n=1315 | Male Patients, n=5015 | P Value | |
|---|---|---|---|---|
| Prehospital ECG notification | 4080 (64.5) | 814 (61.9) | 3266 (65.1) | 0.032 |
| Ambulance transport to non–PCI‐capable hospital | 939 (14.8) | 194 (14.8) | 745 (14.9) | 0.93 |
| Unit skill set | ||||
| MICA, 2013–2015 | 1687/2252 (74.9)* | 335/467 (71.7)* | 1352/1785 (75.7)* | 0.062 |
| MICA, 2016–2018 | 1805/4078 (44.2)* | 350/848 (41.2)* | 1455/3230 (45.0)* | 0.052 |
Data are presented as number (percentage). MICA indicates mobile intensive care ambulance; and PCI, percutaneous coronary intervention.
Number of patients transported by MICA/total patients, in each respective time period.
Time Analyses
Patient, prehospital, and hospital delays are displayed in Table 3 and Figure 3.
Table 3.
Geometric Mean Time Delays According to Sex*
| Number | Geometric Mean Unadjusted | 95% CI | P Value | Geometric Mean Adjusted | 95% CI | P Value | |
|---|---|---|---|---|---|---|---|
| Symptom‐to‐call time, min | |||||||
| Female patients | 1315 | 51.7 | 47.7–56.0 | <0.001 | 47.0 | 43.0–51.3 | <0.001 |
| Male patients | 5015 | 45.9 | 44.1–47.8 | 44.0 | 41.7–46.4 | ||
| Call‐to‐door time, min | |||||||
| Female patients | 1315 | 61.3 | 60.1–62.5 | <0.001 | 58.1 | 56.9–59.4 | <0.001 |
| Male patients | 5015 | 58.0 | 57.4–59.0 | 55.7 | 55.0–56.4 | ||
| Call‐to‐FMC time, min | |||||||
| Female patients | 1315 | 12.0 | 11.6–12.4 | <0.001 | 11.6 | 11.2–12.0 | 0.01 |
| Male patients | 5015 | 11.2 | 11.0–11.4 | 11.0 | 10.8–11.3 | ||
| FMC‐to‐ECG time, min | |||||||
| Female patients | 1315 | 4.03 | 3.82–4.23 | 0.06 | 3.98 | 3.77–4.21 | 0.48 |
| Male patients | 5015 | 3.82 | 3.72–3.92 | 3.90 | 3.77–4.21 | ||
| ECG‐to‐departure time, min | |||||||
| Female patients | 1315 | 20.18 | 19.37–21.03 | <0.001 | 18.32 | 17.53–19.15 | 0.002 |
| Male patients | 5015 | 18.49 | 18.10–18.88 | 17.05 | 16.59–17.52 | ||
| Total scene time, min | |||||||
| Female patients | 1315 | 24.3 | 23.6–25.1 | <0.001 | 22.2 | 21.5–23.0 | <0.001 |
| Male patients | 5015 | 22.4 | 22.0–22.8 | 20.8 | 20.4–21.3 | ||
| Departure‐to‐door time, min | |||||||
| Female patients | 1315 | 18.5 | 17.9–19.2 | 0.59 | 18.5 | 17.9–18.8 | 0.68 |
| Male patients | 5015 | 18.3 | 18.0–18.7 | 18.3 | 17.8–19.2 | ||
| Door‐to‐device time, min* | |||||||
| Female patients | 1121 | 68.2 | 65.5–70.1 | <0.001 | 58.5 | 56.0–61.2 | 0.006 |
| Male patients | 4270 | 61.7 | 60.4–62.3 | 54.9 | 53.4–56.4 | ||
| Call‐to‐device time, min* | |||||||
| Female patients | 1121 | 152.5 | 148.0–157.2 | <0.001 | 137.2 | 132.8–141.8 | <0.001 |
| Male patients | 4270 | 136.3 | 134.2–138.4 | 127.2 | 124.6–129.8 | ||
| Total ischemic time* | |||||||
| Female patients | 1121 | 231.3 | 223.7–239.2 | <0.001 | 207.00 | 199.5–214.7 | <0.001 |
| Male patients | 4270 | 205.0 | 201.5–208.6 | 190.52 | 186.3–194.9 | ||
Adjusted for age, diabetes mellitus, previous coronary artery bypass grafting and/or percutaneous coronary intervention, peripheral vascular and/or cerebrovascular disease, time of symptom onset (categorized as shown) and cardiogenic shock. Values are exponentiated regression coefficients. Adjusted values are for population mean age (62.9 years). FMC indicates first medical contact.
Only in patients who were initially transported to a percutaneous coronary intervention–capable hospital.
Figure 3. Sex discrepancies in patient, prehospital, and hospital reperfusion delays in patients with STEMI transported by EMS.
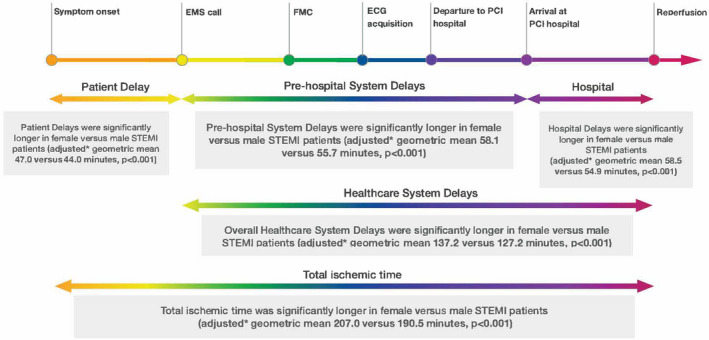
All unadjusted and adjusted geometric means for patient delays, prehospital system delays, and hospital delays were significantly longer in women than men. EMS indicates emergency medical services; FMC, first medical contact; PCI, percutaneous coronary intervention; and STEMI, ST‐segment–elevation myocardial infarction. *Adjusted for age, diabetes mellitus, estimated glomerular filtration rate, previous PCl/coronary artery bypass grafting, history of peripheral vascular disease and cerebrovascular disease, left ventricular ejection fraction, cardiogenic shock or out‐ofhospital cardiac arrest requiring intubation, and occurrence time of symptom onset (day vs night).
Patient Delay (Symptom‐to‐EMS Call Time)
Both unadjusted and adjusted geometric mean symptom‐to‐EMS call times were significantly longer in women compared with men (adjusted, 47.0 versus 44.0 minutes; P<0.001).
Primary End Point: Prehospital System Delay (EMS Call‐to‐Door Time)
Both unadjusted and adjusted geometric mean EMS call‐to‐door times were significantly longer in women than men (adjusted, 58.1 versus 55.7 minutes; P<0.001). Adjusted geometric mean for EMS call‐to‐FMC, ECG‐to‐departure, and total scene time were significantly longer in women than men. There were no sex differences in the adjusted geometric mean for FMC‐to‐ECG time and departure‐to‐door time.
Hospital Delay (DTD Time)
Both unadjusted and adjusted geometric mean DTD times were significantly longer in women than men (adjusted, 58.5 versus 54.9 minutes; P<0.006).
Total Healthcare Delay (EMS Call‐to‐Device Time)
Both unadjusted and adjusted geometric healthcare delays were significantly longer in women than men (adjusted, 137.2 versus 127.2 minutes; P<0.001).
Total Ischemic Time (Symptom‐to‐Device Time)
Both unadjusted and adjusted geometric total ischemic times were significantly longer in women than men (adjusted, 207.0 versus 190.5 minutes; P<0.001).
Guideline‐recommended times achieved are displayed in Figure 4.
Figure 4. Sex discrepancies in achieved guideline‐recommended times.
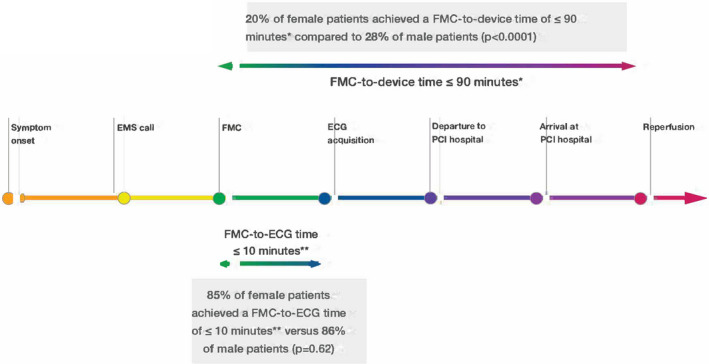
The achieved guideline‐recommended times are outlined. The percentage of female patients who were transported to a PCI‐capable facility achieving a first medical contact‐to‐device time of ≤90 minutes was 20.2% compared with 27.6% of male patients (P<0001). EMS indicates emergency medical services; FMC, first medical contact; and PCI, percutaneous coronary intervention. *According to American Heart Association/American College of Cardiology guidelines.4 **According to European Society of Cardiology guidelines.2
FMC‐to‐ECG Time
Equal proportions of female and male patients with STEMI achieved an FMC‐to‐ECG time ≤10 minutes2 (85.1% versus 85.6%; P=0.62).
FMC‐to‐Device Time
The percentage of female patients who were transported to a PCI‐capable facility achieving a FMC‐to‐device time of ≤90 minutes4 was 20.2% compared with 27.6% of male patients (P<0001).
Clinical Outcomes
shows the 30‐day clinical outcomes. Female patients compared with male patients had higher unadjusted 30‐day major adverse cardiovascular events (12.0% versus 9.1%), all‐cause mortality (9.8% versus 6.7%), major adverse cardiovascular and cerebrovascular events (12.5% versus 9.6%), major bleeding (3.8% versus 2.2%), new heart failure (2.2% versus 1.4%), and new renal impairment (8.1% versus 6.0%). After adjustment for confounders, 30‐day all‐cause mortality (OR, 1.38; 95% CI, 1.06–1.79; P=0.02) and major bleeding (OR, 1.54; 95% CI, 1.08–2.20; P=0.02) were higher in women versus men.
Table 4.
Adjusted and Unadjusted Outcomes According to Sex
| 30‐Day Outcomes | Overall STEMI (n=6330) | Female Patients (n=1315) | Male Patients (n=5015) | Unadjusted P Value | Odds Ratio | 95% CI | Adjusted* P Value |
|---|---|---|---|---|---|---|---|
| MACE | 615 (9.7) | 158 (12.0) | 457 (9.1) | 0.002 | 1.2 | 0.96–1.50 | 0.11 |
| All‐cause mortality | 464 (7.3) | 129 (9.8) | 335 (6.7) | <0.001 | 1.38 | 1.06–1.79 | 0.02 |
| MACCE | 646 (10.2) | 165 (12.5) | 481 (9.6) | 0.002 | 1.2 | 0.96–1.49 | 0.11 |
| Major bleeding | 158 (2.5) | 50 (3.8) | 108 (2.2) | <0.001 | 1.54 | 1.08–2.20 | 0.02 |
| New heart failure | 101 (1.6) | 29 (2.2) | 72 (1.4) | 0.047 | 1.28 | 0.82–2.01 | 0.28 |
| Recurrent MI | 89 (1.4) | 22 (1.7) | 67 (1.3) | 0.36 | 1.15 | 0.70–1.89 | 0.58 |
| New renal impairment | 394 (6.4) | 103 (8.1) | 291 (6.0) | 0.005 | 1.12 | 0.88–1.44 | 0.36 |
Data are presented as number (percentage). MACCE indicates major cardiovascular and cerebrovascular events; MACE, major cardiovascular events; MI, myocardial infarction; and STEMI, ST‐segment–elevation myocardial infarction.
Adjustment was made for patient age, comorbidities, cardiogenic shock, intubation and out‐of‐hospital cardiac arrest, and time of symptom onset (day vs night).
Discussion
The present study investigated differences in time delays in female versus male patients presenting with STEMI transported to hospital by EMS. The principal findings of our study are that female patients with STEMI (1) have longer patient delays, prehospital healthcare delays, hospital delays, and total healthcare delays compared with male patients with STEMI; (2) have time delays that persisted after adjustment for confounders; (3) have two thirds of the total delays resulting from healthcare delays (female patients with STEMI experienced an adjusted excess healthcare system delay of 10 minutes compared with men); and (4) have higher 30‐day all‐cause mortality and major bleeding after adjustment for confounders.
Timely revascularization is of critical importance in patients with STEMI. Women are reported to experience delays in revascularization; however, different results have been published as to from where these delays arise.12, 13, 14, 25, 26 Delays can occur at any stage from symptom onset until definitive treatment is performed and can include patient delays and healthcare system delays. As far as we are aware, our publication is the first to investigate sex differences in all time intervals from EMS call to arrival at the hospital door and subsequent PCI.
Sources of Delay
Our STEMI cohort consisted of 21% female patients who were older and had more comorbidities compared with male patients. We found that female patients experienced delays compared with male patients at most stages from symptom onset to revascularization. Previous studies had reported that the driver for female patients' longer ischemic times was the patient delay itself.13, 14, 25 Our results confirm that female patients experience significant delays from time of symptom onset to calling EMS despite more women ultimately using EMS transport than men. Female patients may misinterpret their symptoms as noncardiac or not visit a healthcare provider because of engagements in caregiver roles.26, 27 Further causes are lower socioeconomic status of women with associated lower risk perception for heart disease as well as gender issues.27, 28 Comparison of time intervals to other literature is difficult because our patient cohort only included patients who were transported by EMS. This means that women in our cohort were more likely to consider their symptoms as suspicious, prompting the call of EMS.
Although patient delays are important, we found that the largest component of time delay in women with STEMI was actually healthcare system delays (prehospital system and hospital delays). In fact, only 20% of women achieved a FMC‐to‐device time of ≤90 minutes. Although hospital delays in women are known, significant delays in women transported by EMS have not been previously described. We know that female patients with myocardial infarction have higher rates of associated symptoms such as nausea, radiation of pain, and shortness of breath.26, 29 Healthcare providers have also been shown to be less likely to attribute women's symptoms to a STEMI compared with men.26, 27, 30 This may lead to an initial misdiagnosis at the time of EMS phone call and the delay in EMS call‐to‐FMC seen in women. However, longer healthcare delays have been described even in women with typical symptoms, suggesting a healthcare worker bias may still exist with women perceived as lower risk for STEMI.27 Interestingly, the FMC‐to‐ECG time was similar between male and female patients with STEMI, an observation that has been previously described.26 Of both female and male patients with STEMI, 85% achieved a FMC‐to‐ECG time of ≤10 minutes. This is not surprising given that EMS paramedics are highly trained and work according to clinical practice guidelines,31 which have been demonstrated to reduce or even avoid sex discrepancies in treatments.32
The ECG‐to‐departure time was again significantly longer in female compared with male patients. This is unexpected given the fact that female and male patients were equally as often transported by mobile intensive care ambulance and advanced life support EMS, and hence the opportunity to diagnose a STEMI at the scene was similar in both women and men. However, the detection of a STEMI pattern on the ECG may be more challenging in women because of the lower baseline J‐point elevation in healthy women compared with men, leading to less‐prominent ST‐segment elevation in case of a STEMI.2, 33 Similarly, previous literature reported reperfusion delays in women even after adjusting for the presence of more subtle ECG characteristics.34
We also found a significant difference for the hospital delay (ie, DTD time) between female and male patients. This is despite similar proportions of female and male patients transported to a PCI‐capable hospital, from which we can infer that a STEMI or at least an acute coronary syndrome was suspected in all of these patients.35 One explanation could be that prehospital ECG notification was lower in female patients, with prehospital ECG transmission known to be associated with shorter DTD times9, 36 because they can facilitate direct access to the catheterization laboratory with bypassing of the emergency department. However, this factor alone is unlikely to account for the delay in women, with a previous study demonstrating female patients had longer FMC‐to‐device times than men, regardless of prehospital ECG transmission.16
Ways to Improve Revascularization Delays in Women
First, we must continue to increase female patients' awareness of their risk of cardiovascular disease and the possible symptoms of a heart attack with public campaigns. More so, we have to increase healthcare providers' awareness for the likelihood of STEMI in female patients, particularly in the setting of atypical or associated symptoms and more subtle ECG findings. Education of healthcare professionals on the role of sex bias should extend from the call center provider responding to the emergency call to the interventional cardiologist activating the emergency cardiac catheterization team. Checklist‐based approaches are known to reduce sex gaps in the treatment of STEMI and should be incorporated at different stages.32 Artificial intelligence and machine learning could also contribute to reducing implicit bias originating from healthcare providers.37
Limitations
Our study has certain limitations. First, this is a retrospective analysis and despite correcting for potential confounders, only variables that are included in the registry can be adjusted for. Second, our registry only captures patients with STEMI treated with PCI, hence we cannot comment on sex differences of patients with STEMI who do not undergo revascularization, and therefore cannot exclude selection and survivor bias. However, it is well known that women with STEMI are less likely to undergo PCI,38 which would only strengthen our results because patients with STEMI not taken to the catheterization laboratory are likely to have an even poorer outcome. Furthermore, only patients who were transported by Ambulance Victoria were included in the data analysis; therefore, we cannot comment on prehospital time discrepancies in all‐comer patients with STEMI. However, data on that have previously been published,13 and the intention of this work was to specifically analyze a homogeneous cohort of patients who were transported by EMS with regard to prehospital healthcare system delays.
Conclusions
In conclusion, despite guideline‐based assessment and treatment pathways through EMS, there are still sex discrepancies with significant patient, prehospital, and hospital reperfusion delays in female patients with STEMI. This likely represents a complex construct of differences in symptoms and ECG changes as well as patient and professional bias, which all require specific strategies to address.
Sources of Funding
None.
Disclosures
Dr Stehli is supported by a Monash University Scholarship. Associate Professor Stub receives a National Heart Foundation Fellowship. Associate Professor Duffy is supported by a National Health and Medical Research Council of Australia grant (No. 1111170). Associate Professor Zaman is supported by a National Heart Foundation Fellowship. She has also obtained research funding from Abbott Vascular and Biotronik Australia and speaking honoraria or consulting fees from AstraZeneca, Amgen, and Medtronic Australia. Dr Nehme is supported by a National Health and Medical Research Council Early Career Fellowship (No. 1146809). The remaining authors have no disclosures to report.
(J Am Heart Assoc. 2021;10:e019938. DOI: 10.1161/JAHA.120.019938.)
For Sources of Funding and Disclosures, see page 10.
REFERENCES
- 1.Cannon CP, Gibson CM, Lambrew CT, Shoultz DA, Levy D, French WJ, Gore JM, Weaver WD, Rogers WJ, Tiefenbrunn AJ. Relationship of symptom‐onset‐to‐balloon time and door‐to‐balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000;283:2941–2947. DOI: 10.1001/jama.283.22.2941. [DOI] [PubMed] [Google Scholar]
- 2.Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli‐Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, ESC Scientific Document Group , et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. DOI: 10.1093/eurheartj/ehx393. [DOI] [PubMed] [Google Scholar]
- 3.Park J, Choi KH, Lee JM, Kim HK, Hwang D, Rhee TM, Kim J, Park TK, Yang JH, Song YB, et al. Prognostic implications of door‐to‐balloon time and onset‐to‐door time on mortality in patients with ST‐segment‐elevation myocardial infarction treated with primary percutaneous coronary intervention. J Am Heart Assoc. 2019;8:e012188. DOI: 10.1161/JAHA.119.012188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.O'Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, CF/AHA Task Force , et al. 2013 ACCF/AHA guideline for the management of ST‐elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:529–555. DOI: 10.1161/CIR.0b013e3182742c84. [DOI] [PubMed] [Google Scholar]
- 5.Krumholz HM, Herrin J, Miller LE, Drye EE, Ling SM, Han LF, Rapp MT, Bradley EH, Nallamothu BK, Nsa W, et al. Improvements in door‐to‐balloon time in the United States, 2005 to 2010. Circulation. 2011;124:1038–1045. DOI: 10.1161/CIRCULATIONAHA.111.044107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Brennan AL, Andrianopoulos N, Duffy SJ, Reid CM, Clark DJ, Loane P, New G, Black A, Yan BP, Brooks M, et al. Trends in door‐to‐balloon time and outcomes following primary percutaneous coronary intervention for ST‐elevation myocardial infarction: an Australian perspective. Intern Med J. 2014;44:471–477. DOI: 10.1111/imj.12405. [DOI] [PubMed] [Google Scholar]
- 7.Spencer FA, Montalescot G, Fox KA, Goodman SG, Granger CB, Goldberg RJ, Oliveira GB, Anderson FA, Eagle KA, Fitzgerald G, et al. Delay to reperfusion in patients with acute myocardial infarction presenting to acute care hospitals: an international perspective. Eur Heart J. 2010;31:1328–1336. DOI: 10.1093/eurheartj/ehq057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Alrawashdeh A, Nehme Z, Williams B, Stub D. Emergency medical service delays in ST‐elevation myocardial infarction: a meta‐analysis. Heart. 2020;106:365–373. DOI: 10.1136/heartjnl-2019-315034. [DOI] [PubMed] [Google Scholar]
- 9.Hutchison AW, Malaiapan Y, Jarvie I, Barger B, Watkins E, Braitberg G, Kambourakis T, Cameron JD, Meredith IT. Prehospital 12‐lead ECG to triage ST‐elevation myocardial infarction and emergency department activation of the infarct team significantly improves door‐to‐balloon times: ambulance Victoria and MonashHEART Acute Myocardial Infarction (MonAMI) 12‐lead ECG project. Circ Cardiovasc Interv. 2009;2:528–534. DOI: 10.1161/CIRCINTERVENTIONS.109.892372. [DOI] [PubMed] [Google Scholar]
- 10.Dracup K, McKinley S, Riegel B, Moser DK, Meischke H, Doering LV, Davidson P, Paul SM, Baker H, Pelter M. A randomized clinical trial to reduce patient prehospital delay to treatment in acute coronary syndrome. Circ Cardiovasc Qual Outcomes. 2009;2:524–532. DOI: 10.1161/CIRCOUTCOMES.109.852608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wilkinson C, Bebb O, Dondo TB, Munyombwe T, Casadei B, Clarke S, Schiele F, Timmis A, Hall M, Gale CP. Sex differences in quality indicator attainment for myocardial infarction: a nationwide cohort study. Heart. 2019;105:516–523. DOI: 10.1136/heartjnl-2018-313959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bugiardini R, Ricci B, Cenko E, Vasiljevic Z, Kedev S, Davidovic G, Zdravkovic M, Milicic D, Dilic M, Manfrini O, et al. Delayed care and mortality among women and men with myocardial infarction. J Am Heart Assoc. 2017;6:e005968. DOI: 10.1161/JAHA.117.005968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Stehli J, Martin C, Brennan A, Dinh DT, Lefkovits J, Zaman S. Sex differences persist in time to presentation, revascularization, and mortality in myocardial infarction treated with percutaneous coronary intervention. J Am Heart Assoc. 2019;8:e012161. DOI: 10.1161/JAHA.119.012161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Meyer MR, Bernheim AM, Kurz DJ, O'Sullivan CJ, Tuller D, Zbinden R, Rosemann T, Eberli FR. Gender differences in patient and system delay for primary percutaneous coronary intervention: current trends in a Swiss ST‐segment elevation myocardial infarction population. Eur Heart J Acute Cardiovasc Care. 2018;8:283–290. DOI: 10.1177/2048872618810410. [DOI] [PubMed] [Google Scholar]
- 15.Diercks DB, Owen KP, Kontos MC, Blomkalns A, Chen AY, Miller C, Wiviott S, Peterson ED. Gender differences in time to presentation for myocardial infarction before and after a national women's cardiovascular awareness campaign: a temporal analysis from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress ADverse Outcomes with Early Implementation (CRUSADE) and the National Cardiovascular Data Registry Acute Coronary Treatment and Intervention Outcomes Network‐Get with the Guidelines (NCDR ACTION Registry‐GWTG). Am Heart J. 2010;160:80–87.e3. DOI: 10.1016/j.ahj.2010.04.017. [DOI] [PubMed] [Google Scholar]
- 16.Roswell RO, Kunkes J, Chen AY, Chiswell K, Iqbal S, Roe MT, Bangalore S. Impact of sex and contact‐to‐device time on clinical outcomes in acute ST‐segment elevation myocardial infarction‐findings from the National Cardiovascular Data Registry. J Am Heart Assoc. 2017;6:e004521. DOI: 10.1161/JAHA.116.004521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Making the Invisible Visible; Heart Foundation, Women and heart disease. Published January 30, 2018. Available at: https://www.heartfoundation.org.au/getmedia/f9e4967e‐6f4e‐4e71‐9b82‐bc1e3b1c5623/Heart_Foundation_Annual_Review.pdf. Accessed April 24, 2021.
- 18.Stub D, Lefkovits J, Brennan AL, Dinh D, Brien R, Duffy SJ, Cox N, Nadurata V, Clark DJ, Andrianopoulos N, et al. The establishment of the Victorian Cardiac Outcomes Registry (VCOR): monitoring and optimising outcomes for cardiac patients in Victoria. Heart Lung Circ. 2018;27:451–463. DOI: 10.1016/j.hlc.2017.07.013. [DOI] [PubMed] [Google Scholar]
- 19.Cox N, Brennan A, Dinh D, Brien R, Cowie K, Stub D, Reid CM, Lefkovits J. Implementing sustainable data collection for a cardiac outcomes registry in an Australian public hospital. Heart Lung Circ. 2018;27:464–468. DOI: 10.1016/j.hlc.2017.01.023. [DOI] [PubMed] [Google Scholar]
- 20.Cox S, Martin R, Somaia P, Smith K. The development of a data‐matching algorithm to define the 'case patient'. Aust Health Rev. 2013;37:54–59. DOI: 10.1071/AH11161. [DOI] [PubMed] [Google Scholar]
- 21.OpenDocument Australian Bureau of Statistics. Socio‐Economic Indexes for Areas (SEIFA). Cat no. 2033.0.55.001. Published: March 27, 2018. Available at: https://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/2033.0.55.001Main+Features12016?. Accessed April 24, 2021.
- 22.Australian Bureau of Statistics . Measures of socioeconomic status. Cat no. 1244.0.55.001. Published: June 22, 2011. Available at: https://www.ausstats.abs.gov.au/Ausstats/subscriber.nsf/0/367D3800605DB064CA2578B60013445C/$File/1244055001_2011.pdf. Accessed April 24, 2021.
- 23.Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction . Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018;72:2231–2264. DOI: 10.1016/j.jacc.2018.08.1038. [DOI] [PubMed] [Google Scholar]
- 24.Mehran R, Rao SV, Bhatt DL, Gibson CM, Caixeta A, Eikelboom J, Kaul S, Wiviott SD, Menon V, Nikolsky E, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123:2736–2747. DOI: 10.1161/CIRCULATIONAHA.110.009449. [DOI] [PubMed] [Google Scholar]
- 25.Benamer H, Bataille S, Tafflet M, Jabre P, Dupas F, Laborne FX, Lapostolle F, Lefort H, Juliard JM, Letarnec JY, et al. Longer pre‐hospital delays and higher mortality in women with STEMI: the e‐MUST Registry. EuroIntervention. 2016;12:e542–e549. DOI: 10.4244/EIJV12I5A93. [DOI] [PubMed] [Google Scholar]
- 26.Sederholm Lawesson S, Isaksson R‐M, Ericsson M, Ängerud K, Thylén I; SymTime Study G . Gender disparities in first medical contact and delay in ST‐elevation myocardial infarction: a prospective multicentre Swedish survey study. BMJ Open. 2018;8:e020211. DOI: 10.1136/bmjopen-2017-020211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lichtman JH, Leifheit EC, Safdar B, Bao H, Krumholz HM, Lorenze NP, Daneshvar M, Spertus JA, D'Onofrio G. Sex differences in the presentation and perception of symptoms among young patients with myocardial infarction: evidence from the VIRGO Study (Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients). Circulation. 2018;137:781–790. DOI: 10.1161/CIRCULATIONAHA.117.031650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pelletier R, Khan NA, Cox J, Daskalopoulou SS, Eisenberg MJ, Bacon SL, Lavoie KL, Daskupta K, Rabi D, Humphries KH, et al. Sex versus gender‐related characteristics: which predicts outcome after acute coronary syndrome in the young? J Am Coll Cardiol. 2016;67:127–135. DOI: 10.1016/j.jacc.2015.10.067. [DOI] [PubMed] [Google Scholar]
- 29.Brush JE Jr, Krumholz HM, Greene EJ, Dreyer RP. Sex differences in symptom phenotypes among patients with acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2020;13:e005948. DOI: 10.1161/CIRCOUTCOMES.119.005948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kirchberger I, Heier M, Kuch B, Wende R, Meisinger C. Sex differences in patient‐reported symptoms associated with myocardial infarction (from the population‐based MONICA/KORA Myocardial Infarction Registry). Am J Cardiol. 2011;107:1585–1589. DOI: 10.1016/j.amjcard.2011.01.040. [DOI] [PubMed] [Google Scholar]
- 31.Chew DP, Scott IA, Cullen L, French JK, Briffa TG, Tideman PA, Woodruffe S, Kerr A, Branagan M, Aylward PE; NHFA/CSANZ ACS Guideline 2016 Executive Working Group . National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the management of acute coronary syndromes 2016. Heart Lung Circ. 2016;25:895–951. DOI: 10.1016/j.hlc.2016.06.789. [DOI] [PubMed] [Google Scholar]
- 32.Huded CP, Johnson M, Kravitz K, Menon V, Abdallah M, Gullett TC, Hantz S, Ellis SG, Podolsky SR, Meldon SW, et al. 4‐step protocol for disparities in STEMI care and outcomes in women. J Am Coll Cardiol. 2018;71:2122–2132. DOI: 10.1016/j.jacc.2018.02.039. [DOI] [PubMed] [Google Scholar]
- 33.Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; Executive Group on behalf of the Joint European Society of Cardiology/American College of Cardiology/American Heart Association/World Heart Federation Task Force for the Universal Definition of Myocardial I . Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018;72:2231–2264. DOI: 10.1016/j.jacc.2018.08.1038. [DOI] [PubMed] [Google Scholar]
- 34.Gupta A, Barrabes JA, Strait K, Bueno H, Porta‐Sanchez A, Acosta‐Velez JG, Lidon RM, Spatz E, Geda M, Dreyer RP, et al. Sex differences in timeliness of reperfusion in young patients with ST‐segment‐elevation myocardial infarction by initial electrocardiographic characteristics. J Am Heart Assoc. 2018;7:e007021. DOI: 10.1161/JAHA.117.007021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Green JL, Jacobs AK, Holmes D, Chiswell K, Blanco R, Bates ER, French W, Kupas DF, Mears G, Roe M, et al. Taking the reins on systems of care for ST‐segment‐elevation myocardial infarction patients: a report from the American Heart Association Mission: Lifeline Program. Circ Cardiovasc Interv. 2018;11:e005706. DOI: 10.1161/CIRCINTERVENTIONS.117.005706. [DOI] [PubMed] [Google Scholar]
- 36.Bata A, Quraishi AUR, Love M, Title L, Beydoun H, Lee T, Nadeem N, Kidwai B, Kells C, Curran H. Initial experience with pre‐activation of the cardiac catheterization lab and emergency room bypass for patients with ST‐elevation myocardial infarction in Halifax, Nova Scotia. Int J Cardiol. 2016;222:645–647. DOI: 10.1016/j.ijcard.2016.07.162. [DOI] [PubMed] [Google Scholar]
- 37.Johnson KW, Torres Soto J, Glicksberg BS, Shameer K, Miotto R, Ali M, Ashley E, Dudley JT. Artificial intelligence in cardiology. J Am Coll Cardiol. 2018;71:2668–2679. DOI: 10.1016/j.jacc.2018.03.521. [DOI] [PubMed] [Google Scholar]
- 38.Khera S, Kolte D, Gupta T, Subramanian KS, Khanna N, Aronow WS, Ahn C, Timmermans RJ, Cooper HA, Fonarow GC, et al. Temporal trends and sex differences in revascularization and outcomes of ST‐segment elevation myocardial infarction in younger adults in the United States. J Am Coll Cardiol. 2015;66:1961–1972. DOI: 10.1016/j.jacc.2015.08.865. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Because of the sensitive nature of the data collected for this study, requests to access the data set from qualified researchers trained in human subject confidentiality protocols may be sent to the VCOR (Victorian Cardiac Outcomes Registry) Data Access, Research and Publications Committee at vcor@monash.edu.