

Abstract
In pediatric arteriography, vascular complications are more common than in adults; thus, the use of the smallest catheter to accomplish the objective of the procedure is recommended. We describe two pediatric cases in which abdominal arterial embolization and arteriography were performed with steerable microcatheters without conventional diagnostic catheters. Additionally, we used an introducer with an outer diameter of 4-F in a Mini Access Kit (Merit Medical, South Jordan, UT) as a vascular sheath to reduce sheath size. We believe that this technique may be feasible and safe for abdominal arterial interventions in children.
Keywords: Arterial access, Embolization, Mini Access Kit, Pediatrics, Steerable microcatheter
Introduction
In pediatric arteriography, vascular complications, including occlusion, vasospasm, and dissection, develop more commonly than in adults. [1]. It is recommended to use the smallest catheter to accomplish the objectives of the procedure [1]. In clinical practice, a 3- or 4-F diagnostic catheter and a compatible vascular sheath are used for most diagnostic arteriography procedures in children [1]. If microcatheters alone are used and sheath size is reduced, the vascular complication rate can be reduced. We report two pediatric cases of abdominal arteriography and intervention successfully performed with a steerable microcatheter without a conventional diagnostic catheter through a 4-F introducer.
Case report
Case 1
A 3-year-old girl was transferred to our hospital from an outside hospital with a diagnosis of rupture of a liver tumor after minor abdominal trauma (Fig. 1). She had no past medical history and her body weight was 16.9 kg. On arrival, the patient experienced hemodynamic shock. Emergency arterial embolization was performed to stop the bleeding. Under general anesthesia, the left common femoral artery was punctured with a 22-G coaxial needle under ultrasound guidance. A 0.018-inch guidewire in a 4-F Merit MAK401 Mini Access Kit (Merit Medical, South Jordan, UT) was advanced, followed by placement of the coaxial introducer in the same kit. The introducer had an outer diameter of 4-F. A hemostasis valve was attached to the introducer, which was used as the vascular sheath. A 2.9-F high-flow steerable microcatheter (SwiftNINJA high flow; Sumitomo Bakelite, Tokyo, Japan) was advanced, and the celiac trunk was selected without a guidewire. Common hepatic angiography revealed enhancement of the liver tumor (Fig. 2A). The segment 6 hepatic artery (A6) was the main feeding artery of the tumor, with A5 as another feeding artery. A selective-type microcatheter (Carry Leon selective; UTM, Nagoya, Japan) with a distal diameter of 1.7-F and proximal diameter of 1.9-F was advanced through the high-flow microcatheter over a 0.014-inch guidewire, and the 2 feeding arteries were selected and embolized with gelatin sponge particles (Fig. 2B andD). After embolization, angiography revealed no persistent tumor enhancement. Finally, angiography of the femoral artery (Fig. 2E) confirmed that there were no abnormalities at the puncture site. The introducer was removed and manual compression was applied for 10 min, followed by compression with a gauze roll and elastic tape for 3 h. The patient's vital signs stabilized after the procedure, and no complications developed. 2 days later, partial resection of the liver was performed to remove the tumor, leading to the diagnosis of hepatoblastoma.
Fig. 1.
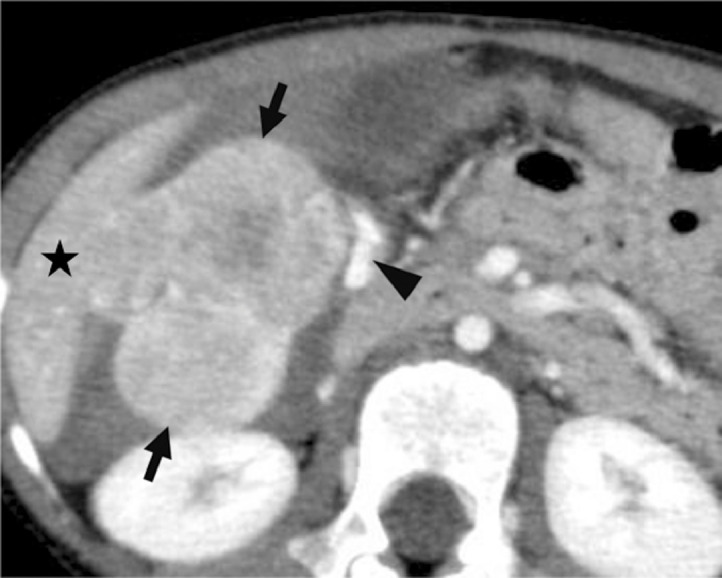
Contrast-enhanced computed tomography scan (Case 1) of the upper abdomen reveals a lobulated tumor (arrows) protruding from the liver (star). Extravasation of contrast medium (arrowhead) is also observed.
Fig. 2.

Angiography (Case 1) during embolization of the liver tumor. (A) Angiography from the common hepatic artery reveals enhancement of the liver tumor (arrows). The segment 6 hepatic artery (A6; arrowhead) is the main feeder of the tumor. This angiography was obtained by a high-flow steerable microcatheter. (B) Angiography from the A6 with a selective-type microcatheter reveals enhancement of the tumor. The catheter tip of a high-flow microcatheter is at the right hepatic artery (arrow). (C) Angiography from the right hepatic artery after embolization of the A6 reveals that a branch of the A5 (arrowhead) also feeds the tumor (arrow). (D) Angiography from the A5 with a selective-type microcatheter reveals enhancement at the medial part of the tumor (arrow). The catheter tip of a high-flow microcatheter is at the right hepatic artery (arrowhead). (E) Angiography from the 4-F introducer reveals no dissection or spasm at the puncture site (arrow).
Case 2
A 7-year-old boy with severe physical and mental disabilities visited our hospital because of melena and anemia. He had many episodes of admission due to central venous catheter infection and acute pancreatitis. The cause of pancreatitis was unclear. His body weight was 10.1 kg. Upper endoscopy revealed bleeding from the papilla of Vater. Contrast-enhanced computed tomography did not reveal the bleeding site. We decided to perform abdominal angiography to identify the cause of the bleeding. Under general anesthesia, a 4-F introducer was placed in the right common femoral artery in the same way as in Case 1. From the introducer, a 2.9-F high-flow steerable microcatheter was advanced, and the celiac trunk was easily selected without a guidewire. Celiac angiography was performed; however, the site of bleeding was not evident. Then, the common and proper hepatic arteries, gastroduodenal arteries, and splenic arteries were selected with the microcatheter using a 0.016-inch guidewire. Angiography of these arteries (Fig. 3) did not show any abnormalities, such as pseudoaneurysms or tumor stains. The procedure was ended, and hemostasis at the puncture site was obtained in the same way as in Case 1. No complications occurred. Although the cause of the hemorrhage was unclear, melena was discontinued after the procedure. The patient was discharged home one week later.
Fig. 3.

Abdominal angiography (Case 2) obtained by a high-flow microcatheter. Angiography from the superior mesenteric artery (A) and gastroduodenal artery (B) shows no sign of bleeding.
Discussion
A small number of studies have reported cases in which a steerable microcatheter with a distal diameter of 2.4-F (SwiftNINJA standard; Sumitomo Bakelite, Tokyo, Japan) was directly advanced via the femoral approach to a target organ without a diagnostic catheter, achieving successful arterial intervention: hepatic arterial infusion chemotherapy, uterine artery embolization, and arterial embolization for pediatric trauma [2], [3], [4]. The steerable tip of a steerable microcatheter plays a key role in increasing the operability of these interventions [2]. In this study, we used a high-flow steerable microcatheter to enable the coaxial advancement of a selective-type microcatheter through it. We believe that more selective advancement of a microcatheter can be achieved with this technique than when only a 2.4-F steerable microcatheter was used.
1 major disadvantage of using a steerable microcatheter without a diagnostic catheter is decreased catheter stability. Thus, we consider that this technique is more useful in the pediatric population than in adults because pediatric arteries are straighter and narrower, without arterial calcification, requiring less catheter stability during the procedure. Additionally, the maximum flow rate of a microcatheter is lower than that of a diagnostic catheter. Although the maximum flow rate with a microcatheter may not be sufficient for abdominal arteriography in adults, it is sufficient in most children.
A 4-F Mini Access Kit (Merit Medical) is similar to a Micropuncture Access Set (Cook Medical, Bloomington, IN), both of which include a 21-G micropuncture needle, 0.018-inch guidewire, and 4-F coaxial introducer and dilator. The introducers have an internal diameter of 2.9-F, allowing the introduction of a high-flow microcatheter. Thus, it can be used as a vascular sheath for microcatheters. This technique has been reported for retrograde access to the pedal arteries [5]. The outer diameter of the introducer is 1.33 mm, whereas the outer diameter of a 3-F vascular sheath is 1.60 mm [6]. Thus, a drastic reduction in sheath size is possible by using the introducer as a vascular sheath, probably leading to lower access site complications.
Conclusions
In conclusion, pediatric arterial interventio. n can be performed with a steerable microcatheter through a 4-F introducer, without a conventional diagnostic catheter. Using this method, vascular complications may be reduced.
Footnotes
Funding: This study was not supported by any funding.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent: Informed consent was obtained from all individual participants included in the study.
Consent for publication: Consent for publication was obtained for every individual person's data included in the study.
Competing Interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Patient Consent
Written consent for publication was obtained from the patient.
References
- 1.Heran MK, Marshalleck F, Temple M, Grassi CJ, Connolly B, Towbin RB. Joint quality improvement guidelines for pediatric arterial access and arteriography: from the societies of interventional radiology and pediatric radiology. J Vasc Interv Radiol. 2010;21(1):32–43. doi: 10.1016/j.jvir.2009.09.006. [DOI] [PubMed] [Google Scholar]
- 2.Koike Y, Kawahara Y, Kiss B, Tannai H, Matsui S. Single-administration hepatic arterial infusion chemotherapy using steerable microcatheter alone through outer cannula of 18-gauge needle: a preliminary study. J Vasc Interv Radiol. 2019;30(3):471–473. doi: 10.1016/j.jvir.2018.08.013. [DOI] [PubMed] [Google Scholar]
- 3.Martin JT, Hulsberg PC, Soule E, Shabandi M, Matteo J. Welcome to the new era: a completely wireless interventional procedure. cureus. 2018;10(9):e3337. doi:10.7759/cureus.3337. [DOI] [PMC free article] [PubMed]
- 4.Harmon TS, Kee-Sampson J, Hester TS, Bashir S, Matteo J. Pediatric traumas and paradigm shifts: the necessary adaption of the steerable microcatheter in pediatric interventional radiology. Cureus. 2019;11(2):e4125. doi: 10.7759/cureus.4125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.El-Sayed H, Bennett ME, Loh TM, Davies MG. Retrograde pedal access and endovascular revascularization: a safe and effective technique for high-risk patients with complex tibial vessel disease. Ann Vasc Surg. 2016;31:91–98. doi: 10.1016/j.avsg.2015.09.015. [DOI] [PubMed] [Google Scholar]
- 6.Aramaki T, Moriguchi M, Bekku E, Endo M, Asakura K, Boku N. Prospective evaluation of the optimal duration of bed rest after vascular interventions using a 3-French introducer sheath. CardioVasc IntervRadiol. 2015;38(1):40–44. doi: 10.1007/s00270-014-0892-3. [DOI] [PubMed] [Google Scholar]