

Abstract
Background:
For unclear reasons, minorities have been historically underrepresented in multiple sclerosis (MS) clinical trials. We hypothesized that different perceptions and preferences about research participation among racial and ethnic groups contribute to this imbalance.
Methods:
Members of the MS Minority Research Engagement Partnership Network developed a Web-based survey in English and Spanish on research impressions, concerns, and preferences regarding study attributes among people with MS. Invitations to take the survey were distributed by network members and partner organizations.
Results:
We included 2599 participants with MS (2111 White, 215 African American; 188 Hispanic). Consistently disliked study attributes included potential harms to health and confusing study information. Compared with White and non-Hispanic participants, respectively, African American (odds ratio [OR] = 2.05, P ≤ .001) and Hispanic (OR = 1.79, P = .003) participants were more concerned about being used by the research team. Hispanic participants were more concerned about research participation carrying risks to their legal status (OR = 1.70, P = .001). Hispanic (OR = 3.18, P ≤ .001) and African American (OR = 5.51, P ≤ .001) participants were more likely to prefer for the study to benefit their own racial/ethnic group. A top concern across all groups was not being fully informed about the research.
Conclusions:
We found strong support for research across racial and ethnic groups; however, minority groups have specific concerns regarding mistrust, receiving poor-quality care, unemployment, health insurance, and legal status. Investigators wanting to recruit a diverse study population are advised to show how they have addressed these concerns and to communicate how the research will advance the science and literature and result in better care and/or other benefits to underrepresented communities.
Keywords: African American, Diversity, Health care disparities, Hispanic, Multiple sclerosis (MS)
Multiple sclerosis (MS) is a chronic demyelinating disease of the central nervous system with onset typically occurring in early adulthood. Although in the United States MS was previously thought to be most prevalent in White people, recent studies of members of the military1 and Kaiser Permanente health system members2 suggest that African American individuals may actually be at increased risk for the disease. Clinical differences have also been reported among racial and ethnic groups; for example, African American people with MS seem to have greater retinal damage,3 brain lesion volume,4,5 and disability progression rates6–9 than White individuals with MS, and Hispanic American people may have a more severe disease course10 and are more likely to present with optic neuritis and transverse myelitis than are non-Hispanic individuals.11
Socioeconomic factors, lack of access to specialists, lack of education about MS treatments, and delays in diagnosis with more severe prognoses may contribute to disparities in health outcomes in the African American and Hispanic communities.10–13 The impact of MS in other communities is less well understood, but disparities may also exist for other groups, such as Asians/Asian Americans, people of Middle Eastern descent, and Native Americans.
As is the case with many other diseases,14–16 minority groups tend to be underrepresented in MS clinical research. This is true for industry-funded research, such as clinical trials for interferon beta,17 natalizumab,18 and ocrelizumab,19 as well as for publicly funded MS studies.20 Even research studies focused specifically on minority concerns have faced difficulty enrolling participants, such as patients with less education or lower socioeconomic status.21 The lack of diversity in research participation has a variety of undesirable effects, including inequitable distribution of the benefits of research participation and imbalance in evidence regarding benefits and harms of interventions among populations,22,23 that help to perpetuate disparities in health care for minority groups.
The MS Minority Research Engagement Partnership Network (MREPN) is an inclusive and comprehensive program that brings together diverse stakeholder groups to identify and address the barriers to minority participation in MS research. It was formed by the Accelerated Cure Project in 2016 with funding support provided by a Eugene Washington PCORI Engagement Award from the Patient-Centered Outcomes Research Institute (PCORI). The MREPN comprises multiple stakeholders representing people with MS, MS and minority advocacy organizations, MS clinicians and researchers, and biopharmaceutical industry representatives. The goals of this network are to promote greater research inclusion of diverse demographic groups of people with MS by better understanding the barriers and facilitators affecting minority participation in MS research and conducting outreach efforts aimed at promoting minority engagement in MS research.
Although previous investigations have been performed in other health conditions to identify factors affecting minority research participation, no such study had yet been performed specifically in MS. To provide insights into how people with MS of different races and ethnicities perceive research participation, and to aid in the development of materials and programs to promote health literacy for increased minority participation in MS research, the MREPN conducted a targeted survey of people diagnosed as having MS.
Methods
Survey Development
Members of the MREPN, including clinicians, researchers, and individuals with MS from diverse backgrounds (African American, Hispanic, and non-Hispanic White), developed an initial list of topics for the survey by consulting the health literature24–26 on factors contributing to minority research disparities. Additional topics were added based on network members’ interests and experiences. The final topic set included overall attitudes toward research, sources of information about research, previous research experience, concerns about research participation, preferences for different research study characteristics, and demographic and MS attributes.
Specific questions were developed to address each topic and were refined based on input from MREPN members. Most questions were developed in a close-ended format to simplify analysis, but open-response questions were included as well to capture additional information on certain topics, such as sources of research information and impressions of research participation. The survey team used monthly conference calls to discuss the survey as well as e-mail for sharing and reviewing edits to the survey and confirming consensus on the final version.
The final 35-question survey (Appendix S1, which is published in the online version of this article at ijmsc.org) was translated into Spanish and reviewed by native Spanish speakers. Both versions (English and Spanish) were programmed on the internet survey site SurveyGizmo.com. Testing for functionality and understandability was performed by MREPN members and by five volunteers (laypeople, one of whom had MS) who had not been involved in the survey development process.
Ethical Approval of Studies
The Copernicus Group Independent Review Board evaluated the study and determined that the proposed activity did not meet the definition of research under US Department of Health and Human Services and US Food and Drug Administration regulations.
Survey Dissemination
All MREPN members with access to people with MS (eg, MS advocacy organizations and clinicians) participated in the survey dissemination process. Invitations to complete the survey were distributed by e-mail, social media, and in-clinic flyers. Other MS advocacy organizations were also asked to help with disseminating the survey to their constituents through e-mail and social media. Survey responses were collected over an approximately 2-month period (May 16 through July 18, 2017). Eligibility criteria included being at least 21 years old and having a diagnosis of MS.
Statistical Methods
All analyses were conducted using the statistical software Stata 13 (StataCorp). Descriptive analyses were used to summarize demographic characteristics. The entire cohort carrying a diagnosis of MS was stratified by self-reported ethnicity (Hispanic, non-Hispanic, and unknown/undisclosed ethnicity) and by self-reported race for the two largest groups: African American and White. Other racial groups (multiracial, Native Hawaiian, Asian, and American Indian) were not included in the analyses because of small sample size. Statistical analyses were performed on impressions regarding MS research, the importance of different MS research topics, places used as sources of information, trusted sources of information, preferred research study activities, concerns regarding research study participation, and preferences regarding different research study attributes.
Two questions were asked to identify places, people, and organizations used by participants to learn about research: “Where would you go for information if you wanted to learn about research or find a study?” and “Which of these would you trust as sources of information about MS research?” For these multiple-choice questions, where participants were allowed to select more than one choice, all the selected sources were later coded as “yes” for analysis purposes. Sources that remained unselected were coded as “no.”
For all analyses, the χ2 test was used to test for independence between race/ethnicity and each answer choice. When independence was not met, answers were dichotomized and logistic regression was performed to test for association between race/ethnicity and that particular response. When associations were found, multivariate logistic regression analyses were conducted for each response that included three different sets of covariates. The first model included the following socioeconomic covariates: education, income, and residential area type. The second model included the demographic covariates sex and year of birth. The third model included disease-specific covariates (time since MS diagnosis, MS care provider, and MS care center). Race and ethnicity were used as the independent variables. The dependent variables were MS research impressions, MS research topics, sources of information, research study attributes, and concerns regarding study participation. Results are reported as odds ratios (ORs), and analyses were determined to be significant if they reached P < .05 for a more conservative approach. Each study dependent variable was modeled separately to minimize repeated-measures effect.
Results
We received 2631 responses to the study, which reduced to 2599 responses after removing ineligible responses (eg, the respondent did not meet the eligibility criteria or provided no information beyond the initial screening question). Ten of these responses were to the Spanish version of the survey; the remainder were to the English version.
Demographic (Table 1) and MS-specific (Table S1) characteristics were compared between self-reported racial and ethnic groups using nonparametric tests. Of the total participants in the study, 7.23% were Hispanic; 8.27% were African American; 92.89% were residents of the United States, with the remainder from 40 other countries; 78.62% were women; 20.77% were men; and 39.57% of the total had participated in research studies previously.
Table 1.
Demographic characteristics of the 2599 survey participants
| Characteristic | Race | Ethnicity | |||||
|---|---|---|---|---|---|---|---|
|
|
|
||||||
| African American (n = 215) | White (n = 2111) | P value | Hispanic (n = 188) | Non-Hispanic (n = 2369) | Unknown (n = 42) | P value | |
| Age | <.001 | <.001 | |||||
| ≤34 y | 19 (8.83) | 151 (7.15) | 35 (18.61) | 179 (7.55) | 1 (0.04) | ||
| 35–55 y | 125 (58.13) | 911 (43.15) | 101 (53.72) | 1058 (44.66) | 21 (0.88) | ||
| ≥56 y | 54 (25.11) | 955 (45.23) | 40 (21.27) | 1024 (43.22) | 12 (0.50) | ||
| No answer | 17 (7.90) | 94 (4.45) | 12 (6.38) | 108 (4.55) | 8 (0.33) | ||
| Sex | .01 | <.001 | |||||
| Male | 26 (12.09) | 452 (21.41) | 33 (17.55) | 490 (20.68) | 14 (33.33) | ||
| Female | 186 (86.51) | 1643 (77.83) | 151 (80.31) | 1863 (78.64) | 19 (45.23) | ||
| Other/no answer | 3 (1.39) | 16 (0.75) | 4 (2.12) | 16 (0.67) | 9 (21.42) | ||
| Educational level | .6 | <.001 | |||||
| Less than HS diploma | 1 (0.46) | 13 (0.61) | 2 (1.06) | 15 (0.63) | 0 | ||
| HS/trade school diploma | 25 (11.62) | 326 (15.44) | 29 (15.42) | 353 (14.90) | 7 (16.66) | ||
| Some college/associate/bachelor’s degree | 127 (59.06) | 1190 (56.37) | 101 (53.72) | 1335 (56.35) | 21 (50.00) | ||
| Graduate school/advanced degree | 59 (27.44) | 565 (26.76) | 56 (29.78) | 645 (27.22) | 6 (14.28) | ||
| No answer | 3 (1.39) | 17 (0.80) | 0 | 21 (0.88) | 8 (19.04) | ||
| Household income | <.001 | <.001 | |||||
| <$50,000 | 102 (47.44) | 714 (33.82) | 78 (41.48) | 820 (34.61) | 14 (33.33) | ||
| $50,001–$100,000 | 49 (22.79) | 542 (25.67) | 46 (24.46) | 606 (25.58%) | 2 (4.76) | ||
| >$100,000 | 36 (16.74) | 449 (21.26) | 40 (21.27) | 492 (20.76) | 4 (9.52) | ||
| No answer | 28 (13.02) | 406 (19.23) | 24 (12.76) | 451 (19.03) | 22 (52.38) | ||
Note: Data are given as number (percentage).
Abbreviation: HS, high school.
Impressions Regarding Research in MS
One section of the survey asked about general opinions about the value and benefits of research. Although most participants of all backgrounds agreed that medical research has led to better MS treatments and that more research involving patients with MS is needed, there were some differences among groups. For instance, Hispanic participants (OR = 1.49, P = .02) and participants of unknown/undisclosed ethnicity (OR = 2.57, P = .004), compared with non-Hispanic participants, had higher odds of agreeing with the following statement: “There is not much left to be learned about MS.” In Hispanic people, this remained significant after adjusting for all the covariates.
African American participants were less likely to agree that medical research has led to better MS treatments (OR = 0.63, P = .002). This association continued to be significant after adjusting for demographic and MS-specific covariates but became stronger after adjusting for socioeconomic factors (OR = 0.57, P ≤ .001).
We also characterized the open-text responses to the question “When you think about the term medical research what comes to mind?” to enhance our understanding of the respondents’ attitudes toward research. Overall, 46% of the responses gave a definition or description of research (eg, “test medicines, exams, and questions”); 42% of the responses were categorized as positive/interested (eg, “a cure for MS and new medications”); 6% were characterized by fear or distrust (eg, “money, pharmaceutical companies, and fake statistics”); and 4% had a tone of frustration (eg, “not enough of it in progressive MS”).
Importance of Different Topics in MS Research
We also surveyed participants’ views on the importance of certain MS research topics. All topics listed were thought to be important by at least 90% of the respondents. African American and White participants had different views on different MS research topics. African American participants had higher odds of considering the following research topics to be important compared with White participants: diet and exercise (OR = 2.13, P ≤ .001) and strategies to diagnose MS more quickly (OR = 2.18, P ≤ .001). These findings remained significant after adjusting for demographic, socioeconomic, and disease-specific covariates.
Sources of Information About Research
Participation in research is influenced by access to information about research opportunities. Therefore, we wanted to learn whether differences existed in the sources people would turn to for research information.
Across all groups, MS organizations and MS websites/blogs were the top two sources that people said they would go to for information about research studies. There was no significant difference in the use of the following sources of information across all ethnic and racial groups: medical clinics, MS organizations, websites or blogs about MS, social media websites, drug company websites, other people with MS, Google/internet search, or church/place of worship. However, the Hispanic group was more likely to select the answer choice “I wouldn’t know where or how to find this information” compared with the non-Hispanic group (unadjusted OR = 2.31, P = .01). This was significant after adjusting for socioeconomic and disease-specific covariates.
In addition to asking where people would look for information about research, we also asked which sources they would trust. Across all groups, MS organizations and one’s own doctor or nurse were the top two responses to this question. The Hispanic group had higher odds of trusting community leaders compared with non-Hispanics (OR = 2.48, P = .01). This finding was significant after adjusting for demographic and disease-specific covariates but lost significance after adjusting for socioeconomic variables.
The African American group had lower odds of trusting a university (OR = 0.60, P = .001) and higher odds of trusting newspapers/magazines (OR = 1.55, P = .01) and other people with MS (OR = 1.57, P= .002) as sources of information compared with White participants. These results were significant after adjusting for socioeconomic, demographic, and disease-specific covariates.
Preferred Research Study Activities
When presented with a list of typical research study activities, participants of all ethnic backgrounds, as well as African American and White individuals, were likely to consider participating in research studies involving receiving drug treatments, receiving nondrug treatments (such as physical therapy, yoga, or massage), having laboratory tests or imaging studies performed, taking surveys, and playing brain training games, with no difference (Figure S1). Participants of all ethnicities would consider participating in a study that required them to follow a special diet. Most of the listed activities received a positive response from 90% or more of the respondents.
Concerns Regarding Participation in Research
By Ethnicity
We asked respondents to characterize their level of concern regarding a variety of potential study-related risks or issues. Participants of all ethnicities considered not being fully informed about the study to be an important concern when considering participating in research, with no difference. Having personal information being released without approval was also an important concern across all groups (Figure S2).
Both Hispanic participants (OR = 1.70, P = .001) and participants of unknown/undisclosed ethnicity (OR = 2.16, P = .02) were more concerned about their research participation carrying risks to their job or legal status compared with non-Hispanic participants. In Hispanic individuals, this association remained significant even after considering socioeconomic and MS-specific characteristics.
Losing health insurance coverage was also concerning to both Hispanic participants (OR = 1.53, P = .007) and participants of unknown/undisclosed ethnicity (OR = 2.67, P = .007) compared with non-Hispanic participants. In Hispanic participants, this issue remained significant after including socioeconomic variables and was borderline after including demographic and disease-specific covariates.
Both the Hispanic (OR = 1.79, P = .003) and the unknown/undisclosed ethnicity (OR = 4.76, P = .009) groups were more concerned about being used or taken advantage of by the research team compared with non-Hispanics. In Hispanic participants, this finding remained significant after adjusting for all three sets of covariates. In the unknown/undisclosed ethnicity group, this association remained after adjusting for demographic and MS-specific covariates but was lost after adjusting for socioeconomic covariates.
Receiving poor-quality medical care was more concerning to Hispanic participants compared with non-Hispanic participants (OR = 1.76, P = .001) even after adjusting for socioeconomic, demographic, and disease-specific variables.
By Race
Both African American and White participants reported that not being fully informed about the study was a concern when participating in research, with no difference. African American participants were more concerned compared with White participants about their personal information being released without their approval (OR = 1.57, P = .003) and about being used or taken advantage of by the research team (OR = 2.05, P ≤ .001) independent of demographic, socioeconomic, and MS-specific characteristics. African American individuals also considered receiving poor-quality medical care a more important concern (OR = 1.45, P = .01) compared with White individuals. This finding was independent of socioeconomic and MS-specific variables and was borderline significant after adjusting for demographic characteristics.
Preferences Regarding Research Study Attributes
Finally, the survey showed a list of potential research study characteristics and asked respondents to indicate how well they would like or dislike them. For the analysis of this section, several participants were excluded due to incomplete responses. We attribute the incompleteness to this being a lengthy section situated toward the end of the survey. We included 1953 participants, of whom 6.75% were Hispanic, 7.27% were African American, 92.31% were residents of the United States, 77.57% were women, and 21.40% were men.
The top three study attributes were preferred across all ethnic and racial groups, with no significant differences: the research would benefit people with MS, the results of individual tests would be received during the study, and the study results would be received once the study was finalized (Figure 1). The top three most disliked study attributes were potential harms to health, confusing study information, and study clinic being difficult to get to (Figure S3).
Figure 1.
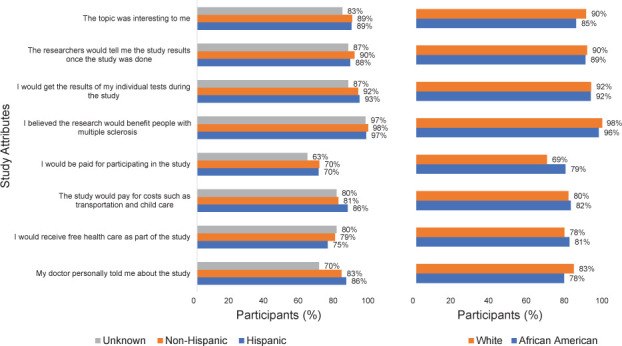
Preferred research study attributes by ethnicity and race
Percentages shown for “I would like it very much” and “I would like it somewhat.”
The preference regarding several study attributes differed across ethnic groups. Hispanic participants showed higher odds of liking for the study to benefit their own racial/ethnic group (3.18, P ≤ .001) compared with non-Hispanic participants, and this result was significant after adjusting for all the covariates. The undisclosed ethnicity group had higher odds of disliking to receive a placebo medication versus the actual drug (OR = 0.29, P = .001) and had lower odds of liking having their family support their study participation (OR = 0.33, P = .008) compared with participants who self-identified as non-Hispanic. This finding was significant after adjusting for socioeconomic and MS-related covariates.
African American individuals had a higher level of preference for compensation for participation in the research study (OR = 1.65, P = .01) and for the study to be beneficial to their own ethnic/racial group (OR = 5.51, P ≤ .001) compared with White participants. This result was significant after adjusting for socioeconomic and MS-specific covariates in the former and for demographic, socioeconomic, and disease-specific covariates in the latter. African American participants also exhibited a greater dislike of the prospect for their health to be harmed as the result of participating in the research study (OR = 0.58, P = .02) compared with White participants. This finding was significant after adjusting for socioeconomic variables but became nonsignificant after adjusting for demographic and disease-specific variables.
Discussion
To support an initiative to understand and address racial and ethnic imbalances in MS research participation, we conducted an exploratory internet-based survey of preferences and opinions among people with MS. In this study, we found similarities and differences across racial and ethnic groups regarding research impressions, topics in MS research, sources of information about research, preferred research study activities, concerns regarding participation in research, and preferred research study attributes. Herein we offer an analysis of these results and describe how investigators can recognize these similarities and differences to more successfully recruit diverse MS study populations while achieving faster study enrollment and better retention.
Overall, the sample revealed support for research, a belief in the need for additional research into MS, and willingness to participate in a variety of research activities, with greater than 85% of respondents being open to studies involving surveys, brain training games, nondrug treatments such as yoga, laboratory testing, and special diets. Research involving drug treatments was less attractive, but most respondents were still willing to consider it. Not being fully informed about the study was the greatest concern regarding participation in research across the entire cohort. Overall, 90% or more of the respondents liked research that would benefit people with MS, as well as receiving individual test results and/or study results from the investigators. A similar majority disliked the idea of their health being harmed due to participation, receiving information about the study that was confusing, or difficulty getting to the study location.
We found that the preferred MS research participation characteristics across racial and ethnic groups are similar to previously published data in other areas of medicine. A systematic review reported that perceived lack of access to information is a health barrier to health research participation among racial/ethnic groups, including the absence of bilingual informational material and research staff.25 Effective communication positively influences the decision to participate in clinical trials in minorities.24 Unintended outcomes, such as harm due to study participation and adverse effects from the intervention under investigation, have also been reported to be barriers for research participation in minorities.25 Similar to research in other areas of medicine, we found that altruism (research participation benefiting others in the community), low risk in participation, and individual benefits to participation (such as receiving individual test results) are incentives or facilitators to participate in MS research across racial and ethnic groups.25
African American participants were less likely than White participants to agree that medical research had led to better treatment, which may reflect worse MS outcomes in general in this community and a desire for more effective treatments.3–9 Compared with non-Hispanic participants, Hispanic participants indicated more concern about risks to their employment/legal status and their health insurance coverage. Hispanics were also more concerned about receiving poor-quality medical care and had more mistrust toward the medical team. Similarly, African American participants expressed more concern than White participants about having their personal information released without approval and receiving poor-quality medical care, and they showed more mistrust toward the medical team.
These responses seem to reflect a higher level of distrust among minority groups, as has been reported in other studies,26 as well as greater concern about possible downsides of research participation. Of particular importance, there is a legacy of mistrust for African American individuals due to the Tuskegee Study,27 lack of research integrity, and the history of racism and discrimination against this community. These barriers have been identified in other studies evaluating attitudes on medical research participation,25 with the present findings highlighting that this is similar in MS research participation. To address these concerns, researchers are advised to be as forthcoming and transparent as possible about key details of their study, such as how participants will be treated, the care they will receive, and the protections that are in place to preserve participants’ rights, confidentiality, and well-being.
One factor that generated a higher preference level among minority groups was the potential for research to benefit the respondent’s racial/ethnic group. African American individuals may experience mistrust toward research due to the belief that the research may not benefit their communities.25 This may reflect a recognition among minority group members of inequities in health outcomes and a desire for research to be conducted that could reduce these inequities.
This study adds to the growing body of knowledge about underrepresentation of minority groups in research studies, and the reasons that may underlie this phenomenon. Our contribution is adding the perspectives of people with MS, a chronic and disabling neurologic disease that takes a greater toll on African American and Hispanic individuals. To our knowledge, this is the first study to compare research experiences, attitudes, and concerns across multiple racial and ethnic groups to determine barriers to and facilitators of research engagement. We also asked about information sources that would be consulted and/or trusted for information about research opportunities to assist researchers interested in reaching out to potential study participants.
The survey involved both structured and semistructured open responses to various questions, providing responses easily analyzed with standard methods in addition to more personalized responses to specific questions. Questions were developed by a network composed of multiple stakeholders, including people with MS from racial and ethnic minority groups, and reflected concepts obtained from existing literature as well as the personal experiences of the survey development team members.
A limitation of this study was the reliance on a convenience sample that was primarily recruited through e-mail invitations sent out by MS organizations. This biased the sample toward participants who had an internet connection and people who were on the distribution list of one of the participating organizations. These factors may have resulted in higher educational and income levels for this cohort compared with the general MS population and in an underrepresentation of minority group members in this study, the very problem we are working to address. Future studies on this topic would likely benefit from more closely working with health care providers who have a high percentage of patients with MS belonging to racial and ethnic minority groups. In addition, a variety of MS advocacy organizations (including members of the MREPN) have begun programming (eg, conferences, webinars) aimed at minority groups. Partnering with these organizations around these programs to recruit participants for research studies may also aid in the recruitment of a more diverse study population. This requires prioritizing time and flexibility in the recruitment schedule to develop the partnership and align with the schedule of the program.
In summary, this study revealed that people with MS belonging to different races and ethnicities agree about the importance of MS research and are interested in participating in research studies. They are interested in learning about research opportunities and would most trust information that is provided by their health care providers and MS organizations. Barriers that deter minority group members from participating in studies include mistrust, concerns about receiving poor-quality medical care, and risks to insurance coverage or legal status. Researchers who are interested in recruiting diverse study cohorts may want to specifically address these concerns, for example, by clearly explaining the protections that are in place to protect the rights and well-being of study participants. Researchers can also make their study more attractive to minority groups by highlighting how their study will benefit specific communities. For example, studies of MS treatments could state as an explicit goal the comparison of outcomes in different racial or ethnic groups.
Researchers are advised to build relationships with individuals and organizations in the communities they wish to engage in a study. These partners can provide important perspectives on the needs, interests, and concerns of their community as well as assist with study design, communications, and recruitment strategies. Involving people with MS belonging to diverse groups in activities such as patient-focused drug development or community-based participatory research could have even more profound effects on overall engagement, leading to greater trust, mutual respect, and, ultimately, the development of evidence benefiting all groups.
The present findings highlight just one aspect of minority representation in MS research: patients’ perspectives and the factors that influence their decisions to participate in research. Two other groups are also important to focus on as influencers of study participation: researchers who design studies and recruit participants and clinicians who are viewed by their patients as trusted sources of information and could serve as conduits of information about research opportunities. Research into their experiences and perspectives would help to round out our understanding of the factors affecting MS research diversity and could point the way to new strategies for correcting this longstanding imbalance.
PRACTICE POINTS
Historically, minorities have had specific concerns regarding participation in research, such as risks to employment, legal status, and mistrust of the research team.
Researchers and clinicians should address these concerns to recruit a diverse study sample but should also be aware that people in all groups recognize the value of research and are willing to participate in studies.
Involving people with MS belonging to diverse groups in activities such as patient-focused drug development or community-based participatory research could have even more profound effects on overall research engagement.
Supplementary Material
Acknowledgments
The authors acknowledge the organizations and clinics that helped disseminate the survey: Can Do Multiple Sclerosis, Multiple Sclerosis Foundation, MS Views and News, Shepherd Center, Stanford Neuroimmunology Clinic, and The University of Texas Southwestern Medical Center. We also thank the people with MS who participated in the survey.
Footnotes
Financial Disclosures: Dr Machemer receives financial compensation from Genentech Inc. Dr Livingston receives financial compensation from EMD Serono Inc. The other authors declare no conflicts of interest.
Funding/Support: This study was funded by a Eugene Washington PCORI Engagement Award made by PCORI. Manuscript writing was supported by a Sylvia Lawry Physician Fellowship Grant through the National Multiple Sclerosis Society.
Prior Presentations: Aspects of this study have been presented as a poster and platform presentation at the Neurology Research Celebration, May 2019 and May 2018, University of Massachusetts Medical School, Worcester, MA, and as a poster at the Consortium of Multiple Sclerosis Centers (CMSC) Annual Meeting, May 2018, Nashville, TN, and Americas Committee on Treatment and Research in MS, February 2018, San Diego, CA.
References
- 1.Wallin MT, Culpepper WJ, Coffman P et al. The Gulf War era multiple sclerosis cohort: age and incidence rates by race, sex and service. Brain. 2012;135(pt 6):1778–1785. doi: 10.1093/brain/aws099. [DOI] [PubMed] [Google Scholar]
- 2.Langer-Gould A, Brara SM, Beaber BE, Zhang JL. Incidence of multiple sclerosis in multiple racial and ethnic groups. Neurology. 2013;80:1734–1739. doi: 10.1212/WNL.0b013e3182918cc2. [DOI] [PubMed] [Google Scholar]
- 3.Kimbrough DJ, Sotirchos ES, Wilson JA et al. Retinal damage and vision loss in African American multiple sclerosis patients. Ann Neurol. 2015;77:228–236. doi: 10.1002/ana.24308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Weinstock-Guttman B, Ramanathan M, Hashmi K et al. Increased tissue damage and lesion volumes in African Americans with multiple sclerosis. Neurology. 2010;74:538–544. doi: 10.1212/WNL.0b013e3181cff6fb. [DOI] [PubMed] [Google Scholar]
- 5.Howard J, Battaglini M, Babb JS et al. MRI correlates of disability in African-Americans with multiple sclerosis. PLoS One. 2012;7:e43061. doi: 10.1371/journal.pone.0043061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kister I, Chamot E, Bacon JH et al. Rapid disease course in African Americans with multiple sclerosis. Neurology. 2010;75:217–223. doi: 10.1212/WNL.0b013e3181e8e72a. [DOI] [PubMed] [Google Scholar]
- 7.Naismith RT, Trinkaus K, Cross AH. Phenotype and prognosis in African-Americans with multiple sclerosis: a retrospective chart review. Mult Scler. 2006;12:775–781. doi: 10.1177/1352458506070923. [DOI] [PubMed] [Google Scholar]
- 8.Cree BAC, Khan O, Bourdette D et al. Clinical characteristics of African Americans vs Caucasian Americans with multiple sclerosis. Neurology. 2004;63:2039–2045. doi: 10.1212/01.wnl.0000145762.60562.5d. [DOI] [PubMed] [Google Scholar]
- 9.Weinstock-Guttman B, Jacobs LD, Brownscheidle CM et al. Multiple sclerosis characteristics in African American patients in the New York State Multiple Sclerosis Consortium. Mult Scler. 2003;9:293–298. doi: 10.1191/1352458503ms909oa. [DOI] [PubMed] [Google Scholar]
- 10.Marrie RA, Cutter G, Tyry T, Vollmer T, Campagnolo D. Does multiple sclerosis-associated disability differ between races? Neurology. 2006;66:1235–1240. doi: 10.1212/01.wnl.0000208505.81912.82. [DOI] [PubMed] [Google Scholar]
- 11.Shabas D, Heffner M. Multiple sclerosis management for low-income minorities. Mult Scler. 2005;11:635–640. doi: 10.1191/1352458505ms1215oa. [DOI] [PubMed] [Google Scholar]
- 12.Rivas-Rodríguez E, Amezcua L. Ethnic considerations and multiple sclerosis disease variability in the United States. Neurol Clin. 2018;36:151–162. doi: 10.1016/j.ncl.2017.08.007. [DOI] [PubMed] [Google Scholar]
- 13.Khan O, Williams MJ, Amezcua L, Javed A, Larsen KE, Smrtka JM. Multiple sclerosis in US minority populations: clinical practice insights. Neurol Clin Pract. 2015;5:132–142. doi: 10.1212/CPJ.0000000000000112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wilder J, Saraswathula A, Hasselblad V, Muir A. A systematic review of race and ethnicity in hepatitis C clinical trial enrollment. J Natl Med Assoc. 2016;108:24–29. doi: 10.1016/j.jnma.2015.12.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Scalici J, Finan MA, Black J et al. Minority participation in Gynecologic Oncology Group (GOG) studies. Gynecol Oncol. 2015;138:441–444. doi: 10.1016/j.ygyno.2015.05.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Williams M, Powers M, Yun Y-G, Foa E. Minority participation in randomized controlled trials for obsessive–compulsive disorder. J Anxiety Disord. 2010;24:171–177. doi: 10.1016/j.janxdis.2009.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cree BAC, Al-Sabbagh A, Bennett R, Goodin D. Response to interferon beta-1a treatment in African American multiple sclerosis patients. Arch Neurol. 2005;62:1681–1683. doi: 10.1001/archneur.62.11.1681. [DOI] [PubMed] [Google Scholar]
- 18.Cree BAC, Stuart WH, Tornatore CS, Jeffery DR, Pace AL, Cha CH. Efficacy of natalizumab therapy in patients of African descent with relapsing multiple sclerosis: analysis of AFFIRM and SENTINEL data. Arch Neurol. 2011;68:464–468. doi: 10.1001/archneurol.2011.45. [DOI] [PubMed] [Google Scholar]
- 19.US Food and Drug Administration Drug trials snapshots: OCREVUS. Accessed June 30, 2020. https://www.fda.gov/drugs/drug-approvals-and-databases/drug-trials-snapshots-ocrevus. [Google Scholar]
- 20.Burke JF, Brown DL, Lisabeth LD, Sanchez BN, Morgenstern LB. Enrollment of women and minorities in NINDS trials. Neurology. 2011;76:354–360. doi: 10.1212/WNL.0b013e3182088260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Buchanan RJ, Zuniga MA, Carrillo-Zuniga G et al. A pilot study of Latinos with multiple sclerosis: demographic, disease, mental health, and psychosocial characteristics. J Soc Work Disabil Rehabil. 2011;10:211–231. doi: 10.1080/1536710X.2011.622959. [DOI] [PubMed] [Google Scholar]
- 22.Knepper TC, McLeod HL. When will clinical trials finally reflect diversity? Nature. 2018;557:157–159. doi: 10.1038/d41586-018-05049-5. [DOI] [PubMed] [Google Scholar]
- 23.Ramamoorthy A, Pacanowski MA, Bull J, Zhang L. Racial/ethnic differences in drug disposition and response: review of recently approved drugs. Clin Pharmacol Ther. 2015;97:263–273. doi: 10.1002/cpt.61. [DOI] [PubMed] [Google Scholar]
- 24.Kurt A, Semler L, Jacoby JL et al. Racial differences among factors associated with participation in clinical research trials. J Racial Ethn Health Disparities. 2017;4:827–836. doi: 10.1007/s40615-016-0285-1. [DOI] [PubMed] [Google Scholar]
- 25.George S, Duran N, Norris K. A systematic review of barriers and facilitators to minority research participation among African Americans, Latinos, Asian Americans, and Pacific Islanders. Am J Public Health. 2014;104:e16–e31. doi: 10.2105/AJPH.2013.301706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.McDonald JA, Vadaparampil S, Bowen D et al. Intentions to donate to a biobank in a national sample of African Americans. Public Health Genomics. 2014;17:173–182. doi: 10.1159/000360472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Shavers VL, Lynch CF, Burmeister LF. Knowledge of the Tuskegee study and its impact on the willingness to participate in medical research studies. J Natl Med Assoc. 2000;92:563–572. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.