

Abstract
Background:
Among Black Americans, interpersonal racial discrimination is common. Stress, including following discrimination, contributes to pregnancy complications. In this secondary analysis, we provide data on associations among discrimination, stress, and their interaction across the life course and inflammation, perceived stress, and depressive symptoms during pregnancy.
Methods:
During the early third trimester, Black American women (n=93) completed the Experiences of Discrimination Scale, Stress and Adversity Inventory, Perceived Stress Scale, and Center for Epidemiologic Studies Depression Inventory. Plasma interleukin(IL)-6, IL-8, tumor necrosis factor(TNF)-α, and IL-β levels were quantified. Associations were examined by linear regression, controlling for demographic, behavioral, and clinical covariates.
Results:
Associations among racial discrimination and plasma IL-8, TNF-α, and IL-β levels depended upon average ratings of life course stress. When stress was low, discrimination in the mid tertile was associated with the highest levels of IL-8, TNF-α, and IL-β. Subscale analyses suggested that findings related to IL-8 were driven by chronic stress whereas findings related to TNF-α and IL-β were driven by acute stress. When examined together, greater discrimination but not greater life course stress was associated with higher prenatal perceived stress. In subscale analyses, the association between discrimination and prenatal perceived stress depended upon average ratings of life course acute stress. When acute stress was low, discrimination in the mid tertile was associated with the highest levels of prenatal perceived stress. When acute stress was high, discrimination in the high tertile was associated with the highest levels of prenatal perceived stress. There were also direct associations among greater life course chronic stress, prenatal perceived stress, and prenatal depressive symptoms. Associations were attenuated when discrimination was included as a covariate.
Conclusions:
The current analyses suggest that among Black Americans, prenatal inflammation, perceived stress, and depressive symptoms may be shaped by racial discrimination and stress across the life course. In many cases, associations among discrimination and prenatal parameters depended upon how stressful exposures to life course stressors had been rated. The data suggest the potential for adaptive plasticity under some stress and highlight the deleterious nature of compounding stress.
Keywords: African Americans, Cytokines, Maternal-Child Nursing, Obstetrics, Stress, Psychological
Among Black Americans, interpersonal experiences with discrimination on the basis of race, ethnicity, or color are common and begin early in life (Assari, 2020; Daniels et al., 2020; Nong et al., 2020). Exposure to this socially-constructed psychological stressor appears to play a significant role in bringing about the disparities that have traditionally been termed “racial health disparities,” potentially via psychoneuroimmunologic mechanisms (Larrabee Sonderlund et al., 2021). For example, Black American women are at greater risk for hypertensive disorders of pregnancy and preterm birth than White American women (Thompson & Suter, 2020), which are major contributors to the racial disparities witnessed in maternal and infant mortality (Chambers et al., 2019; Gyamfi-Bannerman et al., 2020).
One aspect of the maternal stress experience that remains understudied is that of interpersonal racial discrimination and how this unique form of stress interacts with alternative forms of stress (e.g., interpersonal loss, physical danger, humiliation, entrapment, role disruption (Slavich & Shields, 2018)) to shape physiological and psychological health during pregnancy. Multiple frameworks in the stress sciences suggest that wear and tear occurs when stressor exposures are many (Geronimus, 1996; McEwen, 1998), suggesting that increasing levels of each form of stress may potentiate the effects of others. When stress is prolonged or anticipated frequently, such as with racial discrimination, physiological mechanisms meant to protect the body from repeated activation of stress systems (e.g., decreased sensitivity to glucocorticoids) have also been known to inadvertently introduce alternative forms of risk (e.g., decreased ability of glucocorticoids to dampen inflammation) (Barnes & Adcock, 2009). Indeed, racial discrimination has been linked to perinatal glucocorticoid resistance and systemic inflammation (Gillespie & Anderson, 2018; Giurgescu et al., 2016). During chronic stress, psychological coping mechanisms may also reach capacity, increasing risk for and depressed mood, which has been noted during pregnancy (reviewed by Traylor et al., 2020).
To advance our understanding of these important topics, we examined associations among interpersonal racial discrimination, stress, and their interaction across the life course and inflammation, perceived stress, and depressive symptoms during pregnancy among Black American women. We also completed subscale analyses in which stress ratings were partitioned into chronic versus acute stress to determine whether patterns of associations depended upon the nature of the stress experience. The a priori hypotheses of this work were that associations among interpersonal racial discrimination and prenatal parameters would be stronger under conditions of significant life course stress, signifying a progressive toll on physiological and psychological coping capacity. We hypothesized that greater chronic stress (as opposed to acute stress) combined with more experiences of interpersonal racial discrimination would be particularly deleterious.
Methods
Design
A prospective cohort of Black American women were enrolled into the PATH Study (Pathways to Shortened Gestation among Black Women) during their early third trimester of pregnancy. The primary aims of the parent study were to examine associations among psychological stress, genetic variation, functional regulation of the interleukin-1β signaling pathway, and birth timing. Here, we’ve conducted a series of secondary analyses focusing on racial discrimination and markers of systemic inflammation, perceived stress, and depressive symptoms during pregnancy. While the study was powered to address the primary aims of the parent study, post hoc power analysis suggests that our sample size of 93 achieves 0.82 power to detect moderate associations (effect size f2=0.15) using multivariate linear regression with the predictors, interactions, and covariates under study. The study was approved by the Ohio State University and OhioHealth Institutional Review Boards, with participants completing written informed consent prior to data collection and receiving $50 in gift cards at the study visit.
Participants
Women were eligible for the PATH Study if they self-identified as non-Hispanic, Black, and U.S.-born. Eligible women were also required to be aged 18–34, and report non-smoking status and no illicit drug use by the second trimester, and a pre-pregnancy body mass index of 18.5 to 39.9. Upon screening for eligibility, women were also asked to self-report if they’d been told that their pregnancy was “high risk” for any reason or that they had a pregnancy-related complication or condition. Women who reported chronic immune-related conditions (diabetes mellitus, chronic hypertension, heart disease, cancer, human immunodeficiency virus, hepatitis, syphilis, rheumatoid arthritis, sickle cell disease) were deemed ineligible, though post-birth medical record review later identified chronic hypertension among several women. This was relatively rare (n=6) and these individuals were retained in the sample. While mental health conditions have also been considered chronic immune-related conditions, since stress and its correlates were a primary interest of this study, women with diagnoses of depression or anxiety remained eligible. Similarly, while women self-reporting gestational diabetes, a gestational hypertensive disorder, or fetal anomaly before the third trimester were deemed ineligible, several women were later diagnosed with a gestational hypertensive disorder (n = 12) and were retained in the sample. Women with regular medication use with immune implications (e.g., corticosteroids, albuterol more than once weekly) were not eligible. Women were also required to have a dating ultrasound at less than or equal to 15 weeks of pregnancy.
Data Collection
Participants completed a single study visit during the early third trimester of pregnancy. Demographic, behavioral, and clinical data were collected using standardized questionnaires and the psychosocial instruments discussed below were administered. At the conclusion of the visit, venipuncture was performed for collection of whole blood. Participants were then prospectively followed to birth and additional clinical data were manually abstracted during a detailed review of prenatal, labor and delivery, and newborn medical records that occurred during the postpartum period and covered the entire course of the pregnancy and perinatal period.
Measures
Racial Discrimination
The Experiences of Discrimination Scale (EOD) measures self-reported experiences of discrimination on the basis of race, ethnicity, or color across the life course, up to the time of assessment (Krieger, 1990; Krieger & Sidney, 1996). Participants are asked if they have experienced discrimination in the context of one or more situation out of nine assessed situations (e.g., getting service in a store or restaurant, at school, at work). The frequency of an unendorsed situation is scored as zero. For each endorsed situation, the frequency is scored as one (once), two and one half (two to three times), or five (≥ four times). To produce a total frequency, the frequency scores are summed. Test-retest reliability was 0.7 and Cronbach’s α was 0.86 for the EOD among Black samples (Krieger et al., 2005).
Life Course Stress
The Stress and Adversity Inventory (STRAIN) was created to allow for the systematic, computer-based query of experiences with 96 stressors that might be encountered across the life course (e.g., chronic stressors such as relationship problems, acute stressors such as deaths of relatives) (Slavich & Shields, 2018). Its development was guided by tools such as the Life Events and Difficulties Schedule (an extensive, time-intensive interview and panel rating approach (Brown & Harris, 1978)). The STRAIN is now a National Institute of Mental Health Research Domain Criteria-recommended instrument. The STRAIN uses extensive branching logic and can be administered by interview (as was done for the currently study) or completed independently by the participant. Questions that are not pertinent to the participant are not asked. Endorsed stressors are probed further to determine the timing and duration of the stressor and how stressful or threatening the experience was perceived to be by the participant. The STRAIN produces multiple indices of life course stress, including total life course stress up to the point of assessment. Total life course stress can also be partitioned into chronic versus acute stress. The current study examined average ratings of total (for primary analyses), chronic, and acute (for subscale analyses) life course stress. Greater life course stress, as estimated by the STRAIN, correlates positively with perceived stress and depressive symptoms in adulthood and negatively with healthy prenatal behaviors and ratings of wellbeing (McLoughlin, Fletcher, Slavich, Arnold, & Moore, 2021; Smith et al., 2020). STRAIN indices are not significantly associated with personality traits or social desirability and test-retest reliability over a period of two to four weeks is excellent (r ≥ 0.9) (Slavich & Shields, 2018).
Prenatal Perceived Stress
The Perceived Stress Scale (PSS-14) is a widely used stress assessment tool guided by the notion that negative emotional states arise when events are appraised as threating or overwhelming coping resources (Cohen et al., 1995). Participants are asked to reflect on the past month and indicate if they have never, almost never, sometimes, fairly often, or very often had each of a possible 14 experiences (e.g., been upset because of something that happened unexpectedly). Each item is scored from zero to four (with seven items reverse scored). Higher scores indicate greater perceived stress, with a possible range of 0–56. The PSS-14 has been validated in representative samples across various age and racial groups, including during pregnancy. PSS scores correlate positively with depressive symptoms and negatively with physical and mental health-related quality of life among pregnant women (Zhang et al., 2019).
Prenatal Depressive Symptoms
The Center for Epidemiologic Studies Depression Scale (CES-D) was developed to measure depressive symptoms among the general population (Radloff, 1977). Participants are asked to reflect on the past week and indicate if they rarely, some of the time, occasionally, or most of the time experienced feelings consistent with each of twenty statements (e.g., I felt I was just as good as other people). Each items is scored from zero to three (with four items reverse scored). Higher scores indicate more depressive symptoms, with a possible range of 0–60. The CES-D does not appear to demonstrate racial/ethnic bias and demonstrates an internal validity of 0.88–0.92 during pregnancy (Canady et al., 2009; Maloni et al., 2005). The CES-D also shows predictive validity for DSM-determined minor (CES-D≥16) and major (CES-D≥24) perinatal depression among Black American women (Tandon et al., 2012).
Prenatal Inflammatory Markers
Prenatal venous whole blood samples were stored on ice after collection, returned to the laboratory within an hour of venipuncture, and processed immediately. Plasma was isolated from heparinized whole blood by centrifugation at 1200g for 10 minutes at 15°C. Plasma was aliquoted and frozen at −80°C until thawed in batches for multiplexed (simultaneous) quantification of interleukin (IL)-6, IL-8, tumor necrosis factor (TNF)-α, and IL-β using the Meso Scale Discovery Pro-Inflammatory 4-plex kit and Sector Imager 2400 (Meso Scale Discovery, Gaithersburg, MD). This method applies the principles of sandwich immunoassay through the use of electrochemiluminescence. All cytokines were quantified upon sample first thaw. For the PATH Study sample, inter- and intra-assay coefficients of variations were 4.0% and 7.1% for IL-6, 3.6% and 4.0% for IL-8, 7.2% and 3.9% for TNF-α, and 2.3% and 15.5% for IL-1β, respectively.
Statistical Analyses
First, participant characteristics were described and primary variable descriptive statistics produced. Next, bivariate associations among untransformed continuous variables of interest were examined according to Spearman rank-order correlations. Next, variables were examined for normality. Transformations were applied to plasma cytokine values (log, 1/square root, inverse, and log for IL-6, IL-8, TNF-α, and IL-1β, respectively) to address the significant positive skew of the cytokine distributions, as is common for systemic inflammatory markers. This approach allows a linear model to be fit by addressing non-normality and heteroscedasticity of model error terms while also maintaining power, maximizing precision, and minimizing risk for Type I error (Knief & Forstmeier, 2021). For models in which a transformation with an element of inversion was applied to the dependent variable (i.e., IL-8 and TNF-α), directions of associations are reversed in the results text to assist the reader with interpretation.
Next, separate multivariate linear regression models were built with racial discrimination tertile (X1), average life course stress rating (X2), and their interaction (X1*X2) serving as predictors and prenatal cytokine levels, perceived stress, and depressive symptoms as outcomes (Y). All models included the following covariates: maternal age, marital status, health insurance, smoking status, pre-pregnancy body mass index, sleep quality (assessed using the Pittsburgh Sleep Quality Index (Buysse et al., 1989)), maternal parity (nulliparous versus multiparous), fetal sex, gestational age at sampling, and time of day of sampling. Based on our initial hypotheses, frequency of exposures to racial discrimination and average ratings of life course stress were each included as continuous predictors. Upon noting multiple quadratic trends when discrimination served as the predictor, the discrimination variable was recoded as tertiles to aid in the interpretation of the results.
Results
Participant Characteristics
Participant characteristics for the analytical sample (n = 93) are shown in Table 1. The PATH Study enrolled 96 women, with a target enrollment and data collection window of 28 weeks 0 days to 32 weeks 6 days of pregnancy. Ninety-five (98.96%) participants were enrolled within the target window and one (1.04%) participant was enrolled at 19 weeks 4 days due to an incorrectly reported due date. This participant was retained in the analytical sample and gestational age at sampling was included as a covariate. Three women were excluded from analyses due to unsuccessful venipuncture (n = 2) or inability to obtain prenatal and birth records, prohibiting determination of key descriptive and control variables (n = 1). Therefore, the final analytical sample included 93 non-Hispanic Black American women assessed at a mean 30 weeks 2.3 days of pregnancy (SD 1 week 5.91 days).
Table 1.
Participant Characteristics by Prenatal Self-Reported Depressive Symptoms (n=93)
| Full Analytical Sample (n=93) | Lack Clinically-Significant Depressive Symptoms (n=65) | Clinically-Significant Depressive Symptoms (n=28) | ||
|---|---|---|---|---|
| Mean ± SD or Count (%) | Mean ± SD or Count (%) | Mean ± SD or Count (%) | p value | |
| Maternal age | 26.31 ± 4.47 | 26.77 ± 4.37 | 25.25 ± 4.60 | .133 |
| Married (yes) | 22 (23.66%) | 18 (27.69%) | 4 (14.29%) | .193 |
| Private insurance (yes) | 31 (33.33%) | 25 (38.46%) | 6 (21.43%) | .110 |
| Non-smoker (yes) | 71 (76.34%) | 50 (76.92%) | 21 (75.00%) | .841 |
| Pre-pregnancy body mass index | 28.37 ± 5.70 | 28.31 ± 5.64 | 28.51 ± 5.94 | .880 |
| Sleep quality (PSQI global score) | 7.47 ± 3.43 | 6.68 ± 3.15 | 9.32 ± 3.40 | .001 |
| Nulliparity (yes) | 29 (31.18%) | 20 (30.77%) | 9 (32.14%) | .896 |
| Fetal sex (female) | 51 (54.84%) | 36 (55.38%) | 15 (53.57%) | .872 |
| Gestational age at sampling (days) | 212.33 ± 12.91 | 211.72 ± 10.14 | 213.75 ± 17.92 | .490 |
| Time of day of sampling | 1300 hours ± 93.6 min | 1301 hours ± 94.2 min | 1256 hours ± 91.2 min | .826 |
| Prenatal perceived stress (PSS) | 23.31 ± 8.13 | 19.95 ± 6.08 | 31.11 ± 6.88 | <.001 |
| Prenatal Depressive symptoms (CES-D) | 13.57 ± 10.65 | 7.77 ± 4.32 | 27.04 ± 8.54 | <.001 |
Note. PSQI = Pittsburgh Sleep Quality Index; hours = hours (military time); min = minutes; PSS = Perceived Stress Scale; CES-D = Center for Epidemiologic Studies Depression Scale; Lack Clinically-Significant Depressive Symptoms = CES-D Score <16; Clinically-Significant Depressive Symptoms = CES-D Score ≥16
Consistent with the study’s recruitment strategies and eligibility criteria, most participants did not report private insurance (n = 62; 66.67%) and were employed at least part time during pregnancy (n = 68; 73.12%). No participants reported type 1 or type 2 diabetes or gestational diabetes, and six (6.45%) participants were diagnosed with chronic hypertension before (n = 3) or during (n = 3) pregnancy per medical record review. Nine (9.68%) participants were diagnosed with gestational hypertension and three (3.2%) participants were diagnosed with preeclampsia during the assessed pregnancy. No participants demonstrated abnormalities of amniotic fluid volume. Four participants (4.30%) developed chorioamnionitis. The mean gestational age at birth was 39 weeks 0.37 days (SD =1 week 2.68 days).
Of the 93 assessed participants, 65 (69.90%) had a CES-D score ≥ 16 which represents clinically-significant depressive symptoms. As shown in Table 1, participants with clinically-significant depressive symptoms reported higher prenatal perceived stress (t(91) = −7.800, p < .001) and higher prenatal depressive symptoms (t(91)=−14.458, p < .001) compared to participants without clinically-significant depressive symptoms.
Descriptive Statistics and Bivariate Associations
Women were divided into tertiles based on frequency of exposures to discrimination, with the low tertile encompassing those reporting no experiences (n = 47; 50.5%), the mid tertile encompassing those reporting one to three experiences (n = 19; 20.5%), and the high tertile encompassing those reporting more than three experiences (n = 27; 29.0%) of interpersonal racial discrimination. Participants reported experiencing, on average, three instances of individual racial discrimination (SD = 4.94). Participants also reported experiencing, on average, 21.9 life course stressors out of an assessed 96 potential life course stressors (SD = 12.6; 25% = 13, 50% = 21, 75% = 26). Average ratings of life course stress across these stressors ranged from 0 to 4.36 on a scale of 0 to 5 from not at all to extremely stressful (M = 2.29, SD = 0.75, 25th percentile = 1.85, 50th percentile = 2.28, 75th percentile = 2.73).
Bivariate spearman rank-order associations among the primary variables of interest are shown in Table 2. Participants reporting more instances of racial discrimination reported greater average ratings of life course chronic stress, prenatal perceived stress, and prenatal depressive symptoms (ρ ≥ .234). Participants reporting greater average total life course stress reported greater prenatal perceived stress and prenatal depressive symptoms (ρ ≥ .22). Greater average ratings of total life course stress were also associated with higher plasma IL-1β levels (ρ = .232, p = .025). Greater average ratings of life course acute stress were associated with higher plasma IL-8 (ρ = .242, p = .020) and IL-1β (ρ = .295, p = .004) levels.
Table 2.
Spearman associations among racial discrimination, life course stress, and prenatal parameters (n = 93)
| 1.1 | 1.2 | 1.3 | 1.4 | 2.1 | 2.2 | 2.3 | 2.4 | 2.5 | 2.6 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Life Course Parameters (ρ) | ||||||||||
| 1.1 Racial discrimination | 1.0 | - | ||||||||
| 1.2 Life course stress (total) | 0.183 | 1.0 | - | |||||||
| 1.3 Life course stress (chronic) | 0.234* | 0.712* | 1.0 | - | ||||||
| 1.4 Life course stress (acute) | 0.025 | 0.758* | 0.187 | 1.0 | - | |||||
| 2. Prenatal Parameters (ρ) | ||||||||||
| 2.1 Perceived stress | 0.257* | 0.267* | 0.364* | 0.003 | 1.0 | - | ||||
| 2.2 Depressive symptoms | 0.241* | 0.222* | 0.347* | −0.073 | 0.777* | 1.0 | - | |||
| 2.3 Plasma IL-6 | −0.087 | 0.050 | 0.138 | −0.050 | 0.129 | 0.092 | 1.0 | - | ||
| 2.4 Plasma IL-8 | 0.189 | 0.193 | 0.089 | 0.242* | 0.118 | 0.115 | 0.016 | 1.0 | - | |
| 2.5 Plasma TNF-α | −0.017 | 0.033 | 0.107 | 0.037 | 0.135 | 0.178 | 0.280* | 0.226* | 1.0 | - |
| 2.6 Plasma IL-1β | 0.017 | 0.232* | 0.004 | 0.295* | 0.058 | 0.075 | 0.054 | 0.195 | 0.169 | 1.0 |
Note. Life course stress is operationalized as average stress rating across stressors; IL = interleukin; TNF = tumor necrosis factor; for Spearman rank-order associations, variables are untransformed
p ≤ .05;
Discrimination, Total Life Course Stress, and Prenatal Inflammatory Markers
Multivariate linear regression models revealed that associations among racial discrimination and plasma IL-8, TNF-α, and IL-β levels depended upon average ratings of total life course stress, adjusting for demographic, behavioral, and clinical covariates (p values ≤ 0.034; Figures 1a, 1b, and 1c, respectively). For each of the three models, orthogonal polynomial contrasts also revealed the presence of a quadratic trend when discrimination tertile served as the predictor (F(1, 77)IL-8 = 8.91, p = .004; F(1, 77)TNF-α = 6.74, p = .011; F(1, 77)IL-β=5.67, p = .020).
Figure 1. Associations among racial discrimination and prenatal inflammatory markers depend upon average ratings of life course stress.
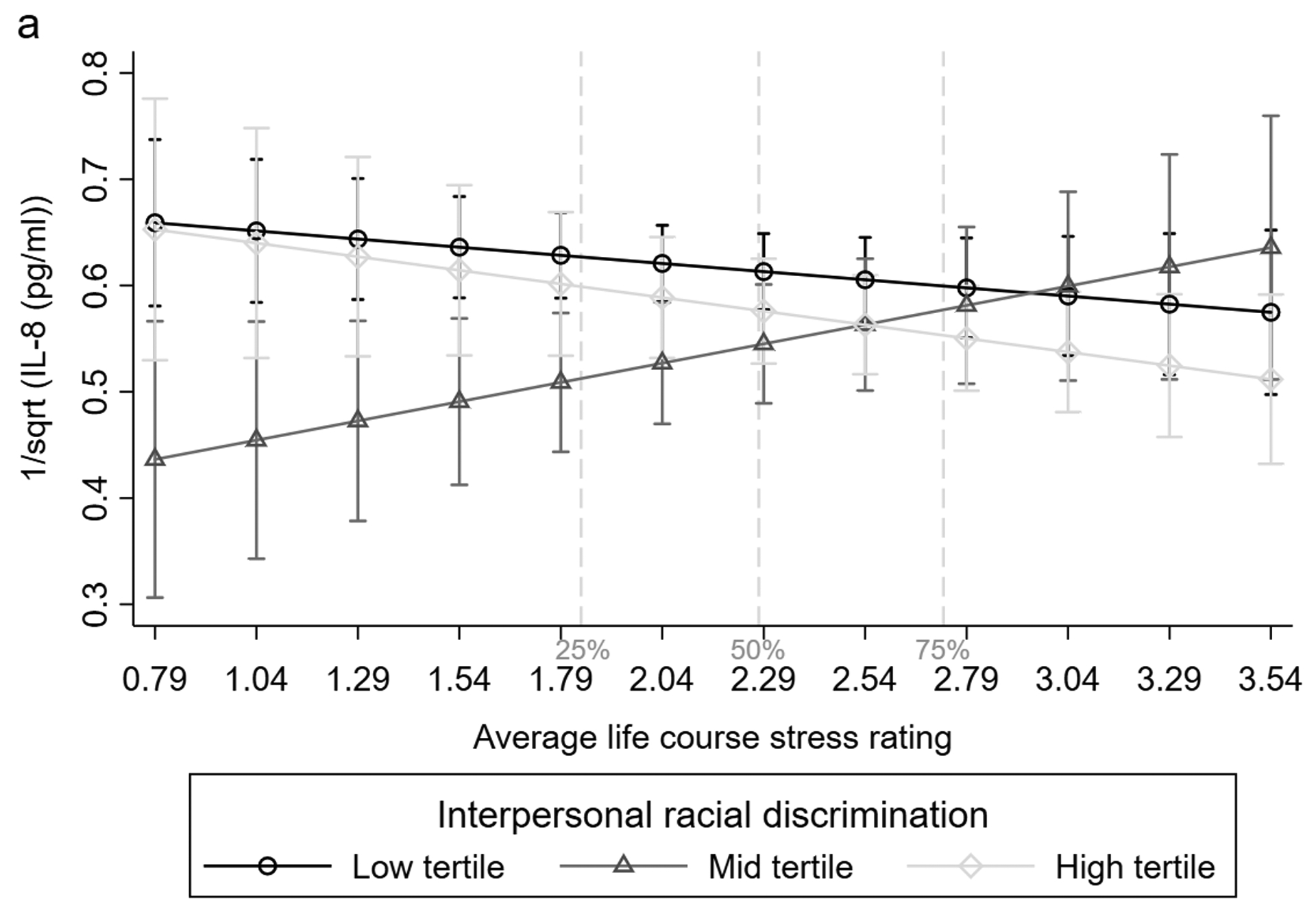
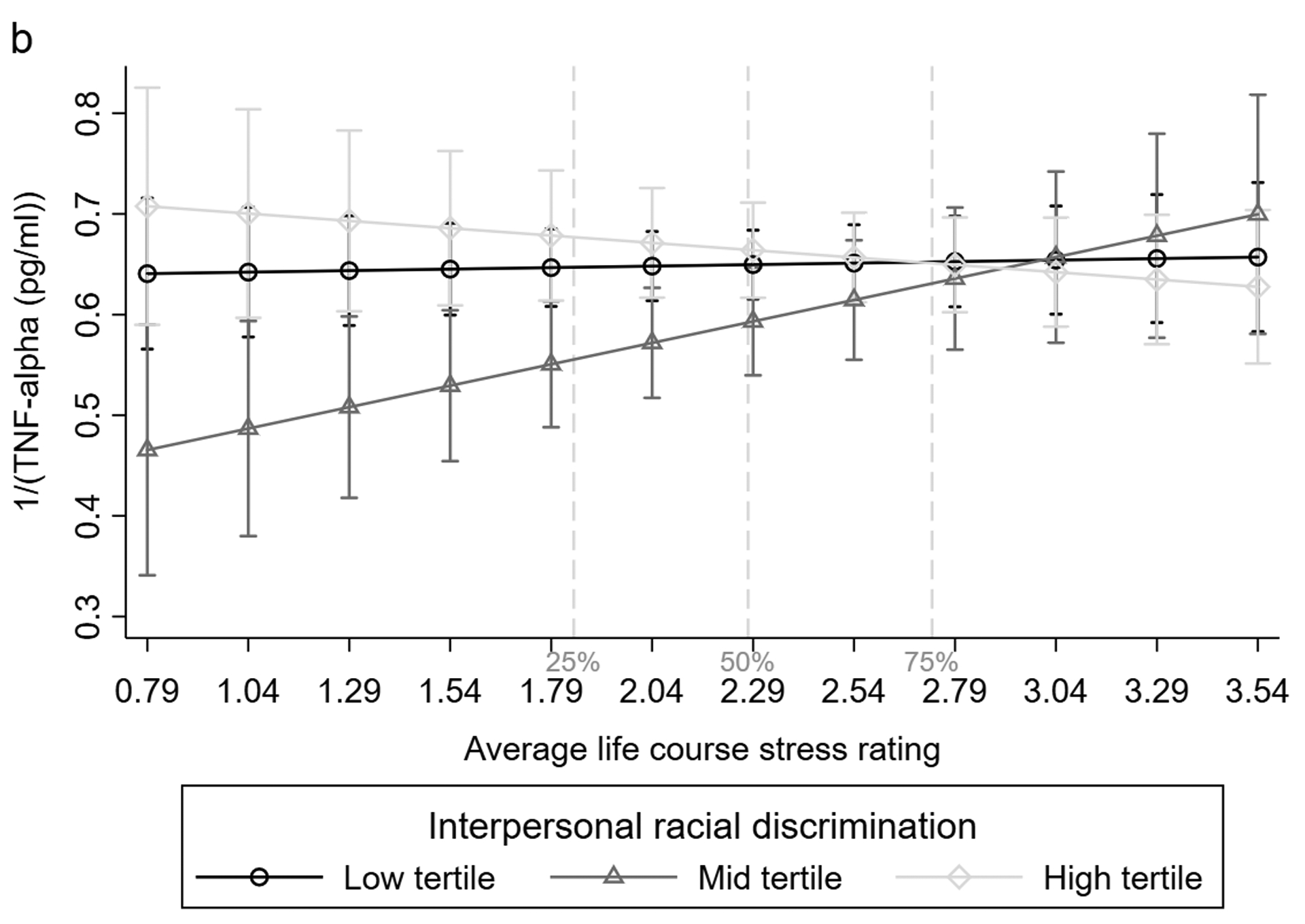
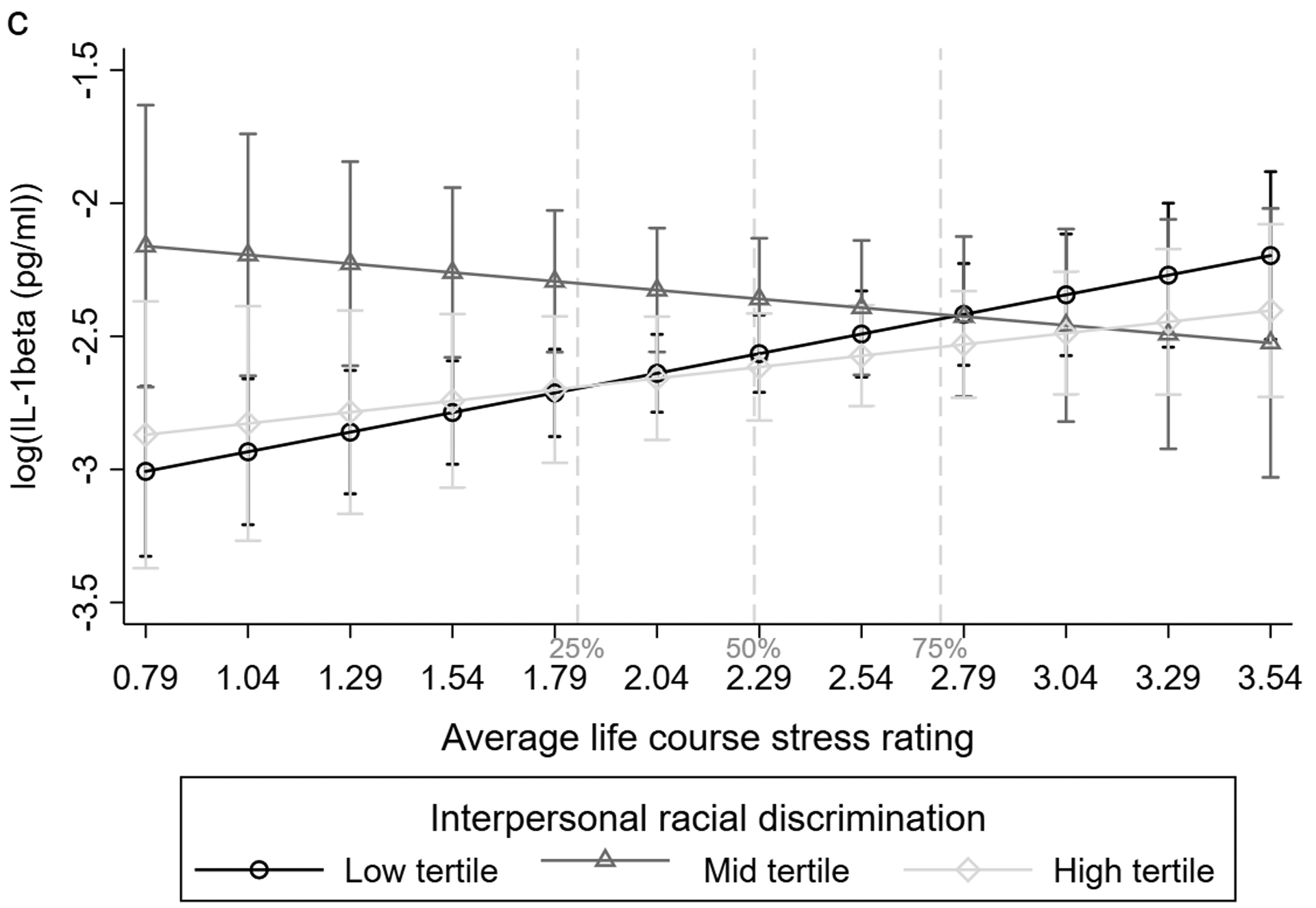
Associations among racial discrimination and a) IL-8, b) TNF-α, and c) IL-1β as a function of life course stress. Cytokine values are transformed. 95% confidence intervals are shown. Estimates are adjusted for maternal age, marital, insurance, and smoking status, pre-pregnancy body mass index, sleep quality, nulliparity, fetal sex, and gestational age and time of day at sampling. Dashed lines represent the cohort 25th, 50th, and 75th percentiles for average ratings of life course stress. IL=interleukin; TNF=tumor necrosis factor; sqrt=square root; pg=picogram; ml=milliliter.
Specifically, participants reporting experiences of racial discrimination in the mid tertile demonstrated significantly higher IL-8 levels than participants reporting discrimination in the low and high tertiles but only when average ratings of total life course stress were below approximately the cohort 50th and 25th percentiles, respectively (interaction: t(77) = 2.16, p = .034; t(77) = 2.39, p = .019, respectively). Participants reporting discrimination in the mid tertile showed significantly higher TNF-α levels than women in the high tertile but only when average ratings of total life course stress were below the cohort 25th percentile (interaction: t(77) = 2.31, p = .024). Participants reporting discrimination in the mid tertile also showed significantly higher TNF-α levels than women in the low tertile (main: β = 0.717, t(77) = 2.12, p = .038). This association did not depend on average total life course stress ratings (interaction: t(77) = −1.73, p = .087). Participants reporting discrimination in the mid tertile also showed significantly higher IL-β levels than the low tertile but only when average total life course stress was below two, corresponding to the approximate 35th percentile (interaction: t(77) = 2.20, p = .031). Participants reporting discrimination in the high tertile did not demonstrate significantly different IL-β levels than those reporting discrimination in the low or mid tertiles (main: β = .200, t(77) = 0.53, p = .459; β = .703, t(77) = 1.43, p = .156, respectively).
There was no evidence of a discrimination*total life course stress interaction in the prediction of maternal plasma IL-6 levels (p values ≥ .402). Therefore, the interaction term was removed and associations among racial discrimination, total life course stress, and IL-6 were examined. No significant associations were witnessed (p values ≥ .323).
Chronic Versus Acute Life Course Stress
In subscale analyses, the relationship between racial discrimination and plasma IL-8 levels depended upon average ratings of chronic life course stress (p values ≤ .035). Relationships among racial discrimination and plasma TNF-α and IL-1β levels depended upon average ratings of acute life course stress (p values ≤ .046), again controlling for pertinent covariates.
Similar to the above, discrimination in the mid tertile predicted significantly higher IL-8 levels than discrimination in the low and high tertiles but only when life course chronic stress was rated below roughly the 50th and 25th percentiles, respectively (interaction: t(77) = 2.14, p = .035; t(77) = 2.68, p = .009, respectively). Discrimination in the mid tertile was associated with significantly higher TNF-α levels than discrimination in the high tertile but only when average life course acute stress was rated below roughly the cohort 35th percentile (interaction: t(77) = 2.12, p = .037). Discrimination in the mid tertile also predicted significantly higher IL-β levels than discrimination in the low and high tertiles but only when average acute life course stress was rated below roughly the 50th and 35th percentiles, respectively (interaction: t(77) = 3.06, p = .003; t(77) = 2.02, p = .046, respectively). As above, neither discrimination, life course chronic stress, life course acute stress, nor their interactions predicted maternal plasma IL-6 levels (p values ≥ .125).
Discrimination, Life Course Stress, and Prenatal Perceived Stress and Depressive Symptoms
Multivariate linear regression models revealed that associations among racial discrimination and prenatal perceived stress and prenatal depressive symptoms did not depend on average ratings of total life course stress, adjusting for pertinent covariates (p values ≥ .181). Therefore, the interaction terms were removed. When examined together, greater racial discrimination but not greater total life course stress predicted higher prenatal perceived stress (main: βmid vs. low = 0.196, t(79) = 1.99, p = .050; βhigh vs. low=0.254, t(79) = 2.43, p = .017). There was a linear trend to the data (F(1, 79) = 5.92, p = .017). Neither discrimination nor total life course stress predicted prenatal depressive symptoms (p values ≥ .116).
Chronic Versus Acute Life Course Stress
In subscale analyses, the relationship between racial discrimination and prenatal perceived stress depended upon average acute life course stress ratings, controlling for pertinent covariates (Figure 2). Discrimination in the mid tertile predicted significantly higher prenatal perceived stress than discrimination in the low tertile but only when average life course acute stress was rated below roughly the mean (interaction: t(77) = 2.22, p = .029). Discrimination in the high tertile predicted significantly higher prenatal perceived stress than discrimination in the mid tertile but only when average acute life course stress was rated above the cohort 90th percentile (interaction: t(77) = 2.01, p = .048).
Figure 2. Associations among racial discrimination and prenatal perceived stress depend upon average ratings of acute stress.
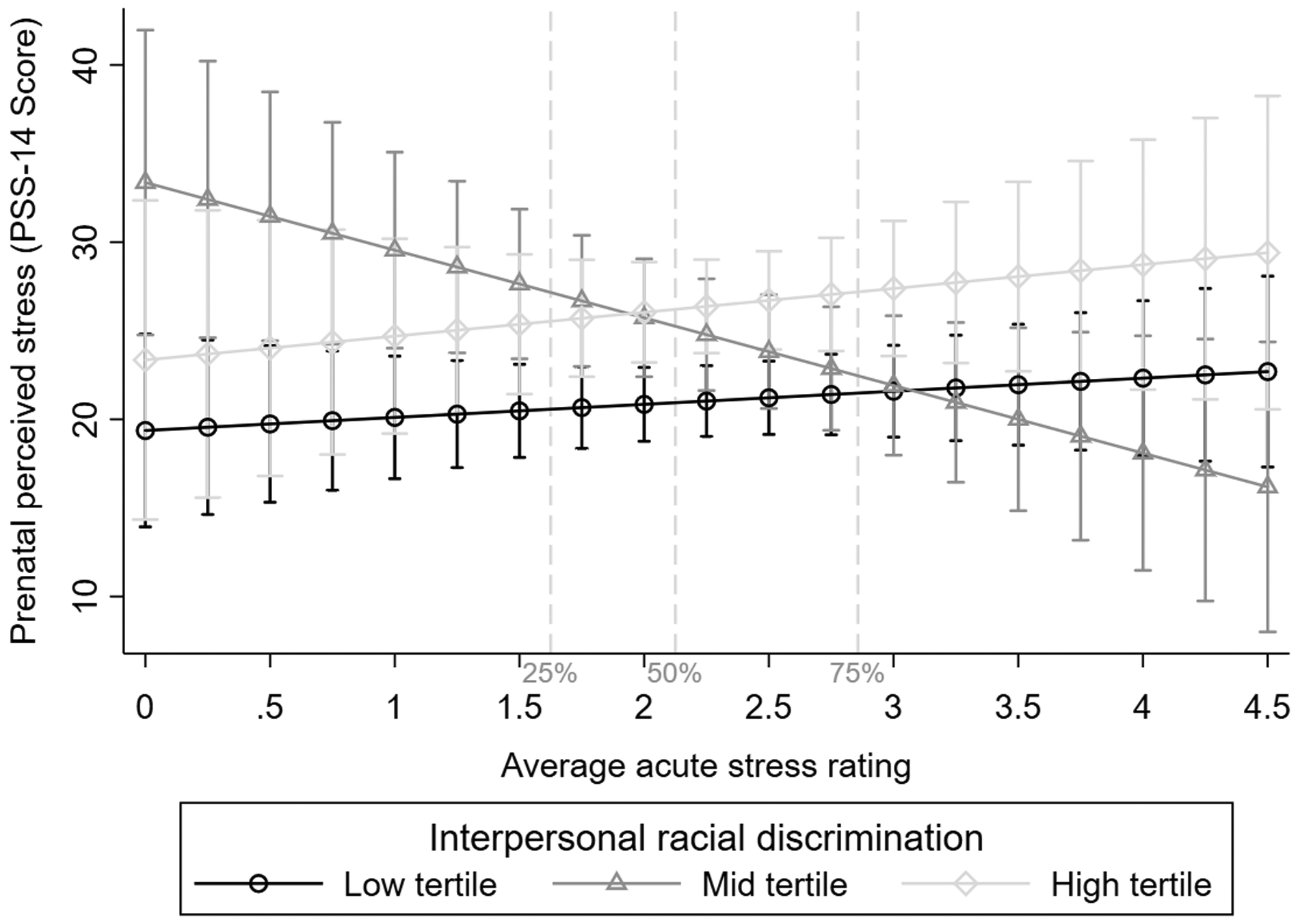
95% confidence intervals are shown. Estimates are adjusted for maternal age, marital, insurance, and smoking status, pre-pregnancy body mass index, sleep quality, nulliparity, fetal sex, and gestational age and time of day at sampling. Dashed lines represent the cohort 25th, 50th, and 75th percentiles for average ratings of acute stress. PSS=perceived stress scale
In removing the interaction terms for models in which there was no evidence of an interaction, greater average life course chronic stress ratings were associated with greater prenatal perceived stress (β = .262, t(80) = 2.55, p = .013) and greater prenatal depressive symptoms (β = .218, t(80) = 2.09, p = .040), holding average ratings of life course acute stress constant. When racial discrimination tertile was also added to these models, associations among average life course chronic stress ratings and prenatal perceived stress and prenatal depressive symptoms were attenuated (β = .203, t(79) = 1.96, p = .053; β = .181, t(79) = 1.70, p = .094).
Discussion
The findings from this secondary analysis are in line with a large literature demonstrating that life course stress, including stress associated with interpersonal racial discrimination, exerts a progressive toll on physiological and psychological coping capacity (Gillespie & Anderson, 2018; Giurgescu et al., 2016). Our findings also add a unique perspective to a growing body of literature suggesting that there are “optimal” levels of life course stress (as opposed to levels that are too high or too low) that can enhance stress responses and health (Dooley et al., 2017; Seery et al., 2013). For example, McEwen and colleagues progressively moved from discussions of stress-associated wear and tear (e.g., McEwen, 1998) to adaptive versus maladaptive plasticity in response to stress (e.g., McEwen & Akil, 2020). Both conceptualizations highlight the deleterious nature of stress when exposures are many, repeated, or prolonged, which can produce allostatic overload. The latter conceptualization also acknowledges the body’s remarkable ability to adapt based on experience. When stress experiences are manageable (“optimal”), the theory posits that we adapt in ways that leave us better prepared to respond to subsequent stressors. While much work remains to advance this important area of science, our findings suggest that an individual’s exposure to stress associated with interpersonal racial discrimination and stress more broadly defined interacts in determining the likelihood of adaptive versus maladaptive plasticity. This is important in discussions of health equity, as interactions may be present even when direct associations among discrimination and health parameters are not evident.
We hypothesized that greater chronic stress combined with greater interpersonal racial discrimination would be particularly deleterious, predicated on the long-held belief that chronic stress exerts considerable wear and tear over time (Dhabhar, 2014). However, we found that the interaction of discrimination and chronic stress predicted IL-8 levels while the interaction of discrimination and acute stress predicted TNF-α and IL-1β levels, suggesting that chronic versus acute stress may play differential roles in determining levels of various pro-inflammatory mediators. While interesting, these findings are not without precedent. For example, some data suggests that levels of IL-8, a chemokine active in neutrophil recruitment, may be particularly susceptible to disturbed sleep during pregnancy, a well-known correlate of chronic stress (Blair et al., 2015). Levels of peripheral TNF-α and IL-1β, potent pro-inflammatory mediators, have been shown to be responsive to beta-adrenergic receptor antagonism or blockade, which is pertinent considering that the immunomodulatory effects of acute stress (i.e., “fight or flight” responses), in particular, are conveyed via beta-adrenergic signaling (Evans et al., 2020). Ross et al. (2019) also recently noted that greater numbers of prenatal but not pre-conception stressful life events predicted third trimester gene expression profiles consistent with enhanced NF-κB and AP-1 activity, suggesting that the timing of stressor exposure may also be of particular importance.
Also of note, while the STRAIN allowed our team to partition life course stress into that which is generally agreed upon to be chronic versus acute in nature, there remains debate regarding how interpersonal racial discrimination should be conceptualized as a stressor. Some instances of racial discrimination are activity-driven (e.g., while driving, shopping, dining). Some are relational (e.g., at school of work). Together, patterns of both discrete and repeated exposures shape physiological stress responses as an individual navigates the world. As such, the threat of exposure to discrimination on its own serves as a salient form of chronic stress during day-to-day activities, a position that is supported by a limited but important qualitative and quantitative literature (e.g., Knighton et al., 2020). Additional studies applying emerging concepts in the stress sciences to the unique and pervasive experience of racial discrimination are not only warranted but imperative to addressing the societally-driven health inequities often described as racial.
Our findings also suggest that patterns of exposures to racial discrimination and broader categories of stress over the life course may play an important role in shaping mental health during pregnancy. First, when considered together, greater discrimination but not greater life course stress predicted prenatal perceived stress, which is consistent with earlier work (Stancil et al., 2000). Though, there is a recent dearth of evidence further exploring such relationships during pregnancy. In addition, when acute stress was low, women in the discrimination mid tertile reported the highest prenatal perceived stress. When acute stress was high, women in the discrimination high tertile reported the highest prenatal perceived stress. Interestingly, chronic stress also seemed to play the most important role in predicting prenatal perceived stress and depressive symptoms, though adjustment for discrimination attenuated these associations. Other studies have supported the presence of a main effect of discrimination on depressive symptoms (Walker Taylor et al., 2018). Such patterns are in line with our original hypotheses and prior literature supporting the potential for a progressive toll on coping capacity. Additional work is needed to understand the relative effects of life course versus current stress, including that associated with racial discrimination, on perinatal mental health, which has been linked to risk for mother and infant, including into childhood.
A major strength of this study is its focus on Black American women, allowing within race comparisons of those with varied life course stress trajectories, including exposures to interpersonal racial discrimination. While past studies have used race as a proxy of exposure to racial discrimination, the descriptive statistics produced for this study as well as past work suggest that interpersonal experiences are varied and must be considered accordingly.
There are also several important limitations to this study. First, while the current study used varied recruitment methods, generalizability of findings must be carefully considered. For example, a large portion of participating women were recruited from sites providing services to patients who are under- or uninsured. Though, women with chronic immune-related conditions, regularly taking medications with immune implications, or reporting a major complication of pregnancy before the third trimester were not eligible for participation. As we note, several women were later discovered to have chronic hypertension (n = 6) or were later diagnosed with a gestational hypertensive disorder (n =12). They were retained in the sample. As such, it is difficult to determine how values for the variables under study may differ among the assessed sample versus the general U.S. population. Greater heterogeneity among the cohort is a priority for future work. Moreover, this study did not collect data on potential mitigating factors, such as social support. This would be informative in future work. This study and many others have also been severely limited in their ability to understand the effects of systemic racism on perinatal health, which is not likely to be captured by standardized surveys with an interpersonal focus. Methodological advancements in this area are sorely needed.
Conclusion
In conclusion, the current analyses suggest that, among Black American women, prenatal inflammatory markers, perceived stress, and depressive symptoms may be shaped by racial discrimination and stress across the life course. In many cases, associations among discrimination and prenatal parameters depended upon how stressful, on average, exposures to life course stressors had been rated. The data suggest the potential for adaptive plasticity under some stress but also highlight the deleterious nature of compounding stress. These findings are important in that greater prenatal inflammation, perceived stress, and depressive symptoms have each been linked to poor birth outcomes, including gestational hypertensive disorders and preterm birth. Interdisciplinary teams are well poised to address the disparities witnessed in such outcomes by carefully considering, expanding, and incorporating data that sheds light on the social and interpersonal phenomena that, together, shape maternal and infant health. Through patient- centered care, the psychological and physiological effects of compounding stress may be screened for, diagnosed, and mitigated, with findings from studies such as this clinically applicable to interventions aimed at combatting maternal and infant morbidity and mortality. Stakeholder-informed development, dissemination, implementation, and evaluation of such clinical programs are critical in promoting perinatal health equity.
Acknowledgements:
We appreciate the contributions of undergraduate research assistants, Amy Kole and Patricia Do, to data collection. We appreciate the contributions of our research participants and partnering care locations.
Conflicts of Interest and Sources of Funding:
No conflicts of interest are declared. This work was supported by the National Institute of Nursing Research of the National Institutes of Health (F31NR01460; SLG); Association of Women's Health, Obstetric and Neonatal Nurses (SLG); Midwest Nursing Research Society (SLG); Sigma Theta Tau International, Epsilon (SLG); Cola-Cola Critical Difference for Women and Department of Women's, Gender and Sexuality Studies, Graduate School, and Office of Diversity and Inclusion of The Ohio State University (SLG). Resources supported by the National Center for Advancing Translational Sciences (UL1TR001070) of the National Institutes of Health were utilized. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies. The funding agencies had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the report for publication.
Footnotes
The authors declare no conflicts of interest.
References
- Assari S (2020). Social epidemiology of perceived discrimination in the united states: Role of race, educational attainment, and income. International Journal of Epidemiologic Research, 7, 136–141. 10.34172/ijer.2020.24 [DOI] [PubMed] [Google Scholar]
- Barnes PJ, & Adcock IM (2009). Glucocorticoid resistance in inflammatory diseases. Lancet, 373, 1905–1917. 10.1016/S0140-6736(09)60326-3 [DOI] [PubMed] [Google Scholar]
- Blair LM, Porter K, Leblebicioglu B, & Christian LM (2015). Poor sleep quality and associated inflammation predict preterm birth: Heightened risk among african americans. Sleep, 38, 1259–1267. 10.5665/sleep.4904 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown GW, & Harris TO (1978). Social origins of depression: A study of psychiatric disorder in women. New York, NY: Free Press. [Google Scholar]
- Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, & Kupfer DJ (1989). The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research, 28, 193–213. 10.1016/0165-1781(89)90047-4 [DOI] [PubMed] [Google Scholar]
- Canady RB, Stommel M, & Holzman C (2009). Measurement properties of the centers for epidemiological studies depression scale (CES-D) in a sample of african american and non-hispanic white pregnant women. Journal of Nursing Measurement, 17(2), 91–104. 10.1891/1061-3749.17.2.91 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chambers BD, Baer RJ, McLemore MR, & Jelliffe-Pawlowski LL (2019). Using index of concentration at the extremes as indicators of structural racism to evaluate the association with preterm birth and infant mortality-california, 2011–2012. Journal of Urban Health : Bulletin of the New York Academy of Medicine, 96, 159–170. 10.1007/s11524-018-0272-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S, Kessler R, & Underwood Gordon L (1995). Measuring stress: A guide for health and social scientists. New York, NY: Oxford University Press. [Google Scholar]
- Daniels KP, Valdez Z, Chae DH, & Allen AM (2020). Direct and vicarious racial discrimination at three life stages and preterm labor: Results from the african american women’s heart & health study. Maternal and Child Health Journal, 24, 1387–1395. 10.1007/s10995-020-03003-4 [DOI] [PubMed] [Google Scholar]
- Dhabhar FS (2014). Effects of stress on immune function: The good, the bad, and the beautiful. Immunologic Research, 58(2–3), 193–210. 10.1007/s12026-014-8517-0 [DOI] [PubMed] [Google Scholar]
- Dooley LN, Slavich GM, Moreno PI, & Bower JE (2017). Strength through adversity: Moderate lifetime stress exposure is associated with psychological resilience in breast cancer survivors. Stress and Health, 33, 549–557. 10.1002/smi.2739 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evans AK, Ardestani PM, Yi B, Park HH, Lam RK, & Shamloo M (2020). Beta-adrenergic receptor antagonism is proinflammatory and exacerbates neuroinflammation in a mouse model of alzheimer’s disease. Neurobiology of Disease, 146, 105089. 10.1016/j.nbd.2020.105089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geronimus AT (1996). Black/white differences in the relationship of maternal age to birthweight: A population-based test of the weathering hypothesis. Social Science & Medicine, 42, 589–597. 10.1016/0277-9536(95)00159-x [DOI] [PubMed] [Google Scholar]
- Gillespie SL, & Anderson CM (2018). Racial discrimination and leukocyte glucocorticoid sensitivity: Implications for birth timing. Social Science & Medicine, 216, 114–123. 10.1016/j.socscimed.2018.08.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giurgescu C, Engeland CG, Templin TN, Zenk SN, Koenig MD, & Garfield L (2016). Racial discrimination predicts greater systemic inflammation in pregnant african american women. Applied Nursing Research, 32, 98–103. 10.1016/j.apnr.2016.06.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gyamfi-Bannerman C, Pandita A, Miller EC, Boehme AK, Wright JD, Siddiq Z, D’Alton ME, & Friedman AM (2020). Preeclampsia outcomes at delivery and race. The Journal of Maternal-Fetal & Neonatal Medicine, 33, 3619–3626. 10.1080/14767058.2019.1581522 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knief U, & Forstmeier W (2021). Violating the normality assumption may be the lesser of two evils. Behavior Research Methods, Advance online publication. 10.3758/s13428-021-01587-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knighton JS, Dogan J, Hargons C, & Stevens-Watkins D (2020). Superwoman schema: A context for understanding psychological distress among middle-class african american women who perceive racial microaggressions. Ethnicity & Health, Advance online publication. 10.1080/13557858.2020.1818695 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krieger N (1990). Racial and gender discrimination: Risk factors for high blood pressure? Social Science & Medicine, 30, 1273–1281. 10.1016/0277-9536(90)90307-e [DOI] [PubMed] [Google Scholar]
- Krieger N, & Sidney S (1996). Racial discrimination and blood pressure: The CARDIA study of young black and white adults. American Journal of Public Health, 86, 1370–1378. 10.2105/ajph.86.10.1370 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krieger N, Smith K, Naishadham D, Hartman C, & Barbeau EM (2005). Experiences of discrimination: Validity and reliability of a self-report measure for population health research on racism and health. Social Science & Medicine, 61, 1576–1596. 10.1016/j.socscimed.2005.03.006 [DOI] [PubMed] [Google Scholar]
- Larrabee Sonderlund A, Schoenthaler A, & Thilsing T (2021). The association between maternal experiences of interpersonal discrimination and adverse birth outcomes: A systematic review of the evidence. International Journal of Environmental Research and Public Health, 18(4). 10.3390/ijerph18041465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maloni JA, Park S, Anthony MK, & Musil CM (2005). Measurement of antepartum depressive symptoms during high-risk pregnancy. Research in Nursing & Health, 28(1), 16–26. 10.1002/nur.20051 [DOI] [PubMed] [Google Scholar]
- McEwen BS (1998). Stress, adaptation, and disease. allostasis and allostatic load. Annals of the New York Academy of Sciences, 840, 33–44. 10.1111/j.1749-6632.1998.tb09546.x [DOI] [PubMed] [Google Scholar]
- McEwen BS, & Akil H (2020). Revisiting the stress concept: Implications for affective disorders. The Journal of Neuroscience, 40(1), 12–21. 10.1523/JNEUROSCI.0733-19.2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLoughlin E, Fletcher D, Slavich GM, Arnold R, & Moore LJ (2021). Cumulative lifetime stress exposure, depression, anxiety, and well-being in elite athletes: A mixed-method study. Psychology of Sport and Exercise, 52, 101823. 10.1016/j.psychsport.2020.101823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nong P, Raj M, Creary M, Kardia SLR, & Platt JE (2020). Patient-reported experiences of discrimination in the US health care system. JAMA Network Open, 3(12), e2029650. 10.1001/jamanetworkopen.2020.29650 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. 10.1177/014662167700100306 [DOI] [Google Scholar]
- Ross KM, Cole SW, Carroll JE, & Dunkel Schetter C (2019). Elevated pro-inflammatory gene expression in the third trimester of pregnancy in mothers who experienced stressful life events. Brain, Behavior, and Immunity, 76, 97–103. 10.1016/j.bbi.2018.11.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seery MD, Leo RJ, Lupien SP, Kondrak CL, & Almonte JL (2013). An upside to adversity?: Moderate cumulative lifetime adversity is associated with resilient responses in the face of controlled stressors. Psychological Science, 24(7), 1181–1189. 10.1177/0956797612469210 [DOI] [PubMed] [Google Scholar]
- Slavich GM, & Shields GS (2018). Assessing lifetime stress exposure using the stress and adversity inventory for adults (adult STRAIN): An overview and initial validation. Psychosomatic Medicine, 80(1), 17–27. 10.1097/PSY.0000000000000534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith T, Johns-Wolfe E, Shields GS, Malat J, Jacquez F, & Slavich GM (2020). Associations between lifetime stress exposure and prenatal health behaviors. Stress and Health, 36(3), 384–395. 10.1002/smi.2933 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stancil TR, Hertz-Picciotto I, Schramm M, & Watt-Morse M (2000). Stress and pregnancy among african-american women. Paediatric and Perinatal Epidemiology, 14, 127–135. 10.1046/j.1365-3016.2000.00257.x [DOI] [PubMed] [Google Scholar]
- Tandon SD, Cluxton-Keller F, Leis J, Le HN, & Perry DF (2012). A comparison of three screening tools to identify perinatal depression among low-income african american women. Journal of Affective Disorders, 136(1–2), 155–162. 10.1016/j.jad.2011.07.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson JA, & Suter MA (2020). Estimating racial health disparities among adverse birth outcomes as deviations from the population rates. BMC Pregnancy and Childbirth, 20(1), 155-020-2847-9. 10.1186/s12884-020-2847-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Traylor CS, Johnson JD, Kimmel MC, & Manuck TA (2020). Effects of psychological stress on adverse pregnancy outcomes and nonpharmacologic approaches for reduction: An expert review. American Journal of Obstetrics & Gynecology MFM, 2(4), 100229. 10.1016/j.ajogmf.2020.100229 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker Taylor JL, Campbell CM, Thorpe RJ Jr, Whitfield KE, Nkimbeng M, & Szanton SL (2018). Pain, racial discrimination, and depressive symptoms among african american women. Pain Management Nursing, 19(1), 79–87. 10.1016/j.pmn.2017.11.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang H, Zhang Q, Gao T, Kong Y, Qin Z, Hu Y, Cao R, & Mei S (2019). Relations between stress and quality of life among women in late pregnancy: The parallel mediating role of depressive symptoms and sleep quality. Psychiatry Investigation, 16(5), 363–369. 10.30773/pi.2019.02.14 [DOI] [PMC free article] [PubMed] [Google Scholar]