

Abstract
This cross-sectional study examines fluoride varnish application rates during well-child medical visits and identify characteristics associated with fluoride varnish receipt.
Introduction
Fluoride varnish is effective at reducing tooth decay, which affects nearly a quarter of US children ages 2 to 5 years and more than half of children ages 6 to 8 years.1,2 To increase young children’s receipt of preventive oral health services, the US Preventive Services Task Force recommends medical providers apply fluoride varnish to young children’s teeth during well-child visits through 5 years of age.2 Offering fluoride varnish in medical settings may increase young children’s receipt of this service because 89% of children younger than 6 years of age had a preventive medical visit in 2019.3 However, fewer than 8% of young Medicaid-enrollees receive fluoride varnish in medical settings,4 and no studies have examined fluoride varnish applications during medical visits for children who are privately insured. Studying children who are privately insured is important because coverage of this service without cost-sharing has been mandated since 2015,5 and fewer than 1 in 3 children under 5 years who are privately insured have an annual dental visit.6 We used data from 4 states to examine fluoride varnish application rates during well-child medical visits and identify characteristics associated with fluoride varnish receipt.
Methods
This cross-sectional study was approved by RAND’s institutional review board, and a waiver of informed consent was granted because of the use of deidentified patient data. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
We used 2016 to 2018 data for children who are privately insured from all payer-claims databases from Maine, Connecticut, New Hampshire, and Rhode Island. We limited the analytic sample to children ages 1 to 5 years and identified well-child visits using CPT codes 99381-3 and 99391-3. Well-child visit periodicity schedules vary by age; thus, our unit of analysis was the well-child visit. We identified fluoride varnish applications (ie, CPT code 99188 and CDT code D1206) during well-child visits with the same service date.
We calculated descriptive statistics and estimated the unadjusted and adjusted odds of a visit including fluoride varnish using logistic regression; we then calculated regression-adjusted probabilities of fluoride application (eMethods in the Supplement). Tests were 2-tailed, statistical significance was set at P < .05, and we used county-level cluster robust standard errors. Data analyses were performed using SAS Version 9.4 and Stata-MP version 16.1 (StataCorp). Analysis was performed during November 2020 to March 2021.
Results
The sample included 328 661 well-child visits for children aged 1 to 5 years (169 001 [51.4%] male; 132 563 [40.3%] were 1-year-olds) Of the visits, 134 662 (41.0%) occurred in Connecticut and 15 756 (4.8%) included fluoride varnish applications (Table). Fluoride varnish was more common among visits for younger children, as illustrated by unadjusted and regression-adjusted probabilities (Figure). A 2-year-old was 7.7 percentage points (pp) (95% CI, 5.9 pp-9.4 pp) more likely to receive fluoride varnish than a 5-year-old. From 2016 to 2018, the regression-adjusted probability of fluoride varnish application increased from 3.6% (95% CI, 2.8%-4.4%) to 5.8% (95% CI, 4.5%-7.1%). Fluoride varnish applications were most common in Rhode Island, with a regression-adjusted probability of 8.7% (95% CI, 5.1%-12.4%). New Hampshire had a lower rate, with a regression-adjusted probability of 2.2% (95% CI, 1.2%-3.3%) of a visit including fluoride varnish.
Table. Characteristics of Well-Child Visits With and Without Fluoride Varnish Applications.
| Characteristic | Overall (N = 328 661) | Observation, No. (%) | Unadjusted odds of fluoride varnish application, OR (95% CI)a | |
|---|---|---|---|---|
| Visit with fluoride varnish application (N = 15 756) | Visit without fluoride varnish application (N = 312 905) | |||
| Visit included fluoride varnish application | 15 756 (4.8) | 15 756 (100) | 312 905 (0) | NA |
| Age, y | ||||
| 1 | 132 563 (40.3) | 7438 (47.2) | 125 125 (40.0) | 13.6 (8.1-22.9)b |
| 2 | 70 365 (21.4) | 5749 (36.5) | 64 616 (20.7) | 20.3 (13.8-30.0)b |
| 3 | 46 345 (14.1) | 2069 (13.1) | 44 276 (14.2) | 10.7 (7.3-15.5)b |
| 4 | 39 693 (12.1) | 327 (2.1) | 39 366 (12.6) | 1.9 (1.6-2.3)b |
| 5 | 39 695 (12.1) | 173 (1.1) | 39 522 (12.6) | [Reference] |
| Sex | ||||
| Male | 169 001 (51.4) | 8129 (51.6) | 160 872 (51.4) | [Reference] |
| Female | 159 660 (48.6) | 7627 (48.5) | 152 033 (48.6) | 1.0 (0.95-1.0) |
| Insurance type | ||||
| Preferred provider organization | 171 273 (52.1) | 8795 (55.8) | 162 478 (51.9) | 1.2 (0.9-1.7) |
| Health maintenance organization | 84 049 (25.6) | 3363 (21.3) | 80 686 (25.8) | 0.9 (0.7-1.4) |
| Point of service | 68 702 (20.9) | 3401 (21.6) | 65 301 (20.9) | 1.2 (0.9-1.6) |
| Exclusive provider organization | 4637 (1.4) | 197 (1.3) | 4440 (1.4) | [Reference] |
| Year of visit | ||||
| 2016 | 111 156 (33.8) | 4060 (25.8) | 107 096 (34.2) | [Reference] |
| 2017 | 110 892 (33.7) | 5563 (35.3) | 105 329 (33.7) | 1.4 (1.1-1.8)b |
| 2018 | 106 613 (32.4) | 6133 (38.9) | 100 480 (32.1) | 1.6 (1.3-2.1)b |
| State of residence | ||||
| Connecticut | 134 662 (41.0) | 3829 (24.3) | 130 833 (41.8) | [Reference] |
| Maine | 80 174 (24.4) | 6410 (40.7) | 73 764 (23.6) | 3.0 (1.5-6.1)b |
| New Hampshire | 64 584 (19.7) | 1401 (8.9) | 63 183 (20.2) | 0.8 (0.3-1.8) |
| Rhode Island | 49 241 (15.0) | 4116 (26.1) | 45 125 (14.4) | 3.1 (1.3-7.2)b |
Abbreviation: OR, odds ratio.
OR and 95% CIs from logistic regression models where the unit of observation was a well-child medical visit; models were estimated separately for each of the independent variables of interest and included county-level cluster robust standard errors.
Indicates difference in OR is statistically significantly different from the reference group.
Figure. Regression-Adjusted Rates of Fluoride Varnish Applications During Well-Child Medical Visits, (N = 328 661).
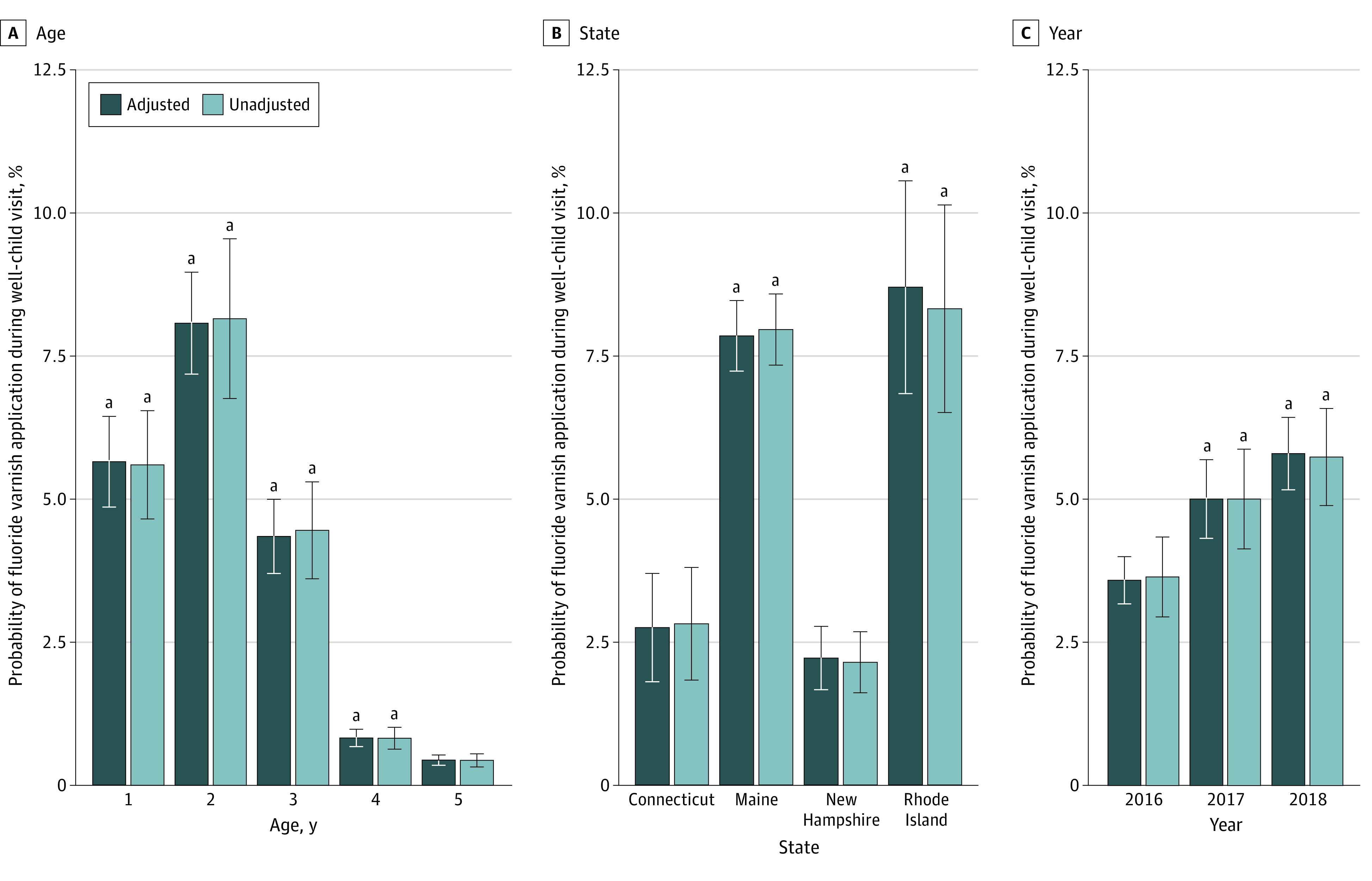
The figure presents unadjusted and regression-adjusted probabilities. Unadjusted probabilities are derived from logistic regression models predicting fluoride varnish applications during well-child medical visits. Models are estimated separately for each of the independent variables of interest (ie, age, state, and year). Regression-adjusted results are from a model controlling for child sex, age, insurance type, visit year, and state. In all models, standard errors are clustered at the county level, and the delta method was used to calculate standard errors for predicted probabilities. We calculated probabilities of fluoride varnish application during a well-child medical visit for each variable category of interest using model estimates to compute the mean of predicted probabilities for the entire sample after setting the covariate of interest (eg, Connecticut) while keeping all other covariates at their observed values.
a Indicates difference in predicted probability is statistically significantly different from the reference group (child age = 5 years, state = Connecticut, year = 2016) at the 5% level.
Discussion
Despite mandatory insurance coverage for fluoride varnish applications in medical settings, we found fewer than 5% of well-child visits for privately insured young children included this service, suggesting efforts are needed to increase pediatric medical providers’ delivery of fluoride varnish. Young children have few dental visits6 and delivering fluoride varnish in medical settings can increase access to preventive oral health services. Although this study was limited to 4 states, these data included a variety of private insurers and clinicians. Differences in fluoride varnish applications across states may be driven by variation in access to dentists and Medicaid payment policy. This study was the first to assess delivery of an evidence-based service for children who are privately insured, which is recommended by the US Preventive Service Task Force and the American Academy of Pediatrics. Although increases over time were encouraging, very low rates of fluoride varnish in medical settings suggest substantial expansion of this service in medical settings is critical for improving children’s oral health and overall well-being.
eMethods.
References
- 1.Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011-2012. NCHS Data Brief. 2015;(191):1-8. [PubMed] [Google Scholar]
- 2.Moyer VA; US Preventive Services Task Force . Prevention of dental caries in children from birth through age 5 years: US Preventive Services Task Force recommendation statement. Pediatrics. 2014;133(6):1102-1111. doi: 10.1542/peds.2014-0483 [DOI] [PubMed] [Google Scholar]
- 3.Child and Adolescent Health Measurement Initiative . 2019. National Survey of Children's Health data query. U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA), Maternal and Child Health Bureau (MCHB). Published 2021. Accessed June 14, 2021. https://www.childhealthdata.org
- 4.Geiger CK, Kranz AM, Dick AW, Duffy E, Sorbero M, Stein BD. Delivery of preventive oral health services by rurality: a cross-sectional analysis. J Rural Health. 2019;35(1):3-11. doi: 10.1111/jrh.12340 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.HealthCare.Gov . Preventive care benefits for children US Center for Medicare & Medicaid Services. Published 2021. Accessed January 21, 2021. https://www.healthcare.gov/preventive-care-children/
- 6.Medicaid and CHIP Payment and Access Commission . Medicaid Access in Brief: Children’s Dental Services. Published 2016. Accessed April 15, 2021. https://www.macpac.gov/wp-content/uploads/2016/06/Medicaid-Access-in-Brief-Childrens-Dental-Services.pdf
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods.