

Abstract
Although most cases occur in immunocompromised individuals, anal tuberculosis can occur in the absence of HIV infection. Anal tuberculosis should be considered in the differential diagnosis of chronic or recurrent anal fistulas.
Keywords: anal fistula, anal tuberculosis, perianal abscess
Although most cases occur in immunocompromised individuals, anal tuberculosis can occur in the absence of HIV infection. Anal tuberculosis should be considered in the differential diagnosis of chronic or recurrent anal fistulas.

1. CLINICAL IMAGES
A 45‐year‐old man presented with a 1‐month history of anal pain and bleeding. He was diagnosed with a perianal abscess, which did not heal after incision and drainage. Subsequently, he underwent radical surgery for an anal fistula (Figure 1). Histology revealed an epithelioid granuloma with caseous necrosis and giant cells (Figure 2). Ziehl‐Neelsen stain was performed, and the result was negative. Chest X‐ray was performed prior to the surgery, which was considered negative. However, a small nodular lesion was found in the right middle lung field by a retrospective review. Although sputum examination (smear, polymerase chain reaction, and culture) yielded negative results for tuberculosis, a gastric aspirate culture was positive for Mycobacterium tuberculosis. Taken together, he was diagnosed with extrapulmonary tuberculosis manifesting with an anal tuberculoma. Human immunodeficiency virus screening test was negative. The lesions improved with standard tuberculosis treatment.
FIGURE 1.
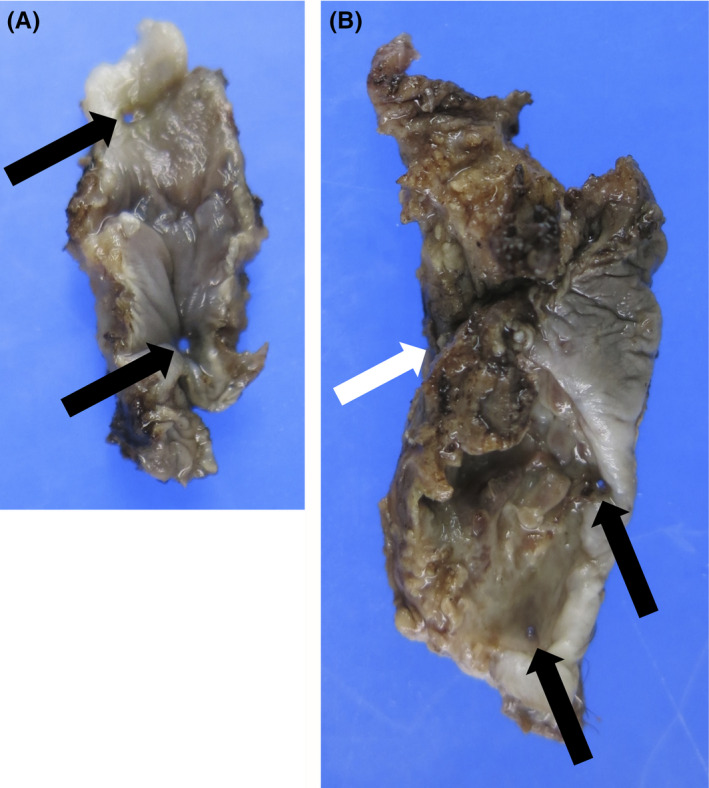
Macroscopic findings of the primary rectal fistula (A: black circle), secondary perianal fistula (B: white circle), and fistula tract (C: gray circle)
FIGURE 2.
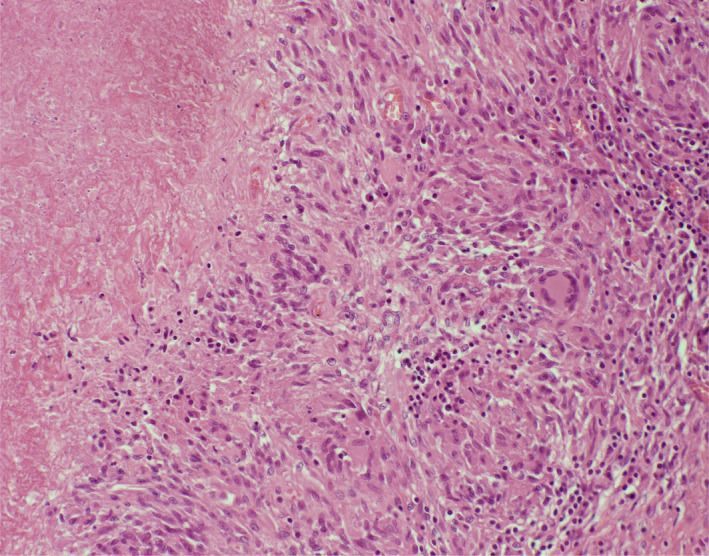
Microscopic examination of the perianal fistula showing caseous necrosis surrounded by epithelioid cells and giant cells
Anal tuberculosis is a rare type of tuberculosis, accounting for 0.7% of extrapulmonary tuberculosis.1 Although most cases occur in immunocompromised individuals, such as those with HIV infection, this case illustrates that anal tuberculosis can occur in the absence of HIV infection.2 Anal tuberculosis should be considered in the differential diagnosis of chronic or recurrent anal fistulas.
CONFLICT OF INTEREST
The authors have declared that no conflict of interest.
AUTHOR CONTRIBUTIONS
Kotaro Sasahara: involved in patient care and wrote the original draft preparation. Keiichiro Kitahama: involved in patient care and edited the draft. Satoshi Aiko: involved in patient care and edited the draft. Ho Namkoong: involved in patient care, performed investigation, and wrote the original draft preparation.
ACKNOWLEDGMENTS
Published with written consent of the patient.
Sasahara K, Kitahama K, Aiko S, Namkoong H. Anal tuberculosis presenting as refractory perianal abscess. Clin Case Rep. 2021;9:e04177. 10.1002/ccr3.4177
DATA AVAILABILITY STATEMENT
Derived data supporting the findings of this study are available from the corresponding author (HN) on request.
REFERENCES
- 1.Alvarez Conde JL, Gutiérrez Alonso VM, Del Riego TJ, García Martínez I, Arizcun Sánchez‐Morate A, Vaquero PC. Perianal ulcers of tubercular origin: A report of 3 new cases. Rev Esp Enferm Dig. 1992;81(1):46‐48. [PubMed] [Google Scholar]
- 2.Tago S, Hirai Y, Ainoda Y, Fujita T, Kikuchi K. Perianal tuberculosis: A case report and review of the literature. World J Clin Cases. 2015;3(9):848‐852. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Derived data supporting the findings of this study are available from the corresponding author (HN) on request.