

Abstract
A 24-year-old pregnant woman applied with 2 days of sudden vision loss. Funduscopy showed serous retinal detachment along in the right eye and tear was not found. In the left eye, there were two small subretinal fluid accumulationsThe patient was diagnosed with serous retinal detachment due to preeclampsia. Serous retinal detachment of the patient regressed spontaneously within 1 month. All pregnant women with gestational hypertension should undergo retinal examination.
Keywords: Gestational hypertension, preeclampsia, serous retinal detachment
INTRODUCTION
Approximately 10% of all pregnancies are complicated by hypertension.[1] Pregnancy-induced hypertension (PIH) is classified as gestational hypertension, preeclampsia, severe preeclampsia, and eclampsia. PIH is a hypertensive disorder in pregnancy which occurs after 20 gestational weeks in the absence of any other causes. (Accompanied by generalized edema or proteinuria to blood pressure greater than 140/90). When there is significant proteinuria, it is termed as preeclampsia; seizure or coma as a consequence of PIH is termed as eclampsia.[2] The visual system is affected in 30%–100% of patients with preeclampsia and serous retinal detachment occurs in <1% of them.[3] The exact pathophysiology of serous retinal detachment is not known. The most common mechanism of serous retinal detachment is vasoconstriction due to hypertension, choroid ischemia, and ischemic injury of the retinal pigment epithelium (RPE). In this way, the blood–retinal barrier break occurs.[4]
In this case report, I report a patient with spontaneous resolution of serous retinal detachment in preeclampsia.
CASE REPORT
A 24-year-old pregnant woman applied with 2 days of sudden vision loss. The patient applied to the obstetrics and gynecology clinic with blurred vision and headache 1 day ago. On physical examination, her systemic BP was 170/110 mmHg. She was at 35 weeks of gestation and there was no systemic BP elevation before. Her heart rate was 93/min; respiratory and cardiovascular systems were normal. There was (+++) proteinuria with the dipstick. Liver function, renal function and coagulation tests, thrombocytes, and hemoglobin were normal. She was diagnosed as preeclampsia and emergency cesarean section was performed. The patient delivered a 2419 g male healthy fetus.
In ophthalmologic evaluation, her right vision was 1 m counting finger and the left vision was 0.7 decimal. Biomicroscopic anterior segment examination was normal in both eyes. Intraocular pressure was 13 mmHg in the right eye and 14 mmHg in the left eye. Funduscopy showed serous retinal detachment along in the right eye and tear was not found. In the left eye, there were two small subretinal fluid accumulations [Figure 1a and b]. Optical coherence tomography (OCT) revealed neurosensory detachment from underlying RPE in the right eye and subretinal thickness was 1380 μm [Figure 1c and d].
Figure 1.
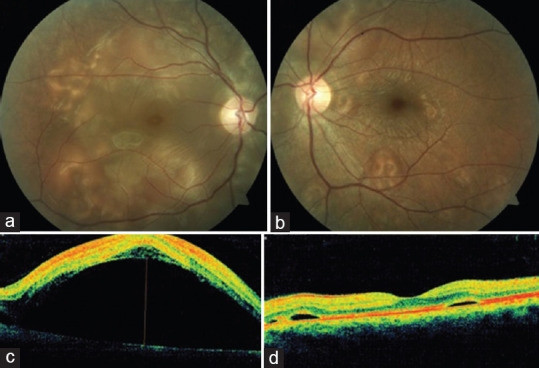
(a-d) Fundus and optical coherence tomography images of the patient at the first visit
On the 2nd postpartum day, her systemic BP was 110/70 mmHg and laboratory parameters were normal. At 1st month postdelivery, her visual acuities improved to 0.7 on the right eye and 1.0 on the left eye. Fundoscopy and OCT were normal except a small subretinal fluid in the right eye. The right eye subretinal thickness was 30 μm [Figure 2a-d]. In the 2nd month, the right eye vision was 1.0 decimal and subretinal fluid showed total resolution [Figure 3a-d].
Figure 2.
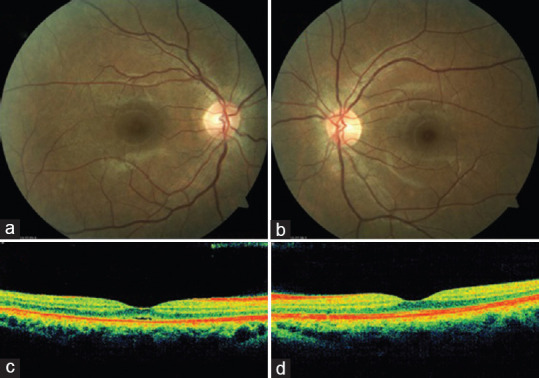
(a-d) Fundus and optical coherence tomography images of the patient at 1st month
Figure 3.
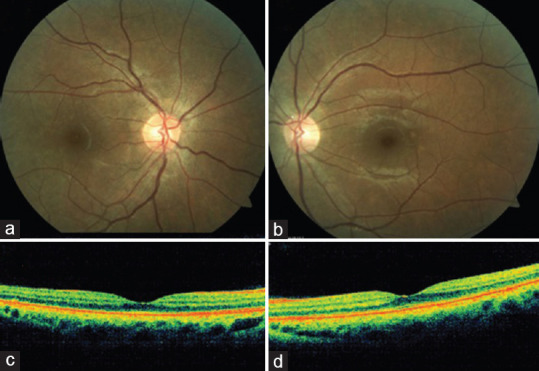
(a-d) Fundus and optical coherence tomography images of the patient at 2nd month
DISCUSSION
The most frequent ocular finding of preeclampsia is diffuse arteriolar spasm on the retina. Serous retinal detachment is a rare complication and is usually seen in cases with severe hypertensive patients. Most of the cases occur bilaterally during the third trimester but may also develop postnatally.[5]
The serous retinal detachment involves the separation of the neurosensory retina from the retina pigment epithelium and there is no tear. The systemic reasons of serous retinal detachment are very broad. Some reasons are collagen vascular diseases, disorders associated with disseminated intravascular coagulopathy, malignant hypertension, hypercortisolism, renal disease, and very rarely malignant diseases.[6]
The management of the serous retinal detachment is the treatment of underlying reason. The breakdown of the blood-retinal barrier (RPE) and failure of the RPE pump function recoveries spontaneously at the postpartum period.[7] In most of the patients, serous retinal detachment shows complete recovery within 2–12 weeks after delivery.[8] Our patient recovered spontaneously in 2 months.
Surgical intervention is usually not necessary and the improvement occurs with clinical control of BP.[9] In our case, the BP spontaneously decreased after birth. In the previous case reports, serous retinal detachment often involves at posterior pole like our case.[10,11]
In the case of Sathish, et al.,[12] a 26-year-old multigravida with preeclampsia developed bilateral choroid ischemia with serious retinal detachments. There was a spontaneous resolution of the serous detachment and the choroid changes in the postpartum period with residual pigment epithelium changes. The fluorescein angiographic studies are usually not performed in pregnancy due to teratogenic effects on the fetus. We also did not do fluorescein angiography.
The OCT is a safe and noninvasive imaging method in this period. The most common OCT finding is the elevation of the inner and outer retinal layers associated with severe neurosensorial retinal detachment as well as intraretinal cysts.[13] In our case, there was severe neurosensorial retinal detachment in the right eye but there were no intraretinal cysts.
All pregnant women with gestational hypertension should undergo retinal examination. Most patients with serous retinal detachment recover spontaneously without sequela within a few weeks.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient (s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initial s will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Hiller KM, Honigman B. Cortical blindness in preeclampsia. Am J Emerg Med. 2004;22:631–2. doi: 10.1016/j.ajem.2004.09.012. [DOI] [PubMed] [Google Scholar]
- 2.Davey DA, MacGillivray I. The classification and definition of the hypertensive disorders of pregnancy. Am J Obstet Gynecol. 1988;158:892–8. doi: 10.1016/0002-9378(88)90090-7. [DOI] [PubMed] [Google Scholar]
- 3.Lee C, Hsu TY, Ou CY, Chang SY, Soong YK. Retinal detachment in postpartum preeclampsia and eclampsia: Report of two cases. Changgeng Yi Xue Za Zhi. 1999;22:520–4. [PubMed] [Google Scholar]
- 4.Lara-Torre E, Lee MS, Wolf MA, Shah DM. Bilateral retinal occlusion progressing to long-lasting blindness in severe preeclampsia. Obstet Gynecol. 2002;100:940–2. [PubMed] [Google Scholar]
- 5.Hutchings K, Sangalli M, Halliwell T, Tuohy J. Bilateral retinal detachment in pregnancy. Aust NZ J Obstet Gynaecol. 2002;42:409–11. doi: 10.1111/j.0004-8666.2002.409_3.x. [DOI] [PubMed] [Google Scholar]
- 6.Wolfensberger TJ, Tufail A. Systemic disorders associated with detachment of the neurosensory retina and retinal pigment epithelium. Curr Opin Ophthalmol. 2000;11:455–61. doi: 10.1097/00055735-200012000-00012. [DOI] [PubMed] [Google Scholar]
- 7.Celik O, Hascalık Ş, Gokdeniz R. Bilateral serous retinal detachment in preeclampsia: Report of two cases. Gynecol Obstet Reprod Med. 2002;8:61–1. [Google Scholar]
- 8.Atış A, Ciftci F, Tutuman T, Turker C, Goker N, Balcıoğlu N. Ağır preeklampside nadir gorulen bir bilateral seroz retina dekolmanı. Şşli Etfal Tıp Bulteni. 2009;43:51–2. [Google Scholar]
- 9.Mihu D, Mihu CM, Tălu S, Costin N, Ciuchină S, Măluţan A, et al. Ocular changes in preeclampsia. Oftalmologia. 2008;52:16–22. [PubMed] [Google Scholar]
- 10.Somfai GM, Miháltz K, Tulassay E, Rigó J., Jr Diagnosis of serous neuroretinal detachments of the macula in severe preeclamptic patients with optical coherence tomography. Hypertens Pregnancy. 2006;25:11–20. doi: 10.1080/10641950500543848. [DOI] [PubMed] [Google Scholar]
- 11.Sheth BP, Mieler WF. Ocular complications of pregnancy. Curr Opin Ophthalmol. 2001;12:455–11. doi: 10.1097/00055735-200112000-00011. [DOI] [PubMed] [Google Scholar]
- 12.Sathish S, Arnold JJ. Bilateral choroidal ischaemia and serous retinal detachment in pre-eclampsia. Clin Exp Ophthalmol. 2000;28:387–90. doi: 10.1046/j.1442-9071.2000.00342.x. [DOI] [PubMed] [Google Scholar]
- 13.Çelik G, Eser A, Günay M, Yenerel N. Bilateral vision loss after delivery in two cases: Severe preeclempsia and hellp syndrome. Turk J Ophthalmol. 2015;45:271–2. doi: 10.4274/tjo.45722. [DOI] [PMC free article] [PubMed] [Google Scholar]