

Abstract
Critical care echocardiography (CCE) is commonly performed in many intensive care units across Australia and New Zealand (ANZ). The scope of practice ranges from Basic CCE through to Advanced CCE and includes the use of transthoracic echocardiography and transoesophageal echocardiography. Many training and qualification pathways exist with no standardisation of education goals. This document defines different levels of CCE expertise and recommends minimum training standards for each level of adult CCE in ANZ. Guidelines committee of College of Intensive Care Medicine's Ultrasound Special Interest Group held multiple face to face meetings, organised teleconferences, conducted a survey of the Fellows of the college and reviewed the international CCE training pathways prior to writing these guidelines.
Keywords: Australia, clinical competence, critical care, echocardiography, intensive care unit, New Zealand, standards
Introduction
Critical care echocardiography (CCE) is widely performed in many intensive care units across Australia and New Zealand (ANZ).1, 2 Recognising the importance of CCE, the College of Intensive Care Medicine (CICM) has established the Ultrasound Special Interest Group (USIG) and included Basic CCE (Focused Cardiac Ultrasound) as a mandatory component of training in its updated 2014 curriculum.3
Expertise and practice in CCE vary widely and includes the use of transthoracic echocardiography (TTE) and/or transoesophageal echocardiography (TOE).4, 5 The scope of practice ranges from Basic CCE, which is used to rapidly characterise causes of shock and respiratory failure, through to Advanced CCE, which entails the performance of comprehensive diagnostic studies similar to that expected of a cardiologist, often with additional advanced haemodynamic assessment using echocardiographic criteria. There are many training and qualification pathways for different levels of expertise, including accredited workshops, short commercial courses, conferences, University courses and Diplomas and CCE Fellowship Programs, with no standardisation of education goals.
In response to these concerns, the USIG conducted a survey on ultrasound utilisation and training amongst the Fellows of CICM. It held face to face consultations and teleconferences with the members and reviewed literature pertinent to this issue. Also, overseas experience in formulating CCE competency levels and their specific training pathways were reviewed and carefully considered. The USIG also reviewed the echocardiography training guidelines from the Australian and New Zealand College of Anaesthetists (ANZCA), the Australasian College for Emergency Medicine (ACEM), the Royal Australasian College of Physicians (RACP) and the Cardiac Society of ANZ (CSANZ). There was no consultation with these craft groups while developing these guidelines.
The document aims to formally define different levels of CCE expertise and to recommend minimum training standards for each level of adult CCE in ANZ. The USIG does not have the mandate or the terms of reference which would position it as a certification authority. Therefore, this document is not prescriptive, but instead is intended to serve as a guide for Fellows, trainees and relevant bodies tasked with training, certification and accreditation in CCE. Parts of this document, but not its entirety, have been endorsed by the Australasian CICM.
Justification for guidelines
Patient safety dictates that standards are required for all areas of medical practice, with a community expectation that these should be defined and documented.
Practice of intensive care medicine
College of Intensive Care Medicine promulgates advice on training and clinical aspects of the practice of intensive care medicine. Echocardiography now forms part of the scope of practice of Intensivists and Core training for CICM includes Basic CCE (Focused Cardiac Ultrasound).3 However, the actual practice of CCE ranges from Basic to expert standard CCE. For that reason, this paper contains recommendations for all recognised levels of CCE practice.
Patient benefit
The use of CCE by Intensivists provides benefits for patients through assessment of haemodynamic state and cardiac pathology.6 While traditional clinical examination and monitoring continue to be the mainstay, there is increasing recognition that more advanced techniques like CCE can help resolve diagnostic or management dilemmas, often in a time critical manner.
Patient risk
Development of appropriate standards for the practice of CCE minimises the risks to patients from incorrectly performed or interpreted studies. Misinterpretation and incorrect reporting of echocardiography studies can result in incorrect treatment decisions and patient harm. Also, the performance of TOE carries procedural risks to the patient that include but are not confined to damage to the teeth, pharynx, oesophagus and stomach including erosions, bleeding, rupture or burns.7 For these reasons, it is important that those practising CCE are appropriately trained and skilled.
Standards for CCE
ANZCA and ACEM have produced standards and recommendations for their Fellows undertaking cardiac and other ultrasound studies.8, 9 ANZCA recognises two levels of expertise of echocardiography: goal‐directed and Comprehensive. Comprehensive echocardiography studies include the use of either TTE or TOE. RACP and CSANZ have produced standards for the practice of cardiac ultrasound for cardiology trainees and Fellows.10, 11 These standards/recommendations have been developed specifically for the echocardiography practice within each relevant specialty.
There are many international organisations which have produced recommendations, accreditation statements and guidelines for levels of practice and training in CCE.12, 13, 14, 15, 16, 17, 18, 19, 21 Achieving consistency with national and international intensive care organisations and related medical bodies was one of the aims of this document. However, it was deemed important that specific guidelines should be developed for Fellows and Trainees of the CICM that best reflect the scope and diversity of practice of intensive care medicine and CCE within the ANZ context.
Issues considered
Critical care echocardiography is generally performed by the physician responsible, at least in part, for the patient's management. Interpretation frequently occurs in real time, sometimes resulting in immediate changes in patient management, and repeated studies may be required to assess patient response. It is often performed in challenging environments not favourable for image optimisation. Patients are frequently poorly positioned and unable to co‐operate with the examination. There is often complex pathophysiology of organs and body systems, significant intercompartmental fluids shifts, altered intrathoracic and intra‐abdominal pressures, multiple pharmacological and mechanical interventions, all of which require consideration for accurate examination interpretation. Clinicians embarking on CCE must have not only great skills in echocardiography but also an in‐depth understanding of critical care medicine and knowledge of individual patient. In acknowledgment of these differences and to better reflect the varying levels or scope of CCE, the choice of terminology has been carefully considered.
Basic CCE
Basic CCE is usually confined to two‐dimensional and M‐mode TTE modalities. It is used to define type of shock or diagnose major haemodynamic abnormalities. It is a rapid bedside technique which requires a limited understanding of ultrasonography, cardiac anatomy, pathophysiology of circulation and basic critical care medicine.
Advanced CCE
These are the examinations performed with a level of expertise similar to what would be expected if a patient was referred to a cardiologist for a TTE or TOE, often with additional advanced assessment of haemodynamic state using echocardiographic criteria. It utilises multiple windows, views and modern echocardiographic modalities (that include but is not limited to a two‐dimensional and M‐mode imaging, Colour and spectral Doppler, tissue Doppler and speckle tracking‐based tissue deformation modalities, three‐dimensional and contrast studies as required in specific cases). Interpretation of results is profoundly influenced by real‐time physiological and pharmacological factors affecting the patient. Incorporation of these factors into reports is a unique and fundamental skill set of the advanced practice of CCE.
TTE and TOE
TTE and TOE techniques of echocardiography share a common basis in ultrasound image formation and cardiac pathologies examined. There are, however, essential differences in probe position, image acquisition and interpretation that necessitate differences in required training. Within ANZ, TTE is by far the most common modality employed reflecting the view amongst practitioners that TTE is of sufficient image quality and clinical value for most ICU patients. There are however significant patient groups and pathologies (e.g. post cardiac surgery, suspected thoracic aortic pathology, assessment of atrial masses and endocarditis) where TTE imaging is suboptimal, inadequate and where the TOE is an essential modality. ICU case mix, resources and local expertise often influence the predominant technique used in that unit. Many Advanced CCE practitioners work in ICUs in which the need and/or exposure to TOE is minimal. It is recommended that the Advanced level of CEE be divided between those who practise TTE only, and those who also use TOE, to best reflect practice and training needs within the ANZ critical care environment.
Expert CCE
To maintain and promulgate excellence in all levels of expertise and training it is recommended that an Expert level in CCE be recognised.22, 23 This is a peer‐endorsed recognition of Intensive Care Specialists who practise at the Advanced level of TTE and TOE in intensive care medicine for at least 7 years and are substantially involved in CCE education and training.
Training
Minimum standards for training include both knowledge and practical skills acquisition. Allowance has been made for the varied methods by which Fellows and trainees achieve these. As noted above, the minimum standards produced by international intensive care organisations, along with the advice of the group of experts were used to develop these recommendations.
Recommendations
Three main levels of training are recommended (Figure 1).
Figure 1.
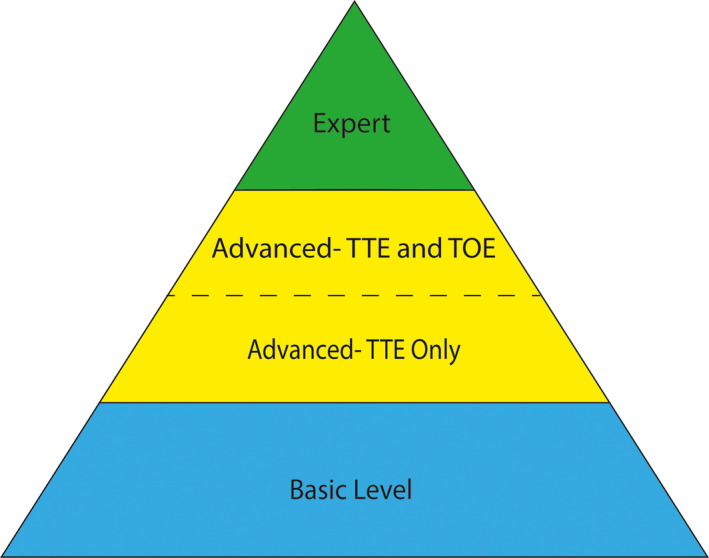
Levels of Training in Adult Critical Care Echocardiography in Australia and New Zealand. TTE, Transthoracic Echocardiography; TOE, Transoesophageal Echocardiography.
The main requirements for accreditation are enumerated in Table 1. These levels also define the milestones for a trainee or a Fellow to follow while pursuing training in CCE.
Table 1.
Training requirements for levels of training in Critical Care Echocardiography in Australia and New Zealand
| Levels of training | Minimum requirements |
|---|---|
| 1. Basic | Attendance in accredited course |
| Logbook of 30 studies performed and reported | |
|
Signed off as pass by CICM‐accredited supervisor All studies must be performed in intensive care environment Ongoing professional development in echocardiography | |
| 2a. Advanced TTE only | Evidence of completion of accredited course with exit examination |
| Logbook of 450 studies | |
| 300 studies performed and reported | |
| 150 studies reported | |
|
At least two‐thirds of all studies should be performed in critical care environment. Ongoing professional development in echocardiography | |
| 2b. Advanced TTE and TOE | Evidence of completion of accredited course with exit examination |
| TTE logbook requirements same as advanced TTE level | |
| Logbook of 50 TOE studies | |
| 25 performed and reported | |
| 25 assisted/observed and reported | |
|
At least a half of all studies should be performed in intensive care environment. Ongoing professional development in echocardiography | |
| 3. Expert level |
Advanced TTE and TOE requirements as in 2b More than 7 years practising at Advanced TTE and TOE level |
| Substantive involvement in education and training | |
|
Echocardiography research profile and publications (desirable) Ongoing professional development in echocardiography |
CICM, College of Intensive Care Medicine; TTE, Transthoracic echocardiography; TOE, Transoesophageal echocardiography.
Basic critical care echocardiography
Basic CCE is designed to functionally identify types of shock, monitor significant physiological abnormalities and guide individual therapy. To perform this, the practitioner should be competent in obtaining basic TTE views, identifying normal versus grossly abnormal anatomical structures and identifying significant functional abnormalities. It is limited to the use of 2D and M‐mode modalities with a clear understanding of the associated limitations of these techniques by the user. Basic CCE studies do not include Doppler techniques or other complex ultrasound modalities as they require an in‐depth understanding of ultrasound physics and training for correct application and interpretation at bedside.
Completion of the basic level of training in adult CCE now constitutes part of the CICM training curriculum. To achieve this level of training, intensive care practitioners should complete a basic echocardiography course that is accredited by CICM, submit a logbook under the supervision of CICM‐accredited supervisors and be signed as a ‘pass’ as well as complete a short online examination.
It is currently accepted that CICM‐accredited supervisors have various backgrounds, including highly experienced ICU sonographers, cardiologists with sufficient ICU experience and ICU specialists with advanced or Expert levels of training in Adult CCE. This approach to the selection of supervisors is temporary and reflects current limitations of widespread availability of supervising CICM Fellows with Advanced CCE training. Over time, it is likely that as the pool of suitably qualified CCE Fellows grows, it will reduce the current reliance on other craft groups in the supervision of Basic CCE training. Also, the introduction of simulation‐based curriculums which can accelerate the learning of Basic CCE may improve training in the future.24
It is important to recognise that Basic CCE includes not only the ability to obtain good echocardiography views (hand skills), but also identification of significant abnormalities (echocardiography knowledge) and integration of echocardiography findings with clinical, laboratory and other imaging results (ICU knowledge and experience). Basic CICM trainees may lack sufficient critical care knowledge and experience to make unsupervised decisions based on echocardiography findings which must always be considered in the context of critically ill patients. More advanced trainees will require varying levels of supervision. Trainees at all stages of intensive care training are encouraged to train in image acquisition and to participate in echocardiography discussion.
Basic echocardiography can be a powerful ICU bedside clinical tool, but its misuse can cause iatrogenic morbidity and mortality. Therefore, trainees undertaking the basic CCE module should refrain from its use for clinical purposes until the review of each echocardiographic study by a CICM supervisor has occurred and/or a formal study completed. This is not dissimilar to any other ICU imaging, but is especially true when significant clinical decisions are made based on echocardiography findings alone. Those advanced ICU trainees who completed their training should be able to perform basic CCE within individually allocated levels of supervision, based on local arrangements and assessment of individual competency. It is recommended that most studies performed by trainees for clinical purposes should be reviewed as part of quality assurance by ICU specialists with Advanced or Expert level of training. All significant findings of anatomical or functional pathology should be further investigated with a formal complete echocardiographic study performed by practitioners with advanced training and expertise.
All studies used for diagnostic or decision‐making purposes must be recorded on a digital media platform in a manner compliant with relevant health record legislation and made readily available for future review and comparison.
Training logbooks should include echocardiography findings and, importantly, clinical interpretation of the study in the context of individual patient and other investigations. It should include clinical conclusions and proposed recommendations. This is the most critical component which should be considered by the supervisor when determining if the particular case qualifies as a ‘Pass’.
Those intensive care practitioners, who are endorsed to perform Basic CCE, must continue practising clinical echocardiography in ICU and participating in continuing medical education to maintain their endorsement.
Advanced critical care echocardiography
This is divided into two subclasses.
Advanced critical care echocardiography in transthoracic echocardiography
Intensive Care Specialists practising TTE at an advanced level should be fully proficient in independent performance and interpretation of TTE in adult intensive care patients with a wide variety of medical and surgical pathologies, including complex haemodynamic abnormalities, variable pharmacological and mechanical cardiorespiratory support, structural and functional cardiac pathology. They should be able to perform echocardiography without supervision and within an appropriate time frame, but with explicit knowledge of personal limitations and insight into when to seek help from the Expert level practitioners in echocardiography. Training to the Advanced level CCE greatly exceeds Basic level of proficiency and takes at least 12–24 months. Advanced level CCE training should be overseen by an Expert level CCE practitioner.
There are three major components which must be satisfied in order to be endorsed for the Advanced level of training: a theoretical component, a practical component supported by a logbook and an exit examination.
Successful completion of the exit theory examination, administered by a nationally or internationally recognised body is required to complete the theoretical component of the Advanced level TTE. The theoretical component of the CICM‐accredited course syllabus should cover ultrasound physics, knobology, artefacts formation and image optimisation. It should also include in‐depth specifics of clinical adult echocardiography (including valvular and quantitative haemodynamic assessment) with emphasis on various shock states, heart–lung interactions, volume state assessment and complex pharmacological and mechanical cardiorespiratory support.
Competency in Advanced level CCE requires an in‐depth understanding of modern intensive care medicine as well as excellent knowledge and experience in modern echocardiography. In effect, it constitutes a subspecialty of intensive care and thus is being reserved for fully qualified Intensive Care Specialists (CICM Fellows or an equivalent).
Competency in Advanced level CCE includes full proficiency in the utilisation of M‐mode, 2D, Colour and spectral Doppler as well as tissue Doppler techniques. Knowledge of current recommendations for chamber quantification, for assessment of native and prosthetic cardiac valves and appropriate use of TTE is an important component of this level of training. Basic knowledge and understanding of principles applicable for 3D echocardiography, advanced tissue deformation and left chamber opacification with ultrasound contrast are recommended, but practical experience in these techniques is not required at this stage.
The minimum requirements for the practical component are based on the benchmark standards outlined within the Diploma of Diagnostic Ultrasound (DDU) critical care syllabus for TTE (Australasian Society of Ultrasound Medicine) and consist of 150 transthoracic examinations (reported) and 300 transthoracic examinations (performed and reported).25 Echocardiographic examinations should be performed in a wide variety of settings with at least two‐thirds of the studies done in an intensive care setting.
Advanced critical care echocardiography in transthoracic and transoesophageal echocardiography
Several pathways leading to the recognition of proficiency in TOE are available in different parts of the world. These pathways reflect local specifics of training and practice, as well as historical developments. Currently, UK, USA and Canada have separate certification systems in TTE and TOE for those who want to gain advanced level training in echocardiography.26, 27, 28, 29 (A point to note, in the USA, National Board of Examination is holding the inaugural examination of Special Competence in Critical Care examination in January 2019, and the certification is still in development). Mainland European recommendations have brought TTE and TOE together to be endorsed as a practitioner with Advanced CCE standing.13, 14 Australian and New Zealand CCE practitioners predominantly use TTE. This is due to significant improvements in quality and availability of echocardiography equipment, non‐invasiveness and convenience of ready TTE availability for bedside ICU use and broader available training. TOE is a semi‐invasive procedure associated with rare, but potentially substantial complications.6 Although it holds a very important place in ANZ intensive care, its use remains reserved for special indications. As a result, TOE studies are performed increasingly infrequently, even in the tertiary ICUs with cardiac surgery programs, leading to the dwindling practical opportunities for initial TOE training in critical care environment as well as for skills maintenance among those practitioners proficient in TOE.
Extensive consultations have been undertaken by USIG regarding the preferred pathway for ANZ intensivists. This was followed by the Echocardiography Training and Practice Survey conducted by USIG among CICM Fellows. Approximately half of the Fellows responded in support of separating TOE pathway, as an extra skill for advanced TTE.
The existing DDU (Critical Care) standard in Australasia specifies minimum requirements for practical TOE training, which include 25 transoesophageal examinations performed and reported and 25 transoesophageal examinations (observed/assisted and reported).25 The examinations should be performed in a wide variety of clinical settings, including cardiology and intraoperative settings, with at least half of the studies performed in the ICU, with suitable supervision. These requirements are in addition to the minimum standards for Advanced TTE training described in the previous section.
TOE education is available to the Intensive Care Specialist by completing qualifications such as DDU (Critical Care) or the equivalent which has both TTE and TOE included within theoretical, practical and examination components of training. Acquisition of appropriate advanced practical and theoretical skills can be assisted via enrolment in the dedicated CCE Fellowship Programs.
Expert level in adult critical care echocardiography
The Expert level in Adult CCE is a peer‐endorsed recognition of Intensive Care Specialists with advanced qualifications in CCE who practise at the Advanced level of TTE and TOE in intensive care medicine for at least 7 years and are substantially involved in CCE education and training. Involvement in echocardiography research and publications are not obligatory, but desirable.
Table 2 compares the current recommendations with the representative international guidelines/certification systems.
Table 2.
Comparison of the current recommendations with international guidelines/certifications
| Levels of training | International Guidelines/Certification systems | |||
|---|---|---|---|---|
| United Kingdom | International Expert Statement on Training Standards for Critical Care Sonography15 | American College of Chest Physicians/La Société de Réanimation de Langue Française statement on competence in critical care ultrasonography18 | CICM Ultrasound SIG's levels of training in Critical Care Echocardiography in Adults | |
| Basic |
Focused intensive care echocardiography12 50 focused TTE scans |
Basic critical care echocardiography 30 Scans. Recommended to be a part of training of critical care physicians |
Goal‐directed echocardiography Includes TTE and TOE Does not specify minimum number of studies required |
Part of core curriculum for ICU training called Focused cardiac ultrasound. Specifies the requirements |
| Advanced | Separate levels for advanced TTE and TOE. Certification by British Society of Echocardiography26, 27 | Requires both TTE and TOE. Does not have separate advanced levels for TTE and TOE. Minimum studies required to achieve competence are 100 TTE and 35 TOE. |
Includes TTE and TOE. Does not separate advanced levels for TTE and TOE. Does not specify minimum required studies to achieve competence |
Advanced level is further divided into (i) TTE only (ii) TTE and TOE Specifies the requirements and minimum studies required to achieve competence |
| Expert | No separate Expert level |
Expert level is mentioned. No guidelines to enumerate requirements |
Does not mention separate Expert Level | Has separate Expert level and enumerates the requirements |
Equipment
Adequate training in all levels of CCE is not possible without appropriate echocardiographic equipment, which should reflect specific local levels of CCE practice and training requirements. Equipment recommendations for CCE have been developed by the relevant USIG subcommittee.30
Continuing medical education and quality assurance
Ongoing participation in professional development activities associated explicitly with CCE is mandatory for all levels of training. Detailed recommendations for continuing medical education/quality assurance requirements in CCE are being developed by USIG.
Conclusions
These recommendations have been developed by a CCE expert group to standardise levels of training in CCE in ANZ. They intend to ensure competency of intensive care practitioners in echocardiographic image acquisition, recognition of pathology and incorporation of echocardiographic results in holistic critical care practice. Introduction of standards intends to improve patient safety and excellence in the quality of delivered medical care. These recommendations are in line with nationally accepted intercraft standards for echocardiography training and could be used as a guide for trainees and trainers in the process of training and practice. These recommendations could also be used as a guide in institutional accreditation for CCE.
Disclosure statement
Authors have no conflict of interest to declare.
Authorship declaration
All authors acknowledge that the authorship listing conforms to the journal's authorship policy. All authors are in agreement with the content of the submitted manuscript.
References
- 1.McLean A, Yastrebov K. Echocardiography training for the intensivist. Crit Care Resusc 2007; 9: 320–2. [PubMed] [Google Scholar]
- 2.Yang Y, Royse C, Royse A, Williams K, Canty D. Survey of the training and use of echocardiography and lung ultrasound in Australasian intensive care units. Crit Care 2016; 20: 339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.College of Intensive Care Medicine of Australia and New Zealand . CICM Focused Cardiac Ultrasound – (T‐35) V6 May 2015 [Internet]. College of Intensive Care Medicine of Australia and New Zealand; 2015. Available from: https://www.cicm.org.au/CICM_Media/CICMSite/CICM-Website/Resources/Trainee%20Resources/T-35-(2014)-Focused-Cardiac-Ultrasound-in-Intensive-Care-Syllabus.pdf [cited 2018 Jun 29].
- 4.Levitov A, Frankel HL, Blaivas M, Kirkpatrick AW, Su E, Evans D, et al. Guidelines for the appropriate use of bedside general and cardiac ultrasonography in the evaluation of critically ill patients‐part II: cardiac ultrasonography. Crit Care Med 2016; 44: 1206–27. [DOI] [PubMed] [Google Scholar]
- 5.Narasimhan M, Koenig S, Mayo P. Advanced echocardiography for the critical care physician. Chest 2014; 145: 129–34. [DOI] [PubMed] [Google Scholar]
- 6.Vignon P. What is new in critical care echocardiography? Crit Care 2018; 22: 40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hilberath JN, Oakes DA, Shernan SK, Bulwer BE, D'Ambra MN, Eltzschig HK. Safety of transesophageal echocardiography. J Am Soc Echocardiogr 2010; 23: 1115–27. [DOI] [PubMed] [Google Scholar]
- 8.Australian and New Zealand College of Anaesthetists . PS46 BP Guidelines on training and practice of perioperative cardiac ultrasound in adults [Internet]. Australian and New Zealand College of Anaesthetists; 2014. Available from: http://www.anzca.edu.au/documents/ps46bp-2014-guidelines-on-training-and-practice-of.pdf [cited 2018 Jun 29]
- 9.Australasian College for Emergency Medicine . P61 version 3. Policy on credentialing for focussed echocardiography in life support [Internet]. Australasian College for Emergency Medicine; 2016. Available from: https://acem.org.au/getmedia/8092e5a4-addf-475d-a16c-1adbbf81a846/Feb_16_P61_Policy_Credentialing_ECG_Life_Support.aspx [cited 2018 Jun 29]
- 10.Adult Medicine Division . Advanced training in cardiology 2017‐18 Program requirements handbook [Internet]. Royal Australasian College of Physicians; 2018. Available from: https://www.racp.edu.au/docs/default-source/default-document-library/at-cardiology-handbook-2017-18.pdf?sfvrsn=12 [cited 2018 Jun 30]
- 11.Cardiac Society of Australia and New Zealand . Position statement for training and performance of adult echocardiography [Internet]. Cardiac Society of Australia and New Zealand; 2015. Available from: http://www.csanz.edu.au/wp-content/uploads/2015/04/Adult-Echo_2015-February.pdf [cited 2018 Jun 30].
- 12.British Society of Echocardiography . Accreditation in critical care echocardiography. Information pack [Internet]. British Society of Echocardiography; 2017. Available from: https://www.bsecho.org/media/191840/acce_accreditation_pack_2016_final.pdf [cited 2018 Jun 30]
- 13.European Society of Intensive Care Medicine . European diploma in advanced critical care echocardiography [Internet]. European Society of Intensive Care Medicine; 2017. Available from: https://www.esicm.org/education/edec-2/ [cited 2018 Jun 30]
- 14.Expert Round Table on Echocardiography in ICU . International consensus statement on training standards for advanced critical care echocardiography. Intensive Care Med 2014; 40: 654–66. [DOI] [PubMed] [Google Scholar]
- 15.Expert Round Table on Ultrasound in ICU . International expert statement on training standards for critical care ultrasonography. Intensive Care Med 2011; 37: 1077–83. [DOI] [PubMed] [Google Scholar]
- 16.Price S, Via G, Sloth E, Guarracino F, Breitkreutz R, Catena E, et al. Echocardiography practice, training and accreditation in the intensive care: document for the World Interactive Network Focused on Critical Ultrasound (WINFOCUS). Cardiovasc Ultrasound 2008; 6: 49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Arntfield RT, Millington SJ, Ainsworth CD, Arora RC, Boyd J, Finlayson G, et al. Canadian recommendations for critical care ultrasound training and competency for the Canadian Critical Care Society. Can Respir J 2014; 21: 341–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mayo PH, Beaulieu Y, Doelken P, Feller‐Kopman D, Harrod C, Kaplan A, et al. American College of Chest Physicians/La Société de Réanimation de Langue Française statement on competence in critical care ultrasonography. Chest 2009; 135: 1050–60. [DOI] [PubMed] [Google Scholar]
- 19.Díaz‐Gómez J, Frankel H, Hernandez A. National certification in critical care echocardiography: its time has come. Crit Care Med 2017; 45: 1801–4. [DOI] [PubMed] [Google Scholar]
- 20.Mayo P, Narasimhan M, Koenig S. Advanced critical care echocardiography: the intensivist as the ACCE of hearts. Chest 2017; 152: 4–5. [DOI] [PubMed] [Google Scholar]
- 21.Oren‐Grinberg A, Talmor D, Brown S. Focused critical care echocardiography. Crit Care Med 2013; 41: 2618–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Vignon P, Cholley BP, De Backer D, Slama M, Vieillard‐Baron A. Learning and competence in critical care echocardiography. In: de Backer D, Cholley B, Slama M, Vieillard‐Baron A, Vignon P, editors. Hemodynamic monitoring using echocardiography in the critically ill. Berlin: Springer; 2011. 275–81. [Google Scholar]
- 23.Cholley B, Vieillard‐Baron A, Mebazaa A. Echocardiography in the ICU: time for widespread use!. Intensive Care Med 2005; 32: 9–10. [DOI] [PubMed] [Google Scholar]
- 24.Vignon P, Pegot B, Dalmay F, Jean‐Michel V, Bocher S, L'her E, et al. Acceleration of the learning curve for mastering basic critical care echocardiography using computerized simulation. Intensive Care Med 2018; 44: 1097–105. [DOI] [PubMed] [Google Scholar]
- 25.Australasian Society for Ultrasound in Medicine . Diploma of diagnostic ultrasound syllabus critical care [Internet]. Australasian Society for Ultrasound in Medicine; 2017. Available from: http://www2.asum.com.au/wp-content/uploads/2015/09/DDU-Critical-Care-Syllabus-06-08-2012.pdf [cited 2018 Jun 30]
- 26.British Society of Echocardiography . Accreditation in adult transoesophageal echocardiography information pack [Internet]. British Society of Echocardiography; 2018. Available from: https://www.bsecho.org/media/191834/toe_accreditation_pack_2018v.1.pdf [cited 2018 Jun 30]
- 27.British Society of Echocardiography . Accreditation in adult transthoracic echocardiography information pack [Internet]. British Society of Echocardiography; 2018. Available from: https://www.bsecho.org/media/226439/tte_accreditation_pack_2018_v.3.pdf [cited 2018 Nov 25]
- 28.National Board of Echocardiogrpahy, Inc . Handbooks for NBE certification programs. Raleigh, NC: National Board of Echocardiography, Inc; 2018. Available from: http://echoboards.org/EchoBoards/Certification/Handbooks_for_All_Certification_Programs/EchoBoards/Certifications/Handbooks_for_NBE_Certification_Programs.aspx?hkey=7112c1e2-41c8-41af-8881-864c460648d4 [cited 2018 Jun 30]. [Google Scholar]
- 29.Denault A, Rochon A. Transesophageal echocardiography training: looking forward to the next step. Can J Anaesth 2011; 58: 1–7. [DOI] [PubMed] [Google Scholar]
- 30.Costello C, Yastrebov K, Yang Y, Hilton A, Vij S, Orde S. Minimum standards for ultrasound equipment in intensive care. Recommendations from CICM Ultrasound Special Interest Group. Australas J Ultrasound Med 2017;20:41–6. [DOI] [PMC free article] [PubMed] [Google Scholar]