

Abstract
This study examines multiple pathways by which maternal childhood sexual trauma may be related to the behavioral development of children. Propensity score matching procedures were used to create matched groups (total N = 204) of mothers who retroactively did or did not self-report childhood sexual trauma in a longitudinal sample of families living in poor, rural communities. Using structural equation modeling, maternal characteristics and behaviors were examined as potential mediators of the relationship between maternal histories of childhood sexual trauma and children’s conduct problems. After controlling for numerous socio-demographic factors, analyses indicate that maternal depressive symptoms, intimate partner violence, and maternal parenting were significant mediators and highlight the lasting impact of childhood sexual trauma on victims and their children.
Keywords: childhood sexual trauma, conduct problems, parenting, maternal depressive symptoms, intimate partner violence
Childhood sexual trauma (CST) is a pervasive, persistent, and pernicious problem in the United States and represents a major public health concern for victims and their children. Compared to women without CST histories, women with CST histories report problems with numerous domains of adult functioning, including greater levels of depression (for reviews, see Paolucci, Genuis, & Violato, 2001; Maniglio, 2010), parenting difficulties (Testa, Hoffman, & Livingston, 2011; Bailey, DeOliveira, Wolfe, Evans, & Hartwick, 2012), and intimate partner violence (DiLillo, Giuffre, Tremblay, & Peterson, 2001). Similarly, children of women with CST histories are believed to be at risk for numerous developmental difficulties including behavior problems, although it is important to note that not all children of mothers with CST histories have compromised behavioral outcomes (Alexander, Teti, & Anderson, 2000; DiLillo & Damashek, 2003).
Methodology may be the cause for some of the heterogeneity of findings across studies, including issues related to sampling, differences in the use of statistical controls in analyses, and definitional issues related to what constitutes sexual trauma (Putnam, 2003). Broadly, definitions of CST range from exposure to pornographic material to physical assault (Putnam, 2003). Moreover, one of the major limitations of previous research on CST has been the absence of comparable/similar control groups (Ryan, Kilmer, Cauce, Watanabe, & Hoyt, 2000).
Recent work expanding earlier models of the sequela of CST have attempted to identify potential mediators in the association between maternal CST histories and developmental outcomes in the next generation. Some of these mediational pathways include mother’s psychopathology and relationship quality (Roberts et al., 2004). Schuetze and Das Eiden (2005) documented that maternal depression and intimate partner violence (IPV) mediated the relation between history of CST and maternal use of punitive discipline with her children, indicating the importance of examining multiple mediators including the mother-child relationship as mechanisms through which maternal history of CST may impact the development of children.
There has been concern about bias arising from the use of retrospective questioning of adults about their childhood experiences (Widom, & Morris, 1997; Fisher, Craig, Fearon, Morgan, Dazzan, Lappin, ... & Murray, 2009). Although recall bias is a common criticism of retrospective reports of adverse experiences in childhood, Hardt and Rutter (2004) concluded in their review that retrospective reports were sufficiently valid to be used for research purposes. Their review points to underreporting of childhood abuse experiences, which would attenuate the association between CST and adult functioning. Furthermore, in their study of the reliability of recall of abuse over time, Dube and colleagues (2004) reported that retrospective responses to childhood abuse and related forms of serious household dysfunction were stable over time (Dube, Williamson, Thompson, Felitti, & Anda, 2004).
Pathways from Maternal Childhood Sexual Trauma to Offspring Conduct Problems
The term conduct problems is used to describe a broad range of disruptive and rule-breaking behaviors, including temper tantrums, frequent arguing with adults, lying, truancy, and more serious types of antisocial behavior such as physical aggression, theft, property destruction, and alcohol and substance use (Hinshaw & Lee, 2003; Fergusson, John Horwood, & Ridder, 2005; Webster‐Stratton, Jamila Reid, & Stoolmiller, 2008). Although many young children experience mild behavior problems such as disobeying adults or temper tantrums, not all young children with early conduct problems develop more severe conduct disorders. For some children, however, research findings indicate that early behavior problems are related to the later development of more serious psychopathology (Hinshaw & Lee, 2003; Lahey, & Waldman, 2003).
Despite the growing literature on conduct problems in older children, less is known about problem behaviors during the early school years. The early school years represent a key developmental phase in which children are required to learn new rules and regulations, set goals, and self-regulate emotions. For children with conduct problems such as aggression and oppositional behavior, emerging evidence suggests that when left untreated, these problem behaviors may become crystallized patterns of antisocial behavior by late childhood and early adolescence (Broidy, Nagin, Tremblay, Bates, Brame, Dodge, ... & Vitaro, 2003; Costello, Mustillo, Erkanli, Keeler, & Angold, 2003), and begin a trajectory of escalating academic problems, school drop-out, substance abuse, delinquency, and violence (Loeber & Farrington, 2000; Snyder, 2001).
The literature on child conduct problems suggests that associations between risk factors and the development of problem behaviors often involve a complex set of interrelated risk processes including parenting behavior and family functioning (Tolan, Dodge, & Rutter, 2013; Pardini, Waller, & Hawes, 2015). These studies suggest that complex models may be necessary to account for the interplay among risk factors in predicting child conduct problems (Kraemer, Stice, Kazdin, Offord, & Kupfer, 2001). This issue may be especially relevant to the study of conduct problems in children whose mothers experienced CST since prior research has documented that mothers with trauma histories are at risk for a number of difficulties in their own adjustment and interpersonal relationships which in turn could influence the behavioral development of their children (Roberts et al., 2004). For example, the sequelae associated with a history of childhood sexual trauma may limit the resources individuals need to care for their offspring and intensify the pressures of parenting (Ruscio, 2001; Testa, Hoffman, & Livingston, 2011). However, despite empirical findings that CST is related to later impaired parenting and maladaptive child outcomes, there is still much we do not understand about the mechanisms by which CST is carried forward to affect the next generation of children.
Roberts et al. (2004) found an association between CST and child adjustment problems was partially mediated by maternal anxiety but not parenting. Collishaw and colleagues (2007) reported that maternal hostility fully mediated the association between maternal CST and offspring behavioral development (Collishaw, Dunn, O’connor, & Golding, 2007). Although limited, these discordant findings highlight the need for additional investigations examining the intergenerational transmission of maternal CST. The present study examined three potential mediators: maternal depressive symptoms, IPV, and parenting behavior, linking maternal CST to child conduct problems.
The role of parenting behaviors
Considering the multiple demands of parenting and the impact of childrearing practices on children, it is critical to gain a better understanding of the relationship between CST and subsequent parenting behaviors. Family systems theorists have long noted that parenting is a complex, multidimensional process that is vulnerable to a variety of influences, such as the parent’s relationship quality with the partner or depressive symptoms (Belsky, 1984; Bornstein, Hahn, & Haynes, 2011). The few studies that have examined the role of intervening variables have found that at least a portion of the relationship between CST and subsequent parenting is accounted for by factors such as depressive symptomatology (Banyard, Williams, & Siegel, 2003; Mapp, 2006) and IPV (Noll, 2005).
Numerous explanations have been posited to understand the association between CST and later parenting difficulties. Researchers speculate that some of the parenting difficulties reported by the survivors may develop from a general home environment characterized by more profuse adversity compared to women without a history of CST (Alexander, 1993). This line of thinking would suggest that survivors are likely to have grown up in a chaotic and dysfunctional family environment that provided them with inadequate exposure to healthy and effective models of parenting (Lyons-Ruth & Block, 1996; DiLillo, 2001). This possibility is supported by reports from mothers with a history of CST who cite a lack of exposure to models of successful caregiving as an impediment to their own effective parenting (Armsworth & Stronck, 1999). It is also likely, however, that the abuse experience and its associated symptoms (e.g., depressive symptoms) may diminish not only the survivors’ ability to manage the demands of parenting, but also their confidence in their own childrearing abilities (DiLillo, 2001; Teti & Gelfand, 1991). Whichever perspective is endorsed, however, what is clear from the literature is that mothers with CST histories report difficulties in the parenting role (DiLillo & Damashek, 2003).
Although prior research has focused attention on the parenting behaviors of women with sexual trauma histories, fewer studies have examined specific parenting outcomes using observational methods that allow for independent assessment of the mother’s behavior while interacting with her child. Parenting observations offer the advantage of recording overt behavior, which may be less open to differing interpretations than are items on a self-report (Lyons-Ruth & Block, 1996). For example, Zvara and colleagues (2015), using observational assessments of parenting behavior reported that females who experienced CST showed poorer functioning across multiple domains of parenting including sensitivity but with maternal report of parenting efficacy (Zvara, Mills-Koonce, Carmody, Cox, 2015). The present study examined sensitive caregiving behaviors, which have been linked to multiple aspects of children’s self-regulatory development and behavioral adjustment (Campbell, Shaw, & Gilliom, 2000).
The role of maternal depressive symptoms
Depression is one of the most commonly occurring and well-established outcomes for adult female survivors of CST with some reports suggesting a fourfold greater lifetime risk of developing major depression than women who do not have a history of abuse (Putnam, 2003, see reviews by Paolucci, et al., 2001). Maternal depressive symptoms have been identified as powerful risk factors for a variety of negative developmental outcomes in children (see reviews by Goodman, 2007; Goodman et al., 2011), and is believed to disrupt effective parenting and undermine intimate relationships (Civic & Holt, 2000; Burke, 2003). Mothers who exhibit higher levels of depressive symptoms tend to be less responsive and show flatter affect with their children (Jameson, Gelfand, Kulcsar, & Teti, 1997). This is especially true when maternal depression is chronic rather than short-term as might be expected for mothers with CST histories given the long term sequela associated with CST (Campbell, Cohn, Flanagan, Popper, & Meyers, 1992; Petterson & Abers, 2001).
Previous parenting research with CST survivors highlights the risk maternal depressive symptoms convey for problems in caregiving (Schuetze and Das Eiden, 2005). CST and its associated symptoms are believed to diminish the survivors’ ability to manage the demands of parenting (DiLillo, 2001) by depleting resources needed for optimal caregiving behavior. However, although research findings have established the link between maternal depressive symptoms and difficulties in parenting, it is still unclear which specific aspects of maternal behavior are influenced by depression (Marmorstein, Malone, & Iacono, 2004; Knutson, DeGarmo, Koeppl, & Reid, 2005). The present study tested whether maternal depressive symptomatology mediated the associations between maternal CST and non-optimal parenting behaviors and subsequent child conduct problems.
The role of intimate partner violence (IPV)
A substantial body of literature has documented the harmful consequences of IPV on numerous child outcomes (Grych & Fincham, 2001; Kitzmann, Gaylord, Holt, & Kenny, 2003) including direct and indirect effects on child difficulties in managing emotions and acquiring self-regulatory skills (Levondosky & Graham-Bermann, 2000; Crockenberg & Langrock, 2001; Cummings & Davies, 2010; Raver, 2004). These studies posit that anger and frustration from the adult relationship carry over into their parenting behavior thereby influencing child outcomes (Cummings & Davies, 2002; Krishnakumar & Buehler, 2000). IPV has been shown to negatively impact parenting behaviors and is associated with less sensitive maternal parenting behaviors (Levendosky & Graham-Bermann, 2000).
Several studies note that women with a history of childhood sexual trauma experience an increased risk of suffering additional interpersonal revictimization as adults, including elevated rates of IPV, with some studies suggesting two to five times greater likelihood of experiencing IPV (Daigneault, Hébert, & McDuff, 2009; DiLillo, et al., 2001). For example, DiLillo et al., (2001) found that women who had a history of CST were more likely to report that their intimate relationships involved severe forms of physical aggression and violence, including pushing, hitting, kicking, and beating, than those who did not have such a history. In a retrospective study of over 17,000 adults, Dong, Anda, Dube, Giles, and Felitti (2003) found that respondents who experienced CST were also significantly more likely to experience IPV. Similarly, Banyard, Williams, Saunders and Fitzgerald (2008) found significant correlations between CST and severe intimate partner violence in adulthood. The present study tested whether IPV mediates the associations between maternal CST and sensitive behaviors and subsequent child conduct problems.
The Current Study
Building upon previous research, the present study used a propensity matched design to examine the associations between maternal childhood sexual trauma and conduct problems in offspring and extends previous research by examining factors in the mothers’ current context that may be related to these associations. More specifically, the current study used a longitudinal approach to examine multiple mediating pathways by which maternal CST may be related to conduct problems in children through maternal depressive symptomatology, IPV and maternal parenting behaviors. Propensity score matching was used to examine the associations between maternal sexual trauma on adult functioning by creating matched groups based on background characteristics (e.g., poverty).
Given previous reports suggesting a unique effect of CST on subsequent parenting behaviors, in the current study, we focused on CST as compared to child maltreatment more broadly (i.e., physical abuse, neglect). For instance, in their study of infant attachment patterns of mothers with childhood experiences of physical or sexual abuse, Lyons-Ruth and Block (1996) found that the strongest correlate of decreased nurturance for the infant was the severity of CST. Additional work found that childhood sexual abuse history was associated with parenting competence above and beyond the effects of other forms of childhood maltreatment (Bailey, DeOliveira, Wolfe, Evans, & Hartwick, 2011).
For the purposes of this study, CST is defined as “the engagement of a child in sexual activities for which the child is developmentally unprepared and cannot give informed consent” (Draucker & Martsolf, 2008, p. 1034). The focus of this study is on females who were forced to engage in physical sexual contact against their will at or under the age of 14. Various researchers posit that when the trauma occurs to young children, they may have less refined coping strategies and less ability to control their environments, which may lead to feelings of helplessness. Others suggest that when the abuse occurs during the early years in which identity and cognitive schemas about self and others are developing, the trauma may become a part of the victim’s internal representations of the self and self in relation to others (Toth, Maughan, Manly, Spagnola, & Cicchetti, 2002). In contrast, another line of thinking maintains that older children and adolescents may be able protect their own sense of self as separate from the experience of the trauma due to a more mature and complex sense of self and a more developed ability to think abstractly.
Based on extant literature, this study proposed several hypotheses: (1) there will be a significant positive association between maternal CST and conduct problems in offspring at grade 1 above and beyond child temperament; (2) the association between maternal CST and offspring conduct problems will be mediated by maternal depressive symptoms and IPV; (3) the pathways between CST, maternal depressive symptoms, IPV, and offspring conduct problems will be further mediated by mothers’ observed parenting behaviors.
Method
Participants
The sample was drawn from the Family Life Project (FLP), a longitudinal, multi-method, multi-respondent study of rural poverty that explored the ways in which child, family, and contextual factors shape child development over time. FLP employed complex sampling procedures to recruit a representative sample in 3 target counties in eastern North Carolina and 3 target counties in central Pennsylvania. Mothers were recruited in the hospital the day after giving birth. A total of 1,292 families enrolled in the FLP by completing the first home visit when the family’s infant was two months old. Of these, 144 biological mothers reported that they had experienced childhood sexual trauma at or before the age of 14. Using propensity score matching procedures, a contrast group was created based on carefully chosen covariates (the procedures for the propensity matching are described in the analysis plan). The selection of the covariates was based on prior research that identified factors such as household income and parental education as risk factors for CST (Butler, 2013). In addition, early work by Finkelhor (1993) noted that a disproportionate number of CST cases reported to Child Protective Services came from families in the lower socioeconomic classes. The selection of the covariates was based on prior research that identified factors such as household income and parental education as risk factors for CST (Butler, 2013). Furthermore, there is some debate in the literature about whether it is CST per se that affects the long term interpersonal problems of adult victims or whether these mental health and parenting problems are related to a general level of family risk that allowed the trauma to occur in the first place (Kendall-Tackett, 2007). Thus, by controlling for early life risk factors, we attempted to isolate the effects of childhood trauma above and beyond the effects of family of origin and other traumas experienced in childhood. Women who have experienced childhood sexual trauma (as assessed by the Trauma History Questionnaire, Green, 1996) were matched on mothers’ childhood demographic variables to a group of women (controls) who have not experienced childhood sexual trauma.
Although all 144 women reporting CST were entered into the PSM procedures, thirty-nine (39) of these participants did not have exact matches with women in the not abused group, and thus were not included in the final subsample for this analysis. The final subsample (n=204) for the current study after completion of the PSM procedures was 105 women who experienced childhood sexual trauma matched to 99 women who did not. We further examined the demographic characteristics of the CST group before (n=144) and after (n=105) the matching procedures with regards to maternal age, race, education and income, finding no significant differences between the CST group before and after the matching procedures.
Procedures
Data for the present study were derived from the 6-, 24-, 36- and 60-month child-age and 1st grade data collection time points. At each of these time points, two research assistants visited children and families in their homes where they administered interviews and questionnaires to the parents (via laptop computer), conducted child assessments, and video recorded parent-child interactions for later coding. Visits lasted between two and three hours each. The covariates for the matching procedure were drawn from the 2-month interview in which mothers reported on their own families of origin. Trauma history data were collected at two different time points, either the 36- or the 60- month visit, depending on time restrictions for the visit. Mothers only completed the trauma questionnaire once.
Measures
Trauma History Questionnaire.
At either the 36- or the 60-month home visit (depending on time availability), the Trauma History Questionnaire (THQ; Green, 1996) was administered to all primary caregivers. The THQ is a 24-item self-report measure that assesses experiences with potentially traumatic events, such as crime, general disaster, and sexual and physical assault. For each event endorsed, respondents were asked to provide the frequency of the event, their age at the time of the event, and the nature of their relationship with the abuser for those events involving perpetrators (e.g., sexual abuse or being beaten). For the purposes of this study, we selected the item related to sexual abuse/assault. Respondents were first asked, “Has anyone ever done something sexual to you against your will, such as made you have intercourse, oral or anal sex, touched private parts of your body, or made you touch theirs, or otherwise forced you to have unwanted sexual contact?” If the respondent answered yes, then they were asked, “How old were you when this occurred?” Respondents were asked to rate on a 6-point Likert-type scale (where 1= 0–4 years of age, 2 = 5–11 years of age, 3 = 12–14 years of age, 4 = 15–18 years of age, 5 = 19–25 years of age, and 6 = 26+ years of age). The subsample of women who reported experiencing sexual trauma at or before the age of 14 was used in the present analysis.
Mothers’ family of origin information for propensity score matching.
The variables for the propensity score matching were drawn from the 2-, 36-, and 60-month interviews. At the 2-month interview, mothers were asked if, when they were growing up (aged 0 −18), any family members with whom they lived received AFDC (Aid to Families with Dependent Children), food stamps or Medicaid, or lived in public housing. They were also asked the highest grade completed by the primary mother-figure that was in their childhood home, with the scale ranging from 0= no school to 22= PhD, where values 0–11 indicate highest grade level completed, and values 12–22 include milestones such as obtaining a Graduate Equivalency Diploma (GED) (12), graduating from high school (14), completing a four year college degree (18), and obtaining a PhD (22). From either the 36- or 60-month interview additional non-sexual traumas experienced in childhood (e.g., being mugged or beaten, experiencing natural disasters such as tornadoes or hurricanes) were also used in the matching procedure (i.e., Trauma History Questionnaire, Green, 1996).
Maternal depressive symptomatology.
The Brief Symptom Inventory (BSI; Derogatis, 2000) was administered to mothers at the 6-, 15-, 24-, and 36-month visits. The BSI is a 23-item self-report questionnaire regarding psychological distress. Mothers were asked to rate on a 4-point Likert-type scale (where 0 = not at all and 4 = extremely) how distressed they were by each symptom over the past seven days. The measure’s six-item depression subscale was used in this study. A latent variable for maternal depressive symptoms was created using maternal reports across the four time points to capture a global assessment of depressive symptomatology. Cronbach’s alphas ranged from .83 - .88 in our sample for the four time points.
Intimate partner violence.
To assess intimate partner violence (IPV), the Conflict Tactics Scale-Couple Form Revised (CTS-R; Straus, Gelles, & Smith, 1990) was administered to all mothers at the 6-, 15-, 24-, and 36-month visits. Scores on the 9-item Physical Violence subscale of this measure (which captures incidences of physical aggression and violence) from each of the four time points were used in this study. An example item reads ‘‘How often in the past 12 months have you/your partner kicked, bit, or hit him/her/you with a fist?” In an effort to more accurately capture the experience of the mothers in this sample across the four assessments when the target child was 6, 15, 24, and 36 months old, a latent variable for IPV was created using maternal reports of their own IPV and their report of their partners’ IPV across the four time points. Cronbach’s alphas for the 18-item total scores for physical violence ranged from .74 −.88 in our sample for the four time points.
Observed maternal parenting behaviors.
When the children were 60-months old, mother-child dyads were presented with two developmentally appropriate activities. The tasks included (1) an activity involving the mother and child each building towers to match a model provided using wooden blocks, and (2) a card game called ‘slap-jack’. For the tower building task, mothers were told that this was a task for the child to complete but that they could provide any assistance they deemed necessary. For the card task, mothers were instructed that when the card turned up was a ‘Jack,’ both the mother and child were to slap the pile. The first one to slap the pile won those cards. Mothers then taught the game to their child and the mother and child played the game. It was expected that this activity would provide an opportunity to observe expression of affect from the mother and the child as well as the child’s emotional regulation in a potentially exciting and/or frustrating situation. The two digitally recorded episodes lasted approximately 15 minutes in total.
For the 60-month parent-child interactions, global rating scales of parent behavior (Cox and Crnic, 2002) were subsequently coded by trained coders observing the digital recordings. The codes relevant to the current study included: sensitivity/responsiveness, detachment/disengagement, stimulation of cognitive development, and positive regard. These scales were adapted from those used by the National Institute for Child Health and Human Development Study of Early Child Care and Youth Development (NICHD SECCYD, 1999). Coders rated parenting behaviors on a 7-point scale (1 = not at all characteristic and 7 = very characteristic). Both frequency and intensity of behavior or affect toward the child were considered. The sensitivity/responsiveness scale, adapted from Ainsworth, Blehar, Waters, and Wall (1978), describes the degree to which the parent was aware of and responsive to the child’s bids and signals for attention and achieved synchrony with the child. The detachment/disengagement scale describes the degree to which the parent was emotionally distant, uninvolved, or unaware of the child’s signals or needs for appropriate facilitation or care. The stimulation of cognitive development scale measures the degree to which the parent engaged in age-appropriate behaviors that foster cognitive and physical development of the child. The positive regard scale rates the quantity and intensity of the parent’s expression of positive feelings toward the child, including praise, smiling, physical affection, playful behavior, and overall enjoyment. All coders were blind to other information about the families. Two master coders trained and certified all coders until each demonstrated reliability across subscales (.80 intraclass correlation or higher with a criterion coder). Every coder also continued to code at least 20% of cases with a criterion coder throughout the coding period to ensure continued reliability with the criterion/master coder. For this subsample, inter-rater reliability was greater than .80 across pairs of coders for sensitive parenting.
A composite measure of sensitive parenting was created as the mean of the reverse score for the detachment/disengagement scale and the scores for sensitivity/responsiveness, positive regard, and stimulation of cognitive development scales. Higher sensitive parenting reflects parenting behaviors that are child-centered, engaged, warm, and stimulating, whereas lower sensitivity scores reflect parenting behaviors that are cold and inattentive to the child’s needs.
Child conduct problems.
Child conduct problems at Grade 1 were assessed using the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997). The SDQ is a 25-item parent report of child behaviors rated on a 3-point Likert scale. The 5-item subscale for conduct problems was used in current analyses. Mothers reported on their children’s behavior with such items as “can be spiteful to others” and “often loses temper.” Cronbach’s alpha for this measure at grade 1 was .74.
Control variables.
A number of demographic covariates were incorporated into the current investigation in order to account for the possibility that these factors were partially responsible for any observed relation between CST, IPV, maternal depressive symptomatology, maternal parenting behaviors, and child conduct problems. Poverty status, maternal education, ethnic minority status, and child sex have each been identified as important correlates of parenting (see Conger, Conger, & Martin, 2010, for a review). Thus, the family’s income-to-needs ratio, maternal education and the race and sex of the target child were included as covariates in this model. Income-to-needs ratios were calculated at each assessment time point by dividing the total household income from all possible sources by the federally determined poverty threshold for the number of people living in the household for that year. Income-to-needs ratios above 1.0 indicate that a family is able to provide for basic needs, whereas values below 1.0 indicate that they are not.
In addition, given previous research suggesting that child temperament may be related to maternal depressive symptoms, less sensitive parenting, and child conduct problems (Putnam, Sanson, & Rothbart, 2002; Bridgett, Gartstein, Putnam, McKay, Iddins, Robertson,...& Rittmueller, 2009; Frick & Morris, 2004; Tronick, 1989), we controlled for child temperamental reactivity at age 6 months as assessed by the Infant Behavior Record (IBR; Bayley, 1969) and adapted for use by Stifter & Corey (2001). Completed independently by both research assistants, the IBR scales included sociability, positive affect, attention, activity level, reactivity, and irritability. The summed mean score of the two data collectors’ ratings was used. Alphas ranged from .70 (irritability) to .88 (attention). Given that the overwhelming majority of the African American families who participated in this study resided in North Carolina, location of residence (Pennsylvania vs. North Carolina) was included to address a potential confound between site and ethnicity.
Analysis Plan
Propensity score matching.
Propensity score matching for this study followed the method developed by Rosenbaum and Rubin (1983) and involved several steps and followed “exact match” procedures allowing for replacements. Matching with replacements allows a given control or comparison unit to be included in more than one matched set (Hill & Reiter, 2006). The benefit to this type of matching is that it reduces bias because it does not ‘force’ a match to comparison units that may be different in terms of the estimated propensity score (Dehejia & Wahba, 2002). After the conclusion of the matching procedures, a subsample of participants with and without sexual trauma histories was identified (n=204). Diagnostic tests determined that the two groups were more similar to each other than with the larger sample from which the subsample was derived (i.e., the full FLP sample from which the comparison group was drawn). This means that, based on childhood family of origin variables, the two groups were statistically not different, leaving childhood sexual trauma (yes or no) as the one differentiator among those variables considered (See Table 1). Details of the matching procedures have been previously published (Zvara et al., 2015).
Table 1.
Descriptive Statistics and Correlations among Variables:
| 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|
| 1. 1st Grade Conduct Problems | 1 | ||||
| 2. Depressive Symptoms^ | .29** | 1 | |||
| 3. Intimate Partner Violence^^ | .32** | .26** | 1 | ||
| 4. Sensitive Parenting | −.29** | −.23** | −.21** | 1 | |
|
| |||||
| Mean (sd) | .35 (.40) | .43 (.50) | 6.1 (5.1) | 3.8 (1.1) | |
| Range | 0–1.8 | 0–2.8 | 1–26.6 | 1–7 | |
Note: *p < .05
p < .01
Depressive symptoms summed across five time points
IPV summed across five time points
Structural equation modeling (SEM) was used to test the proposed models (Schumacker & Lomax, 1996). Models were parameterized using the Mplus 6.0 software package (Muthén & Muthén, 2010) using the robust maximum likelihood estimator. Full information maximum likelihood (FIML) was used as the missing data technique (Arbuckle, 1996). FIML estimation uses all available observations and provides unbiased estimation of model parameters in the presence of missing data. There was an average of 15% missing data on our mediators and control variables across time points. The goodness-of-fit of the models was examined using the comparative fit index (CFI) and the root mean square error of approximation (RMSEA). The CFI varies between 0 and 1.0 and values of .90 or higher indicate acceptable fit (Hu & Bentler, 1995). The RMSEA is bounded by zero and will take on that value when a model exactly reproduces a set of observed data. A value of .05-.06 is indicative of close or adequate fit, a value of .08 is indicative of marginal fit, and higher values are indicative of poor fit (Browne & Cudeck, 1994).
Results
Preliminary Analyses
Matching results and balance checking for matched sample.
The matching methods reduced the standardized mean difference with each covariate when compared to the unmatched data suggesting that the two groups are more similar with each other than with the larger FLP sample from which the control sample was drawn on those covariates. In addition, following the PSM, all matching variables were regressed on childhood sexual trauma history. There were no significant differences between the post-matched groups on any of these variables (results not shown due to page limitations). This means that based on childhood family of origin variables, the two groups were statistically not different leaving childhood sexual trauma (yes or no) as the one differentiator among the variables considered.
Descriptive statistics.
Descriptive statistics and bivariate correlations are presented in Table 2. The group with CST histories was comprised of 57.1% European Americans and 42.9% African Americans, whereas the NCST group was comprised of 55.6% European Americans and 44.4% African Americans. Of the 105 women in the CST group, 12% of the women reported sexual trauma before the age of 4, 59% between the ages of 4–11, and 29% between the ages of 12–14. Approximately half of the women in the CST group reported four or more sexual trauma experiences, and 55% reported that the perpetrator was either a parent or other relative (e.g., grandparent, uncle).
Independent sample t-tests were conducted to compare mean differences between the two groups with regards to descriptive information and found there was no significant difference between the two groups for maternal age, with mothers in the CST group reporting a mean age of 25.5 (sd = 5.2) and NCST mothers reporting a mean age of 26.1 (sd = 5.4). There was also no significant difference between the two groups for maternal education, with mothers in the CST group reporting 14.1 years of education (sd = 2.9) and mothers in the NCST group reporting 14.5 years (sd = 2.6) of education. There was, however, a group difference noted for mean family income-to-needs, (M = 1.40, sd = 1.13) and (M = 2.1, sd = 2.56), t (204) = 2.53, p < .001, meaning that, on average, the CST group reported significantly less current household income compared to the NCST group.
An examination of the bivariate correlations among key variables found that child conduct problems were positively related to maternal depressive symptoms (r = .29, p < .01), intimate partner violence (r = .32, p < .01), and inversely related to sensitive parenting (r = −.29, p < .01).
Mediation Analysis
In the next set of analyses, we tested the full theoretical model linking maternal childhood sexual trauma to children’s conduct problems at grade 1 through maternal depressive symptoms, IPV and maternal parenting, and controlling for the family’s current income-to-needs ratio, maternal education, data collection site, child race, sex, temperament ratings, and additional maltreatment experienced by the victim. Paths were estimated to include all covariates and subsequent predictors of child conduct problems. In the next model, which included maternal depressive symptoms, IPV, and maternal sensitivity as mediators, the estimated path was significant above and beyond controls. All significant paths can be found in Figure 1. This model was a good fit to the data, χ2 (48, N = 204) = 77, p < .01, CFI = .90, RMSEA = 0.06. When considered in a model with maternal depressive symptoms, IPV, and sensitive parenting, there was no direct significant association between childhood sexual trauma and conduct problems, but there was a trend towards significance (β = .11, p = .07). We did find, however, a main effect of childhood sexual trauma on depressive symptoms (β = .27, p < .001), which in turn was related to conduct problems (β = .19, p < .01). Childhood sexual trauma was positively related to the IPV latent variable (β = .30, p < .001), which in turn was related to maternal sensitivity (β = −.42, p < .001). Childhood sexual trauma was related to maternal sensitivity (β = −.39, p < .001), which was related to child conduct problems (β = −.26, p < .01). Moreover, there were significant indirect pathways from maternal childhood sexual trauma and child conduct problems. One pathway was through maternal depressive symptoms (childhood sexual trauma → maternal depressive symptoms → child conduct problems, β = .04, p < .05); a second pathway was through maternal sensitive parenting (childhood sexual trauma → maternal sensitive parenting → child conduct problems, β = .06, p < .05); and a third pathway was through IPV and maternal parenting behaviors (childhood sexual trauma → IPV → maternal sensitive parenting → child conduct problems, β = .03, p < .05). The model accounted for 22.6% of the variance in child conduct problems.
Figure 1.
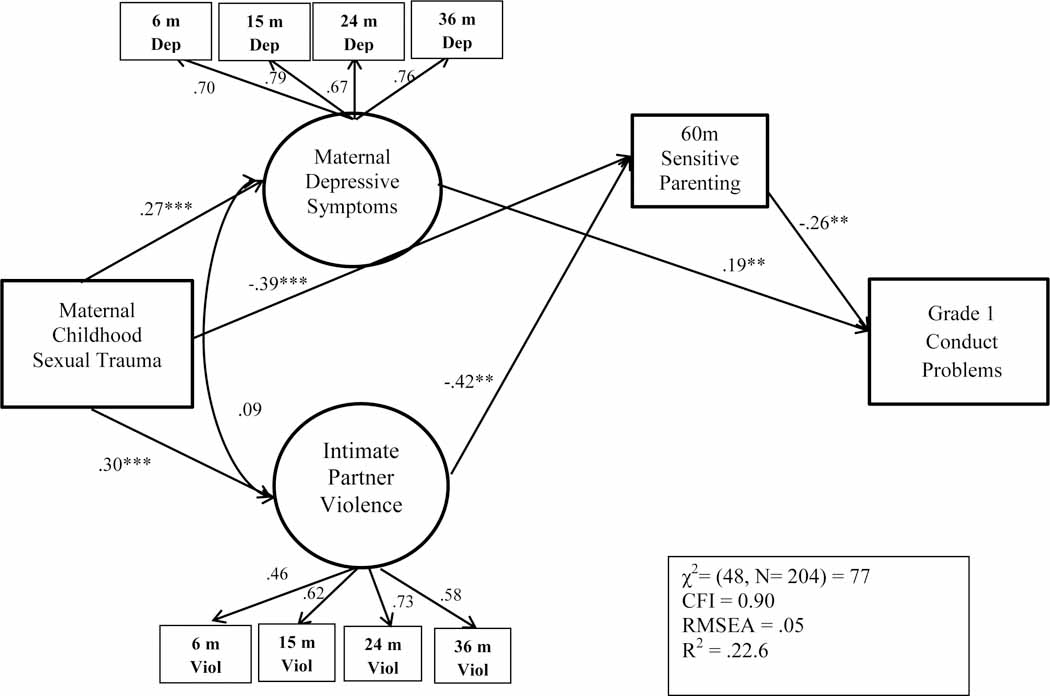
The mediating role of maternal depressive symptoms, IPV and maternal sensitive parenting in associations between maternal childhood sexual trauma and child conduct problems at 1st grade.
Following procedures outlined by Holmbeck (1997, 2002), a second model was estimated in which the paths from CST to child conduct problems were set to zero. A chi-squared difference test revealed that constraining these paths to zero did not result in a significant decrement to model fit. These findings, in addition to the significant indirect effect, confirm full mediation indicating that, after controlling for numerous covariates, IPV across the first three years of life and maternal sensitive parenting at 60 months fully mediated the relation between CST and child conduct problems at grade 1.
Discussion
This study adds to the literature on intergenerational associations of CST by examining the relations between maternal trauma histories and children’s behavioral development and possible explanatory mechanisms for these relations. A clear strength of this study is the inclusion of maternal history of CST, IPV, maternal depression, parenting dimensions, and child conduct problems allowing us to simultaneously examine dimensions likely to impact child functioning and to investigate pathways and relative contributions of multiple constructs. Examination of intergenerational processes linking parents’ histories with subsequent parenting practices and children’s outcomes provides an important contribution to the literature. Additional strengths of this current study include the use of a clear definition of childhood sexual trauma, a propensity matched sample with appropriate controls, and a longitudinal design to study the extent to which a mother’s childhood sexual trauma history exerts itself across time to influence the development of her child.
Using propensity score matching with family of origin variables to create a control group from within the same community sample and by controlling for additional maltreatment experienced by the victim, the present study attempted to isolate the associations of childhood sexual trauma above and beyond the effects of family of origin risks and other traumas experienced in childhood. In addition, we examine maternal psychological and relational characteristics (depressive symptoms, IPV) across the early years of her offspring’s life (6 months - 36 months) along with parenting behavior to allow for a better understanding of how developmental risk may be transferred across generations by examining conduct problems in children of women who have and have not reported trauma histories. These findings have implications for researchers and clinicians working with school aged children whose mothers report childhood sexual abuse histories, as it appears that maternal CST may be associated with conduct problems.
Although past research has suggested evidence to support these models, this study is, to the best of the authors’ knowledge, the first to simultaneously test multiple direct and indirect associations between maternal childhood sexual trauma, maternal psychological, behavioral, and relational characteristics, and children’s conduct problems. Consistent with expectations, this study found support for the idea that mothers’ childhood sexual trauma is related to the developmental outcomes of the next generation. More specifically, even after controlling for numerous characteristics associated with child and family risk, there were multiple significant pathways by which maternal childhood sexual trauma was related to offspring conduct problems. The results highlighted the unique roles of maternal depressive symptoms, IPV, and parenting behaviors as key mediators in the examination of intergenerational linkages of maternal childhood sexual trauma.
The findings from the current study reveal maternal depressive symptomatology as a particularly significant mediating pathway to child conduct problems for families with women reporting CST. Indirect pathways from maternal depressive symptomatology remained significant in the presence of numerous covariates, suggesting that maternal depressive symptoms have an independent effect on child conduct problems above and beyond the effect of IPV and parenting for mothers with CST histories. Although not surprising given the numerous reports highlighting elevated rates of depression and depressive symptoms for survivors of CST, the current study findings point to the need for increased awareness of the linkages of CST on development of offspring through maternal depressive symptomatology. Screening mothers with CST histories for depressive symptomatology may alert interventionists to the need for providing additional services to children and families with a mother reporting childhood sexual trauma.
In the current study, we found two indirect pathways from CST to child conduct problems through less sensitive parenting, (maternal childhood sexual trauma → maternal sensitive parenting → child conduct problems, and maternal childhood sexual trauma → IPV → maternal sensitive parenting → child conduct problems). These indirect paths suggest that CST has a direct and indirect effect on mother’s ability to provide warm, responsive care. That IPV is associated with less sensitive parenting is consistent with previous research that found partner violence to be negatively related to parenting behaviors including observed parenting warmth, which, in turn, was associated with increased behavior problems in children (Levendosky & Graham-Bermann, 2000). These findings are particularly troublesome given the findings of previous research linking IPV to a range of adverse outcomes in school age children, including behavioral problems (Grych & Fincham, 2001; Kitzmann et al., 2003; Levondosky & Graham-Bermann, 2000), and highlight the need for screening for CST in adult and child mental health settings as well as domestic violence shelters. Given the complex interplay among the mediating influences between CST and parenting, mental health services must target all of these factors that independently and together may increase the likelihood of poor parenting outcomes and child conduct problems. By expanding our understanding of the indirect associations of childhood sexual trauma in areas such as mental health and IPV, practitioners can become more informed of the stressors that affect some women’s parenting capacities and create service responses that enhance the lives of trauma survivors and their children.
We did not, however, find support for our hypothesis that depressive symptoms and sensitive parenting would mediate the association between CST and conduct problems. It may be that mothers with CST histories struggle with their own regulatory processes (i.e., depression) and are thus less responsive to their children’s bids for attention and care (Ruscio, 2001). Although parental sensitivity is multifaceted, one key component is support for child needs and the ability to read signals from children related to what they may require from the caregiver. A mother who is focused on her own regulation is less likely to be emotionally attuned to the needs of her child. Given the significant indirect paths from CST to child conduct problems through IPV and parenting, another possible explanation may relate to the broader contextual risk that may accompany maternal depression, such as increased family stress and lower levels of support. Therefore, it would be important for future work to disentangle the processes by which maternal depression may impact children’s behavioral development including the interplay among multiple environmental exposures.
Strengths and Limitations
The current study extends our understanding of the impact of maternal childhood sexual trauma on children’s emotional functioning in an understudied population of rural families. The longitudinal models allowed us to examine these relationships over a relatively large span of time, allowing for a clearer understanding of the long-term associations of maternal childhood sexual trauma. In addition, much of what we know regarding the parenting of mothers with CST histories has been through the use of self-report measures. The present study uses independent assessment of parenting behavior in the context of a dyadic interaction to allow for an objective understanding of parenting behavior. Further, this is one of the first studies to examine the influence of caregivers’ histories of childhood sexual trauma on children’s behavioral development using multiple domains of parenting.
Despite these strengths, several limitations should be noted. As with most studies of childhood adverse experiences and particularly with sexual victimization, the current study relies on a self-reported measure of sexual trauma as recalled years after the event. Researchers have expressed concern that the passage of time may distort recollections of the experience (Dube et al., 2004; Hardt & Rutter, 2004). For example, if an individual who has experienced sexual trauma is assigned to a non-trauma control group while someone who did not experience the trauma is classified as having the trauma, then these false negatives and false positives will obscure distinctions between women who have and have not experienced childhood sexual trauma (Briere & Elliott, 2003).
Furthermore, we relied on maternal retrospective recall to characterize their childhood sociodemographic characteristics, which played a critical role in selecting a group of comparison families. Although it could be argued that many adults may not be aware of, much less be able to recall, their families’ SES status or highest grade completed by their mothers, early work by Krieger and colleagues (1998) support the validity of adult recall of measures of childhood socioeconomic factors in childhood including parental education (Kreiger, Okamoto, & Selby, 1998; see also, Batty, Lawlor, Macintyre, Clark, & Leon, 2005; Mckenzie, & Carter, 2009). In addition, although we used numerous variables from the family of origin for the matching procedure, we did not account for all of the potential confounders that might have been relevant to subsequent parenting of survivors, such as family dysfunction in the women’s family of origin (e.g., parental marital conflict, mental health, or substance use).
Also, using mother’s report of their sexual trauma, depressive symptoms, IPV, and child conduct problems brings to bear the issue of single source reporting and the possibility of shared method variance that could inflate some of the associations detected. However, as previously noted, due to the longitudinal nature of the study, data for this study was collected with considerable time intervals (e.g., from 6 months to the time the child entered grade 1) and, as such, are unlikely to be subject to shared variance as might arise, for example, from current psychological state. Importantly, both techniques used in this current study, PSM and SEM, have been associated with causal analysis in the literature; however, interpreting these estimates as causal hinges on the assumption that there are no omitted variables in the PSM stage and no omitted paths in the SEM stage (Imai, Keele & Tingley, 2010). Thus, the findings from this study must be interpreted as correlational in nature.
Future Directions
Our study was limited to families living in rural, low-income communities who had given birth to a child. Although the sample used in the current study was both economically and racially diverse, it likely was not representative of all children living in homes characterized by maternal CST; thus, future research should explore these associations using data from different populations. Moving forward, vigilance to definitional issues relating to what constitutes childhood sexual trauma will allow researchers to compare and assess findings across studies and create a cohesive and organized body of work potentially providing practitioners avenues for targeted interventions.
In our assessment of IPV, we did not consider the chronic nature of the violence between adults. Therefore, it is possible that, if a mother was in a violent relationship during the child’s infancy, but not later in development, the impact on the child would differ from children who had more chronic exposure or who had violence exposure later in childhood. Future research will need to tease apart the effects of chronicity of IPV in the lives of women with CST histories. Similarly, we did not consider factors such as the severity, frequency, or age of abuse initiation in our analysis which could affect the impact sexual abuse has on subsequent functioning. Examining additional aspects of the abuse experience will provide a more nuanced approach to understanding the long term sequela of CST. In addition, given the co-occurrence of CST with childhood neglect, it is possible that many of the mothers in this sample may have experienced sexual abuse in the context of child neglect. Future studies will need to differentiate the unique effects of CST above and beyond the effects of childhood neglect.
In order to get a fuller conceptualization of the impact of child sexual trauma on parenting behavior, and to ultimately understand the mechanisms by which a mother’s childhood sexual trauma may exert itself long term and influence the development of her offspring, additional studies testing moderating and mediating relationships among a variety of variables that may impact childrearing would greatly increase knowledge. For example, characteristics of the child may play an important role in moderating the associations of caregiver trauma histories on children. This, along with other considerations within the family system, characteristics of the child such as temperament should be included as part of the broader context of parental functioning for mothers with a history of CST. Investigating for whom and under what circumstances maternal CST impacts young children’s behavioral development, therefore, may be an important future direction given that these moderation analyses have the potential to identify groups of children that may be at heightened risk for the negative consequences of maternal experiences.
Acknowledgments
Support for this research was provided by the National Institute of Child Health and Human Development (PO1-HD-39667), with co-funding from the National Institute on Drug Abuse. Additional support was provided by the National Institute on Alcohol Abuse and Alcoholism (A12–0934) awarded as a predoctoral fellowship (F31) to the lead author.
References
- Ainsworth MDS, Blehar MC, Waters E, & Wall S (1978). Patterns of attachment: A psychological study of the strange situation Lawrence Erlbaum. [Google Scholar]
- Alexander PC (1993). The differential effects of abuse characteristics and attachment in the prediction of long-term effects of sexual abuse. Journal of Interpersonal Violence, 8, 346–362. [Google Scholar]
- Alexander PC, Teti L, & Anderson CL (2000). Childhood sexual abuse history and role reversal in parenting. Child Abuse & Neglect, 24, 829–838. [DOI] [PubMed] [Google Scholar]
- Arbuckle JL (1996). Full information estimation in the presence of incomplete data. In Marcoulides GA & Schumacker RE (Eds.), Advanced structural equation modeling (pp. 243–277). Mahwah, NJ: Erlbaum. [Google Scholar]
- Banyard VL, Williams LM, & Siegel JA (2003). The impact of complex trauma and depression on parenting: An exploration of mediating risk and protective factors. Child Maltreatment, 8(4), 334–349. [DOI] [PubMed] [Google Scholar]
- Batty GD, Lawlor DA, Macintyre S, Clark H, & Leon DA (2005). Accuracy of adults’ recall of childhood social class: findings from the Aberdeen children of the 1950s study. Journal of Epidemiology and Community Health, 59(10), 898–903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bayley N . (1969). Bayley Scales of Mental Development New York: Psychological Corporation. [Google Scholar]
- Belsky J (1984). The determinants of parenting: A process model. Child Development, 55, 83–96. [DOI] [PubMed] [Google Scholar]
- Bentler PM (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238–246. [DOI] [PubMed] [Google Scholar]
- Bornstein MH, Hahn CS, & Haynes OM (2011). Maternal personality, parenting cognitions, and parenting practices. Developmental Psychology, 47, 658–675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bridgett DJ, Gartstein MA, Putnam SP, McKay T, Iddins E, Robertson C, ... & Rittmueller A (2009). Maternal and contextual influences and the effect of temperament development during infancy on parenting in toddlerhood. Infant Behavior and Development, 32(1), 103–116. [DOI] [PubMed] [Google Scholar]
- Briere J, & Elliott DM (2003). Prevalence and psychological sequelae of self-reported childhood physical and sexual abuse in a general population sample of men and women. Child Abuse & Neglect, 27, 1205–1222. [DOI] [PubMed] [Google Scholar]
- Browne MW, & Cudeck R (1993). Alternative ways of assessing model fit. Sage Focus Editions, 154, 136–136. [Google Scholar]
- Butler AC (2013). Child sexual assault: Risk factors for girls. Child abuse & neglect, 37(9), 643–652. [DOI] [PubMed] [Google Scholar]
- Campbell SB, Shaw DS, & Gilliom M (2000). Early externalizing behavior problems: Toddlers and preschoolers at risk for later maladjustment. Development and Psychopathology, 12, 467–488. [DOI] [PubMed] [Google Scholar]
- Conger RD, Conger KJ, & Martin MJ (2010). Socioeconomic status, family processes, and individual development. Journal of Marriage and Family, 72, 685–704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cox MJ, & Crnic K (2002). Qualitative ratings for parent-child interaction at 3–12 months of age Unpublished manuscript, University of North Carolina at Chapel Hill. [Google Scholar]
- Cox MJ, & Harter KSM (2003). Parent-child relationships. In Bornstein MH, Davidson L, Keyes CLM, & Moore KA (Eds.), Wellbeing: Positive development across the life course (pp. 191–204). Mahwah, NJ: Erlbaum. [Google Scholar]
- Crockenberg S, & Langrock A (2001). The role of specific emotions in children’s responses to interparental conflict: A test of the model. Journal of Family Psychology, 15(2), 163–182. [DOI] [PubMed] [Google Scholar]
- Cummings EM, & Davies PT (2010). Marital conflict and risky families. In Cummings EM, & Davies PT (Eds). Marital conflict and children: An emotional security perspective (pp 5–21). New York and London: The Guilford Press. [Google Scholar]
- Deater-Deckard K, Dodge KA (1997). Externalizing behavior problems and discipline revisited: Nonlinear effects and variation by culture, context, and gender. Psychological Inquiry, 8, 161–175. [Google Scholar]
- Dehejia R, & Wahba S (2002). Propensity score matching methods for non-experimental causal studies. Review of Economics and Statistics, 84, 151–161. [Google Scholar]
- Derogatis L (2000). Brief Symptom Inventory 18 Minneapolis, MN: NCS Pearson. [Google Scholar]
- DiLillo D (2001). Interpersonal functioning among women reporting a history of childhood sexual abuse: Empirical findings and methodological issues. Clinical Psychology Review, 21, 553–576. [DOI] [PubMed] [Google Scholar]
- DiLillo D, & Damashek A (2003). Parenting characteristics of women reporting a history of childhood sexual abuse. Child Maltreatment, 8, 319–333. [DOI] [PubMed] [Google Scholar]
- DiLillo D, Giuffre D, Tremblay GC, & Peterson L (2001). A closer look at the nature of intimate partner violence reported by women with a history of child sexual abuse. Journal of Interpersonal Violence, 16(2), 116–132. [Google Scholar]
- Dubowitz H, Black MM, Kerr MA, Hussey JM, Morrel TM, Everson MD, & Starr RH (2001). Type and timing of mothers’ victimization: effects on mothers and children. Pediatrics, 107(4), 728–735. [DOI] [PubMed] [Google Scholar]
- Ethier LS, Couture G, & Lacharité C (2004). Risk factors associated with the chronicity of high potential for child abuse and neglect. Journal of Family Violence, 19(1), 13–24. [Google Scholar]
- Fergusson DM, Horwood LJ, Lyndkey MT. (1996). Child sexual abuse and psychiatric disorder in young adulthood, II: psychiatric outcomes of childhood sexual abuse. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 1365–1374. [DOI] [PubMed] [Google Scholar]
- Fisher HL, Craig TK, Fearon P, Morgan K, Dazzan P, Lappin J, ... & Murray RM (2009). Reliability and comparability of psychosis patients’ retrospective reports of childhood abuse. Schizophrenia Bulletin, sbp103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzpatrick M, Carr A, Dooley B, Flanagan‐Howard R, Flanagan E, Tierney K, ... & Egan J (2010). Profiles of adult survivors of severe sexual, physical and emotional institutional abuse in Ireland. Child Abuse Review, 19, 387–404. [Google Scholar]
- Foster CJE, Garber J, & Durlak JA (2008). Current and past maternal depression, maternal interaction behaviors, and children’s externalizing and internalizing symptoms. Journal of Abnormal Child Psychology, 36(4), 527–537. [DOI] [PubMed] [Google Scholar]
- Frick PJ, & Morris AS (2004). Temperament and developmental pathways to conduct problems. Journal of Clinical Child and Adolescent Psychology, 33(1), 54–68. [DOI] [PubMed] [Google Scholar]
- Goodman R (1997). The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. [DOI] [PubMed] [Google Scholar]
- Goodman SH, Rouse MH, Connell AM, Broth MR, Hall CM, & Heyward D (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14(1), 1–27. [DOI] [PubMed] [Google Scholar]
- Green BL (1996). Trauma history questionnaire. In Stamm BH (Ed.), Measurement of stress trauma and adaptation (pp. 366–369). Lutherville, MD: Sidran. [Google Scholar]
- Grych JH, & Fincham FD (Eds.). (2001). Interparental conflict and child development: Theory, research and applications Cambridge University Press. [Google Scholar]
- Gustafsson HC, & Cox MJ (2012). Relations among intimate partner violence, maternal depressive symptoms, and maternal parenting behaviors. Journal of Marriage and Family, 74(5), 1005–1020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hardt J, & Rutter M (2004). Validity of adult retrospective reports of adverse childhood experiences: review of the evidence. Journal of Child Psychology and Psychiatry, 45(2), 260–273. [DOI] [PubMed] [Google Scholar]
- Hill J, Pickles A, Burnside E, Byatt M, Rollinson L, Davis R, Harvey K (2001). Child sexual abuse, poor parental care and adult depression: evidence for different mechanisms. The British Journal of Psychiatry, 179(2), 104–109. [DOI] [PubMed] [Google Scholar]
- Hill J, & Reiter JP (2006). Interval estimation for treatment effects using propensity score matching. Statistics in Medicine, 25(13), 2230–2256. [DOI] [PubMed] [Google Scholar]
- Imai K, Keele L, & Tingley D (2010). A general approach to causal mediation analysis. Psychological Methods, 15(4), 309–334. [DOI] [PubMed] [Google Scholar]
- Kendall-Tackett K (2002). The health effects of childhood abuse: Four pathways by which abuse can influence health. Child Abuse & Neglect 26(6), 715–729. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Gardner CO, & Prescott CA (2002). Toward a comprehensive developmental model for major depression in women. American Journal of Psychiatry, 159(7), 1133–1145. [DOI] [PubMed] [Google Scholar]
- Kitzmann KM, Gaylord NK, Holt AR, & Kenny ED (2003). Child witnesses to domestic violence: A meta-analytic review. Journal of Consulting and Clinical Psychology, 71(2), 339–352. [DOI] [PubMed] [Google Scholar]
- Kraemer HC, Stice E, Kazdin A, Offord D, & Kupfer D (2001). How do risk factors work together? Mediators, moderators, and independent, overlapping, and proxy risk factors. American Journal of Psychiatry, 158(6), 848–856. [DOI] [PubMed] [Google Scholar]
- Krieger N, Okamoto A, & Selby JV (1998). Adult female twins’ recall of childhood social class and father’s education: a validation study for public health research. American Journal of Epidemiology, 147(7), 704–708. [DOI] [PubMed] [Google Scholar]
- Levendosky AA, & Graham-Bermann SA (2000). Behavioral observations of parenting in battered women. Journal of Family Psychology, 14(1), 80–94. [DOI] [PubMed] [Google Scholar]
- Levendosky AA, Huth-Bocks AC, Shapiro DL, & Semel MA (2003). The impact of domestic violence on the maternal-child relationship and preschool-age children’s functioning. Journal of Family Psychology, 17(3), 275–287. [DOI] [PubMed] [Google Scholar]
- Lovejoy MC, Graczyk PA, O’Hare E, & Neuman G (2000). Maternal depression and parenting behavior: A meta-analytic review. Clinical Psychology Review, 20(5), 561–592. [DOI] [PubMed] [Google Scholar]
- Lyons-Ruth K, & Block D (1996). The disturbed caregiving system: Relations among childhood trauma, maternal caregiving, and infant affect and attachment. Infant Mental Health Journal, 17(3), 257–275. [Google Scholar]
- Mckenzie SK, & Carter KN (2009). Are retrospective measures of childhood socioeconomic position in prospective adult health surveys useful? Australasian Epidemiologist, 16(3), 22–24. [Google Scholar]
- Mapp SC (2006). The effects of sexual abuse as a child on the risk of mothers physically abusing their children: A path analysis using systems theory. Child Abuse & Neglect, 30(11), 1293–1310. [DOI] [PubMed] [Google Scholar]
- Marmorstein NR, Malone SM, & Iacono WG (2004). Psychiatric disorders among offspring of depressed mothers: Associations with paternal psychopathology. American Journal of Psychiatry, 161, 1588–1594. [DOI] [PubMed] [Google Scholar]
- Molnar BE, Buka SL, & Kessler RC (2001). Child sexual abuse and subsequent psychopathology: results from the National Comorbidity Survey. American Journal of Public Health, 91(5), 753–760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, & Muthén B (2010). Mplus 6.0 Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- NICHD Early Child Care Research Network (1999). Child care and mother–child interaction in the first three years of life. Developmental Psychology, 35, 1399–1413. [PubMed] [Google Scholar]
- Noll JG (2005). Does childhood sexual abuse set in motion a cycle of violence against women? What we know and what we need to learn. Journal of Interpersonal Violence, 20(4), 455–462. [DOI] [PubMed] [Google Scholar]
- Noll JG, Trickett PK, & Putnam FW (2003). A prospective investigation of the impact of childhood sexual abuse on the development of sexuality. Journal of Consulting and Clinical Psychology, 71(3), 575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paolucci EO, Genuis ML, & Violato C (2001). A meta-analysis of the published research on the effects of child sexual abuse. The Journal of Psychology, 135(1), 17–36. [DOI] [PubMed] [Google Scholar]
- Pereda N, Guilera G, Forns M, & Gómez-Benito J (2009). The prevalence of child sexual abuse in community and student samples: A meta-analysis. Clinical Psychology Review, 29(4), 328–338. [DOI] [PubMed] [Google Scholar]
- Putnam FW (2003). Ten-year research updates review: Child sexual abuse. Journal of the American Academy of Child & Adolescent Psychiatry, 42(3), 269–278. [DOI] [PubMed] [Google Scholar]
- Putnam SP, Sanson AV, & Rothbart MK (2002). Child temperament and parenting. Handbook of Parenting, 1, 255–277. [Google Scholar]
- Raver C (2004). Placing emotional self‐regulation in sociocultural and socioeconomic contexts. Child Development, 75(2), 346–353. [DOI] [PubMed] [Google Scholar]
- Roberts R, O’Connor T, Dunn J, & Golding J (2004). The effects of child sexual abuse in later family life; mental health, parenting and adjustment of offspring. Child Abuse & Neglect, 28(5), 525–545. [DOI] [PubMed] [Google Scholar]
- Rosenbaum PR, & Rubin DB (1983). The central role of the propensity score in observational studies for causal effects. Biometrika, 70(1), 41–55. [Google Scholar]
- Ruscio AM (2001). Predicting the child-rearing practices of mothers sexually abused in childhood. Child Abuse & Neglect, 25(3), 369–387. [DOI] [PubMed] [Google Scholar]
- Ryan KD, Kilmer RP, Cauce AM, Watanabe H, & Hoyt DR (2000). Psychological consequences of child maltreatment in homeless adolescents: Untangling the unique effects of maltreatment and family environment. Child Abuse & Neglect, 24(3), 333–352. [DOI] [PubMed] [Google Scholar]
- Schuetze P, & Das Eiden RD (2005). The relationship between sexual abuse during childhood and parenting outcomes: Modeling direct and indirect pathways. Child Abuse & Neglect, 29(6), 645–659. [DOI] [PubMed] [Google Scholar]
- Schumacker RE, & Lomax RG (1996). A beginner’s guide to structural equation modeling Mahwah, NJ: Lawrence Erlbaum Associates, Inc. [Google Scholar]
- Senn TE, & Carey MP (2010). Child maltreatment and women’s adult sexual risk behavior: Childhood sexual abuse as a unique risk factor. Child Maltreatment, 15, 324–335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Straus MA, Gelles RJ, & Smith C (1990). Physical violence in American families: Risk factors and adaptations to violence in 8,145 families (pp. 29–47). New Brunswick, NJ: Transaction Publishers. [Google Scholar]
- Stuart EA (2010). Matching methods for causal inference: A review and a look forward. Statistical Science: A Review Journal of the Institute of Mathematical Statistics, 25, 1–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tolan PH, Dodge K, & Rutter M (2013). Tracking the multiple pathways of parent and family influence on disruptive behavior disorders. In Tolan PH & Leventhal BL (Eds). Disruptive Behavior Disorders (pp. 161–191). New York: Springer. [Google Scholar]
- Trickett PK, Noll JG, & Putnam FW (2011). The impact of sexual abuse on female development: Lessons from a multigenerational, longitudinal research study. Development and Psychopathology, 23(2), 453–476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weich S, Patterson J, Shaw R, & Stewart-Brown S (2009). Family relationships in childhood and common psychiatric disorders in later life: systematic review of prospective studies. The British Journal of Psychiatry, 194(5), 392–398. [DOI] [PubMed] [Google Scholar]
- Widom CS, & Morris S (1997). Accuracy of adult recollections of childhood victimization, part 2: childhood sexual abuse. Psychological Assessment, 9(1), 34–46. [Google Scholar]
- Zvara BJ, Mills-Koonce WR, Carmody KA, Cox M, & Family Life Project Key Investigators. (2015). Childhood sexual trauma and subsequent parenting beliefs and behaviors. Child Abuse & Neglect, 44, 87–97. [DOI] [PMC free article] [PubMed] [Google Scholar]