

Abstract
Introduction
Considerable evidence supports an association between poor impulse control (impulsivity) and violent crime. Furthermore, impulsivity and aggression has been associated with reduced levels of serotonergic activity in the brain. Selective serotonin reuptake inhibitors (SSRIs) are a class of antidepressants that aim to regulate brain serotonin concentrations. Several small studies in psychiatric populations have administered SSRIs to impulsive–aggressive individuals, resulting in reduced impulsivity, anger, aggression and depression. However, no clinical trial has been undertaken in a criminal justice population. This protocol describes the design and implementation of the first systematic study of the potential benefits of SSRIs in impulsive–violent offenders who are at high risk of reoffending.
Methods and analysis
A randomised, double-blinded, multicentre trial to test the clinical efficacy of an SSRI, sertraline hydrochloride, compared with placebo on recidivism and behavioural measures (including impulsivity, anger, aggression, depression and self-reported offending) over 12 months. 460 participants with histories of violence and screening positive for impulsivity are recruited at several local courts and correctional service offices in New South Wales, Australia.
Ethics and dissemination
Results will be submitted for publication in a peer-reviewed journal. Possible implications of the effectiveness of this pharmacological intervention include economic benefits of reducing prison costs and societal benefits of improving safety. This study has received ethical approval from the University of New South Wales, Aboriginal Health & Medical Research Council, Corrective Services NSW and the NSW Justice Health and Forensic Mental Health Network.
Trial registration number
ACTRN12613000442707.
Keywords: impulse control disorders, public health, forensic psychiatry
Strengths and limitations of this study.
The study has its origins in the link between impulsivity, offending behaviour and brain serotonin dysregulation.
This large-scale, community-based study is one of the first to use a pharmacotherapy (selective serotonin reuptake inhibitor) to address offending.
The trial has significant ethical and medical oversight to ensure it is conducted to the highest standards.
The study has developed a unique infrastructure in the community for recruiting and retaining this unique and challenging group.
The primary outcome, reoffending, will be determined by linkage with official court offending records. While this represents a well-defined and unambiguous outcome, it is likely to constitute an underestimate of the actual frequency of reoffending, given the well-recognised underdetection of such episodes.
Introduction
Background
Violence is a leading cause of death and injury worldwide and a large percentage of prison inmates have histories of violent offending, including domestic violence.1 Between 1996 and 2010, violent crimes (homicide, assault, sexual assault and robbery) rose by around 30% in Australia;2 and many of those convicted return to prison within 2 years (44% of those convicted for assault and 47% of those convicted for robbery).3 In 2016, 2.2 million adults in Australia were estimated to have been victims of domestic violence from a partner from the age of 15.4 The rate of domestic violence reoffending within 12 months in New South Wales continues to increase, reaching around 16% in 2018.5
Impulsivity and offending
Impulsivity can be defined as ‘behaviour without adequate thought, the tendency to act with less forethought than do most individuals of equal ability and knowledge, or a predisposition toward rapid, unplanned reactions to internal or external stimuli without regard to the negative consequences of these reactions’.6
Numerous studies support the strong association between poor impulse control (impulsivity) and crime, including violent crime. Horvath found a correlation between impulsivity scores and self-reported criminal behaviour in a sample of American undergraduates.7 Krueger examined the relationship between personality characteristics and delinquency in a large sample of New Zealand youth, and found that an index of ‘control’ was negatively correlated with self-reported delinquency.8 In another study, university students examined the records of 251 crimes and were more likely to classify violent offences (manslaughter, murder, assault and rape) as impulsive than non-violent offences (arson and forgery).3
Impulsivity is also associated with reoffending, especially violent reoffending. A Canadian study found that half of a recidivist sample took approximately 1 hour from first conceptualising a crime to execution of the act.9 In a study measuring impulsivity in murderers, Heilbrun found that those who committed ‘impulsive’ homicide had a higher recidivism rate (62%) compared with premeditated murderers (45%).10
Impulsivity, aggression, and serotonin
Evidence from pharmacological, brain imaging and receptor subtyping research suggests a relationship between serotonergic dysfunction, aggression and impulsivity.11 Reduced levels of cerebrospinal-fluid concentrations of 5-hydroxyindoleactic acid (5-HIAA), a metabolite of serotonin believed to be a marker of presynaptic serotonergic activity in the brain, have been correlated with measures of aggression and impulsivity in free ranging monkeys,12 young men with personality disorders,13 psychiatric patients,14 and violent offenders.15 Lower 5-HIAA concentrations were found among impulsive recidivists who committed violent offences or arson than among matched non-recidivists.15
Aggression refers to behaviour intended to harm another individual who does not wish to be harmed.16 The hypothalamus, periaqueductal grey and amygdala are some structures known to be important in the mediation of aggressive behaviours and there are rare clinical case reports of individuals with lesions (eg, tumours) in these structures manifesting highly pathological impulsive–aggressive behaviours.17 The prefrontal cortex is also a component of the relevant neural network, and damage to it, especially the ventromedial and orbitofrontal regions, have also been associated with impulsive (but not predatory) aggression.18 Because the prefrontal cortex is frequently damaged in the context of traumatic brain injury (TBI), TBI is a common potential cause of impulsive–aggression.19
Selective serotonin reuptake inhibitors (SSRIs)
The biological evidence supporting the link between serotonin dysfunction and aggression, and the availability of selective serotonin reuptake inhibitors (SSRIs) that aims to regulate brain serotonin concentrations has prompted researchers to trial the use of such medications to reduce anger and aggression.20–25 These studies have mostly been conducted in small, clinical populations of those with borderline personality20 26 and intermittent explosive disorder.21 24 One study conducted on 12 parolees found decreases in impulsivity and aggression over 3 weeks following administration of paroxetine.25 Similarly, neuropsychiatric disorders following traumatic brain injury such as depression and obsessive compulsive disorder have been successfully targeted with SSRIs.27 However, no systematic study has been conducted of the potential benefits of SSRIs for those in the criminal system who are both impulsive and violent and at high risk of reoffending.
Genetic responses to SSRIs
Several studies have shown that responses to SSRIs are related to functional polymorphisms of the promoter region of the serotonin transporter gene (5-HTTLPR).28–30 In terms of transcriptional activity, the long (l) variant is more than twice as active as the short (s) variant. In a study of 102 patients with depression, individuals bearing l/l or l/s genotypes were significantly more likely to respond to the SSRI fluvoxamine than those with the s/s genotype, with almost twice the reduction in depression scores after 6 weeks of treatment.29 A similar association of these polymorphisms with differential responsiveness to SSRIs has been described in patients with generalised social anxiety disorder.30 The influence of these HTTLPR polymorphisms on the efficacy of SSRIs in reducing impulsivity has not been reported.
In addition to the polymorphic nature of 5-HTTLPR promoter there are other metabolic enzymes that are involved in the metabolism of SSRIs which are also polymorphic. These include enzymes that encoded by the CYP450 genes CYP2D6 and CYP2C19. Variance in the metabolism and or uptake of SSRIs will result in variable responses to these agents. Genetic variation underscores the response to SSRIs, which is reflected in differential treatment efficacy. Polymorphisms in the HTTLPR gene (associated with serotonin reuptake) as well as in the CYP450 genes (CYP2D6 and CYP2C19) influence SSRI metabolism (for review see Probst-Schendzielorz et al. 2015)31 and these will be examined in our study using the Illumina Global Screening Array (GSA) or other applicable technology as it becomes available (such as direct massively parallel sequencing).
Rationale
While violence and offending behaviour are complex phenomena, the biological, behavioural, psychiatric, criminological and pharmacological evidence provides compelling support for the role of the serotonin system in impulsive–violence. In 2010, the UK National Institute of Clinical Excellence suggested in relation to antisocial personality, which is common among prisoners and offenders, that ‘impulsive dyscontrol and aggressive behaviour are important features of antisocial personality disorder and might usefully be targeted with SSRIs or mood stabilisers’.32
Pilot study
In 2008, we conducted an open-label pilot study examining the impact of sertraline given to men in the criminal justice system with histories of violence who were assessed as impulsive.33 Marked reductions were observed from baseline to 3-month follow-up in scores measuring impulsiveness (35% reduction), irritability (45%), anger (63%), assaultive behaviour (51%), verbal assault (40%), indirect assault (63%) and depression (62%).33 All who completed the pilot requested a referral to continue the medication under the supervision of their general practitioner.
Following the pilot study, a placebo-controlled, double-blind, randomised (1:1), parallel-arm superiority trial was developed which includes reoffending as a primary objective, as well as changes in behavioural measures as per the pilot study.
Study objectives
Primary objectives
Evaluate the effectiveness of SSRI (sertraline) in reducing reoffending in impulsive, repeat-violent offenders.
Secondary objectives
Examine the effectiveness of SSRI (sertraline) in improving behavioural measures (impulsivity, anger, aggression, irritability, quality of life, social functioning, substance use and alcohol consumption, self-reported offending, depression and psychological distress) in impulsive, repeat-violent offenders.
Investigate whether polymorphisms in the serotonin transporter gene 5-HTTLPR affect the efficacy of SSRI in reducing impulsivity in impulsive, repeat-violent offenders.
Methods
Intervention
Study drug
The SSRI used in this trial is sertraline hydrochloride (SETRONA in Australia).34 Sertraline is primarily used to treat major depression in adults but is also indicated for obsessive compulsive disorder, premenstrual dysphoric disorder, panic disorder and social anxiety in both adults and children.34
The trial medication comes in tablet form in a blister-pack. During dosage titration after the active run-in period, medication (active and placebo) is provided in an identical Webster Pack.
Placebo
Placebo sertraline contains the inactive ingredients of SETRONA (microcrystalline cellulose, calcium hydrogen phosphate, sodium starch glycollate, hydroxypropyl cellulose, magnesium stearate, white Opadry, hypromellose, titanium dioxide, macrogol 400, purified talc).34 Placebo tablets are identical in shape, colour and delivery to SETRONA. The dosing is the same as the active and both tablets are taken orally.
Treatment regimen
A dose of 100 mg/d of sertraline was chosen, balancing an expectation of efficacy with respect to the reduction of impulsivity at that dose against the risk of side effects at higher doses of the medication.
Dosage begins at 25 mg and is increased to 100 mg as follows: 25 mg/day (¼ tablet) for 1 day; 50 mg/day (½ tablet) for 1 day and 100 mg/d (one tablet) for the remainder of the 12 months.
Participants are offered the opportunity to remain on the study beyond 12 months, until the trial closes when the final participant reaches 12 months duration. If a participant consents to this, they are followed up every 3 months by research clinicians and every 6 months by a psychiatrist. Participants continue to take active medication or placebo, depending on their study arm. Those wishing to discontinue the trial at 12 months undergo the withdrawal procedure.
Study setting
The trial opened for recruitment in October 2013 and will cease recruitment at the end of June 2021. Referrals come from magistrates and lawyers at local courts in the Sydney Metropolitan, Central Coast, Western Sydney and Hunter areas of New South Wales. Magistrate referrals are based on a policy developed by the NSW Chief Magistrate’s Office which allows proceedings against an individual to be postponed for several weeks for individuals to be considered for the trial and determine eligibility (box 1).
Box 1. Eligibility criteria for participants.
Inclusion criteria
Male sex, and over the age of 18 years.
History of two or more violent offences (eg, manslaughter, robbery, assault and domestic violence).
Score of 70 or over on the Barratt Impulsiveness Scale.36
Medically fit to undertake the trial.
Able to provide informed consent.
Ability to communicate in English.
Exclusion criteria
Current use of any serotonergic drug.
Current use of Antabuse (disulfiram) medication.
History of adverse drug reactions to selective serotonin reuptake inhibitors.
Current use of any antipsychotic medication or prescription of an anticonvulsant medication for a mood disorder or the prescription of lithium carbonate.
Severe mental illness (eg, schizophrenia, bipolar disorder and major depression).
Considered to be at high risk of suicide.
Anticipation of receiving a custodial sentence.
Significant renal or hepatic impairment.
Inability to provide informed consent.
Conviction for murder or child sexual assault.
Impending deportation, moving interstate returning to a remote area.
Participants can also be recruited from those serving community orders under the supervision of Corrective Services NSW. Other passive recruitment methods include study flyers available at courts and other locations, word-of-mouth, self-referral, a free call number and study website (www.shortfuses.com.au).
Participants in the trial must have at least: (i) two prior convictions for violent offences; or (ii) one prior conviction for a violent offence and one current violent offence before the court for which they have entered a guilty plea or (iii) two violent charges which may include violent acts documented in the police fact sheet for which they intend to enter a guilty plea. The offence profile is confirmed by the ReINVEST clinician reviewing their criminal record, police fact sheet, offender management record or by liaising with an official representative (eg, lawyer, community corrections officer and police).
Eligibility criteria
The study’s eligibility criteria are outlined in box 1.
Sample size
The expected rate of first violent or impulsive reoffence in the control group is expected to be approximately 33% at 12 months, and a minimum of 12% reduction in this rate using sertraline would be considered sufficient to be clinically meaningful and have an impact on practice in this area. A sample size of 460 patients (230 in each group) would provide 80% power with 95% confidence to detect this difference. This sample size also allows for a cross-over/non-compliance rate of approximately 3.8%. While these estimates are conservative, if the control rate was 37%, the study would still have 80% power to detect a 12% absolute reduction. Reoffending rates will be monitored to ensure that the sample size will provide sufficient power to detect meaningful differences. This also includes an assessment of the non-compliance and cross-over rates. It is important to consider the attrition rate; we estimate that at least 1800 men will need to be assessed at the selection phase to achieve the sample size required for the trial.
The study will be reviewed prior to closing recruitment to ensure that appropriate conclusions can be made and, if necessary, the sample size reviewed to achieve adequate study power. Such reviews are made blinded to allocated treatment using pooled data.
Participants are financially reimbursed with $50 for the initial visit, $20 per assessment visit and $10 per visit when collecting medication to cover travel expenses.
Study outcomes
Primary study outcomes
The primary outcome is any instance of a convicted violent offence in the 12 months postrandomisation, obtained from the NSW Bureau of Crime Statistics and Research’s Reoffending Database (BOCSAR’s RoD). This includes the following Australian and New Zealand Standard Offence Classification (ANZSOC) categories: 01 (homicide and related offences); 02 (acts intended to cause injury); 03 (sexual assault and related offences); 04 (dangerous and negligent acts endangering persons); 05 (abduction, harassment and other offences against the person) and 06 (robbery, extortion and related offences).35 Court records and databases will also be checked to identify any events which may have been missed due to a ‘no show’ during the follow-up period.
Secondary study outcomes
The secondary outcomes are changes in behavioural measures of impulsivity,36 anger,37 aggression,38 irritability,38 quality of life,39 social functioning,40 substance use and alcohol consumption,41 42 self-reported offending, depression,43 and psychological distress44 in those taking SSRI compared with placebo.
Another secondary outcome will be determined by any significant differences in impulsivity36 and depression43 between those with s/s versus any l/l or l/s 5-HTTLPR polymorphisms in participants given SSRI.
Primary safety endpoints
The primary safety endpoints are death by suicide, serious drug overdose or development of serotonin toxicity45 (ie, these adverse events may or may not be related to the study treatment).
Study design
The study design is shown in figure 1.
Figure 1.
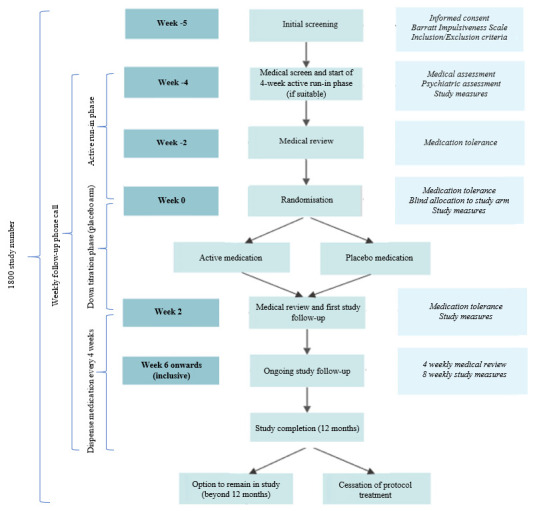
Study design.
Assessments
A number of assessments are undertaken prior to randomisation—an initial eligibility screen; medical screen; active run-in phase—and during the 12-month follow-up period (table 1).
Table 1.
Assessments and procedures by study week
| Initial screen (−5) |
Medical screen/run-in (−4) |
Review (−2) |
Rando. (0) | 2 | 6 | 10 | 14 | 18 | 22 | 26 | 30 | 34 | 38 | 42 | 46 | 1 year | |
| Eligibility criteria | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Demographic and criminographic information | ✓ | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Impulsivity, anger and aggression | |||||||||||||||||
| Barratt Impulsiveness Scale36 | ✓ | – | – | ✓ | ✓ | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – |
| State Trait Anger Expression Inventory37 | – | ✓ | – | – | ✓ | ✓ | – | – | – | ✓ | – | – | – | ✓ | – | – | – |
| Anger, Irritability and Assault Questionnaire38 | – | ✓ | – | ✓ | ✓ | ✓ | – | – | – | ✓ | – | – | – | ✓ | – | – | – |
| Lifestyle and mental health | |||||||||||||||||
| Short-Form-1239 | – | ✓ | – | – | ✓ | ✓ | – | – | – | ✓ | – | – | – | ✓ | – | – | – |
| Duke Social Support Index40 | – | ✓ | – | ✓ | – | – | – | – | – | ✓ | – | – | – | ✓ | – | – | – |
| Wechsler Individual Achievement Test61 | – | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Psychiatric assessment | – | ✓ | – | – | – | – | – | – | – | – | ✓ | – | – | – | – | – | ✓ |
| MINI International Neuropsychiatric Interview*62 | – | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| International Personality Disorders Examination63 | – | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Beck Depression Inventory43 | – | ✓ | ✓ | ✓ | ✓ | ✓ | – | ✓ | – | – | – | ✓ | – | – | – | – | – |
| Kessler Psychological Distress Scale44 | – | ✓ | – | ✓ | ✓ | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – |
| Alcohol Use Disorders Identification Test42 | – | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Substance use41 | – | ✓ | – | ✓ | ✓ | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – |
| Eysenck Impulsivity Questionnaire64 | – | ✓ | – | ✓ | ✓ | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – |
| Level of Service Inventory-Revised49 | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Offending behaviour | |||||||||||||||||
| Self-reported offending | – | – | – | ✓ | ✓ | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – | ✓ | – |
| BOCSAR’s Reoffending Database | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | ✓ |
| Other | |||||||||||||||||
| Sniffin’ Sticks65 | – | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Medical monitoring | |||||||||||||||||
| Medical assessment | – | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Saliva sample47 | – | ✓ | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Barnes’ Akathisia Rating Scale60, side effects | – | – | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Compliance monitoring | – | – | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Dispense study medication | – | ✓ | – | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
*Post-traumatic stress disorder, generalised anxiety disorder, social phobia, antisocial personality, obsessive compulsive disorder and panic disorder modules only.
Initial screening
This assesses whether a potential participant satisfies all of the health, offending and impulsivity (ie, score of 70 or more on the Barratt Impulsiveness Scale)36 inclusion criteria, and does not trigger any exclusion criteria (box 1). The BIS has been used for over 50 years and is perhaps the most widely used psychometric instrument to measure impulsivity. It has been used in over 500 studies in populations such as those with substance abuse/dependence specifically, depression, bipolar disorder, attention deficit hyperactivity disorder, suicide attempters and criminal offenders.46 It measures three components of impulsivity: cognitive (making quick decisions), motor (acting without thinking) and non-planning (lack of ‘futuring’ or forethought).
Medical screen and baseline assessments
If participants pass the initial screen and provide informed consent (see online supplemental files 1 and 2), they then complete a medical screening, psychiatric assessments and trial questionnaires (table 2) to further determine suitability and collect baseline measures. The medical screening involves a blood test (full blood count with platelets), liver function tests, thyroid function tests and urea, electrolytes and creatinine, jugular venous pressure, respiratory rate, chest sounds, air entry, cranial nerves, peripheral strength and reflexes, thyroid examination, cardiac sounds, blood pressure and heart rate. All participants are reviewed by a psychiatrist prior to commencing the trial medication.
Table 2.
Details of study assessments
| Assessment/procedure | Details |
| Demographic and criminographic information | Age, ethnicity, marital status, children, education, employment, accommodation, incarceration history, institution history (eg, juvenile detention centre, special school). |
| Barratt Impulsiveness Scale (BIS-11)36 | 30-item questionnaire that assesses three subtypes of trait impulsiveness: attentional impulsiveness, motor impulsiveness and non-planning impulsiveness. |
| State Trait Anger Expression Inventory (STAXI-2)37 | 57-item questionnaire that records subjective levels of anger in different situations including currently, in general and general behaviour when angry. |
| Anger, Irritability and Assault Questionnaire (AIAQ)38 | 42-item questionnaire that records subjective levels of anger, irritability and aggression in the past 2 weeks. |
| Short-Form-12 (SF-12)39 | 12-item questionnaire that provides a validated index of subjectively perceived quality of life. |
| Duke Social Support Index (DSSI)40 | 11-item questionnaire that provides a validated index of the degree of social support available to the participant. |
| Wechsler Individual Achievement Test (WIAT-11)61 | Provides a measure of reading ability. |
| Psychiatric assessment | Assesses mental health and enquires about psychiatric history, history of suicide and self-harm, and sexual history. |
| Mini International Neuropsychiatric Interview (MINI; post-traumatic stress disorder, generalised anxiety disorder, social phobia, antisocial personality disorder, obsessive–compulsive disorder, panic disorder only)62 | Provides an index of levels of anxiety, and personality disorder over a defined interval of time prior to the interview. |
| International Personality Disorders Examination (IPDE)63 |
Assesses impulsive personality disorder, dissocial personality disorder, borderline personality disorder. |
| Beck Depression Inventory-II (BDI-II)43 | 21-item questionnaire that enquires about symptoms over the past week to measure the severity of depression. |
| Kessler Psychological Distress Scale (K-10)44 | 10-item questionnaire intended to yield a global measure of distress based on questions about anxiety and depressive symptoms in past 4 weeks. |
| Alcohol Use Disorders Identification Test (AUDIT)42 |
Measures alcohol consumption in the previous 12 months. Indicates safe, harmful and hazardous alcohol use. |
| Substance use | Provides information on alcohol and drug use history. Questions derived from the 2001 New South Wales inmate health survey.41 |
| Eysenck Impulsivity Questionnaire (EIQ)64 | 54-item questionnaire that assesses impulsive personality. |
| Level of Service Inventory-Revised (LSI-R)49 | Measures offender risks and needs. Predictive of recidivism. |
| Self-reported offending* | Enquires about whether a criminal act or offence has been committed in the past 8 weeks, and if so, details about the offence(s). |
| Sniffin’ Sticks (16-item version)65 | This is used to examine for anosmia (loss of sense of smell), a possible proxy for prefrontal cortex damage. |
| Barnes’ Akathisia Rating Scale (BARS)60 | A rating scale to assess drug-induced akathisia. |
| Compliance monitoring | Provides a self-reported number of days per week, on average, that the participant ingested the study medication. |
*Subject to mandatory reporting under s316 of the NSW Crimes Act 1900.66
bmjopen-2020-044656supp001.pdf (96.9KB, pdf)
bmjopen-2020-044656supp002.pdf (130.7KB, pdf)
Genetic testing
Polymorphisms in the HTTLPR gene (associated with serotonin reuptake) as well as in the CYP450 genes (potentially linked to SSRI metabolism) will be examined using the Illumina GSA array or other applicable technology as it becomes available (such as direct massively parallel sequencing). If a participant consents to be involved in the genetics aspect of the study, a 2 mL saliva sample is collected by the research clinician using an Isohelix Genefix device during medical screening.47 Once provided, the tube is placed in a sealed, clinical sample bag and stored between 15°C and 30°C until couriered to the University of Newcastle for DNA isolation and specific polymorphism analysis.
Saliva samples have yielded sufficient high-quality DNA for genotyping. The relative success in isolating usable DNA is 98.24% of samples yielded sufficient DNA for genotyping. The range of DNA concentrations was 4 ng/ul (total volume 200 ul) to >1000 ng/ul (total volume 200 ul). When applied to a GSA array, samples had uniform assay characteristics.
To ensure confidentiality, all samples are deidentified and only the principal investigator is able to reidentify individual samples, if required. DNA samples and results are to be kept securely for 15 years post-publication.48
Active run-in phase
A 4-week run-in phase, during which all participants take the active medication, occurs prior to randomisation to identify those who react poorly to the medication or are not willing to commit to 12 months follow-up after initially consenting.
Randomisation and blinding
Eligible participants are randomised to either the active or placebo groups using an online randomisation system (Flexetrials software, developed and managed by the NHMRC Clinical Trials Centre, University of Sydney), and allocated a unique medication kit number to blind allocation.
Randomisation is performed using computer-generated random blocks of size 10, to ensure that in every block of 10 subjects, 50% are randomised to active treatment and 50% to placebo. Participants are stratified on age, impulsivity score (Barratt Impulsiveness Scale, BIS-11),36 Aboriginality, and Level of Service Inventory-Revised (LSI-R) score.49
At randomisation, participants are given a Webster Pack containing 2 weeks of medication. Participants randomised to the placebo arm of the study are titrated down to 50 mg/d for a week and then take a week of placebo medication. Those randomised to the active arm of the study receive a Webster Pack identical to the placebo group, but containing 2 weeks supply of 100 mg/d active medication.
There are no differences in the packaging or appearance of active drug and placebo to prevent the participant or research team being able to discriminate between them. The research clinician distributes medication kits to the participant at monthly face-to-face assessments.
Unblinding is only authorised by the clinical coordinator in consultation with the Medical Assessment Committee (MAC). This process is facilitated through the NHMRC Clinical Trials Centre who are responsible for the randomisation process. If a participant is unblinded, an unblinded report form is emailed to the MAC for review.
Participants returning to custody
As part of providing consent, participants give permission to the research team to liaise with Justice Health and Forensic Mental Health Network (JH&FMHN) in the event of their incarceration to potentially continue on the study or facilitate the withdrawal procedure. Participants are instructed to inform JH&FMHN nursing staff on reception that they are participating on the trial. Participants are withdrawn from the study if sentenced to a period of imprisonment of greater than 6 months.
For participants who wish to continue on the study while in custody, research clinicians assist custodial staff with obtaining the study medication via the JH&FMHN Central Pharmacy, which is administered by the clinic nurses. Participants are flagged in the JH&FMHN Patient Administration System using the pre-existing alerts system. Participants are reviewed by a research clinician every 8 weeks while in custody for assessment and administration of the study tools as per the study protocol.
Patient and public involvement
Subsequent to commencing the trial, we conducted deliberative work to determine the public’s appetite for interventions such as this, the attributes of the trial and willingness to pay for them.50–52 Prisoners were surveyed to determine possible interest in such a trial with 52% expressing an interest in learning more about the study.53
A 2008 pilot study was conducted on 34 impulsive violent men prior to seeking funding for the larger current study.33 For the current study, we invited participants to share their experiences of the trial in a video which is used as part of the recruitment process.54
Challenges
High attrition rates are problematic in longitudinal studies and clinical trials, particularly those involving challenging populations such as injecting drug users, ex-prisoners, and those with serious mental illness.55–58 Transient accommodation, frequent changing of mobile phones, chaotic lifestyles and limited social connections can hamper effective follow-up by researchers.58 A systematic review of longitudinal research with offenders found the average attrition rate was around 42% (Doring et al, unpublished manuscript). The current trial has a similar attrition rate with drop-out between randomisation and 12 months on the trial being around 47%. Other drop-out rates are 14% before initial screening, 18% after being screened and 15% during the run-in phase before randomisation. The run-in phase is a way of facilitating early discontinuation of participants who decide that they do not like being on medication or react poorly to it.
Studies that employ more retention strategies have lower drop-out rates. The current study uses several strategies to minimise loss to clinical follow-up such as establishing a systematic protocol for participant contact, scheduling appointments, obtaining contact details for alternative contacts, financial reimbursement for participation and ensuring staff receive specialised training in dealing with offender populations.
There are also challenges with study recruitment. A qualitative analysis conducted by the research team shows that the status of the current study being a ‘trial’ represents an impediment for some professional groups (eg, magistrates, community corrections officers and lawyers) who perceive that it is unfair to refer an individual to a placebo arm or a study that may prove inefficacious.
Statistical analysis
Primary outcomes
All analyses will be intention to treat. The primary analysis of reoffending within 12 months will be an unadjusted χ2 analysis. The effect of treatment will be given as a relative risk and 95% CI.
Efficacy of the treatment will also be evaluated using survival analysis with time to reoffending as the outcome and the explanatory variable of active SSRI or placebo. Other analyses will examine for treatment arm-specific differences in rates of offending. Additional analyses will be undertaken to seek correlates of apparent treatment response (eg, baseline impulsivity score, etc.).
Secondary outcomes
Changes in impulsivity,36 anger,37 aggression,38 irritability,38 quality of life,39 social functioning,40 substance use and alcohol consumption,41 42 depression43 and psychological distress44 scores from baseline to 12-month follow-up for the behavioural measures will be compared between treatment and placebo groups using independent t-tests.
Self-reported offending is typically more common than confirmed convicted offending.59 Analyses will be conducted to compare rates of self-reported offending of those in the treatment arm with those in the placebo arm.
To investigate whether polymorphisms in the serotonin transporter gene 5HTTLPR affect the efficacy of SSRIs, in those prescribed SSRI (ie, the treatment arm of the study) changes in impulsivity36 and depression43 from baseline to 12 months will be compared between those with s/s versus l/s or l/l alleles using a repeated measures analysis.
Data management
Records management is guided by systems implemented by the NHMRC Clinical Trials Centre, in line with requirements for record keeping in the NSW private sector, medico-legal requirements and the NSW State Records Act 1998. Trial documents are stored under medical records conditions for 15 years postpublication in the secure UNSW Shared File storage, with access restricted to the appropriate researchers who have access to UNSW networks.48 On the case report forms and other documents, a unique study code is used to identify the records.
Monitoring
Free call number
A 1800 free call number provides participants with access to the clinical coordinator or delegate 24/7 via a paging service, in the event of an emergency that pertains to participation in the trial. Emergency use of the 1800 number includes (but not be limited to) medical emergencies (eg, overdose, serious adverse event (SAEs)) and psychiatric emergencies (eg, suicidal ideation, self-harm and psychotic episode).
Weekly phone contact
Participants have weekly telephone contact with the research clinician to monitor any physical or psychological side effects of the trial medication, and determine their level of agitation using the Barnes’ Akathisia Rating Scale.60
Medical Assessment Committee (MAC)
The MAC comprises senior clinicians from the team. Its primary function is to assess those cases where the research clinicians and treating psychiatrists require further input and decision-making. Additionally, the MAC meets to discuss SAEs or unusual adverse events. In most cases, the trial psychiatrist and clinical coordinator are responsible for day-to-day medical decision-making. The MAC can be convened at short notice if required with the clinical coordinator arranging a teleconference with available members. The MAC is responsible for deciding whether an individual should be withdrawn from the trial on medical grounds.
Study governance
The study is overseen by a four-member Independent Data Safety Monitoring Board (IDSMB) comprising a senior clinical trials expert, an experienced biostatistician, a psychiatrist with experience in the forensic area and a psychologist with experience in delivering programmes in prison. Formal terms of reference have been written for the IDSMB. An IDSMB secretary organises these annual meetings and keeps minutes. A statistician provides reports to the IDSMB as requested.
Serious adverse events (SAEs)
The definition of an SAE is explained in box 2. SAEs are reported by the clinical coordinator to the MAC for decision-making and then to the IDSMB and the appropriate ethics committees, where appropriate, as soon as information becomes available. Adverse events are reported to the MAC as soon as possible.
Box 2. Serious adverse event definition.
A serious adverse event (SAE) is defined as one of the following.
An event that results in death.
An event that is life-threatening: a life-threatening event is present when the patient was, in the opinion of the Medical Assessment Committee, at immediate risk of death from the event as it occurred. This definition does not include an event that, had it occurred in a more serious form, might have caused death.
An event that is disabling or incapacitating.
An event that is a congenital anomaly in the offspring of a patient (male or female) who received the study drug.
An event that requires inpatient hospitalisation or prolongs a current hospitalisation. ‘Inpatient’ hospitalisation means that the patient has been formally admitted to a hospital for medical reasons. It does not include presentation at an emergency room. (An event only evaluated in the emergency room should be captured as an adverse event.)
Events that are not included in the above listed criteria for being SAEs, but may jeopardise the patient or require medical or surgical intervention to prevent one of the outcomes listed above or are otherwise considered medically significant by the investigator.
Cessation of protocol treatment
Requests to be withdrawn from the trial, or a decision by the clinical coordinator, psychiatrist or MAC that an individual should be discontinued on medical, psychiatric or other grounds (eg, sentenced to more than 6 months in prison or pending deportation) may occur. Grounds for medical discontinuation include: withdrawal due to unwanted side-effects; increased agitation as assessed by Barnes’ Akathisia Rating Scale;60 evidence of serotonin toxicity;45 evidence for delirium, mania or hypomania; need for commencement of mood stabiliser medication for the treatment of bipolar affective disorder or schizoaffective disorder; major neurological illness such as stroke, significant traumatic brain injury and request by an external medical practitioner to break the code on medical grounds.
The Participant Information Sheet contains instructions regarding the cessation of protocol treatment, which is also verbally explained by research clinicians. At discontinuation, the participant is advised to take half a tablet per day for 7 days from their medication pack, regardless of their study arm. Participants withdrawn from the study for medical reasons are offered a follow-up visit with the study psychiatrist. If they decline, the research clinicians advise the participant’s general practitioner of the discontinuation.
Ethics and dissemination
Ethics approval
The study has been approved by these independent ethics committees: UNSW Human Research Ethics Committee (HREC) (HC11390, HC17771), Aboriginal Health & Medical Research Council HREC (822/11) and Corrective Services NSW HREC (09/26576). NSW Justice Health and Forensic Mental Health Network HREC (G8/14) approval allows participants to continue on the study while incarcerated. The relevant parties will be notified of any amendments to the study protocol. Ethics approval will be obtained if and when necessary.
Dissemination
On completion of the trial, the results will be written up for publication in peer-reviewed medical journals. We will also provide feedback to stakeholders via presentations and reports in industry publications such as the Aboriginal and Islander Health Worker Journal.
Supplementary Material
Footnotes
Contributors: TB, PWS, LK, VC, RJS, LG, JJ, AE, DW, KW, AJ, AC, SA, PBM, DC, CD and DV conceived and designed the study and/or acquired the funding. TB, PWS, LK, DG, VC, RJS, LG, AE, DW, KW, AJ and PBM obtained ethics approval. ACK and VG developed and manage the randomisation and data management software for the trial. RJS is responsible for overseeing the genetic component of the study. TB, PWS, BT, LK, RJS, DG, VC, LG, AE, ACK, VG, JJ, DW, KW, AJ, AC and DC drafted and revised the manuscript. TB, PWS, VG, ACK and BT will analyse and interpret the data. All authors read and approved the final manuscript.
Funding: Initial funding was provided from an Australian National Health and Medical Research Council partnership grant in 2009 (NHMRC; No. 533559). From 2018, subsequent funding has been provided by the NSW Department of Communities and Justice.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Ethics statements
Patient consent for publication
Not required.
References
- 1.World Health Organization . World report on violence and health. Geneva, 2002. https://www.who.int/violence_injury_prevention/violence/world_report/en/summary_en.pdfdoi:https://www.who.int/violence_injury_prevention/violence/world_report/en/summary_en.pdf [Google Scholar]
- 2.Australian Institute of Criminology . Australian crime: facts and figures 2011. Canberra, 2012. https://aic.gov.au/publications/facts/2011 [Google Scholar]
- 3.Heilbrun AB. Psychopathy and violent crime. J Consult Clin Psychol 1979;47:509–16. 10.1037/0022-006X.47.3.509 [DOI] [PubMed] [Google Scholar]
- 4.ABS . Personal safety, Australia, 2016. Canberra: ABS, 2017. [Google Scholar]
- 5.NSW Government . Reducing domestic violence reoffending 2018, 2018. Available: https://www.nsw.gov.au/improving-nsw/premiers-priorities-2015-2019/reducing-domestic-violence-reoffending/ [Accessed Jul 2019].
- 6.International Society for Research on Impulsivity . What is impulsivity? Available: http://www.impulsivity.org/about-us [Accessed cited May 2021].
- 7.Horvath P, Zuckerman M. Sensation seeking, risk appraisal, and risky behavior. Pers Individ Dif 1993;14:41–52. 10.1016/0191-8869(93)90173-Z [DOI] [Google Scholar]
- 8.Krueger RF, Schmutte PS, Caspi A, et al. Personality traits are linked to crime among men and women: evidence from a birth cohort. J Abnorm Psychol 1994;103:328–38. 10.1037/0021-843X.103.2.328 [DOI] [PubMed] [Google Scholar]
- 9.Zamble E, Quinsey VL. Dynamic and behavioral antecedents to recidivism: a retrospective analysis. Report No. 17. Ottawa: Correctional Services Canada, Research Branch, 1991. [Google Scholar]
- 10.Heilbrun AB, Heilbrun LC, Heilbrun KL. Impulsive and premeditated homicide: an analysis of subsequent parole risk of the murderer. J Crim Law Criminol 1978;69:108. 10.2307/1142500 [DOI] [Google Scholar]
- 11.Krakowski M. Violence and serotonin: influence of impulse control, affect regulation, and social functioning. J Neuropsychiatry Clin Neurosci 2003;15:294–305. 10.1176/jnp.15.3.294 [DOI] [PubMed] [Google Scholar]
- 12.Higley JD, Mehlman PT, Higley SB, et al. Excessive mortality in young free-ranging male nonhuman primates with low cerebrospinal fluid 5-hydroxyindoleacetic acid concentrations. Arch Gen Psychiatry 1996;53:537–43. 10.1001/archpsyc.1996.01830060083011 [DOI] [PubMed] [Google Scholar]
- 13.Brown GL, Goodwin FK, Ballenger JC, et al. Aggression in humans correlates with cerebrospinal fluid amine metabolites. Psychiatry Res 1979;1:131–9. 10.1016/0165-1781(79)90053-2 [DOI] [PubMed] [Google Scholar]
- 14.Stanley B, et al. Association of aggressive behavior with altered serotonergic function in patients who are not suicidal. Am J Psychiatry 2000;157:609–14. 10.1176/appi.ajp.157.4.609 [DOI] [PubMed] [Google Scholar]
- 15.Linnoila M, Virkkunen M, Scheinin M, et al. Low cerebrospinal fluid 5-hydroxyindoleacetic acid concentration differentiates impulsive from nonimpulsive violent behavior. Life Sci 1983;33:2609–14. 10.1016/0024-3205(83)90344-2 [DOI] [PubMed] [Google Scholar]
- 16.Baron RA, Richardson DR. Perspectives in social psychology. In: Human aggression. 2nd Edn. Plenum Press, 1994. [Google Scholar]
- 17.Darby RR, Horn A, Cushman F, et al. Lesion network localization of criminal behavior. Proc Natl Acad Sci U.S.A. 2018;115:601–6. 10.1073/pnas.1706587115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Anderson SW, Bechara A, Damasio H, et al. Impairment of social and moral behavior related to early damage in human prefrontal cortex. Nat Neurosci 1999;2:1032–7. 10.1038/14833 [DOI] [PubMed] [Google Scholar]
- 19.Tateno A, Jorge RE, Robinson RG. Clinical correlates of aggressive behavior after traumatic brain injury. J Neuropsychiatry Clin Neurosci 2003;15:155–60. 10.1176/jnp.15.2.155 [DOI] [PubMed] [Google Scholar]
- 20.Salzman C, Wolfson AN, Schatzberg A, et al. Effect of fluoxetine on anger in symptomatic volunteers with borderline personality disorder. J Clin Psychopharmacol 1995;15:23–9. 10.1097/00004714-199502000-00005 [DOI] [PubMed] [Google Scholar]
- 21.Reist C, Nakamura K, Sagart E, et al. Impulsive aggressive behavior: open-label treatment with citalopram. J Clin Psychiatry 2003;64:81–5. [PubMed] [Google Scholar]
- 22.Janowsky DS, Shetty M, Barnhill J, et al. Serotonergic antidepressant effects on aggressive, self-injurious and destructive/disruptive behaviours in intellectually disabled adults: a retrospective, open-label, naturalistic trial. Int J Neuropsychopharmacol 1999;8:37–48. 10.1017/S146114570400481X [DOI] [PubMed] [Google Scholar]
- 23.Fava M, Vuolo RD, Wright EC, et al. Fenfluramine challenge in unipolar depression with and without anger attacks. Psychiatry Res 2000;94:9–18. 10.1016/S0165-1781(00)00120-7 [DOI] [PubMed] [Google Scholar]
- 24.Coccaro EF, Lee RJ, Kavoussi RJ. A double-blind, randomized, placebo-controlled trial of fluoxetine in patients with intermittent explosive disorder. J Clin Psychiatry 2009;70:653–62. 10.4088/JCP.08m04150 [DOI] [PubMed] [Google Scholar]
- 25.Cherek DR, Lane SD, Pietras CJ, et al. Effects of chronic paroxetine administration on measures of aggressive and impulsive responses of adult males with a history of conduct disorder. Psychopharmacology 2002;159:266–74. 10.1007/s002130100915 [DOI] [PubMed] [Google Scholar]
- 26.Silva H, Iturra P, Solari A, et al. Fluoxetine response in impulsive-aggressive behavior and serotonin transporter polymorphism in personality disorder. Psychiatr Genet 2010;20:25–30. 10.1097/YPG.0b013e328335125d [DOI] [PubMed] [Google Scholar]
- 27.Yue JK, Burke JF, Upadhyayula PS, et al. Selective serotonin reuptake inhibitors for treating neurocognitive and neuropsychiatric disorders following traumatic brain injury: an evaluation of current evidence. Brain Sci 2017;7. 10.3390/brainsci7080093. [Epub ahead of print: 25 07 2017]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Smits KM, Smits LJM, Schouten JSAG. Influence of SERTPR and STin2 in the serotonin transporter gene on the effect of selective serotonin reuptake inhibitors in depression: a systematic review. Mol Psychiatry 2004;9:433–41. 10.1038/sj.mp.4001488 [DOI] [PubMed] [Google Scholar]
- 29.Smeraldi E, Zanardi R, Benedetti F, et al. Polymorphism within the promoter of the serotonin transporter gene and antidepressant efficacy of fluvoxamine. Mol Psychiatry 1998;3:508–11. 10.1038/sj.mp.4000425 [DOI] [PubMed] [Google Scholar]
- 30.Stein MB, Seedat S, Gelernter J. Serotonin transporter gene promoter polymorphism predicts SSRI response in generalised anxiety disorder. Psychopharmacology 2006;197:68–72. 10.1007/s00213-006-0349-8 [DOI] [PubMed] [Google Scholar]
- 31.Probst-Schendzielorz K, Viviani R, Stingl JC. Effect of cytochrome P450 polymorphism on the action and metabolism of selective serotonin reuptake inhibitors. Expert Opin Drug Metab Toxicol 2015;11:1219–32. 10.1517/17425255.2015.1052791 [DOI] [PubMed] [Google Scholar]
- 32.National Institute of Clinical Excellence . Antisocial personality disorder: treatment, management and prevention. National clinical practice guideline number 77. British Psychological Society and Royal College of Psychiatrists, 2010. [PubMed] [Google Scholar]
- 33.Butler T, Schofield PW, Greenberg D, et al. Reducing impulsivity in repeat violent offenders: an open label trial of a selective serotonin reuptake inhibitor. Aust N Z J Psychiatry 2010;44:1137–43. 10.3109/00048674.2010.525216 [DOI] [PubMed] [Google Scholar]
- 34.MIMS Australia . SETRONA, 2011. Available: https://www.mydr.com.au/medicines/setrona-tablets [Accessed Aug 2019].
- 35.Australian Bureau of Statistics . Australian and New Zealand standard offence classification (ANZSOC). 3rd Edn. Canberra, Australia, 2011. [Google Scholar]
- 36.Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. Journal of Clinical Psychology 1995;51:768–74. [DOI] [PubMed] [Google Scholar]
- 37.Spielberger CD. State-trait anger expression inventory- 2 professional manual. In: Psychological assessment resources. Odessa: FL, 1999. [Google Scholar]
- 38.Coccaro EF, Harvey PD, Kupsaw-Lawrence E, et al. Development of neuropharmacologically based behavioral assessments of impulsive aggressive behavior. J Neuropsychiatry Clin Neurosci 1991;3:S44–51. 10.1001/archpsyc.1997.01830240035005 [DOI] [PubMed] [Google Scholar]
- 39.Ware JE, Kosinski M, Keller SD. SF-12: how to score the SF-12 physical and mental health summary scales. 3rd Edn. Quality Metric: Lincoln RI, 1998. [Google Scholar]
- 40.Koenig HG, Westlund RE, George LK, et al. Abbreviating the duke social support index for use in chronically ill elderly individuals. Psychosomatics 1993;34:61–9. 10.1016/S0033-3182(93)71928-3 [DOI] [PubMed] [Google Scholar]
- 41.Butler T, Milner L. The 2001 New South Wales inmate health survey. Sydney: Corrections Health Service, 2003. [Google Scholar]
- 42.Saunders JB, Aasland OG, Babor TF, et al. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption. Addiction 1993;88: :791–804. 10.1111/j.1360-0443.1993.tb02093.x [DOI] [PubMed] [Google Scholar]
- 43.Beck A, Steer R, Brown G. Beck depression inventory-II. San Antonio, TX: The Psychological Corporation, 1996. [Google Scholar]
- 44.Kessler RC, Barker PR, Colpe LJ, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry 2003;60:184–9. 10.1001/archpsyc.60.2.184 [DOI] [PubMed] [Google Scholar]
- 45.Dunkley EJC, Isbister GK, Sibbritt D, et al. The Hunter serotonin toxicity criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM 2003;96:635–42. 10.1093/qjmed/hcg109 [DOI] [PubMed] [Google Scholar]
- 46.Stanford MS, Mathias CW, Dougherty DM, et al. Fifty years of the Barratt impulsiveness scale: an update and review. Pers Individ Dif 2009;47:385–95. 10.1016/j.paid.2009.04.008 [DOI] [Google Scholar]
- 47. Isohelix. GeneFIX saliva collection brochure. Available: https://isohelix.com/wp-content/uploads/2018/03/GeneFiX-Saliva-Collection-Brochure.pdf [Accessed Sep 2019].
- 48.The National Health and Medical Research Council, the Australian Research Council and Universities Australia . National statement on ethical conduct in human research. Canberra: Commonwealth of Australia, 2007. [Google Scholar]
- 49.Andrews DA, Bonta JL. The utility of level of service inventory - revised. Toronto, Canada: Multi-Health Systems, 1995. [Google Scholar]
- 50.Settumba SN, Chambers GM, Shanahan M, et al. Are we getting value for money from behavioral interventions for offenders? A research note reviewing the economic evaluation literature. Am J Crim Justice 2018;43:411–31. 10.1007/s12103-017-9399-1 [DOI] [Google Scholar]
- 51.Settumba SN, Shanahan M, Butler T, et al. Developing attributes and attribute-levels for a discrete-choice experiment: an example for interventions of impulsive violent offenders. Appl Health Econ Health Policy 2019;17:683–705. 10.1007/s40258-019-00484-5 [DOI] [PubMed] [Google Scholar]
- 52.Settumba SN, Shanahan M, Chambers GM, et al. Assessing societal and offender perspectives on the value of offender healthcare: a stated preference research protocol. BMJ Open 2019;9:e024899. 10.1136/bmjopen-2018-024899 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Schofield PW, Xu A, Simpson P, et al. Pharmacotherapy to reduce violent offending? Offenders might be interested. Aust N Z J Psychiatry 2019;53:697–8. 10.1177/0004867419835937 [DOI] [PubMed] [Google Scholar]
- 54.Justice NSW . ReINVEST: reducing impulsivity in repeat violent offenders, 2018. Available: https://www.youtube.com/watch?v=jcA8iJ-43xo&t=4s
- 55.Brochu S, Cournoyer L-G, Tremblay J, et al. Understanding treatment impact on drug-addicted offenders. Subst Use Misuse 2006;41:1937–49. 10.1080/10826080601025995 [DOI] [PubMed] [Google Scholar]
- 56.DeVall KE, Lanier CL. Successful completion: an examination of factors influencing drug court completion for white and non-white male participants. Subst Use Misuse 2012;47:1106–16. 10.3109/10826084.2012.680171 [DOI] [PubMed] [Google Scholar]
- 57.Fujii DE, Ahmed I, Jokumsen M, et al. The effects of clozapine on cognitive functioning in treatment-resistant schizophrenic patients. J Neuropsychiatry Clin Neurosci 1997;9:240–5. 10.1176/jnp.9.2.240 [DOI] [PubMed] [Google Scholar]
- 58.Goshin LS, Byrne MW. Predictors of post-release research retention and subsequent reenrollment for women recruited while incarcerated. Res Nurs Health 2012;35:94–104. 10.1002/nur.21451 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Gilman AB, Hill KG, Kim BKE, et al. Understanding the relationship between self-reported offending and official criminal charges across early adulthood. Crim Behav Ment Health 2014;24:229–40. 10.1002/cbm.1934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry 1989;154: :672–6. 10.1192/bjp.154.5.672 [DOI] [PubMed] [Google Scholar]
- 61.Weschler D. WAIS-R manual. New York: The Psychological Corporation, 1981. [Google Scholar]
- 62.Sheehan D, et al. Reliability and validity of the M.I.N.I. international neuropsychiatric interview (M.I.N.I.): according to the SCID-P. European Psychiatry 1997;12:232–41. 10.1016/S0924-9338(97)83297-X [DOI] [Google Scholar]
- 63.Loranger AW, Janca A, Sartorius N. Assessment and diagnosis of personality disorders. The ICD-10 international personality disorder examination (IPDE). Cambridge: Cambridge University Press, 1997. [Google Scholar]
- 64.Eysenck SB, McGurk BJ. Impulsiveness and venturesomeness in a detention center population. Psychol Rep 1980;47:1299–306. 10.2466/pr0.1980.47.3f.1299 [DOI] [PubMed] [Google Scholar]
- 65.Hummel T, Kobal G, Gudziol H, et al. Normative data for the "Sniffin' Sticks" including tests of odor identification, odor discrimination, and olfactory thresholds: an upgrade based on a group of more than 3,000 subjects. Eur Arch Otorhinolaryngol 2007;264:237–43. 10.1007/s00405-006-0173-0 [DOI] [PubMed] [Google Scholar]
- 66.NSW Crimes Act (1900), in s316. New South Wales, Australia: 1900. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2020-044656supp001.pdf (96.9KB, pdf)
bmjopen-2020-044656supp002.pdf (130.7KB, pdf)