

Abstract
Expanding hypertension services in low- and middle-income countries requires efficient and effective service delivery approaches that meet the needs and expectations of people living with hypertension within the resource constraints of existing national health systems. Ideally, a hypertension program will extend treatment coverage while maintaining service quality, maximizing efficient resource utilization and improving clinical outcomes. In this article, we discuss lessons learned from HIV differentiated service delivery initiatives, and make the case that the same approach should be adopted for hypertension programs.
Keywords: Hypertension, health systems, health policy, HIV/AIDS, chronic disease
Background
Hypertension is the leading single cause of cardiovascular disease (CVD) worldwide, responsible for more deaths than all infectious diseases combined in the pre-COVID era [1,2]. Globally, hypertension prevalence is growing most rapidly in low- and middle-income countries (LMICs) [3], reflecting aging populations and a rising risk factor prevalence. Approximately 17.5% of adults in LMICs are living with hypertension, of whom only 39% have had their hypertension diagnosed, just 29% are being treated, and a mere 10% have well-controlled blood pressure (BP) [4].
Controlling hypertension is a public health priority, but health systems in many LMIC are not on track to reach the World Health Organization (WHO) goal of 25% reduction in raised BP by 2025 [5]. In order to achieve global and national targets, a new approach is required that delivers efficient and effective hypertension services at scale in resource-constrained settings.
We propose that key lessons can be learned from a service delivery approach used for HIV, another chronic condition [6]. Both hypertension and HIV require primary prevention services, screening and diagnosis, linkage to care, lifelong behavioral and biomedical interventions, ongoing clinical and laboratory monitoring, and support for long-term medication adherence [7]. Yet the scale-up of HIV services has been considerably more effective, with 81% of people living with HIV (PLHIV) aware of their diagnosis, 67% on treatment, and 59% achieving viral suppression [8]. In addition to robust funding and political commitment, HIV programs have benefited from innovative service delivery models that can be adapted for other chronic conditions [9].
At the heart of successful HIV scale-up is a public health approach, including the use of simplified treatment algorithms that enable standardized national training programs, task sharing among health care workers, decentralized clinical and laboratory services largely delivered at the primary care level, streamlined procurement of drugs and commodities, and consistent monitoring and evaluation processes [10]. More recently, the public health approach to HIV programming has adopted the principles of differentiated service delivery (DSD), a strategy in which service delivery models are tailored for different groups of PLHIV according to their clinical characteristics, specific population type and context. The goal of DSD is to increase service coverage, quality and efficiency, provide person-centred care, and improve outcomes, within the context of resource and health system limitations [11].
While initially developed in the context of HIV, DSD was conceptualized from the start to apply to any chronic disease, including hypertension [12,13,14]. In this article, we make the case for applying the DSD model to hypertension services and outline the steps required to implement this strategy.
DSD: Lessons from HIV and the case for extending them to hypertension
DSD is a patient-centered approach that simplifies and adapts health services to reflect the preferences and expectations of recipients of care, while reducing unnecessary burdens on patients and the health system [15]. DSD focuses less on the ‘what’ of service delivery and more on the ‘how’ – specifically on how to optimize the delivery of clinical, laboratory, pharmacy and psychosocial support services using four building blocks: [15] where (service location), when (service frequency and time), who (health worker cadres), and what (the package of services). For example, services for people established on HIV treatment are designed to maximize both choice and efficiency, with less frequent clinical and pharmacy visits and services delivered either at health facilities or in the community by a wide range of health workers, including peers and/or lay health workers. In contrast, services for people with more complex or advanced disease may be delivered primarily at health facilities, with more frequent visits, by more highly trained healthcare workers. Figure 1 depicts illustrative DSD models widely used for individuals established on HIV treatment.
Figure 1.
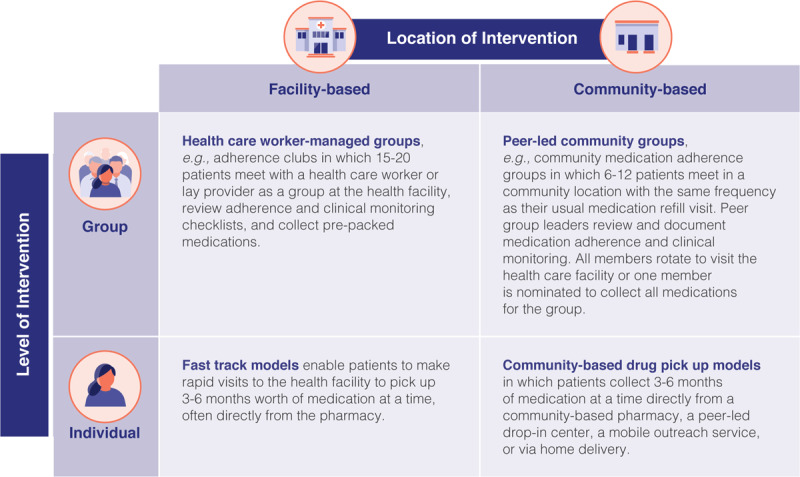
Illustrative DSD models for people doing well on treatment.
A growing body of evidence supports the effectiveness of DSD for improving HIV cascade outcomes while controlling or reducing cost [11,16,17]. DSD also promoted health system and patient resilience during the COVID-19 pandemic: [18,19] efficiency, decentralization of services, and streamlined interactions with the health system were ever more critical when travel was curtailed, clinics were closed, and financial and human resources were shifted away from chronic disease services [20].
The hypertension cascade data make it clear that the status quo service delivery models are not serving the needs of people living with hypertension. The capacity of the primary health care system to manage chronic care of any kind is limited in most LMICs, limiting access to diagnostic and treatment services and defeating efforts to control many non-communicable diseases. Considering the even larger cohort of patients in need of hypertension care, pivoting to a public health approach, and more specifically to a DSD strategy, may enable countries to leverage lessons from HIV programs to improve hypertension diagnosis, linkage to treatment, and control of blood pressure at scale.
DSD for hypertension: What would it take?
In theory, DSD models developed for ART delivery and described in Figure 1 should translate well to hypertension and may address several of the critical barriers to the scale-up of hypertension services in LMICs [21,22]. Less-intensive models that de-link medication dispensing from clinical examination for people established on treatment are more convenient for people with hypertension and more efficient for overburdened health facility staff. Enabling task-shifting to non-physician clinicians and laypeople can expand the geographic coverage and reach of hypertension services.
There is an emerging body of evidence for the use of differentiated hypertension models. For example, DSD models have been designed for people with both HIV and hypertension in Eswatini, using a facility-based group model [23]. A pilot project in Kenya also used a facility-based group model for PLHIV and for people with hypertension and diabetes and found the model feasible, efficacious, and acceptable to both patients and healthcare workers [24,25]. A pilot of hypertension adherence and treatment clubs in Nigeria is underway [26], and a multicomponent intervention focused on home visits by community health workers (CHWs) has already demonstrated significant improvement in hypertension control in rural communities across several South Asian countries in a randomized controlled trial [27]. But what will it take to deliver DSD-for-hypertension at scale?
Moving a new model to scale requires supportive government policies and guidelines along with champions on both the ‘supply side’ (the health system) and the ‘demand side’ (recipients of care and communities). And while DSD models can be more efficient than standard models, achieving broad scale coverage will nonetheless require increased funding for hypertension services. Figure 2 lays out key steps necessary to adopt DSD for hypertension.
Figure 2.

Key Steps Necessary for DSD in Hypertension.
* Organized into WHO health systems building blocks [35].
An assessment of current policies can help countries understand the present policy environment, and the changes necessary to enable DSD approaches to care. Existing global hypertension programs, such as those of WHO-HEARTS and Resolve to Save Lives, an initiative of Vital Strategies, already involve many of these components and may be able to provide technical support for incorporating DSD and its health systems framework [28,29,30].
Countries and health systems preparing to commit to DSD must also make the policy and business case for this approach. In some cases, more evidence is needed to do so. How are we to gather this evidence?
First, standardized targets, indicators and monitoring and evaluation (M&E) frameworks are essential. The UNAIDS 95-95-95 goals for HIV urge each country to ensure that 95% of people living with HIV know their HIV status [31], 95% of those individuals receive ART, and 95% of those on ART achieve sustained viral suppression. Similar bold and defined targets can be developed for the hypertension care cascade, which can help drive and refine innovative models of care, such as DSD. Clear indicators to define the number of people diagnosed with HTN, linked to treatment, retained in care, and achieving BP control must be part of the implementation of DSD models for HTN. When paired with quality improvement responses, ongoing impact assessments can accompany implementation and scale-up and identify the challenges to meeting these targets that will inevitably arise [32].
The design of additional studies will depend on evidence gaps identified. These can include mixed methods implementation studies to document quality, coverage, impact, and acceptability, qualitative explorations of user and health care worker experiences, time-motion studies to estimate health workforce need and to identify areas for increasing efficiencies, and costing and economic analyses, including mathematical models to assess cost-effectiveness or help in budget planning [33,34].
Conclusion
The epidemic of hypertension in LMICs demands immediate action to slow and reverse the growing burden of cardiovascular disease. However, interventions must take a public health approach, and be tailored both to health system capacity and to the needs of people with hypertension. Adopting a DSD approach for hypertension has the potential to expand treatment coverage, improve BP control, maintain or improve quality of care, and make the most of limited health care resources.
Ethics and Consent
Ethics Committee approval was not sought as this manuscript does not involve original data or human subjects research.
Funding Information
No third-party funding sources were involved in the writing of this manuscript or the decision to submit it for publication.
No original data was used in the preparation of this manuscript; however, all authors had full access to the final manuscript text.
All authors accept responsibility to submit for publication.
Competing Interests
Dr. Tisdale has no competing interests to disclose.
Ms. Cazabon has no competing interests to disclose.
Dr. Moran reports personal fees from Resolve to Save Lives, an initiative of Vital Strategies, during the conduct of the study.
Dr. Rabkin has no competing interests to disclose.
Dr. Bygrave has no competing interests to disclose.
Dr. Cohn has no competing interests to disclose.
Author Contributions
Rebecca Tisdale: literature search, figures, writing – original draft, writing – review and editing.
Danielle Cazabon: writing – original draft, writing – review and editing.
Andrew E. Moran: conceptualisation, supervision, writing – original draft, writing – review and editing.
Miriam Rabkin: writing – review and editing.
Helen Bygrave: writing – review and editing.
Jennifer Cohn: conceptualisation, supervision.
References
- 1.Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 10November 2018; 392(10159): 1736–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 10November2018; 392(10159): 1923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: A systematic analysis of population-based studies from 90 countries. Circulation. 9August2016; 134(6): 441–50. DOI: 10.1161/CIRCULATIONAHA.115.018912 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Geldsetzer P, Manne-Goehler J, Marcus ME, et al. The state of hypertension care in 44 low-income and middle-income countries: A cross-sectional study of nationally representative individual-level data from 1.1 million adults. Lancet. 2019; 394: 652–662. DOI: 10.1016/S0140-6736(19)30955-9 [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization (WHO). Set of 9 voluntary NCD targets for 2025. (2011). https://www.who.int/nmh/global_monitoring_framework/gmf1_large.jpg?ua=1 (accessed 8 September 2020).
- 6.Rabkin M, El-Sadr W. Why reinvent the wheel? Leveraging the lessons of HIV scale-up to confront non-communicable diseases. Global Public Health. 2011; 6(3): 247–56. DOI: 10.1080/17441692.2011.552068 [DOI] [PubMed] [Google Scholar]
- 7.Geldsetzer P, Ortblad K, Bärnighausen T. The efficiency of chronic disease care in sub-Saharan Africa. BMC Med. December2016; 14(1): 1–4. DOI: 10.1186/s12916-016-0675-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.UNAIDS. Seizing the moment: Tackling entrenched inequalities to end epidemics: Global AIDS Update 2020; 2020. https://www.unaids.org/sites/default/files/media_asset/2020_global-aids-report_en.pdf (accessed 30 July 2020).
- 9.Palma AM, Rabkin M, Nuwagaba-Biribonwoha H, et al. Can the success of HIV scale-up advance the global chronic NCD agenda? Global Heart. 2016; 11(4). DOI: 10.1016/j.gheart.2016.10.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ford N, Ball A, Baggaley R, et al. The WHO public health approach to HIV treatment and care: Looking back and looking ahead. Lancet Infect Dis. 2018; 18: e76–e86. DOI: 10.1016/S1473-3099(17)30482-6 [DOI] [PubMed] [Google Scholar]
- 11.Ehrenkranz P, Grimsrud A, Rabkin M. Differentiated service delivery: Navigating the path to scale. Curr Opin HIV/AIDS. January2019; 14(1): 60–65. DOI: 10.1097/COH.0000000000000509 [DOI] [PubMed] [Google Scholar]
- 12.Rabkin M, Nishtar S. Scaling up chronic care systems: Leveraging HIV programs to support non-communicable disease services. J Acquire Immune Defic Syndr. 2011; 57: S87–90. DOI: 10.1097/QAI.0b013e31821db92a [DOI] [PubMed] [Google Scholar]
- 13.Rabkin M, Kruk ME, El-Sadr WM. HIV, aging and continuity care: Strengthening health systems to support services for noncommunicable diseases in low-income countries. AIDS. 2012; 26(Suppl 1): S77–83. DOI: 10.1097/QAD.0b013e3283558430 [DOI] [PubMed] [Google Scholar]
- 14.El-Sadr WM, Harripersaud K, Rabkin M. Reaching global HIV/AIDS goals: What got us here, won’t get us there. PLoS Med. 2017; 14(11): e1002421. DOI: 10.1371/journal.pmed.1002421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.International AIDS Society. Differentiated care for HIV: A decision framework for antiretroviral therapy delivery. (2016). https://www.differentiatedcare.org/Portals/0/adam/Content/yS6M-GKB5EWs_uTBHk1C1Q/File/Decision%20Framework.pdf. (accessed 16 July 2020).
- 16.Roberts DA, Tan N, Limaye N, Irungu E, Barnabas RV. Cost of differentiated HIV antiretroviral therapy delivery strategies in sub-Saharan Africa: A systematic review. J Acquire Immune Defic Syndr. 1December2019; 82: S339–47. DOI: 10.1097/QAI.0000000000002195 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Barker C, Dutta A, Klein K. Can differentiated care models solve the crisis in HIV treatment financing? Analysis of prospects for 38 countries in sub-Saharan Africa. J Int AIDS Soc. 2017; 20(Suppl 4): 21648. DOI: 10.7448/IAS.20.5.21648 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wilkinson L, Grimsrud A. The time is now: Expedited HIV differentiated service delivery during the COVID-19 pandemic. J Int AIDS Soc. May2020; 23(5): e25503. DOI: 10.1002/jia2.25503 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Golin R, Godfrey C, Firth J, et al. PEPFAR’s Response to the Convergence of the HIV and COVID-19 Pandemics in Sub-Saharan Africa. J Int AIDS Soc. August2020; 23(8): e25587. DOI: 10.1002/jia2.25587 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.World Health Organization (WHO). ‘Community drug distribution at doorsteps: Essential health services decentralized to care for hypertensives under the IHCI initiative.’ (22 July 2020). https://www.who.int/india/news/feature-stories/detail/community-drug-distribution-at-doorsteps-essential-health-services-decentralized-to-care-for-hypertensives-under-the-ihci-initiative (accessed 5 August 2020).
- 21.Bygrave H, Golob L, Wilkinson L, Roberts T, Grimsrud A. Let’s talk chronic disease: Can differentiated service delivery address the syndemics of HIV, hypertension and diabetes? Curr Opin HIV/AIDS. 1July2020; 15(4): 256–60. DOI: 10.1097/COH.0000000000000629 [DOI] [PubMed] [Google Scholar]
- 22.Kwon C, Webster R, Santo K, Atkins E. Community Group-Based Models of Medication Delivery: Applicability to Cardiovascular Diseases. Glob Heart. 5May2021; 16(1): 36. DOI: 10.5334/gh.763 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kambale H. ‘DSD Models for HIV/NCD Integration.’ Presentation to HIV Learning Network: The CQUIN Project for Differentiated Service Delivery, ICAP-Columbia University Mailman School of Public Health. (29July2020). https://cquin.icap.columbia.edu/wp-content/uploads/2020/07/6c.-DSDM-for-HIV-NCDs-integration-in-Eswatini_draft.pdf (accessed 4 June 2021).
- 24.Khabala KB, Edwards JK, Baruani B, et al. Medication Adherence Clubs: A potential solution to managing large numbers of stable patients with multiple chronic diseases in informal settlements. Trop Med Int Health. 2015; 20(10): 1265–1270. DOI: 10.1111/tmi.12539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Venables E, Edwards JK, Baert S, Etienne W, Khabala K, Bygrave H. ‘They just come, pick and go.’ The acceptability of integrated medication adherence clubs for HIV and non communicable disease (NCD) patients in Kibera, Kenya. PLoS One. 2016; 11(10): e0164634. DOI: 10.1371/journal.pone.0164634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Santo K, Isiguzo GC, Atkins E, et al. Adapting a club-based medication & delivery strategy to a hypertension context: The CLUBMEDS Study in Nigeria. BMJ Open. 2019; 9: e029824. DOI: 10.1136/bmjopen-2019-029824 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jafar TH, Gandhi M, De Silva HA, et al. A community-based intervention for managing hypertension in rural South Asia. NEJM. 20February2020; 382(8): 717–26. DOI: 10.1056/NEJMoa1911965 [DOI] [PubMed] [Google Scholar]
- 28.World Health Organization. Hearts: technical package for cardiovascular disease management in primary health care. (2016). http://apps.who.int/iris/bitstream/10665/252661/1/9789241511377-eng.pdf?ua=1. (accessed 31 July 2020).
- 29.Resolve to Save Lives. Hypertension fact sheet. https://resolvetosavelives.org/assets/Resources/Resolve-to-Save-Lives-Hypertension-Fact-Sheet.pdf. (accessed 31 July 2020).
- 30.Frieden TR, Varghese CV, Kishore SP, et al. Scaling up effective treatment of hypertension—A pathfinder for universal health coverage. J Clin Hypertens. 2019; 21: 1442–9. DOI: 10.1111/jch.13655 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.UNAIDS. Fast-Track: ending the AIDS epidemic by 2030. (2014). https://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014report_en.pdf (accessed 4 June 2021).
- 32.Grimsrud A, Bygrave H, Doherty M, et al. Reimagining HIV service delivery: The role of differentiated care from prevention to suppression. J Int AIDS Soc. 2016; 19: 21484. DOI: 10.7448/IAS.19.1.21484 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Dowdy DW, Powers KA, Hallett TB. Towards evidence-based integration of services for HIV, non-communicable diseases and substance use: Insights from modelling. J Int AIDS Soc. June2020; 23(S1): e25525. DOI: 10.1002/jia2.25525 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kibachio J, Mwenda V, Ombiro O, et al. Recommendations for the use of mathematical modelling to support decision-making on integration of non-communicable diseases into HIV care. J Int AIDS Soc. 2020; 23(S1): e25505. DOI: 10.1002/jia2.25505 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.World Health Organization (WHO). Monitoring the building blocks of health systems: A handbook of indicators and their measurement strategies. (2010). https://www.who.int/healthinfo/systems/WHO_MBHSS_2010_full_web.pdf?ua=1 (accessed 4 August 2020).