

Abstract
Background:
Shalakya Tantra is one of the eight branches of Ayurveda, which also includes ophthalmology. Shushkakshipaka (dry eye syndrome) is one of the diseases, involving all parts of eye (Sarvagata Netra Roga) characterized by Gharsha (gritty feeling), Toda (pricking type of pain), Kunita (photophobia), Avila Darshana (blurred vision), Daha (burning sensation) and Raktaraji (congestion in the eye). All these symptoms are similar to the symptoms of dry eye syndrome.
Aims and objective:
The objective of the present study was to evaluate and compare the effect of Triphala Ghrita and Goghrita Manda (supernant liquid part of cow ghee) Tarpana (therapeutic procedure done on the eye) in the management of Shushkakshipaka.
Materials and methods:
Thirty patients fulfilling the inclusion criteria of Shushkakshipaka were selected from the outpatient department and inpatient department of Shalakya Tantra, Sri Dharmasthala Manjunatheshwara College of Ayurveda, Hassan. Clinical signs and symptoms were given suitable scores according to their severity, and assessment was based on the relief in these symptoms after the treatment. Patients of dry eye syndrome were allocated alternatively in two groups for Tarpana, namely Triphala Ghrita Tarpana (TGT) group and Goghrita Manda Tarpana (GMT) group and Tarpana was given for 7 consecutive days in afternoon with follow up after 15 days for 2 months.
Results:
Moderate relief (50%–75% relief) was seen in 73.3% of the patients in both the groups, while marked relief (>75% but <100% relief) was seen in 26.7 patients in both the groups. Relief in symptoms like Gharsha (74%), Avila Darshana (65%), Upadeha (80%), Daha (72%), Kunita (78%), Toda (59%) and Raktaraji (83%) was obtained.
Conclusion:
The effect of Goghrita Manda Tarpana (GMT) on Garsha, Toda and Daha was better in immediately after treatment than Triphala Ghrita Tarpana (TGT).
Keywords: Ayurveda, dry eye syndrome, Goghrita Manda, Shushkakshipaka, Triphala Ghrita
Introduction
Shushkakshipaka[1] is one of the Sarvagata Netra Roga[2] mentioned by Sushruta as well as Vagbhata under eye disease, caused by Vata and Pitta and characterized of Gharsha (gritty feeling), Toda (pricking type of pain), Upadeha (membrane formation), Krichronmeelan (difficulty in blinking), Vishushkata (dryness), Ruksha Daruna Vartma (rough eyelids) etc.[1] These symptoms can be correlated with the symptoms of dry eyes in modern medicine, which is a leading cause of ocular discomfort affecting millions of people.
Dry eye syndrome[3] is a spectrum of disorders ranging from mild eye strain to foreign-body sensation, pain, burning and sight-threatening complications. Patients suffer considerable discomfort due to it, which interfere with daily routine activities. The symptoms of dry eye syndrome aggravates in conditions with pollution and humidity such as in air conditioning and indoor heaters.[4] Unfortunately, despite of many researches being undertaken on dry eye syndrome, permanent cure for dry eyes is still not available nor seems closer.
Tarpana[5] is one of the important ocular therapeutic (Kriyakalpa) which nourishes the eyes and cures the Vata Pitta diseases.[6,7] It may be useful in the management of Shushkakshipaka due to its oleation (Snehana) and Vata and Pitta pacifying actions.
Triphala Ghrita and Goghrita Manda are indicated in Netra Roga (eye diseases) because of its Chakshushya (improves vision), Snehana (oleation) and Rasayana (rejuvenating) properties.[8] Triphala Ghrita contains Triphala which has been reported to have the immunomodulator, antimicrobial and anti-inflammatory activities[9] and thus may help in checking the progress of dry eye syndrome by preventing T-cells from releasing cytokines (primarily interleukin-6) that incite the inflammatory component of dry eyes.
Aim of the study
• To evaluate and compare the efficacy of Triphala Ghrita Tarpana (TGT) and Goghrita Manda Tarpana (GMT) in the management of Shushkakshipaka.
Source of data
The patients with classical signs and symptoms of Shushkaakshipaka like Gharsha, Toda and Daha in the eyes were selected as per the inclusion and exclusion criteria from the outpatient department and inpatient department of postgraduate studies in Shalakya Tantra of SDM College of Ayurveda and Hospital, Hassan
Trial Drug: Triphala Ghrita was procured form SDM Pharmacy, Udupi and Goghrita Manda was procured from the Kriyakalpa Unit of SDM College of Ayurveda and Hospital, Hassan.
Materials and methods
A prospective comparative clinical study was designed and conducted. The diagnosis was established on the basis of history and symptoms mentioned in classical texts. Approval from Institutional Ethical Committee was taken before commencing the trial. Patient information sheet was given to 30 patients and informed consent was taken from all the patients. The diagnosis was confirmed by Schirmer’s test values by level of wetting of tear strip and tear break-up time by the appearance of dry spots in tear film.[Table 1]
Table 1.
Grading of objective parameters
| Objective parameters | Observation | |||
|---|---|---|---|---|
|
| ||||
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | |
| Schirmer’s test | Level of wetting of tear strip above 15 mm in 1 min | Level of wetting of tear strip above 10 mm - 15mm in 1 min | Level of wetting of tear strip above 5 mm - 10 mm in 1 min | Level of wetting of tear strip at 1 mm - 5 mm in 1 min |
| Tear break-up time | The appearance of dry spots after 15 sec | The appearance of dry spots between 10 and 15 sec | The appearance of dry spots between 5 and 10 sec | The appearance of dry spots within 5 sec |
Statistical Tests
The demographic data has been presented in percentage. The scoring of criteria of assessment was analyzed statistically in terms of mean values of B.T. (before treatment), A.T. (after treatment), S.D. (standard deviation) and S.E. (standard error). The effect of therapy in both the groups was assessed by applying student’s paired ‘t’ test for comparing before treatment and after treatment scores of assessment criteria. The results obtained were considered highly significant for P < 0.001, significant for P < 0.05 and insignificant for P > 0.05.
Inclusion criteria
Patients aged above 5 years and below 60 years of either sexes
Patients having classical signs and symptoms of Shushkakshipaka like Gharsha (gritty feeling), Toda (pricking type of pain), Upadeha (membrane formation), Krichronmeelan (difficulty in blinking), Vishushkata (dryness), Ruksha Daruna Vartma (rough eyelids)
Eligible cases for Tarpana
Exclusion criteria
Shushkakshipaka (dry eye Syndrome) associated with other specific ocular diseases such as Savrana Shukla (corneal ulcer), Arma (pterygium).
Those contraindicated for Tarpana – Netra Ragata (redness of eye), Jwara (fever) and Pratishaya (rhinitis).
Treatment group
Thirty patients of Shushkakshipaka (dry eye syndrome) were selected by random sampling technique (convenience method) of sampling and patients were allocated alternatively into following two groups each comprising 15 patients.
Group TGT – 15 patients were subjected for Triphala Ghrita Tarpana
Group GMT – 15 patients were subjected for Goghrita Manda Tarpana.
Posology
Tarpana
For the purpose of Tarpana procedure, black lentil flour and water were mixed together to form a dough. This dough was then used to create a circular wall around the eyes. Then, the patient was asked to close the eyes and Ghrita was filled in the space inside the circular boundary. After pouring Ghrita, the patient was asked to open and close the eyes gradually. Approximately 10–15 ml of Triphala Ghrita or Gogritha Manda was used for Tarpana daily in the afternoon for consecutive 7 days for 1000 Matra Kala/30 Minutes[1,7] Patients were advised not to tilt the head and to blink the eyes intermittently. Patients were not taking any allopathic drugs or any other internal medicines during the course of the treatment.
Follow-up
The follow-up was done at an interval of every 15 days up to 60 days and reappearance of the symptoms within the follow-up period was considered as recurrence of the disease.
Assessment of Therapy
The assessment of the therapies was done on the basis of status of signs and symptoms before and after the completion of the treatment, on the basis of self-formulated scoring scale. The grading was done of objective parameters graded as per the Table 1. Gharsha (gritty feeling in the eyes), Avila Darshana (blurred vision), Upadeha (excessive stringy mucus/filmy feeling in the eyes), Daha (burning sensation in the eyes), Kunita (photophobia), Toda (pricking type of pain in the eyes) and Raktaraji (congestion in the eyes) were included in subjective parameters [Table 2]. The overall assessment was done on the basis of parameters as mentioned in Table 3.
Table 2.
Grading’s of Subjective parameters
| Symptom | Status of the symptom | |||
|---|---|---|---|---|
|
| ||||
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | |
| Gharsha (gritty feeling) | Absent | Occasionally present | Frequently present with lacrimation | Continuously present with lacrimation and congestion. |
| Avila Darshana (blurring of vision) | Absent | Occasionally present | Intermittently present | Frequently present |
| Upadeha (excessive stringy mucus/filmy feeling in the eyes) | Absent | Occasionally present and the patient is able to open the eyes easily | Frequently present and patient is able to open the eyes easily | Frequently present and patient is able to open the eyes with much difficulty |
| Daha (burning sensation in the eye) | No burning sensation in eyes | Occasional burning sensation in eyes | Regular burning sensation in eyes | ------- |
| Kunita (photophobia) | Absent | Sensitivity to bright light and other bright stimulus | Sensitivity to mild sunlight but comfortable in dim lights | Sensitivity to even dim light with an inability to open eyes |
| Toda (pricking type of pain in the eyes) | Absence of pricking pain | Mild - tolerable and negligible pricking pain | Moderate - constant and tolerable pricking pain | Severe - intolerable and constant pricking pain |
| Raktaraji (congestion) | Absent | Discrete, thin vessels vascular network limited to palpebral conjunctiva and fornix | Prominent vascular network involving peripheral part of bulbar conjunctiva | Fiery red involving whole bulbar conjunctiva and circumcorneal zone |
| Daruna and Ruksha Vartma | Absent | Occasionally present | Intermittently present | Frequently present |
Table 3.
Gradation index for overall response
| Response | Result % (Criteria of response) |
|---|---|
| No improvement | <25% relief in signs, symptoms and clinical tests |
| Mild relief | 25%.50% relief in the signs, symptoms and clinical tests |
| Moderate relief | 50%.75% relief in the signs, symptoms and clinical tests |
| Marked relief | >75% but <100% relief in the signs symptoms and clinical tests |
| Complete relief | 100% relief in the signs, symptoms and clinical tests |
Observation
Age wise distribution of patients showed that maximum 46% of the patients were in the age group of 21 – 35 years, followed by 27% patients who were in the age group of 5 -20 years, 17% were in the age group of 51-75 years and 10% were between the age group of 36-50 yrs. Out of 30 cases, incidence of Shushkakshipaka was observed 60% in female and 40% in male patients. Socio-economic status wise distribution of patients showed that maximum of 73% belonged to middle class followed by 23% patients who belonged to upper class and 04% belonged to lower class. Prakriti wise distribution showed that 63% were of Vata-Pittaja, 27% were of Vata-Kaphaja and 10% were of Pitta-Kaphaja Prakriti. Severity wise distribution showed that 80% were of moderate and 20% were of severe grade. Distribution of cause in patients showed that maximum of 67% had exposure to wind, dust, air-condition, exposure to sunlight, temperature change, followed the 53% of the patients who were using Amla (sour), Ushna-Tikshna (hot and spicy) food article, 30% patients had habit of prolonged reading, 27% had history of headache, 10% had history of rheumatoid arthritis, 07% each had history of dandruff, joint pain and chronic rhinitis, 03% each had history of myopia, multiple sclerosis, acne and chalazion.
Among 30 patients of Shushkakshipaka, 30 (100%) of patients had Garsha, Avila Darshana, Daha, Kunita, Toda/Pakavata Shoola, 29 (97%) of patients had Upadeha and 24 (80%) of patients had Raktaraji.
Result
Dry eye includes a spectrum of disorders ranging from mild eye strain to foreign-body sensation, pain, burning sensation with sight threatening complications. Patients face considerable discomfort with this affliction which interferes with the daily routine functioning. In this study, 30 patients of Shushka-Akshipaka (dry eye) were treated in two groups, each comprising 15 patients.
Efficacy of Triphala Ghrita Tarpana (TGT): 15 patients in this group were given Tarpana with Triphala Ghrita of approximately 10–15 ml in afternoon for consecutive 7 days for 30 minutes. In this group, significant relief was found in Gharsha (74%), Avila Darshana (65%), Upadeha (80%), Daha (72%), Kunita (78%), Toda (59%), Raktaraji (83%), Schirmer’s test of right eye (70%), Schrimer’s test of left eye (68%), tear break-up time of right eye (70%) and tear break-up time of left eye (69%). In 15 patients of group where Triphala Ghrita Tarpana was done, complete remission was not observed in any patient, marked relief in 26.7% and moderate relief in 73.3% of patients. In 15 patients of this group after all follow-ups, 13 patients sustained the effect of therapy, while 2 patients got recurrence in the symptoms [Table 4 and Figure 2].
Table 4.
Effect of Triphala Ghrita Tarpana
| Symptoms | Mean score | % of reduction in mean score | S.D of mean (±) | S.E of mean (±) | t | P | |
|---|---|---|---|---|---|---|---|
|
| |||||||
| BT | AT | ||||||
| Gharsha | 2.06 | 0.53 | 74.19 | 0.516 | 0.13 | 11.49 | <0.001 |
| Avila Darshana | 1.93 | 0.66 | 65.51 | 0.593 | 0.153 | 8.26 | <0.001 |
| Upadeha | 1.66 | 0.33 | 80 | 0.617 | 0.159 | 8.36 | <0.001 |
| Daha | 2.13 | 0.6 | 71.8 | 0.51 | 0.13 | 11.49 | <0.001 |
| Kunita | 1.8 | 0.4 | 77.77 | 0.50 | 0.13 | 10.68 | <0.001 |
| Toda/Pakavat Shoola | 2.26 | 0.93 | 58.82 | 0.67 | 0.17 | 7.63 | <0.001 |
| Raktaraji | 0.8 | 0.13 | 83.33 | 0.73 | 0.19 | 3.50 | <0.001 |
| Schirmer’s Test of Right Eye | 2 | 0.6 | 70 | 0.77 | 0.20 | 6.99 | <0.001 |
| Schirmer’s Test of Left Eye | 2.26 | 0.73 | 67.64 | 0.83 | 0.21 | 7.12 | <0.001 |
| Tear Break up Time of Right Eye | 2 | 0.6 | 70 | 0.81 | 0.21 | 6.63 | <0.001 |
| Tear Break up Time of Left Eye | 1.93 | 0.6 | 68.96 | 0.79 | 0.20 | 6.46 | <0.001 |
BT: Before treatment, AT: After treatment, SD: Standard deviation, SE: Standard error
Figure 2.
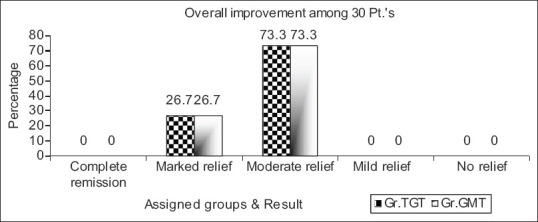
Overall percentage of improvement in the patients. TGT: Triphala Ghrita Tarpana, GMT: Goghrita Manda Tarpana group
Efficacy of Gogritha Manda Tarpana (GMT): 15 patients in this group were given Tarpana with Goghrita Manda of approximately 10–15 ml in the afternoon for consecutive 7 days for 30 minutes. In this group, the significant relief was found in Gharsha (68%), Avila Darshana (69%) [Figure 1] (73%), Upadeha (68%), Daha (53%), Kunita (68%), Toda (60%), Raktaraji (100%), Schirmer’s test of right eye (69%), Schrimer’s test of left eye (72%), tear break-up time of right eye (70%) and tear break-up time of left eye (70%) [Figure 1]. In 15 patients of this group, complete remission was not observed in any patient, marked relief in 26.7%, and moderate relief in 73.3% of patients [Figure 2]. In 15 patients of group GMT after all follow-ups, 11 patients sustained the effect of therapy, while 4 patients got recurrence in the symptoms. In nutshell, the present clinical study has established that Tarpana with Goghrita Manda yields good result in follow-up than that of Triphala Ghrita Tarpana [Tables 5 and 6, Figure 3].
Figure 1.

Comparison of improvement in the symptoms between the groups – TGT: [TGT: Triphala Ghrita Tarpana, GMT: Goghrita Manda Tarpana, AT: After treatment, RE: Right Eye, LE: Left Eye]
Table 5.
Effect of Goghrita Manda Tarpana
| Symptoms | Mean score | % of reduction in mean score | S.D of mean (±) | S.E of mean (±) | t | P | |
|---|---|---|---|---|---|---|---|
|
| |||||||
| BT | AT | ||||||
| Gharsha | 2.06 | 0.6 | 67.74 | 0.50 | 0.13 | 10.68 | <0.001 |
| Avila Darshana | 1.73 | 0.46 | 73.07 | 0.45 | 0.11 | 10.71 | <0.001 |
| Upadeha | 1.46 | 0.46 | 68.18 | 0.53 | 0.13 | 7.24 | <0.001 |
| Daha | 2.13 | 1 | 53.12 | 0.35 | 0.09 | 12.47 | <0.001 |
| Kunita | 1.86 | 0.6 | 67.85 | 0.59 | 0.15 | 8.26 | <0.001 |
| Toda/Pakavat Shoola | 2.33 | 0.93 | 60 | 0.63 | 0.16 | 8.57 | <0.001 |
| Raktaraji | 1.06 | 0 | 100 | 0.45 | 0.11 | 9.02 | <0.01 |
| Schirmer’s Test of Right Eye | 2.4 | 0.73 | 69.44 | 0.74 | 0.19 | 8.68 | <0.001 |
| Schirmer’s Test of Left Eye | 2.13 | 0.6 | 71.87 | 0.63 | 0.16 | 9.27 | <0.001 |
| Tear Break up Time of Right Eye | 2.46 | 0.73 | 70.27 | 0.61 | 0.15 | 10.87 | <0.001 |
| Tear Break up Time of Left Eye | 2.2 | 0.66 | 69.69 | 0.63 | 0.16 | 9.38 | <0.001 |
BT: Before treatment, AT: After treatment, SD: Standard deviation, SE: Standard error
Table 6.
Symptom wise effect in follow-up in the patients
| Symptom wise effect in 15 days follow-up (n=30) | Group TGT % of patients | Group GMT % of patients | ||
|---|---|---|---|---|
|
|
|
|||
| Sustained | Relapsed | Sustained | Relapsed | |
| Gharsha (gritty feeling) | 80 | 20 | 73.3 | 26.6 |
| Avila Darshana (blurring of vision) | 93.33 | 6.66 | 100 | 0 |
| Upadeha (excessive stringy mucs/filmy feeling in the eyes) | 93.33 | 6.66 | 100 | 0 |
| Daha (burning sensation in the eyes) | 60 | 40 | 86.66 | 13.33 |
| Kunitna (photophobia) | 93.33 | 6.66 | 73.3 | 26.6 |
| Toda (pricking pain in the eyes) | 86.66 | 13.33 | 93.33 | 6.66 |
| Raktaraji (congestion in the eyes) | 93.33 | 6.66 | 93.33 | 6.66 |
| Schirmer’s test RE | 80 | 20 | 86.66 | 13.33 |
| Schirmer’s test LE | 73.33 | 26.66 | 100 | 0 |
| Tear break-up time - RE | 66.66 | 33.33 | 86.66 | 13.33 |
| Tear break-up time - LE | 86.66 | 13.33 | 86.66 | 13.33 |
TGT: Triphala Ghrita Tarpana, GMT: Goghrita Manda Tarpana, RE: Right Eye, LE: Left Eye
Figure 3.
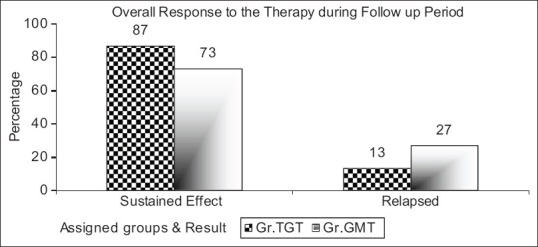
Overall response to the therapy during follow-up period in the patients. [TGT: Triphala Ghrita Tarpana, GMT: Goghrita Manda Tarpana]
Discussion
Dry eyes are one of the most common causes of chronic low-grade burning, irritation, and discomfort of the eyes. It is caused due to disturbance in the tear film function owing to change in lipid, water, or mucin component of the tears.
It is now recognized that dry eye syndrome results from an underlying cytokine and receptor-mediated inflammatory process affecting the lacrimal glands. Inflammation, in turn, can either decrease tear production or alter the contents of the tear film and disrupt homeostasis at the ocular surface, leading to dry eye syndrome. These findings have redirected treatment efforts toward more targeted therapies aimed at resolving the underlying inflammation. Anti-inflammatory/immunomodulatory treatments are now becoming standard therapy for moderate to severe dry eye syndrome.
Contemporary tear substitutes stimulate the cell surface glycoproteins that maintain ocular hydration and mucoadhesive property due to lipid content in it. It slows the evaporation of the tear film, thus resolves the condition which leads to dry eye.
Tarpana forms an occlusive film over the surface of the eyeball and improves the composition of tear film by enhancing the mucin and aqueous layers. It prevents frictional damage to the ocular surfaces secondary to lid movement or extra ocular movements. It helps by retaining fluid and maintaining hydration of the ocular surface. It is effective in reducing evaporation rate and blinking rate in patients with dry eye syndrome.[8] It prevents desiccation from corneal tear film and reduces burning sensation in patients with dry eye syndrome. It also reduces reflex tearing and the need for artificial tears and warm compressors. It is well tolerated by the patients and provides a totally new therapeutic approach providing steady levels of medication to the ocular surface which offers additional benefits in the management of dry eye syndrome.
Triphala Ghrita as being the best immune-modulator, it confers anti-inflammatory activity and in dry eye syndrome thereby prevents T-cells from releasing cytokines (primarily interleukin-6) that incite the inflammatory component of dry eye. As Triphala Ghrita is best for its antibiotic activity, it reduces the inflammation and improves lipid production in dry eye syndrome.[9]
Goghrita Manda is a Sneha Dravya (oily material) belonging to Jangama Varga (animal origin). It is considered best in all Sneha Dravyas. Ayurveda recommends Goghrita as best and if not specified, the epithet Ghrita always applies to Goghrita. Goghrita is lipophilic in nature which facilitates absorption through corneal epithelium.
Moreover, compared to the artificial tear products, as Triphala Ghrita or Goghrita is rich in lipid content which reflects mucoadhesive properties, the degree of contact time with the ocular surface is greater. Hence, the effect of Tarpana is better as it has got contact time of more than 15 min. Tarpana also stimulates the lacrimal glands to produce tears. Mucin layer which is present in tear film allows the Ghrita to spread over the ocular surface. This approach provides long lasting relief to the patients with moderate-to-severe dry eye symptoms.
Conclusion
The explanation of clinical features of Shushkakshipaka in all classical texts collectively gives complete picture that resembles with dry eye syndrome. The effect of Triphala Ghrita Tarpana is better in the subsequent follow-up than immediately after effect of the treatment with minimal recurrence, in the cases of dry eye syndrome. The effect of Goghrita Manda Tarpana is better in immediately after effect of the treatment but found to have a greater rate of recurrence.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Srikanthamurthy KR. Sushruta Samhita of Sushruta, Uttara Tantra. Ch. 6. Ver. 26. Reprint edition. Varanasi: Chaukhamba Orientalia; 2002. p. 137. [Google Scholar]
- 2.Acharya YT. Sushruta Samhita of Sushruta, Uttara Tantra. Ch. 6. Ver. 26. 9th ed. Varanasi: Chaukhamba Orientalia; 2007. p. 605. [Google Scholar]
- 3.Khurana AK, Choudhary R, Ahluwalia BK, Gupta S. Hospital epidemiology of dry eye. Indian J Ophthalmol. 1991;39:55–8. [PubMed] [Google Scholar]
- 4. [[last access date 03/06/2009]]. Available from: http://www.shroffeyecentre.com/services/faq-what-is-dry-eye-syndrome-2 .
- 5.Ambikadutta SK. Sushruta Samhita of Sushruta, Uttara Tantra. Ch. 18. Ver. 17-18. Edition 4th. Varanasi: Chaukhamba Sanskrit Sansthana; 2004. p. 149. [Google Scholar]
- 6.Acharya YT. Sushruta Samhita of Sushruta, Uttara Tantra. Ch. 18, Ver. 17-18. Edition 3th. Varanasi: Chaukhamba Surbharati Publication; 2008. p. 634. [Google Scholar]
- 7.Shiva Prasad Sharma editor. Ashtanga Samgraha of Vagbhatta, Sutra Sthana. Ch. 18, 33. Ver. 17-18, 1. Edition 3th. Varanasi: Chaukhamba Sanskrit Series; 2006. p. 235. [Google Scholar]
- 8.Chouhan B, Kumawat RC, Kotecha M, Nathani S. Triphala – A comprehensive Ayurvedic review. Int J Res Ayurveda Pharm. 2013;4:512–7. [Google Scholar]
- 9.Gowda DV, Muruli G, Rangesh PR, Deshapande RD. Phytochemical and pharmacological actions of Triphala; Ayurvedic formulation – A review. Int J Pharm Sci Rev Res. 2012;15:16–5. [Google Scholar]