

Abstract
Purpose
Soft contact lenses (SCLs) are effective for refractive error correction, but prolonged wear triggers discomfort and discontinuation. This study investigates whether water gradient technology of delefilcon A-based SCLs improve tear film dynamics.
Methods
This retrospective observational study included 50 asymptomatic delefilcon A or narafilcon A users. Data on thin aqueous layer break (TALB; %), noninvasive tear break-up time (NIBUT), tear meniscus height (TMH; mm), subjective dryness, and higher-order aberrations (HOAs) were collected. Measurements of the bare eye, the SCL-worn eye after 15 minutes (visit 1 [v1]) and 30 ± 5 days after v1 after SCL was worn for ≥5 hours (visit 2 [v2]) were recorded.
Results
TALB was significantly reduced in the delefilcon A group compared to the narafilcon A group (33.3% vs. 85.5% at v1; P < 0.0001 and 31.7% vs. 80.4% at v2; P < 0.0001). The NIBUT was also significantly higher in the former (4.2 ± 2.1 seconds vs. 2.9 ± 1.5 at v1; P < 0.01 and 4.1 ± 2.3 seconds vs. 2.7 ± 1.6 seconds at v2; P < 0.01) across both visits. The TMH was significantly reduced in the former in both v1 and v2. The total ocular HOAs were significantly lower in the former at v1 (P < 0.001) and v2 (P < 0.05) compared to the bare eye.
Conclusions
The water gradient technology of delefilcon A reduces TALB and increases NIBUT.
Translational Relevance
The use of water gradient technology improves tear film dynamics and alleviate pathological break-up pattern, improving lens performance.
Keywords: water gradient, structure; silicone hydrogel-soft contact lens; thin aqueous layer break; tear film; contact lenses
Introduction
Advances in the field of corneal physiology have extensively improved the material, design, and production of soft contact lenses (SCLs), making them one of the safest and most sought after and effective interventions for refractive error correction.1 However, continuous and extended SCL wear has been associated with side effects and undue stress to the corneal physiology mainly due to oxygen shortage,2 corneal neovascularization,3 and endothelial damage.1
Silicone hydrogel (SH) SCLs were developed about 2 decades ago to counter the caveats associated with SCLs and conventional hydrogel lenses.4,5 The interaction of the mobile silicon-oxygen bonds imparts distinct surface and mechanical properties to the SHs, enhancing oxygen permeability, reducing protein deposition and modest frictional interaction, and causing increased lipid and elastic response.6 Studies have also established that SH lenses reduce the level of limbal redness,7 alleviate contact lens-associated keratitis,8 and enhance the supply of oxygen to the ocular surface over their conventional hydrogel counterparts.9 Despite these advantages, symptoms associated with contact lens discomfort (CLD) persist.10 SCLs (both conventional and SH) wear alters the lipid layer by reducing the prelens lipid layer thickness; increasing tear evaporation rate; reducing tear break-up time; and altering the concentration of cholesterol esters, wax esters, and phospholipids.11
The tear film kinetics of SCL are governed by features such as a shorter break-up time, decreased contact lens surface coverage by the tear film during the overall interblink period, and greater contact lens surface exposure to the atmosphere at the time of the blink.12 The two key factors that cause CLD were reported to be the contact lens material and environment.10 Specifically, the factors associated with the lens material include lubricity and water content.
Dailies Total1 (DT1; delefilcon A) was developed as a water gradient SH-SCL whose lens surface has distinct properties designed to minimize surface problems associated with the SH-SCLs. It has a core silicone hydrogel material comprising 33% water that can transit to the outer surface layer with 80% water. The surface has a low compression modulus and a unique water gradient technology that ensures that the surface is lubricated along with continual high oxygen transmission.13 The present study investigates whether the water gradient structure of SH-SCL, delefilcon A, contributes to improving the tear film dynamics including break-up patterns, noninvasive tear break-up times (NIBUT), tear meniscus height (TMH), and other end points such as higher-order aberrations (HOAs), subjective dryness, and SCL thickness, compared to the conventional SH-SCLs, narafilcon A.
Materials and Methods
Study Design
This retrospective observational study included 50 regular SH-SCL asymptomatic users. The study was approved by the institutional review board of Kawasaki Medical School Hospital (approval number 3403). Informed consent was obtained from all the study participants, and the study adhered to the tenets of the Declaration of Helsinki and was performed according to Good Clinical Practice (GCP). The study end points were evaluated by the researchers in a masked manner. The identity of the sponsor of the study (Alcon) was masked to the assessors until the completion of the study. This study did not involve patients or the public in its design, participant recruitment, or conduct.
Data Collection
The study observation period was defined as the date from which the patient started receiving care at the study site until the last data point was measured and was between May 1, 2019, and February 29, 2020. To ensure uniform data collection, assessment, and compliance with GCP, onsite training was conducted. The patient data records were selected based on the study inclusion and exclusion criteria and the patients receiving care between May 1, 2019, and February 29, 2020, were included in the study. To minimize bias, the eligible patients were enrolled in one of the two study groups (delefilcon A and narafilcon A) allotted in a consecutive series. Delefilcon A lenses are SH-SCLs with a water gradient structure and high lubricity surface.14,15 The core has a low water content of 33%, similar to other conventional SH-SCLs.16 To compare delefilcon A with conventional SH-SCLs, we chose narafilcon A as the control lens, because its core also has a low water content of 46%.17 Both are daily disposable SH-SCLs.18 The water content of narafilcon A is constant throughout the lens, whereas water gradient technology of delefilcon A creates a low water content core with a high water content surface.17 Numerous previous studies of delefilcon A have also compared it with narafilcon A.19–22
The background data included age, gender, power (diopter), Schirmer's test (mm), central corneal thickness (CCT; µm), ophthalmic solution use, and the following data elements measured on the bare eye, namely TALB (%), NIBUT (seconds) by the tear interferometer DR-1α (Kowa, Tokyo, Japan), and video-corneal topographer Keratograph 5M (Oculus, Wetzlar, Germany), TMH (mm), subjective dryness estimated by the visual analog scale (VAS; minimum 0 and maximum 100), and ocular HOA. The post-baseline data were categorized as visit-1 (v1) and visit-2 (v2) for each patient based on the chronology of availability. For data based on the qualification tests, bare eye measurements, the time that SCLs were worn to the hospital, removed, and washed-out was set as ≥30 minutes. Data were collected for clinical v1 after tests and observation parameters were measured post-SCL wearing for 15 minutes. For clinical v2, data from tests and observation parameters measured after wearing SCLs for ≥5 hours, after 30 ± 5 days of wearing SCLs following v1, were collected. Between v1 and v2, SCLs were used 5 to 12 hours per day, and 5 to 7 days per week. Room temperature and humidity was maintained at 23 to 25°C and 30 to 40%.
Using the tear interferometer DR-1α (Kowa, Tokyo, Japan), the break up pattern with SCLs was classified into six patterns consist of area break (AB), line break (LB), thin aqueous layer break (TALB), spot break (SB), dimple break (DB), and random break (RB), as previously reported by Yokoi et al.23,24 For these break-up pattern, the three videos captured using the DR-1α were judged in a masked manner. A total of nine judgments comprising three videos by three researchers per one eye were used, and the majority of the break-up patterns were adopted. From the previous reports,23–25 AB is observed when there is no aqueous tear on the SCL surface; LB, when streak line shape near the lower SCL because of aqueous tear deficient and suction effect on the aqueous tear from the lower tear meniscus; TALB, when colorful interference fringes immediately after eye opening when there is no lipid layer on the SCL surface due to thin aqueous tear; SB, when the wettability of the SCL surface is decreased and observed spot shape; DB, when streak line shape around the central SCL because of impaired wettability of the SCL surface; and RB, after the complete establishment of tear film and the result of evaporation of aqueous tear. For instance, AB, LB, and TALB were defined as aqueous deficient types. SB and DB were defined as decreased wettability types. RB was defined as increased evaporation type.
For the NIBUT, the three videos captured using the tear interferometer DR-1α were analyzed in a masked manner, and the three break-up times were averaged.
TMH, CCT, and SCL thickness were obtained using anterior segment optical coherence tomography (AS-OCT) CASIA 2 (Tomey Corporation, Nagoya, Japan). The analysis software (Tomey Corporation) identified and digitized the anterior corneal or SCL surfaces and posterior corneal surfaces as well as tear meniscus areas. All of the digitization were confirmed by researches in a masked manner. For TMH and CCT, the three measurement values were averaged. SCL thickness were calculated as CCT wearing SCL − CCT without SCL.
Ocular HOAs measured were total HOA, coma, trefoil, spherical, tetrafoil, and second order astigmatism aberrations through a 6 mm pupil using a Shack—Hartmann wavefront sensor in the KR-1W Wavefront Analyzer (TOPCON, Tokyo, Japan). The HOA values (RMS; in µm) measured every 1 to 10 seconds after each blink were averaged.
All the data from the measurements done on bilateral eyes were collected.
Study Participants and Visits
Participants
A retrospective review of the clinical records (including video records), of 50 SH-SCL users was conducted for the potential participants who were able to achieve a clinically acceptable fit with each of the study lenses. Asymptomatic participants who were ≥20 years of age with far corrected vision of ≥0.8 in both eyes, those wearing contact lenses at least 5 days a week for greater than 5 hours a day, and regular users of Dailies Total 1 (DT1); Alcon (delefilcon A) or 1-Day Acuvue TruEye (TE): Johnson & Johnson Vision (narafilcon A) lenses were included from one site (Inoue eye clinic) in Japan.
Contact lens wearers without active ocular surface disorders, such as epithelial disorders, infections, conjunctivitis, ocular inflammatory disease, and nasolacrimal duct obstruction were selected. As an exception, those with a dry eye with a short break-up time were included in the study because such symptoms are often evident in contact lens users and hold clinical significance capable of being targeted effectively with delefilcon A. Those individuals with a history of ocular surface surgery or those who were considered unsuitable by the principal investigator were excluded from the study. To minimize the intervention in this retrospective study, subjects were enrolled as delefilcon A or narafilcon A habitual users. The 50 SH-SCL users consisted of a consecutive series of 25 delefilcon A habitual users and 25 narafilcon A habitual users who met the above criteria.
Statistical Analysis
The study was designed to assess the difference between delefilcon A and narafilcon A groups in terms of tear film dynamics. The sample size was planned for examining the null hypothesis of no difference between the two groups (delefilcon A/narafilcon A) with the specified probability. The data distributions were assessed for normality using the Shapiro-Wilk test. Following the assumption that all the data on the outcomes of interest followed a parametric distribution, the two-sample independent t-test was used to analyze the data, except for the male/female ratio, ophthalmic solution use ratio, and TALB ratio. Additionally, the paired t-test with Bonferroni correction were performed to compare the HOAs among bare eyes, v1, and v2. For the male/female ratio, ophthalmic solution use, and TALB ratio, Pearson's chi-squared test was used. All the statistical analyses were performed using the SPSS version 25.0 (IBM Corp. Released 2017; IBM SPSS Statistics for Windows, Version 25.0; Armonk, NY: IBM Corp. USA).
Results
Enrollment
In this study, a total of 50 patient records were reviewed and 100 eyes of 50 regular SH-SCL users were enrolled into 2 groups. These were 25 regular users (50 eyes) of delefilcon A-based DT1, and 29 regular users (58 eyes) of narafilcon A-based TE. In the 29 narafilcon A participants, 4 participants (8 eyes) also used delefilcon A and were included in the delefilcon A group. For those 4 participants that used both lenses, the v1 and v2 measurements were recorded for an additional day after 60 days, compared to the measurements for the individuals using only either delefilcon A and narafilcon A.
The study of three patients who never appeared for the v2 was discontinued after v1. The three patients included two participants from the delefilcon A group and one participant from the narafilcon A group. There were no reports of discontinuation due to adverse events.
Demographics
The study comprised a total of 10 male subjects and 40 female subjects with an average age of 34.59 ± 9.95 years and 32.47 ± 8.66 years for the delefilcon A and narafilcon A groups, respectively. There were no significant differences between the study groups in the baseline parameters (Table 1), and studied parameters in bare eye (Table 2). No ophthalmic solution was used other than artificial tears or anti-allergic eye drops.
Table 1.
Comparison of the Background Data Between the Two SH-SCLs
| Narafilcon A (in Narafilcon A) Average ± SD | Delefilcon A (in Delefilcon A) Average ± SD | P Value Delefilcon A vs. Narafilcon A | |
|---|---|---|---|
| CCT (µm) | 533.7 ± 32.2 | 530.7 ± 31.2 | 0.32 |
| Power (diopter) | −3.71 ± 1.47 | −3.30 ± 1.50 | 0.17 |
| Schilmer’ test (mm) | 20.7 ± 2.8 | 17.5 ± 0.9 | 0.20 |
| Age (years) | 32.47 ± 8.66 | 34.59 ± 9.95 | 0.42 |
| Female ratio | 0.83 | 0.70 | 0.28a |
| Artificial tears use | 20.7% (6/29) | 40.0% (10/25) | 0.12a |
| Anti-allergic use | 3.5% (1/29) | 12.0% (3/25) | 0.23a |
The data are expressed as mean ± standard deviation.
P values were calculated using two-sample independent t-test in all instances except for Female ratio and ophthalmic solution use ratio where the Pearson chi-squared test was used.
CCT, central corneal thickness; SD, standard deviation; SH-SCL, silicone hydrogel-soft contact lens.
Table 2.
Comparison of the End Points Between the Two SH-SCLs
| Narafilcon A (in Narafilcon A) (Average ± SD) | Delefilcon A (in Delefilcon A) (Average ± SD) | P Value Delefilcon A vs. Narafilcon A | |
|---|---|---|---|
| Bare eye: | |||
| NIBUT (DR-1α) (in seconds) | 6.9 ± 2.9 | 6.7 ± 3.2 | 0.71 |
| TMH (mm) | 0.25 ± 0.07 | 0.27 ± 0.07 | 0.20 |
| Subjective dryness (VAS score) | 53.8 ± 23.1 | 49.6 ± 23.1 | 0.36 |
| NIBUT (in seconds) (Keratograph 5M) | 7.3 ± 3.1 | 7.6 ± 3.6 | 0.60 |
| TALB (%) | 0 | 0 | 1a |
| HOA (RMS; in µm) | 0.39 ± 0.13 | 0.39 ± 0.18 | 0.95 |
| Visit 1 (v1): | |||
| NIBUT (DR-1α) (in seconds) | 3.0 ± 1.6 | 4.2 ± 2.2 | 0.0016 |
| TMH (mm) | 0.24 ± 0.07 | 0.19 ± 0.06 | 0.002 |
| Subjective dryness (VAS score) | 16.4 ± 16.4 | 19.6 ± 18.6 | 0.37 |
| NIBUT (in seconds) (Keratograph 5M) | 6.3 ± 2.9 | 7.1 ± 2.7 | 0.13 |
| TALB (%) | 88.5 | 33.3 | <0.0001a |
| SCL thickness (µm) | 94.1 ± 6.7 | 106.4 ± 11.5 | <0.0001 |
| HOA (RMS; in µm) | 0.40 ± 0.16 | 0.34 ± 0.15 | 0.18 |
| Visit 2 (v2): | |||
| NIBUT (in seconds) (DR-1α) | 2.7 ± 1.6 | 4.1 ± 2.4 | 0.0017 |
| TMH (mm) | 0.22 ± 0.08 | 0.18 ± 0.05 | 0.019 |
| Subjective dryness (VAS score) | 26.7 ± 21.6 | 23.0 ± 17.0 | 0.35 |
| NIBUT (in seconds) (Keratograph 5M) | 6.8 ± 3.6 | 6.3 ± 2.7 | 0.49 |
| TALB (%) | 80.4 | 31.7 | <0.0001a |
| SCL thickness (µm) | 93.5 ± 7.0 | 103.0 ± 8.8 | <0.0001 |
| SCL thickness ratio (v2/v1) | 0.994 ± 0.082 | 0.977 ± 0.077 | 0.28 |
| HOA (RMS; in µm) | 0.40 ± 0.14 | 0.35 ± 0.13 | 0.14 |
| CLDEQ-8 questionnaire score in v2: | |||
| 1-a discomfort: frequency | 1.15 ± 0.81 | 1.14 ± 0.84 | 0.98 |
| 1-b discomfort: severity | 1.33 ± 1.23 | 1.43 ± 1.31 | 0.72 |
| 2-a dryness: frequency | 1.30 ± 0.60 | 1.24 ± 0.93 | 0.73 |
| 2-b dryness: severity | 1.48 ± 1.08 | 1.71 ± 1.37 | 0.37 |
| 3-a blurry vision: frequency | 0.85 ± 0.90 | 0.76 ± 0.62 | 0.56 |
| 3-b blurry vision: severity | 0.81 ± 0.99 | 0.95 ± 1.10 | 0.53 |
| 4 The need for closing eyes | 0.52 ± 0.79 | 0.81 ± 0.92 | 0.11 |
| 5 The need for removing the lenses | 1.44 ± 1.00 | 1.33 ± 1.22 | 0.63 |
The data are expressed as mean ± standard deviation.
P values were calculated using two-sample independent t-test in all instances except for TALB (%) where the Pearson chi-squared test was used. Compared with narafilcon A, there were significant changes in TALB, NIBUT, TMH in delefilcon A.
CLDEQ-8, contact lens dry eye questionnaire-8; HOA, higher-order aberration; NIBUT, non-invasive tear break-up time; SD, standard deviation; SH-SCL, silicone hydrogel-soft contact lens; TALB, thin aqueous layer break; TMH, tear meniscus height; VAS, subjective dryness estimated by the visual analog scale.
Abnormal Break-Up Patterns: Thin Aqueous Layer Break
Among the abnormal break-up patterns assessed at v1 and v2, there was a significantly lower rate of TALB in the delefilcon A compared to the narafilcon A (P < 0.0001; Fig. 1, Supplementary Video 1). At v1 after 15 minutes of SCL wear, the TALB was 33.3% and 88.5% in the delefilcon A group and narafilcon A group, respectively. At v2 after ≥5 hours of SCL wear, the TALB was 31.7% and 80.4% in the delefilcon A group and narafilcon A group, respectively.
Figure 1.

Comparison of break-up patterns between study groups at visit 1 and visit 2. Abnormal break-up pattern TALB was significantly suppressed in the SH-SCL (delefilcon A) equipped with a water gradient structure. *** P < 0.0001, Pearson's chi-square test. TALB, thin aqueous layer break; RB, random break; DB, dimple break; LB, line break; AB, area break; SB, spot break; v1, visit 1; v2, visit 2.
NIBUT
There was a significant difference in NIBUT measured with DR-1α, between the two study groups. At v1, the mean NIBUT in the delefilcon A group and narafilcon A group was 4.2 ± 2.2 seconds and 3.0 ± 1.6 seconds, respectively. At v2, the mean NIBUT in the delefilcon A group and narafilcon A group was 4.1 ± 2.4 seconds and 2.7 ± 1.6 seconds, respectively.
The NIBUT was significantly higher in the delefilcon A group than in the narafilcon A group (P = 0.0016 at v1, and P = 0.0017 at v2; Table 2, Fig. 2). The NIBUTs measured with the Keratograph 5M while wearing the SCLs showed no significant difference across groups.
Figure 2.
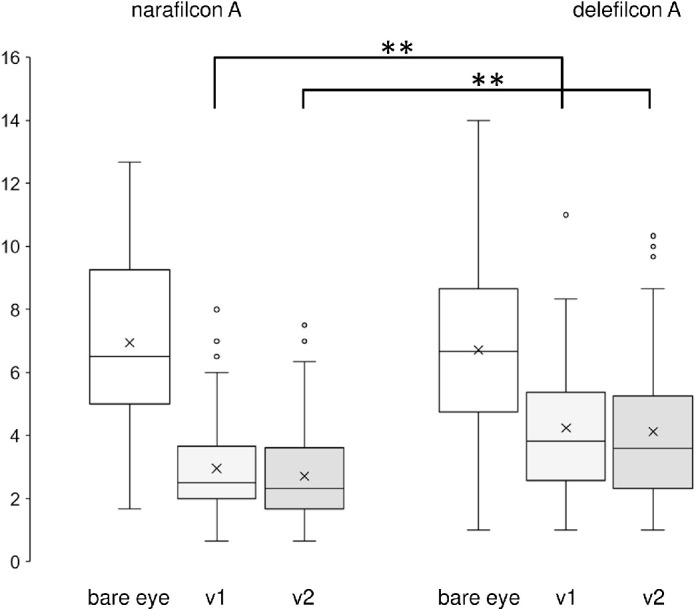
Comparison of NIBUT measured by DR-1α. The amount of NIBUT (in seconds) shortening was significantly inhibited with delefilcon A as compared to narafilcon A. The horizontal lines in the box and whisker plots represent the median values, and the bottom and top of the boxes represent the lower and upper quartiles, respectively. The x represents the mean and the bars represent the minimum and maximum values within 1.5 times the lower and upper quartiles. ** P < 0.01, t-test, the two-sample independent t-test.
TMH
At baseline, when measured on a bare eye, the mean TMH was 0.27 ± 0.07 mm and 0.25 ± 0.07 mm in the delefilcon A and narafilcon A groups, respectively. After SCL wear at v1 and v2, there was a decrease in TMH in both delefilcon A and narafilcon A groups. TMH was found to be significantly lower in the delefilcon A group at both v1 and v2 than in the narafilcon A group (P = 0.002 and P = 0.019, respectively; Fig. 3).
Figure 3.
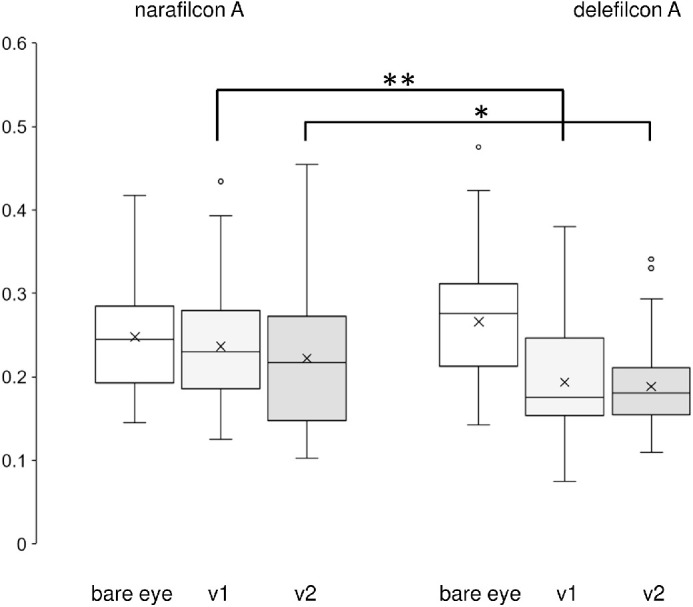
Comparison of TMH measured across study groups and visits. The tear meniscus height (TMH; in mm) was lower with delefilcon A in both visit 1 (v1) and visit 2 (v2). The horizontal lines in the box and whisker plots represent the median values, and the bottom and top of the boxes represent the lower and upper quartiles, respectively. The x represents the mean and the bars represent the minimum and maximum values within 1.5 times the lower and upper quartiles. ** P < 0.01, *P < 0.05, the two-sample independent t-test.
Subjective Dryness
The mean subjective dryness score measured on the bare eye through a VAS was 49.6 ± 23.1 and 53.8 ± 23.1 in the delefilcon A and narafilcon A groups, respectively.
At v1 and v2, there was a decrease in subjective dryness scores in the delefilcon A group (19.6 ± 18.6 and 23.0 ± 17.0, respectively) and in the narafilcon A group (16.4 ± 16.4 and 26. 7 ± 21.6) from the baseline.
No significant difference in the VAS scores on subjective dryness was observed between the delefilcon A and narafilcon A groups across both visits. No differences were observed between the study groups when the CLDEQ-8 questionnaire was administered at v2.
Total Ocular HOAs
When measured one second after eye blink on the bare eye, the total ocular HOAs (RMS; in µm) in the delefilcon A group were 0.39 ± 0.18 at baseline and significantly decreased to 0.34 ± 0.15 at v1 and to 0.35 ± 0.13 at v2 (P = 0.0003 at v1 and P = 0.038 at v2). In the narafilcon, A group, the bare eye HOAs were 0.39 ± 0.13, and there was no significant difference observed in HOAs at visits v1 and v2 compared to the bare eye (Fig. 4, Table 3). The total ocular HOAs, 2 seconds after the blink did not significantly (P ≥ 0.05) differ from those at the bare eye in both delefilcon A and narafilcon A groups.
Figure 4.
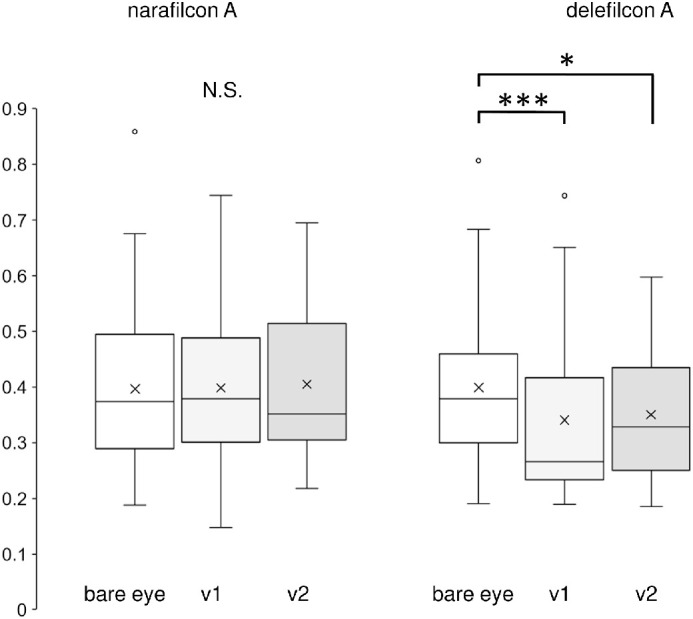
Total ocular HOAs across study visits, 1 secondafter eye blink. In delefilcon A, the total ocular HOAs (RMS; in µm) in visit 1 (v1) and visit 2 (v2) is superior to bare eye. The horizontal lines in the box and whisker plots represent the median values, and the bottom and top of the boxes represent the lower and upper quartiles, respectively. The x represents the mean and the bars represent the minimum and maximum values within 1.5 times the lower and upper quartiles. *** P < 0.001, * P < 0.05, paired t-test with Bonferroni correction. HOAs, higher-order aberrations.
Table 3.
Comparison of HOAs Between the Two SH-SCLs Across Study Visits, 1 Second After Eye Blink
| HOA (RMS; in µm) | Narafilcon A (in Narafilcon A) (Average ± SD) | Delefilcon A (in Delefilcon A) (Average ± SD) | P Value Delefilcon A vs. Narafilcon A | ||
|---|---|---|---|---|---|
| Bare eye: | |||||
| Total | 0.39 ± 0.13 | 0.39 ± 0.18 | 0.95 | ||
| Third | |||||
| Coma | 0.20 ± 0.11 | 0.19 ± 0.10 | 0.73 | ||
| Trefoil | 0.18 ± 0.11 | 0.15 ± 0.08 | 0.14 | ||
| Fourth | |||||
| Spherical | 0.14 ± 0.09 | 0.18 ± 0.10 | 0.10 | ||
| Tetrafoil | 0.07 ± 0.04 | 0.08 ± 0.04 | 0.49 | ||
| Second astigmatism | 0.09 ± 0.07 | 0.07 ± 0.05 | 0.30 | ||
| HOA (RMS; in µm) | Narafilcon A (in Narafilcon A) (Average ± SD) | P Value vs. Bare Eye | Delefilcon A (in Delefilcon A) (Average ± SD) | P Value vs. Bare Eye | P Value Delefilcon A vs. Narafilcon A |
| Visit 1 (v1): | |||||
| Total | 0.40 ± 0.16 | 0.66 | 0.34 ± 0.15 | 0.0003 | 0.18 |
| Third | |||||
| Coma | 0.18 ± 0.08 | 0.11 | 0.17 ± 0.09 | 0.06 | 0.60 |
| Trefoil | 0.20 ± 0.12 | 0.69 | 0.12 ± 0.07 | 0.0041 | 0.005 |
| Fourth | |||||
| Spherical | 0.11 ± 0.09 | 0.34 | 0.11 ± 0.09 | <0.0001 | 0.036 |
| Tetrafoil | 0.11 ± 0.10 | 0.13 | 0.08 ± 0.04 | 0.93 | 0.21 |
| Second astigmatism | 0.10 ± 0.05 | 0.58 | 0.09 ± 0.06 | 0.99 | 0.33 |
| Visit 2 (v2): | |||||
| Total | 0.40 ± 0.14 | 0.73 | 0.35 ± 0.13 | 0.038 | 0.14 |
| Third | |||||
| Coma | 0.19 ± 0.10 | 0.66 | 0.19 ± 0.11 | 0.41 | 0.91 |
| Trefoil | 0.20 ± 0.10 | 0.12 | 0.14 ± 0.09 | 0.017 | 0.023 |
| Fourth | |||||
| Spherical | 0.12 ± 0.08 | 0.028 | 0.12 ± 0.08 | 0.0008 | 0.90 |
| Tetrafoil | 0.10 ± 0.06 | 0.014 | 0.09 ± 0.07 | 0.82 | 0.88 |
| Second astigmatism | 0.09 ± 0.04 | 0.39 | 0.10 ± 0.06 | 0.08 | 0.95 |
The data are expressed as mean ± standard deviation. P values were calculated using two-sample independent t-test to compare between the two SH-SCL groups. P values were calculated using the paired t-test with Bonferroni correction to compare the HOAs among bare eye, v1, and v2.
HOA, higher-order aberration; SD, standard deviation; SH-SCL, silicone hydrogel-soft contact lens.
SCL Thickness
The SCL thickness measured at v1 was 106.4 ± 11.5 mm and 94.1 ± 6.7 mm in the delefilcon A and narafilcon A groups, respectively. At v2, the delefilcon A and narafilcon A groups had an SCL thickness of 103.0 ± 8.8 mm and 93.5 ± 7.0 mm, respectively. There was no significant difference in the rate of decay from v1 to v2, between both study groups.
Discussion
This study assessed whether the water gradient structure of the SH-SCL, delefilcon A, has an impact on tear film dynamics, including break-up patterns, NIBUT, and TMH measured for the bare eye and while wearing SCL. It also assessed the impact on ocular HOAs, subjective dryness, and SCL thickness. Overall, the SH-SCL delefilcon A lenses with a water gradient structure showed a significantly lower TALB compared to the conventional SH-SCL narafilcon A. The tear break-up times as measured by interferometry were significantly increased in the SH-SCL delefilcon A lens wearers compared to the SCL narafilcon A lens wearers. However, the TMH, which is a measure of the tear volume was significantly lowered in delefilcon A wearers compared to narafilcon A lens wearers.
Prolonged soft contact lens usage often produces dry eye syndrome that results in discomfort that eventually lead to the discontinuation of use.26–28 SCL use often induces reversible changes in the corneal and conjunctival sensitivity and inflammation producing dry eye.29–32 The dry eye syndrome arises either due to inadequate tear film secretion or excessive water loss from the tear film by evaporation. According to the National Eye Institute and Industry Workshop, contact lens-associated dry eye occurs due to the evaporative loss of tears33,34 that reduces the break up time (BUT).
Tear film dynamics and break-up patterns like TALB were initially proposed by Yokoi and Georgiev,23,25 as one of the major mechanisms of diagnosis and pathogenesis of dry eye. TALB is known to occur immediately after eye-opening when there is no lipid layer on the SCL surface due to a thin aqueous layer tear, and rarely observed in bare eye.24 In our study, we found a significant decrease in TALB among the SH-SCL delefilcon A lens wearers compared to the SCL narafilcon A lens wearers. The conventional SH SCLs (narafilcon A) has a low water content of 30% to 40% in all the layers such that the SCL surface is water-repellent, and tears evaporate immediately and easily from the surface. In our results, almost all break-up patterns were TALB among conventional SH-SCL wears in both v1 and v2 (Supplementary Video 1). On the contrary, delefilcon A exploits the innovative water gradient technology to provide surface lubrication (or wettability), which reduces the TALB of the surface of the lens and retains the wettability of the surface.
Previous studies have reported that the delefilcon A lens has prolonged wettability19 and a longer NIBUT (13.4 seconds) compared to narafilcon A (12.3 seconds; P < 0.001).21 Another study by Guillon et al.35 showed that the mean NIBUT of delefilcon A was longer (9.2 seconds) than that of narafilcon A (5.1 seconds, P = 0.006). The recent study by Itokawa et al.24 showed that the NIBUT measured by Keratograph 5M did not correlate to that measured by DR-1α in the eyes with SCL and proposed the possibilities that Keratograph 5M frequently captures the tear dynamics in the posterior but not the anterior surface of SCL, resulting in inaccurate NIBUT values. In our measurements, Keratograph 5M was unstable as reported by Itokawa et al.; thus, we used DR-1α measurements for the NIBUT analysis. The results of NIBUT measured in the current study also showed similar results. The mean break-up time in the delefilcon A lens wearers at visits v1 and v2 were 4.2 seconds and 4.1 seconds, respectively, whereas the mean break-up time in the narafilcon A group was about 3.0 seconds and 2.7 seconds at visits v1 and v2, respectively. The differences were statistically significant. In our results, NIBUTs were relatively shorter than the previous reports. This may be because we included the patients with a dry eye with a short break-up time, which is clinically important in SCL users including delefilcon A.
The TMH evaluates the tear volume, and a low tear meniscus height correlate to dry eye. Previous studies have established that in dry eye syndrome, discomforts arise due to the reduction in the tear meniscus.36,37 A study by Wolffsohn et al.21 had demonstrated that TMH of delefilcon A was greater (0.35 mm) than that of narafilcon A (0.32 mm; P = 0.016). However, in the current study, the TMH was found to be significantly lower with delefilcon A in both v1 and v2 compared to that with narafilcon A. This shortening of TMH could be attributed to the thin high-water content film that absorbs the tears in eyes with relatively short NIBUT in our study.
Measurement of the higher-order aberrations represents the quality of vision. A previous study by Mico et al.17 has shown that delefilcon A demonstrates a lower level of aberrations compared to other lenses. In the current study, the total ocular HOAs were significantly lower in the delefilcon A group at v1 and v2 compared to the bare eye, 1 second after eye blink. No such significance was observed in the narafilcon A group. Thus, lower HOAs in the delefilcon A group could result in a higher quality of vision compared to that of the bare eye. This may be because the delefilcon A surface is optically smooth due to the tear rich environment shortly after an eye blink compared to narafilcon A, which have relatively water repellent surface and frequently accompany TALB. The reduction of HOAs was not observed after 2 seconds after the eye blink. The NIBUT was 4.2 ± 2.2 seconds at v1 and 4.1 ± 2.4 seconds at v2 in delefilcon A. After 2 seconds after the eye blink, the tear film on the delefilcon A may be disturbed if not broken up. In HOAs, a decrease in trefoil aberration by delefilcon A use was observed at both v1 and v2, likely one of the reasons for the reduction in total HOAs. In addition, spherical aberration decrease was observed in delefilcon A eyes in v1 and v2, and narafilcon A eyes in v2, which may also contribute to the total HOA decrease, considering the previous report that SH-SCL use affects spherical aberration.38
For assessing the subjective dryness experienced by the participants, the contact lens dry eye questionnaire (the CLDEQ-8) was used.39 Chalmers et al.27 previously reported the use of the CLDEQ-8 questionnaire. In this study, there was no difference in the subjective dryness between SCLs with (delefilcon A) or without (narafilcon A) the water gradient structure. The absence of any changes in the subjective dryness score using the VAS could be either because this study was a parallel-design study, with few comparisons made with respect to SCL-worn by the same subject, or that this study was conducted on normal subjects; hence, there might have been no evident differences in the subjective symptoms.
Delefilcon A constitutes the daily disposable water gradient contact lenses marketed as DAILIES TOTAL1 (by Alcon Laboratories, Inc., Fort Worth, TX, USA). They possess the characteristics of both conventional hydrogel and SH lenses. The delefilcon A lenses have a SH core with a water content of 33% ± 2% and a surface water content of 84.6%.13 They have a total surface thickness of 5.9 ± 0.8 µm, including a 1 to 2 µm transition zone and 4 to 5 µm outer surface layer with a lower compression modulus and a significant modulus gradient in the zone of transition.13 These features result in a water gradient that transitions from the lower water content core to the higher water content outermost hydrophilic gel layer, which provides high oxygen transmissibility and high tensile modulus to these lenses compared to their conventional SH counterpart, narafilcon A, which has only 46% water content. Therefore, the water gradient structure might have contributed to a reduction of TALB and an increase in NIBUT among the delefilcon A lens users.
This was a retrospective and an observational study. Therefore, no randomization was done. To minimize the bias, the break-up patterns and NIBUT were assessed by the researchers under masked conditions. In addition, a consecutive series of individuals were included in both delefilcon A and narafilcon A groups with characteristics that matched the inclusion criteria to negate the chance of bias. In this study, artificial tears or anti-allergic ophthalmic solutions were used in some patients, which could impact the results on tear dynamics; however, the distribution of participants did not differ between the delefilcon A and narafilcon A groups.
Conclusion
In conclusion, the tear film dynamics, including break-up patterns and break-up times, are significantly influenced by the water gradient structure of the delefilcon A lens. Thus, the usage of the delefilcon A lens can alleviate the abnormal break-up pattern among the lens wearers and improve lens performance.
Supplementary Material
Acknowledgments
The authors thank H. Kamao, Y. Ieki, K. Tomita, A. Masuda, Y. Mito, and Y. Setoguchi for the discussions, advice, and criticism that greatly benefited this project.
Funded in part by an unrestricted investigator-initiated grant from Alcon Japan Ltd (Grant Number: 42166553). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Approved by the institutional review board of Kawasaki Medical School Hospital (approval number 3403). Informed consent was obtained from all study participants, and the study adhered to the tenets of the Declaration of Helsinki.
Disclosure: H. Fujimoto, Alcon (F), Otsuka (F), Kowa (F, P), Santen (F), Novartis (F); S. Ochi, Santen (F); T. Yamashita, Alcon (F); Y. Inoue, Santen (F); J. Kiryu, (F), Kowa (F), Alcon (F), Novartis: (F), Otsuka (F)
Supplementary Materials
Supplementary Video 1. Representative tear interferometer movie using the DR-1α in an eye with narafilcon A silicone hydrogel-soft contact lens. The thin aqueous layer break (TALB) was observed. The colorful interference fringes shortly after eye opening and thin aqueous tear gradually evaporate.
References
- 1.Inoue T, Maeda N, Young LS, et al.. Epithelial pigment slide in contact lens wearers: a possible marker for contact lens-associated stress on the corneal epithelium. Am J Ophthalmol .2001; 131(4): 431–437. [DOI] [PubMed] [Google Scholar]
- 2.Chan WK, Weissman BA.. Corneal pannus associated with contact lens wear. Am J Ophthalmol .1996; 121(5): 540–546. [DOI] [PubMed] [Google Scholar]
- 3.Holden BA, Mertz GW.. Critical oxygen levels to avoid corneal edema for daily and extended wear contact lenses. Invest Ophthalmol Vis Sci .1984; 25(10): 1161–1167. [PubMed] [Google Scholar]
- 4.Dumbleton KA, Woods CA, Jones LW, Fonn D.. Comfort and adaptation to silicone hydrogel lenses for daily wear. Eye Contact Lens .2008; 34(4): 215–223. [DOI] [PubMed] [Google Scholar]
- 5.Dumbleton K, Woods CA, Jones LW, Fonn D.. The impact of contemporary contact lenses on contact lens discontinuation. Eye Contact Lens .2013; 39(1): 93–99. [DOI] [PubMed] [Google Scholar]
- 6.Chirila TV.An introduction to ophthalmic biomaterials and their application through tissue engineering and regenerative medicine. Biomat Regenerat Med Ophthalmol .Cambridge, England, UK: Woodhead Publishing; 2010: 1–13. [Google Scholar]
- 7.Fonn DP, Situ P, Simpson T.. Hydrogel lens dehydration and subjective comfort and dryness ratings in symptomatic and asymptomatic contact lens wearers. Optom Vis Sci .1999; 76(10): 700–704. [DOI] [PubMed] [Google Scholar]
- 8.Efron N, Morgan PB.. Rethinking contact lens-associated keratitis. Clin Exp Optom .2006; 89(5): 280–298. [DOI] [PubMed] [Google Scholar]
- 9.Maldonado-Codina C, Morgan PB, Schnider CM, Efron N.. Short-term physiologic response in neophyte subjects fitted with hydrogel and silicone hydrogel contact lenses. Optom Vis Sci .2004; 81(12): 911–921. [PubMed] [Google Scholar]
- 10.Nichols JJ, Jones L, Nelson JD, Stapleton F, Sullivan DA, Willcox MD.. The TFOS international workshop on contact lens discomfort: introduction. Invest Ophthalmol Vis Sci .2013; 54(11): TFOS1–TFOS6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rohit A, Willcox M, Stapleton F.. Tear lipid layer and contact lens comfort: a review. Eye Contact Lens .2013; 39(3): 247–253. [DOI] [PubMed] [Google Scholar]
- 12.Guillon M, Dumbleton K, Theodoratos P, et al.. Association between contact lens discomfort and pre-lens tear film kinetics. Optom Vis Sci .2016; 93(8): 881–891. [DOI] [PubMed] [Google Scholar]
- 13.Pruitt J, Qiu Y, Thekveli S, Hart R.. Surface characterization of a water gradient silicone hydrogel contact lens (delefilcon A). Invest Ophthalmol Vis Sci .2012; 53(14): 6107. [Google Scholar]
- 14.Tighe BJ.A decade of silicone hydrogel development: surface properties, mechanical properties, and ocular compatibility. Eye Contact Lens .2013; 39(1): 4–12. [DOI] [PubMed] [Google Scholar]
- 15.Dunn AC, Urueña JM, Huo Y, et al.. Lubricity of Surface Hydrogel Layers. Tribol Lett .2013; 49: 371–378. [Google Scholar]
- 16.Belda-Salmerón L, Ferrer-Blasco T, Albarrán-Diego C, Madrid-Costa D, Montés-Micó R. Diurnal variations in visual performance for disposable contact lenses. Optom Vis Sci .2013; 90(7): 682–690. [DOI] [PubMed] [Google Scholar]
- 17.Montés-Micó R, Belda-Salmerón L, Ferrer-Blasco T, Albarrán-Diego C, García-Lázaro S. On-eye optical quality of daily disposable contact lenses for different wearing times. Ophthalmic Physiol Opt .2013; 33(5): 581–591. [DOI] [PubMed] [Google Scholar]
- 18.Varikooty J, Keir N, Richter D, Jones LW, Woods C, Fonn D.. Comfort response of three silicone hydrogel daily disposable contact lenses. Optom Vis Sci .2013; 90(9): 945–953. [DOI] [PubMed] [Google Scholar]
- 19.Varikooty J, Schulze MM, Dumbleton K, et al.. Clinical performance of three silicone hydrogel daily disposable lenses. Optom Vis Sci .2015; 92(3): 301–311. [DOI] [PubMed] [Google Scholar]
- 20.Dursch TJ, Liu DE, Oh Y, Radke CJ.. Fluorescent solute-partitioning characterization of layered soft contact lenses. Acta Biomater .2015; 15: 48–54. [DOI] [PubMed] [Google Scholar]
- 21.Wolffsohn JS, Mroczkowska S, Hunt OA, Bilkhu P, Drew T, Sheppard A.. Crossover evaluation of silicone hydrogel daily disposable contact lenses. Optom Vis Sci .2015; 92(11): 1063–1068. [DOI] [PubMed] [Google Scholar]
- 22.Rex J, Knowles T, Zhao X, Lemp J, Maissa C, Perry SS.. Elemental Composition at Silicone Hydrogel Contact Lens Surfaces. Eye Contact Lens .2018; 44(Suppl 2): S221–S226. [DOI] [PubMed] [Google Scholar]
- 23.Yokoi N, Sakai R, Georgiev GA, Kato H, Sotozono C, Kinoshita S.. Impact of soft contact lens wear on tear film breakup patterns, meniscus tear volume, and tear film stability. Invest Ophthalmol Vis Sci .2018; 59:E–Abstract 1751. [Google Scholar]
- 24.Itokawa T, Suzuki T, Iwashita H, Hori Y.. Comparison and evaluation of prelens tear film stability by different noninvasive in vivo methods. Clin Ophthal. (Auckland, NZ). 2020; 14: 4459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yokoi N, Georgiev GA.. Tear-film-oriented diagnosis for dry eye. Jpn J Ophthalmol .2019; 63(2): 127–136. [DOI] [PubMed] [Google Scholar]
- 26.Young G, Veys J, Pritchard N, Coleman S.. A multi-center study of lapsed contact lens wearers. Ophthalmic Physiol Opt .2002; 22(6): 516–527. [DOI] [PubMed] [Google Scholar]
- 27.Chalmers RL, Begley CG.. Dryness symptoms among an unselected clinical population with and without contact lens wear. Cont Lens Anterior Eye .2006; 29(1): 25–30. [DOI] [PubMed] [Google Scholar]
- 28.Richdale K, Sinnott LT, Skadahl E, Nichols JJ.. Frequency of and factors associated with contact lens dissatisfaction and discontinuation. Cornea .2007; 26(2): 168–174. [DOI] [PubMed] [Google Scholar]
- 29.Schultz CL, Kunert KS.. Interleukin-6 levels in tears of contact lens wearers. J. Interferon Cytokine Res. 2000; 20(3): 309–310. [DOI] [PubMed] [Google Scholar]
- 30.Liu H, Begley C, Chen M, et al.. A link between tear instability and hyperosmolarity in dry eye. Invest Ophthalmol Vis Sci .2009; 50(8): 3671–3679. [DOI] [PubMed] [Google Scholar]
- 31.Situ P, Simpson TL, Jones LW, Fonn D.. Effects of silicone hydrogel contact lens wear on ocular surface sensitivity to tactile, pneumatic mechanical, and chemical stimulation. Invest Ophthalmol Vis Sci .2010; 51(12): 6111–6117. [DOI] [PubMed] [Google Scholar]
- 32.Dogru M, Ward SK, Wakamatsu T, et al.. The effects of 2-week senofilcon—a silicone hydrogel contact lens daily wear on tear functions and ocular surface health status. Cont Lens Anterior Eye .2011; 34(2): 77–82. [DOI] [PubMed] [Google Scholar]
- 33.Pflugfelder SC, Solomon A, Stern ME.. The diagnosis and management of dry eye: a twenty-five-year review. Cornea .2000; 19(5): 644–649. [DOI] [PubMed] [Google Scholar]
- 34.Lemp A.Report of the National Eye Institute/Industry workshop on clinical trials in dry eyes. Eye Contact Lens .1995; 21(4): 221–232. [PubMed] [Google Scholar]
- 35.Guillon M, Patel T, Patel K, Gupta R, Maissa CA.. Quantification of contact lens wettability after prolonged visual device use under low humidity conditions. Cont Lens Anterior Eye .2019; 42(4): 386–391. [DOI] [PubMed] [Google Scholar]
- 36.Del Águila-Carrasco AJ, Ferrer-Blasco T, García-Lázaro S, Esteve-Taboada JJ, Montés-Micó R. Assessment of corneal thickness and tear meniscus during contact-lens wear. Cont Lens Anterior Eye .2015; 38(3): 185–193. [DOI] [PubMed] [Google Scholar]
- 37.Potvin R, Makari S, Rapuano CJ.. Tear film osmolarity and dry eye disease: a review of the literature. Clinical Ophthalmology (Auckland, NZ). 2015; 9: 2039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Awwad ST, Sanchez P, Sanchez A, McCulley JP, Cavanaugh HD.. A preliminary in vivo assessment of higher-order aberrations induced by a silicone hydrogel monofocal contact lens. Eye Contact Lens .2008; 34(1): 2–5. [DOI] [PubMed] [Google Scholar]
- 39.Begley CG, Chalmers RL, Mitchell GL, et al.. Characterization of ocular surface symptoms from optometric practices in North America. Cornea .2001; 20(6): 610–618. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.