

Abstract
Optimal use and distribution of coronavirus disease 2019 (COVID‐19) vaccines involves adjustments of dosing. Due to the rapidly evolving pandemic, such adjustments often need to be introduced before full efficacy data are available. As demonstrated in other areas of drug development, quantitative systems pharmacology (QSP) is well placed to guide such extrapolation in a rational and timely manner. Here, we propose for the first time how QSP can be applied in the context of COVID‐19 vaccine development.
The severe acute respiratory syndrome‐coronavirus 2 (SARS‐CoV‐2) pandemic has catalyzed a remarkable mobilization in vaccine development. The virus genome was sequenced almost instantly after the first cases were identified and new vaccines entered clinical trials within a couple of months, followed by regulatory approval and rollout of national vaccination programs within a year. Most of these vaccines use platform modalities, some like mRNA vaccines approved for the first time, which will enable even more rapid updates following the discovery of new variants.
In the initial stages of COVID‐19 vaccine development, there was little time for extensive optimization of treatment regimen (i.e., dose amount, number of doses, and dosing intervals). To date, most vaccines have progressed successfully from first‐in‐human studies to demonstration of efficacy in the wider population within months. However, often only after regulatory approval and roll‐out in the real world does the critical importance of optimization of dosing regimens become apparent, mainly due to the challenges of balancing limited supply with near‐universal demand in the context of epidemiological and health‐economical outcomes at local and international levels. For example, the United Kingdom Joint Committee on Vaccination and Immunisation (UK JCVI) recommended to extend the interval between the primary and booster doses from the originally approved 3 or 4 weeks to 12 weeks (which at the time of the recommendation had not been tested), thus allowing single dose vaccination of twice the number of people in the first phase of the rollout. 1 Another potential example of a possible area for dose optimization, both in terms of efficacy and supply chain management, is the increased response reported for an arm of an AZD1222 trial where half of the primary dose, followed by a booster dose was tested. 2 In addition, there is growing realization that different vaccines may have to be combined, but it will not be possible to test all possible combinations in actual clinical trials in a timely manner. 3
We anticipate that the requirement for dose optimization will remain when the focus will shift to sustaining long‐term COVID‐19 vaccination programs in the light of emerging new strains for the virus. In addition, due to the wide‐spread roll‐out of vaccination programs and expected drop in COVID‐19 incidence, it will become more difficult to run clinical trials in a timely manner. Recently, we described how quantitative systems pharmacology (QSP) is being used in immuno‐oncology (IO) drug development to address similar challenges (i.e., decreasing access to sufficient number of clinical trial participants and the inability to explore all possible combination therapies and dosing regimens), in a timely manner. 4 We now propose that QSP can be used in a similar manner in COVID‐19 vaccine development and present the first results demonstrating proof‐of‐principle.
QSP focusses on supporting drug development with mechanistic modeling and simulation of underlying biology. A typical QSP model consists of a pharmacokinetic module, describing absorption, distribution, and elimination of the drug, connected to a systems biology model quantitatively describing biology of the disease and mechanisms of drug action. The model (usually expressed as a set of Ordinary Differential Equations), is first parameterized with diverse literature and preclinical data usually available before the start of a drug development project. The model then extrapolates from these data and produces a first hypothesis about efficacious dosing regimens, often before clinical data are available. When a stage of clinical trial is completed, the model is validated, refined, and then applied for extrapolation, thus informing the next stage of the program. Recently, an increasing number of models have reached the maturity required to inform regulatory submission, 5 with most applications in combination with dose selection in IO. 4 In terms of regulatory acceptance, QSP follows the trajectory of physiologically‐based pharmacokinetics (PBPKs), where system‐wide mechanistic models of physiology underlying pharmacokinetics are now routinely used in lieu of clinical trials on drug‐drug interactions and other fields. In an analogous manner, QSP models informed by a fast‐expanding volume of preclinical and clinical data on COVID‐19 immunology and vaccination may be useful for optimization of COVID‐19 vaccine dosing regimens, especially in the context of increasing challenge of clinical subject recruitment and confounding factors. We further discuss QSP and other approaches in the Supplementary Material.
Since 2017, the Immunogenicity QSP Consortium 6 has focused on modeling the formation of anti‐drug antibodies (ADAs), an unwanted immunological response to therapeutic protein drugs. We used the seminal model of Chen, Hickling, and Vicini 7 as a starting point and created a platform model, which has now been validated with ~ 20 clinical compounds. In the wake of the SARS‐CoV‐2 pandemic, we repurposed this model to COVID‐19 vaccines. Because the basic biology of the humoral immune response is the same regardless of whether we simulate an unwanted ADA response to therapeutic proteins or desired immunogenicity to a vaccine antigen, we could quickly repurpose and expand the model by developing a vaccine administration module (See Supplementary Material for more detail). This illustrates an important and at times underestimated feature of QSP—mechanistic platform models can be quickly applied across seemingly unrelated therapeutic areas, which share the same underlying fundamental biology. Likewise, preclinical and clinical data collected in seemingly unrelated projects can be integrated within a single QSP platform and contribute to confidence in its application.
Figure 1 illustrates possible application of the new QSP model to dose regimen selection in mRNA COVID‐19 vaccines. Our example focusses on extrapolation of longitudinal antibody response from phase I/II clinical trial data to dosing intervals, dose amounts, and long‐term vaccination, which have not yet been tested in actual clinical trials. We use the virtual population methodology 8 to generate ensembles of parameter sets (typically referred to as virtual patients), which fall within the range of observed patient variability in 120 days long anti‐receptor binding domain (RBD) IgG titer profiles collected by Widge et al., 9 for individual subjects treated with two 100 μg doses of mRNA‐1273 vaccine administered with an interval of 28 days. Figure 1a shows both the calibration result and a virtual trial showing extrapolation beyond 120 days to examine response durability, as well as the predicted effect of a second 100 μg dose on antibody levels. Importantly, we can quantitatively predict the magnitude of the booster effect produced by vaccination after 11 months and the durability of antibody response in the following year. The calibrated model can then be used to examine different intervals between the first and second dose (Figure 1b). In agreement with the expectation of many immunology experts, 1 and preliminary evidence from a subset of the AZD1222 phase III trial, 2 expansion of the dosing interval is predicted to increase antibody responses. Our model predicts a bell‐shaped response, with an optimum between 7 and 8 weeks (Figure 1b). The 12 weeks interval proposed by UK JCVI is predicted to lead to lower immune response than this predicted optimum, but the expected response is still higher than with the original 28 days interval. Importantly, in the model, the second dose given after 12 weeks still acts as a booster rather than as a new primary dose. A potential downside of extending the time of the dosing interval is that subjects may be left unprotected due to antibodies dropping to low levels before the booster dose is administered. To explore this issue in a quantitative manner, we used convalescent serum concentration as an acceptable level for protection (Figure 1a,b). Although the question of whether IgG levels are a correlate of protection remains subject to debate and investigation, we note that the median convalescent IgG level is very close to the level observed in COVID‐19 vaccine phase III trials between days 10 and 14, the earliest timepoints where placebo and vaccine incidence curves separate 10 (detailed discussion in Supplementary Material). The prolonged exposure of the virus to relatively low level of antibodies may also increase concerns related to the selection of vaccine‐escaping mutant strains, 1 although the modeling of in vivo virus mutation rates over 12 weeks would be needed before drawing conclusions.
FIGURE 1.
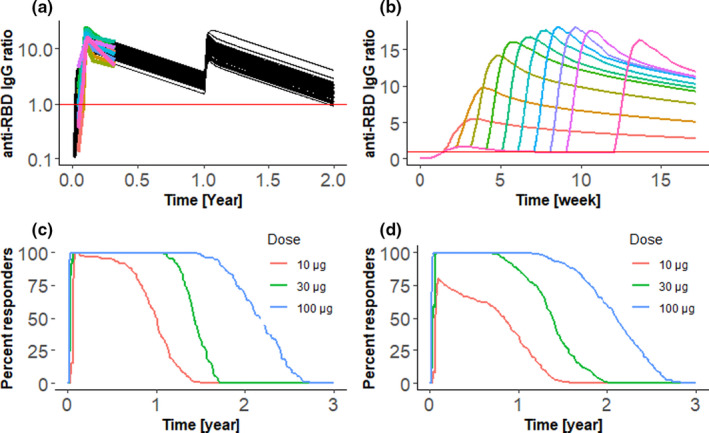
Example application of a quantitative systems pharmacology vaccine model to extrapolate from phase I/II data to different dosing regimens and long‐term vaccination. Plots a and b show ratio of anti‐receptor binding domain (RBD) IgG to the geometric mean of convalescent serum concentrations, plotted by red horizontal line. (a) Calibration with mRNA‐1273 data and extrapolation to annual vaccination. Black lines show simulation results for 85 virtual patients. Colored lines show clinical data available for first 120 days. A 100 ug dose was given at days 0, 28, and 365. (b) Extrapolation to different intervals between primary and booster dose. The model calibrated for mRNA‐1273 vaccine was used to predict antibody response for 100 ug dose administered at intervals of 1–9 and 12 weeks. We plot median IgG ratio of 85 virtual subjects. Administration of second dose leads to burst of antibody production, with the maximum ratio of anti‐RBD IgG to the geometric mean of convalescent serum concentrations following a bell‐shaped curve. (c, d) Extrapolation from phase I/II data on BNT162b2 vaccine to different dose amount in younger (c) and older (d) adults. Two doses were given with 21‐day intervals and amounts of 10, 30, and 100 μg. The 246 and 121 virtual patients were simulated in older and younger age groups. Plots show percent of virtual patients with the anti‐RBD antibody amounts above median convalescent serum concentrations at each time point. Response durability depends on the dose. The 10 μg dose results in a substantially lower antibody response in older individuals
Figure 1c,d illustrate an application of the QSP model to examine the effects of varying dose amounts in different age groups. Whereas QSP is in principle applicable toward mechanistically modeling the aging immune system, we adopted a more phenomenological approach here and created two virtual populations calibrated by the clinical data of Walsh et al., 11 collected separately for younger (18–55 years) and older (65–85 years) adults. Using median convalescent serum concentration as a threshold, we calculated the percent of responding subjects at different time points (Figure 1c,d). Our results show that the antibody response is similar across age groups for 30 and 100 μg doses, consistent with observed high efficacy in older adults. However, lowering the dose to 10 μg is predicted to have a larger negative impact in older adults (Figure 1d).
Another important application of large‐scale mechanistic models is to generate virtual trials that enable the investigation of biomarkers, which were not measured in the actual clinical trials. For example, Figure 2 shows the time profiles of plasma memory B cells and memory CD4 T‐cells simulated by the model calibrated with mRNA‐1273 data (Figure 1a). These results can be used in two ways. First, the model can be subject to additional calibration by other biomarkers than IgG, thus increasing confidence in results. Second, the model validated for biomarker prediction can be used to guide the selection of the most informative biomarkers for clinical investigation.
FIGURE 2.
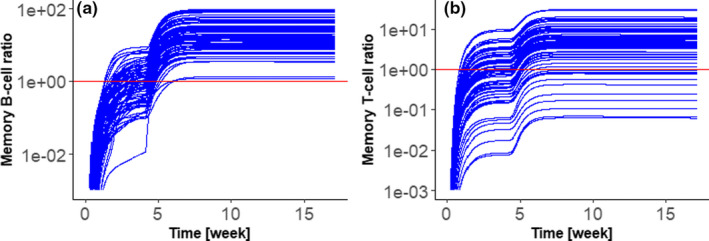
Example application of a quantitative systems pharmacology (QSP) model calibrated by phase I/II data for the investigation of biomarkers, which were not observed in the clinic. The QSP model was calibrated by clinical data for anti‐receptor binding domain (RBD) IgG titers following the administration of 100 μg mRNA‐1273 vaccines to younger adults at day 0 and 28. Calibrated mechanistic model simulates not only antibodies, but also other biomarkers of interest. Here, we plot (a) memory B‐cells and (b) memory CD4 T‐cells in the plasma compartment. Plots show ratios of the number of cells in plasma compartment, to the median number of cells at day 28, before the booster dose was administered. Administration of booster dose increases both B and T cell memory. The model predicts considerable variability of individual responses, especially for T‐cells
In summary, we believe that dose regimen optimization will become increasingly important in ongoing and future development of COVID‐19 vaccines. Is seems clear that the old “trial and error” vaccine development paradigm is inadequate to meet the worlds urgent needs. We therefore propose that, similar to other areas of drug development like IO, 4 running virtual trials ahead of and in parallel with actual clinical trials using QSP models, like the one presented here, should become standard practice in vaccine development.
CONFLICT OF INTEREST
The authors are employees of Certara UK Ltd.
AUTHOR CONTRIBUTIONS
M.G. and R.D. build the model and conducted simulations. R.D. contributed to writing of the manuscript. P.H.v.d.G. and A.M.K. wrote the manuscript.
Supporting information
Supplementary Material
Mario Giorgi and Rajat Desikan contributed equally to this work.
FUNDING INFORMATION
No funding was received for this work.
REFERENCES
- 1. Iacobucci G, Mahase E. Covid‐19 vaccination: what's the evidence for extending the dosing interval? BMJ. 2021;372:n18. [DOI] [PubMed] [Google Scholar]
- 2. Voysey M, Clemens SAC, Madhi SA, et al. Safety and efficacy of the ChAdOx1 nCoV‐19 vaccine (AZD1222) against SARS‐CoV‐2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet. 2021;397:99‐111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Ledford H. Could mixing COVID vaccines boost immune response? Nature. 2021;590(7846):375‐376. [DOI] [PubMed] [Google Scholar]
- 4. Chelliah V, Lazarou G, Bhatnagar S, et al. Quantitative systems pharmacology approaches for immuno‐oncology: adding virtual patients to the development paradigm. Clin Pharmacol Ther. 2021;109(3):605‐618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Zineh I. Quantitative systems pharmacology: a regulatory perspective on translation. CPT Pharmacometrics Syst Pharmacol. 2019;8:336‐339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Kierzek AM, Hickling TP, Figueroa I, et al. A quantitative systems pharmacology consortium approach to managing immunogenicity of therapeutic proteins. CPT Pharmacometrics Syst Pharmacol. 2019;8:773‐776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Chen X, Hickling TP, Vicini P. A mechanistic, multiscale mathematical model of immunogenicity for therapeutic proteins: part 2‐model applications. CPT Pharmacometrics Syst Pharmacol. 2014;3:e134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Allen RJ, Rieger TR, Musante CJ. Efficient generation and selection of virtual populations in quantitative systems pharmacology models. CPT Pharmacometrics Syst Pharmacol. 2016;5:140‐146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Widge AT, Rouphael NG, Jackson LA, et al. Durability of responses after SARS‐CoV‐2 mRNA‐1273 vaccination. N Engl J Med. 2021;384:80‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA‐1273 SARS‐CoV‐2 vaccine. N Engl J Med. 2021;384:403‐416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Walsh EE, Frenck RW, Falsey AR, et al. Safety and immunogenicity of two RNA‐based Covid‐19 vaccine candidates. N Engl J Med. 2020;383:2439‐2450. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material