

Abstract
Objective
This study aimed to develop a model evaluating the role of repeating quarantine instructions and healthy practices among COVID‐19 patients and contact persons at‐home quarantine and to evaluate the instructions' adequacy in decreasing the rate of disease spread with better clinical outcomes.
Methods
A structured questionnaire was distributed to COVID‐19 patients (mild and moderate cases isolated at home) and contacting persons during May and June 2020. Data were collected using a structured online survey collected every five days for three times from each participant. The questionnaire was divided into three sections, consisting of 35 questions for a total possible score of 0 to 35.
Results
A total of 150 valid participant's responses out of 304 participants were obtained. Among the150 total participants, 88 were infected with COVID‐19, and 62 were contacting with COVID‐19 patients. The improvement in the score of awareness and adherence to instructions for the infected patients and their contacts was significantly high in the third questionnaire than in the second and the first questionnaire. The people who live in cities followed the instructions provided at the home quarantine better than those who live in the country. The city patients improved in symptoms better than the country patients. Also, patients followed the instructions better than their contacts. City females adhered to the instructions better than city males. Young people had high awareness score than older people. City people are committed to taking both immune boosters supplements as prophylaxis or prescribed medications on time for treatment more than country people.
Conclusion
This study offers useful insights into factors associated with the role of repeating quarantine instructions and healthy practices to overcome the COVID‐19 pandemic. So, repeating the instructions is important to increase adherence to the instructions, decrease the rate of disease progression and decrease the spread of the infection.
What's known
The role of repeating quarantine instructions and healthy practices between COVID‐19 patients and contact persons at‐home quarantine is very critical in decreasing the rate of disease progress.
What's new
The improvement in the score of awareness and adherence to instructions for the infected patients and their contacts was significantly high in the third questionnaire than the second questionnaire than the first questionnaire.
Repeating the instructions is important to increase adherence to the instructions, decrease the rate of disease progression and decrease the spread of the infection.
1. INTRODUCTION
The coronavirus disease (COVID‐19) is a new viral infection that started in China and caused the infection outbreak in the rest of the world. It is a rapidly spreading virus and is very contagious. 1 , 2 COVID‐19 has attracted wide attention all over the world. 3 The transmission route between people is through airborne droplets, touching or close contact with an infected person or a contaminated surface. 4 That leads to the phenomenon of clustering infection in families and hospitals. 5 Therefore, awareness of quarantine instructions provided by the World Health Organization (WHO) and national governments are fundamental for COVID‐19 patients isolated at home quarantine and their close contacts. to confront the disease and prevent its spread. 6 Since treatment protocols against SARS‐CoV‐2 are still developing, public education and awareness of infection control measures are the mainstays to minimise the viral spread either in health care settings or in the community, 6 especially in countries with limited income resources, where health care systems, at best, have limited capacity to respond appropriately to outbreaks. Thus, management of the pandemic depends mostly on people's adherence to the recommended instructions and measures taken. 5 , 7 , 8 In addition, continuous counselling and repeating instructions to the quarantined COVID‐19 patients and people in close contact with them play a vital role in increasing their awareness, and limiting the spread of infection. 9
Hence, the present work aimed to develop a model evaluating the role of repeating quarantine instructions and healthy practices to increase awareness and practices related to the COVID‐19 quarantine instructions among the COVID‐19 patients, including mild and moderate cases isolated at home and the persons contacting them at home quarantine; also, to evaluate the adequacy of the instructions to attain better clinical manifestations.
2. METHODS
This study was a prospective study that included subjects with reverse transcription‐polymerase chain reaction (RT‐PCR) confirmed COVID‐19 with mild and moderate symptoms, isolated at home. The subjects diagnosed at Beni‐Suef Chest hospital or Beni‐Suef fever hospital then they were quarantined at home and followed by members of the preventive medicine department of the Egyptian ministry of health. The study protocol was approved by the Research Ethical Committee of the Faculty of Pharmacy, Beni‐Suef University (REC‐H‐PhBSU‐20010) and by the Declaration of Helsinki. Participants provided written informed consent. The recruitment of participants was carried out from May to July 2020. Eligible participants were either mild cases with various symptoms including fever, sore throat, cough, malaise, nausea, vomiting, diarrhoea, loss of taste and smell, and normal chest imaging without dyspnoea or moderate cases with abnormal chest imaging, however they have no dyspnoea or shortness of breath. The included participants were isolated at home without the need to be admitted to the hospital. Home contacts of home isolated COVID‐19 patients were also recruited. Participants with any identified psychological, mental illness, or disability that hinder them from following instructions and understanding counselling were excluded from the study. The recruited COVID‐19 patients and their contacts that met eligibility criteria and accepted to participate received an initial 15‐minute direct verbal counselling session about quarantine instructions conducted by a member of the preventive medicine department of the Egyptian ministry of health, in addition to the provision of demonstrative written materials. The intervention included initial repeating quarantine instructions and healthy practices by the home quarantine health team (member of the preventive medicine department of the Egyptian ministry of health) who follow‐up and repeating instructions and healthy practices by home visiting or by telephone. Data were collected using the structured online survey collected every five days for three times from each participant. The questionnaire included 35 items that assessed the participant's level of awareness of the quarantine instructions. All survey assessment questions were developed by the investigators from the instructions provided by the Ministry of Health and the WHO questionnaire. 9 These questionnaires included three main parts to assess their knowledge about the necessary practices. The average time required to fill the questionnaire was 20 minutes.
As shown in Tables 1 and 2, the questionnaire was divided into four sections:
Participants' demographic characters and clinical presentations: (Table 1).
-
Questionnaire about awareness and health practices towards COVID‐19 and home Quarantine Instructions for infected patients and contacting people: (Table 2) which included:
Awareness of the country's efforts to counter COVID‐19.
Home quarantine instructions for infected patients and contacting people.
Instructions for family members of infected patients and contacting people who are at home quarantine.
TABLE 1.
Participants' demographic data
| Characteristic | Number of participants (%) |
|---|---|
| Gender | |
| Male | 83 (55.3%) |
| Female | 67 (44.7%) |
| Age group (years) | |
| 17‐29 | 12 (9.3%) |
| 30‐45 | 107 (71.3%) |
| ≥46 | 31 (20.7%) |
| Educational level | |
| Ignorant | 2 (1.3%) |
| Knows reading and writing | 12 (8%) |
| Sec. school | 21 (14%) |
| Bachelor | 51 (34%) |
| Master/PhD | 12 (8%) |
| Marital status | |
| Unmarried | 35 (23.3%) |
| Married | 93 (62%) |
| Divorced | 12 (8%) |
| Widower | 10 (6.7%) |
| Current place of residence | |
| City | 92 (61.3%) |
| Country | 58 (38.6%) |
| Occupation | |
| Unemployed | 35 (23.3%) |
| Employed | 115 (76.7%) |
TABLE 2.
Questionnaire of awareness and health practices towards COVID‐19 Home Quarantine Instructions for infected patients and contacting people
| Questions | Options |
|---|---|
| I: Awareness of the country's efforts to counter COVID‐19 | |
| Q1: The Egyptian Ministry of Health provided fast and reliable data on the number of people infected and deaths with COVID‐19 | True, False, I don't know |
| Q2: The media play a vital role in informing Egyptians of COVID‐19 and virus prevention methods | True, False, I don't know |
| Q3: Is the result of the information provided by the social media regarding the infection with Corona virus, the Egyptian community in the village started to follow the government's instructions despite its hardness | True, False, May be |
| Q4: How satisfied are you with the hospital services in the area where you live | Not satisfied, Neutral, Satisfied |
| II: Home Quarantine Instructions for infected patients and contacting people | |
| Q5: Are you committed not to leave the house for the duration of the self‐isolation period? | Yes, No, To some extent |
| Q6. Is there a family member who is healthy and does not suffer from chronic diseases and is caring for you? | |
| Q7: Do you care about house cleanliness and good ventilation of rooms? | Yes, No, To some extent |
| Q8: Do you care about disinfection of surfaces that are touched using disinfectants such as chlorine (0.5%) while wearing rubber gloves during cleaning | Yes, No, To some extent |
| Q9: During sneezing or coughing, do you cover the nose and mouth with disposable tissues, then dispose of it by placing it in a bag that is closed, and then wash your hands immediately with soap and water? | Yes, No |
| Q10: Do you wash your hands frequently with soap and water for at least 20 s? | Yes, No |
| Q11: Do you avoid touching the eyes, nose and mouth with unwashed hands? | Yes, No |
| Q12: Do you avoid sharing personal household items such as dishes, cups, towels, bedding or clothes with other family members? | Yes, No, To some extent |
| Q13: Do you commit to eating meals separately from family members? | Yes, No |
| Q14: Do you maintain a balanced diet without fats, oil and sugar? | Yes, No, To some extent |
| Q15: Do you drink a lot of fluids? | Yes, No |
| Q16: Do you drink warm water instead of cold drinks? | Yes, No |
| Q17: Do you eat vegetables and fruits a lot? | Yes, No |
| Q18: Do you avoid excessive or inappropriate use of antibiotics? | Yes, No |
| Q19: Do you measure the temperature every 8 h? | Yes, No |
| Q20: Do you use vitamins D and A to strengthen the immune system? | Yes, No |
| Q21: Do you use omega‐3 to strengthen immunity? | Yes, No |
| Q22: Are you committed to taking your prescribed medication on time for treatment or to prevent the virus? | Yes, No, To some extent |
| Q23: As a result of your commitment to health guidelines and taking medications prescribed for you regularly | I feel better symptoms of corona |
| I feel an increase in the symptoms of corona | |
| I don't feel any improvement in the symptoms of corona | |
| No symptoms were reported during the isolation period | |
| Q24: If it is necessary to go to the hospital, will you keep wearing the mask and avoid public and crowded transportation as possible? | Yes, No |
| III: Instructions for family members of infected patients and contacting people who are at home quarantine | |
| Q25: Family members are committed to remain in a room other than the isolated person as much as possible and to keep at least two meters away in case of mixing | Yes, No, To some extent |
| Q26: The rest of the family is committed to use a separate sleeping room and a separate bathroom, if available | Yes, No |
| Q27: Does the family prevent visitors who do not have a basic need to be at home? | Yes, No, To some extent |
| Q28: Do family members have to wear a medical mask when they are near an isolated person (for example when entering his room)? Dispose of it after use by placing it inside a sealed bag and throwing it in the trash? | Yes, No, To some extent |
| Q29: During sneezing or coughing, do the rest of the family members commit to covering the nose and mouth with disposable tissues, then they are disposed of by placing them inside a bag that is closed and then their hands are washed immediately with soap and water? | Yes, No, To some extent |
| Q30: Do family members have to wash their hands frequently with soap and water for at least 20 s? | Yes, No, To some extent |
| Q31: Can the rest of the family members avoid touching their eyes, nose and mouth with unwashed hands? | Yes, No, To some extent |
| Q32: Do the rest of the family avoid sharing personal household items such as dishes, cups, towels, bedding, or clothing with the isolated person? | Yes, No, To some extent |
| Q33: Do family members care about disinfection of surfaces that are touched using disinfectants such as chlorine (0.5%), while wearing rubber gloves during cleaning | Yes, No, To some extent |
| Q34: Do family members make sure that the shared spaces in the house have good ventilation? | Yes, No, To some extent |
| Q35: Does the family avoid mixing and crowded places? | Yes, No, To some extent |
2.1. Evaluation of the answers
Answers to the last three parts of the questionnaire were recorded as (Yes), (No) and (To some extent). The person was given a score = 1 if he/she gave the correct answer for the question and a zero score if he/she fails to provide the correct answer to end up with a total range from 0 to 35. Finally, the participants were classified according to the quarantine instructions awareness if he/she scored >28 out of 35 (>80%) points. 10 , 11 , 12 , 13 The estimation of the minimum required sample size was carried out using G* power 3.1 software. The calculations were performed based on a 50% anticipated probability of positive response and good knowledge, with a 95% confidence interval and precision limit of 5%.
2.2. Statistical analysis
Statistical analysis and data visualisation were performed in GraphPad Prism (V.7.00, San Diego, CA, USA) and R statistical platform (https://www.r‐project.org) with ggplot2 package. Values of P ≤ .05 were statistically significant. The normality of data was assessed before running the analysis. Repeated measures models were applied using a generalised estimating equation (GEE) rather than mixed models to minimise the problems of convergence. Wilcoxon matched‐pairs signed‐rank and Mann‐Whitney tests were used to evaluating the overall response and awareness scores during the three questionnaires in between participants. Friedman test was used to evaluate the participants' scores in different variables. Data modelling using Design Expert 7.0.0 (Stat‐Ease Inc, Minneapolis, MN, USA) with model inputs (Age, gender, level of education, and the number of individuals in each family) and output (Score).
3. RESULTS
3.1. Participants' demographics
A total of 304 subjects were recruited into the study, however, only 150 eligible participants completed the study. About 25% of the withdrawn subjects reported failure to respond due to technical problems, while the remainder withdrew without giving reasons. Among the 150 total participants, 88 (58.6%) were infected with COVID‐19, and 62 (41.3%) were in contact with COVID‐19 patients. The demographics of the included subjects are shown in Table 1. Most of the participants were in the age group of 30 to 45 years and 55.3% of them were males. The respondents included different educational levels ranged between those with bachelor's degrees and lower levels.
The questionnaire included 20 questions for the evaluation of the patient's knowledge and commitment to the quarantine instructions in addition to 15 questions for family members at home quarantine (Table 2). Generally, counselling visits resulted in higher awareness scores among COVID‐19 patients and their contacts and most participants responded positively to the activity performed either by phone or by the online questionnaire. The overall change in the reported responses by participants across the three counselling visits showed a statistically significant increase (P < .001) for both confirmed cases and contacts, as shown in Figure 1.
FIGURE 1.
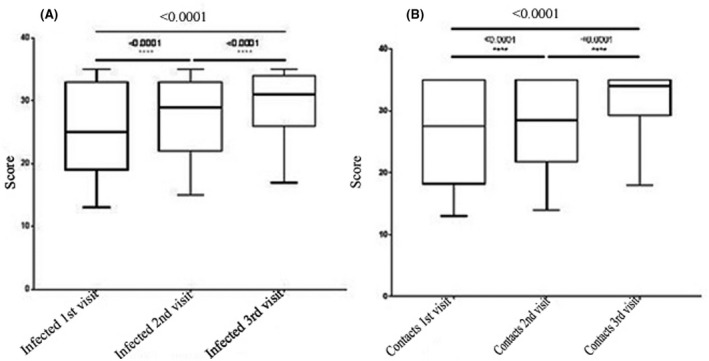
Box plots showing improved awareness scores during successive questionnaires for (A) all infected patients and (B) all contact people
3.2. The effect of demographic variables on awareness scores
A total of 58 (38.6%) subjects included both infected cases and their contacts were rural residents. The mean awareness scores after the three consecutive visits for patients and their contacts who lived in the city differed significantly from those living in the country and the estimated p‐value was P < .001 and P = .0072, respectively, as shown in Figure 2.
FIGURE 2.
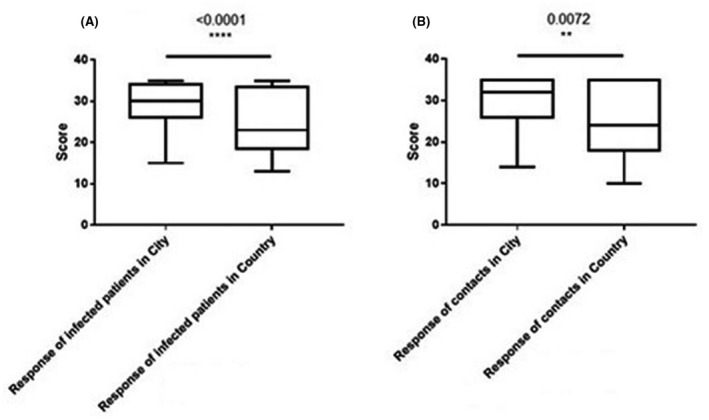
Box plots showing the overall response and awareness scores during the three questionnaires between (A) infected patients in the city compared with the country, and (B) contacts people in the city compared with the country
However, the answers to the questionnaire showed evidence of ceiling effect, since the majority of responses were at the maximum possible levels. The association between the participants' scores and the different demographic parameters was performed. There were significant differences in the achieved awareness scores between respondents depending on gender, age, educational levels, employment status, and marital status (P < .05). Multivariate analyses revealed that city residents with education levels higher than high school and employed regardless of gender had significantly higher scores in awareness (P < .05). However, contacts showed lower awareness scores after the completion of the counselling visits; especially for rural residents regardless of age, gender, occupation and marital status.
Most of the participants (92.5%) had confidence in the governmental regulations and the Egyptian ministry of health services such as hotline and healthcare settings, while 7.5% had no such confidence. Moreover, the attitude of confidence differed significantly across the included participant's categories of educational levels, occupation and marital status (P < .05).
Data modelling showed that the older the patient or the contact persons the lower the total score as demonstrated in Figure 3. For the COVID‐19 group, this decrease in score with increasing age was comparable between both genders, while for the contact persons the level decrease more for males with increasing age compared with females that maintained high score levels with increasing age. Also, the effect of education level resulted in a strong increase in the score for higher levels of education for both genders regarding the COVID‐19 group as demonstrated in Figure 4. The number of individuals for each family showed a great effect on the total score, the greater the number of individuals in each family the lower the score level regarding females while males showed no significant difference as demonstrated in Figure 5.
FIGURE 3.
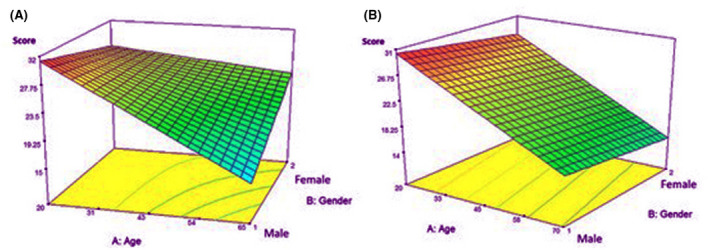
A response surface plot represents the relationship between age and gender compared with the total score for both groups; (A) for contacts, (B) for patients
FIGURE 4.
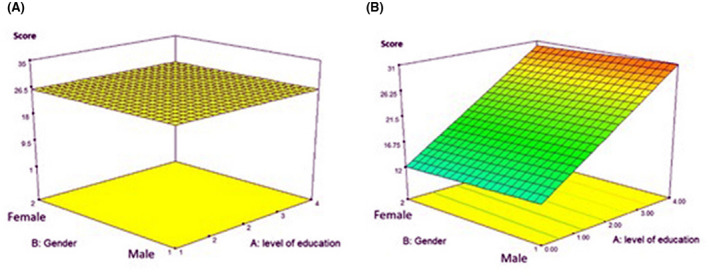
A response surface plot represents the relationship between gender and level of education (the higher the level of education the higher the encoded number) compared with the total score for both groups; (A) for contacts, (B) for patients
FIGURE 5.
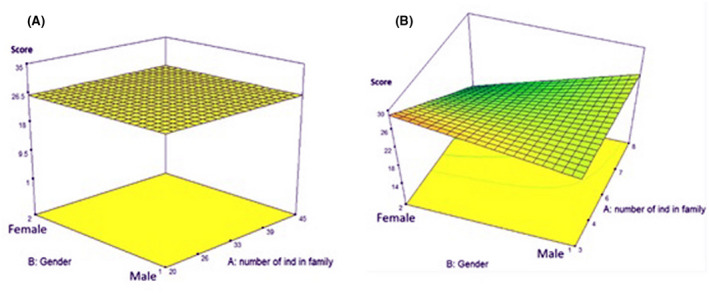
A response surface plot represents the relationship between gender and the number of individuals in each family compared with the total score for both groups; (A) for contacts, (B) for patients
4. DISCUSSION
The present study was conducted among COVID‐19 patients and their home contacts. Overall, a COVID‐19 counselling visits intervention had a significant impact on the levels of awareness about quarantine instructions and healthy practices. Since there is a lack of medical cure for the pandemic, the global response is based on self‐hygiene such as hand washing in addition to public health strategies such as minimisation of social gatherings and home quarantine for both infected and their contacts. These strategies are fundamental to control the spread of the virus and to reduce the burden of the outbreak. 14 In this predominantly male with fairly high education and city residents, we found a mean increase of knowledge and awareness scores of around 30% after the completion of three consecutive visits.
We analysed the data to recognise predictors for those participants who responded positively to the counselling visits and found that participants who lived in the rural community were less likely to respond to the intervention with significantly lower awareness scores compared with city residents. Since most of the country residents showed improper attitudes toward infection control practices including disinfection of surfaces that were touched, covering mouth and nose while sneezing or coughing using a disposable tissue, and sharing personal tools. This is maybe due to the lower education levels and the lack of technology for the people who live in the country since highly educated persons can get knowledge from different sources compared with low educated ones. 7 Therefore, their achieved awareness scores were markedly less than those of city inhabitants. Thus, they needed more frequent repetition of quarantine instructions and healthy practices to increase awareness about self‐hygiene and home hygiene. 15
The infected patients showed higher commitment to the quarantine instructions and proper medication use, in contrast to the contacts that showed a significantly lower awareness score. This behavior may be explained in the light of the idea that most of the contacts who participated in the study were not categorised as vulnerable populations since they did not fulfil the risk factors identified for severe COVID‐19 such as elderly or presence of comorbidities. Moreover, the burden of psychological depression and loneliness resulted from quarantine instructions hindered most of the contacts against responding to the instructions and avoid social gatherings; maybe also because they were not infected. Yet, so they did not pay attention to adhere to the instructions.
Consequently, infected patients from the city felt better symptoms of COVID‐19, since they were committed to health guidelines and taking the prescribed medications on time for treatment more than the country patients.
The significant improvement in awareness score and adherence to instructions concerning the infected married male and their contacts through the three questionnaires was obvious. This perception can be attributed to the financial output of the pandemic and the quarantine, and their fear of what is at risk from mandatory unemployment.
Even though the results may be altered as a consequence of the ceiling effect in which the responses tend to cluster towards the upper end of responses, the present study results were consistent with several studies which reported the positive effect of repeated counselling on awareness scores and adherence to instructions. 15 , 16 , 17
Most of the participants in this study (about 76.7%) were employed, but they showed no significant difference in the score compared with unemployed patients. This may be due to their limited resources in addition to the psychological consequences of not working during the pandemic which causes their lack of interest in the instructions.
From data modelling findings, there was an inverse relationship between increasing age and the level of score. Young people have a high score of awareness than elderly people. Moreover, with a certain high infection and death rate in the elderly, it was essential to care for the health status of older close contacts during the quarantine period. 16 , 17 That is noticeable in infected patients for both genders, however, female contacts showed unusually high awareness score levels with increasing age. The explanation for this phenomenon may be due to their psychological stability, desire for life and their fear of being infected. Besides, it was observed that people who have many members in their families had a lower level of awareness score because they were more vulnerable to infection from crowding than a low family member.
From all participants who live in the country, the age group 45‐59 years is the only group that showed a significant improvement in their score's questionnaire upon the application of repeating quarantine instructions and healthy practices questionnaires. This group was committed to the instructions, keeping social distance, and staying home. The same was reported in a cross‐sectional study in the united states. 15 From all infected participants who live in the city, the age group 30‐44 years and the age group 60‐80 years are the groups who showed a significant difference in the score between questionnaires because they were concerned about their health and wanted to recover quickly. However, their contacts showed no significant difference in the score between questionnaires as it seemed that they were not paying attention to the infection.
It was shown before that when we know how the infection is transmitted and what the preventive instructions are; the spread of the infection decreases. 18 , 19 Most of the participants knew that the cause of their infection resulted from gathering with contacts and social workers. This indicates the high awareness of the Egyptian people about the COVID‐19 disease by the online information, social media and follow‐up by the Ministry of Health to COVID‐19 patients and their contacting persons. 20
Most of the participants had high confidence about the vital role of the government and international organisations to overcome the pandemic. The majority of them, around (92%), trusted the Egyptian ministry of health and WHO. in providing reliable and fast information about the number of people infected and deaths with the COVID 19, while the minority (7.5%) had no such confidence and believe that corona represents a social stigma in Egypt. They also follow the WHO and the Ministry of Health during this period to limit the spread of coronavirus infection; and agreed with the media in informing the public about infection and awareness about the quarantine instructions. 21 , 22 , 23 , 24 As the media enters every home and affects people, it is useful to develop the instructions through the media to reach the maximum benefit. 25
The strength points of this study lie in the adequate assessment of awareness and practices toward COVID‐19 which was developed by in‐depth personal interviews and follow‐up and the application of multi‐dimensional measures; in addition to randomisation of the recruited population.
5. LIMITATIONS
The study included skilful populations in smartphone use and software technology. Some rural populations have limited resources and are devoid of these skills, especially elderly ones. Patients with severe cases who needed to be admitted to the hospital are excluded from the study. Besides, there is no long‐term follow‐up to evaluate the clinical outcomes of this conducted survey.
6. CONCLUSION
This study offers useful insights into factors associated with the role of repeating quarantine instructions and healthy practices in increasing the COVID‐19 instructions awareness and practices to improve the infected cases and decrease the spread and transmission of the infection through the community. The improvement in the score of awareness and adherence to instructions for the infected patients and their contacts was significantly high in the third questionnaire than the second questionnaire than the first questionnaire. The people who live in cities follow the instructions provided to them at the home quarantine, are committed to taking the prescribed medication on time for treatment and so showed improvement in symptoms better than those who live in the country. Also, patients follow the instructions better than their home contacts do. City females adhere to the instructions better than city males. Young people have high score awareness than older people.
DISCLOSURE
No conflict to declare.
AUTHOR CONTRIBUTIONS
Conception and design: Mohamed EA Abdelrahim. Administrative support: All authors. Provision of study materials or patients: All authors. Collection and assembly of data: All authors. Data analysis and interpretation: All authors. Manuscript writing: All authors. Final approval of manuscript: All authors.
Elgendy MO, Abdelrahman MA, Osama H, El‐Gendy AO, Abdelrahim MEA. Role of repeating quarantine instructions and healthy practices on COVID‐19 patients and contacted persons to raise their awareness and adherence to quarantine instructions. Int J Clin Pract. 2021;75:e14694. 10.1111/ijcp.14694
DATA AVAILABILITY STATEMENT
The datasets analysed during the current study are available from the corresponding author on reasonable request.
REFERENCES
- 1. Meng L, Hua F, Bian Z. Coronavirus disease 2019 (COVID‐19): emerging and future challenges for dental and oral medicine. J Dent Res. 2020;99(5):481‐487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Sayed AM, Khalaf AM, Abdelrahim MEA, et al. Repurposing of some anti‐infective drugs for COVID‐19 treatment: a surveillance study supported by an in silico investigation. Int J Clin Pract. 2021;75(4):e13877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565‐574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Khader Y, Al Nsour M, Al‐Batayneh OB, et al. Dentists’ awareness, perception, and attitude regarding COVID‐19 and infection control: cross‐sectional study among Jordanian dentists. JMIR Public Health Surveill. 2020;6(2):e18798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Wang Y, Di YU, Ye J, et al. Study on the public psychological states and its related factors during the outbreak of coronavirus disease 2019 (COVID‐19) in some regions of China. Psychol Health Med. 2021;26(1):13‐22. [DOI] [PubMed] [Google Scholar]
- 6. Cook TM, El‐Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID‐19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia. 2020;75(6):785‐799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Al‐Mohrej OA, Al‐Shirian SD, Al‐Otaibi SK, Tamim HM, Masuadi EM, Fakhoury HM. Is the Saudi public aware of Middle East respiratory syndrome? J Infect Public Health. 2016;9(3):259‐266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. La V‐P, Pham T‐H, Ho M‐T, et al. Policy response, social media and science journalism for the sustainability of the public health system amid the COVID‐19 outbreak: the Vietnam lessons. Sustainability. 2020;12(7):2931. [Google Scholar]
- 9. Elbur A, Alharthi A, Aljuaid A, et al. Knowledge of Middle East respiratory syndrome coronavirus (MERS‐CoV) and its management: a survey among Saudi people in Taif; Kingdom of Saudi Arabia. IOSR J Pharm. 2016;6(8):33‐39. [Google Scholar]
- 10. Al‐Tawfiq JA, Zumla A, Gautret P, et al. Surveillance for emerging respiratory viruses. Lancet Infect Dis. 2014;14(10):992‐1000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Mohamed MB, Mahmoud MA. Effects of educational program on MERS‐corona‐virus among nurses students at Jazan University. International Journal of Advance Research, Ideas and Innovations in Technology. 2017;4(1):618‐625. [Google Scholar]
- 12. Alghamdi IG, Hussain II, Almalki SS, Alghamdi MS, Alghamdi MM, El‐Sheemy MA. The pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia: a descriptive epidemiological analysis of data from the Saudi Ministry of Health. Int J Gen Med. 2014;7:417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Mackay IM, Arden KE. MERS coronavirus: diagnostics, epidemiology and transmission. Virol J. 2015;12(1):1‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Rabbani SA, Mustafa F, Mahtab A. Middle East Respiratory Syndrome (MERS): awareness among future health care providers of United Arab Emirates. Int J Med Public Health. 2020;10(1):8‐13. [Google Scholar]
- 15. Li S, Feng BO, Liao W, et al. Internet use, risk awareness, and demographic characteristics associated with engagement in preventive behaviors and testing: cross‐sectional survey on COVID‐19 in the United States. J Med Internet Res. 2020;22(6):e19782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Chen D, Song F, Tang L, et al. Quarantine experience of close contacts of COVID‐19 patients in China: a qualitative descriptive study. Gen Hosp Psychiatry. 2020;66:81‐88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Abdelhafiz AS, Alorabi M. Social stigma: the hidden threat of COVID‐19. Front Public Health. 2020;8:429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Liu Y, Yan L‐M, Wan L, et al. Viral dynamics in mild and severe cases of COVID‐19. Lancet Infect Dis. 2020;20(6):656‐657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Khan MU, Shah S, Ahmad A, Fatokun O. Knowledge and attitude of healthcare workers about middle east respiratory syndrome in multispecialty hospitals of Qassim, Saudi Arabia. BMC Public Health. 2014;14(1):1‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Elgendy MO, Abd Elmawla MN, Abdel Hamied AM, et al. COVID‐19 patients and contacted person awareness about home quarantine instructions. Int J Clin Pract. 2021;75(4):e13810. [DOI] [PubMed] [Google Scholar]
- 21. Zawbaa HM, El‐Gendy A, Saeed H, et al. A study of the possible factors affecting COVID‐19 spread, severity and mortality and the effect of social distancing on these factors: Machine learning forecasting model. Int J Clin Pract. 2021;75(6):e14116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Kamal M, Abo Omirah M, Hussein A, et al. Assessment and characterisation of post‐COVID‐19 manifestations. Int J Clin Pract. 2021;75(3):e13746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Saeed H, Osama H, Madney YM, et al. COVID‐19; current situation and recommended interventions. Int J Clin Pract. 2021;75(5):e13886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Osama El‐Gendy A, Saeed H, Ali AMA, et al. Bacillus Calmette‐Guérin vaccine, antimalarial, age and gender relation to COVID‐19 spread and mortality. Vaccine. 2020;38(35):5564‐5568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Elgendy MO, El‐Gendy AO, Abdelrahim ME. Public awareness in Egypt about COVID‐19 spread in the early phase of the pandemic. Patient Educ Couns. 2020;103(12):2598‐2601. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets analysed during the current study are available from the corresponding author on reasonable request.