

Abstract
OBJECTIVES:
The aim of the study was to clinically evaluate and compare 0.016-inch superelastic nickel–titanium (NiTi) and 0.016-inch heat-activated nickel–titanium (NiTi) archwires in terms of alignment efficiency, root resorption, and pain intensity.
METHOD:
A total of 20 patients requiring fixed orthodontic treatment, having Little's irregularity index of 5–8, and requiring first premolar extractions were recruited. They were randomly allocated to receive two different archwires (0.016-inch superelastic NiTi or 0.016-inch thermoelastic NiTi). Good-quality impressions were taken of the lower arch before archwire placement (T0) and at every month after that till the alignment was complete. The rate of tooth alignment was measured on casts by determining Little's irregularity index. The pain experienced by the patient was assessed 24 hours and 1 week after the placement of the archwire on a visual analogue scale. Cone beam computed tomographic radiographs of lower anterior teeth were taken before and after alignment to assess root resorption. Data obtained were subjected to statistical analysis using the SPSS software (version 20.0). The level of significance was kept at 5%.
RESULTS:
The repeated measures ANOVA indicated that there was no significant difference in the aligning efficiency of superelastic and heat-activated NiTi wires. (p = 0.45). The Mann Whitney U test showed that superelastic NiTi wires had statistically significant higher VAS scores than heat-activated NiTi at 24 hours and 1-week interval (p < 0.05). Student's t-test indicated greater root resorption with superelastic NiTi but the difference was not statistically significant.
CONCLUSION:
Both the wires showed similar aligning efficiency and resulting root resorption. Superelastic NiTi was observed to produce more pain compared to heat-activated NiTi in the aligning phase.
Keywords: Arch wire, alignment, root resorption
Introduction
The first step of fixed orthodontic treatment constitutes alignment and leveling of the teeth. This can generally be achieved by crown tipping without any significant root movement.[1]
In orthodontics, it has become a generally accepted concept that light, continuous forces are necessary to achieve functional and regulated movement of the tooth with minimal adverse effects on the teeth and surrounding structures.[2]
Initial archwires are the wires used for initial leveling and alignment that must be flexible and transmit light forces with a wide range of activation.[3] A variety of wire materials have been developed to provide a force–deflection curve with a definite platform and a wide range of activation.[4]
Because of their low flexural rigidity, high spring back, and superelasticity, NiTi archwires have many advantages over other wires for initial alignment.[5]
Superelastic NiTi has a transition temperature range (TTR) below room temperature while thermoelastic NiTi wires have TTR close to body temperature. This control of the transition temperature range is possible due to the addition of copper to nickel and titanium.[5] Stress-induced phase transformation in superelastic NiTi is observed only in areas of severe crowding while the true shape memory effect is temperature dependent. Therefore, it can be assumed that thermoelastic alloys exhibiting the true shape memory effect would produce lighter forces as compared to superelastic NiTi.[6]
Several in vitro studies have demonstrated these desirable properties in a controlled laboratory environment. However, in vitro tests, no matter how complicated, cannot fully predict the clinical performance of the archwires, which is more important for orthodontists and their patients.
Fear of pain has been reported to be a key factor in discouraging patients from seeking treatment with orthodontics.[7] Orthodontic tooth movement leads to an inflammatory response in the periodontium and dental pulp stimulating the release of different biochemical mediators which causes the sensation of pain. Orthodontic pain is experienced by a majority of patients 4 to 24 hours after archwire placement which usually lasts for 2–3 days and gradually disappears after 5 days.[8] It has been suggested that lighter forces reduce tissue trauma and patient discomfort. However, there has been limited research regarding the discomfort caused by these archwires.
Apical root resorption that commonly occurs during orthodontic treatment is of great concern to the orthodontist.[9] Its etiology is multifactorial and may be associated with individual biological variability, genetic predisposition, the effect of mechanical factors, root morphology, and tooth injuries sustained before orthodontic treatment. The higher forces for a prolonged duration are also known to result in greater root resorption[10] Therefore, the knowledge of the extent of forces exerted by the archwire and the resulting root resorption is necessary to allow the clinician to make an informed choice.
Systematic analyses concluded that earlier research on the efficiency of aligning archwires posed a high risk of bias, a brief follow-up duration, and did not mention any adverse consequences such as pain and root resorption.[11,12] According to systematic reviews, there is insufficient evidence to determine whether any of the archwires evaluated are better or worse in terms of rate of alignment, root resorption, or pain experienced by patients when compared to another.
Hence, the purpose of this study was to evaluate the rate of alignment, root resorption, and pain intensity using two different initial aligning archwires, i.e., superelastic Ni-Ti archwires and heat-activated NiTi archwires.
Materials and Methods
According to the power analysis (PASS 11, Kaysville, Utah, USA) for an independent t -test with a significance level of 0.05 and power of 80%, the sample size required was seven per group. Three additional subjects per group were recruited in case of subject attrition.
A total of 20 patients were chosen to enroll in the study on the basis of the following criteria:
15–25 years of age, with crowding in the lower anterior segment providing a mandibular irregularity index 5–8 requiring fixed orthodontic treatment with first premolar extraction. Only patients with no relevant medical history or recent history of intake of drugs such as nonsteroidal antiinflammatory drugs were included.
Patients with systemic diseases, active periodontal disease, spacing in the lower anterior region, and previous orthodontic treatment were excluded.
The project was approved by the Institutional Ethical Committee. (ITSCDSR/L/2019/005).
The patients involved in the sample were bonded with MBT brackets (0.022 × 0.028 in slot) and assigned randomly to two categories, 0.016-inch heat-activated Ni-Ti (Test group A) and 0.016-inch superelastic NiTi wire (test group B) using sealed opaque envelopes to prevent bias in the distribution. Allocation of wires during the evaluation phase was hidden from the investigator and the researchers and no other wire was used during the whole analysis.
The rate of alignment was assessed in the mandibular arch using Little's Irregularity Index (LI). Good-quality alginate impressions were taken at the prealignment phase (T0). After the placement of bonded attachments and bands, the aligning archwire was placed using elastomeric ligatures. The patient was recalled every month and impressions taken. Dental casts were prepared for each stage. This procedure was repeated until the completion of anterior alignment (LI = 0). [Figures 1-4].
Figure 1.

Patient photograph and dental cast immediately after the placement of the archwire
Figure 4.

Measuring the irregularity index using Vernier caliper
Figure 2.

Patient photograph and dental cast 1 month after the placement of the archwire
Figure 3.

Patient photograph and dental cast 2 months after the placement of the archwire
Pain perception of the patients was recorded after 24 hours and 1 week after the placement of the archwire on a visual analog scale.
Small field-of-view cone beam computed tomography scans of the patients were taken before and after the completion of the aligning phase of the treatment to determine the amount of root resorption [Figures 5 and 6].
Figure 5.
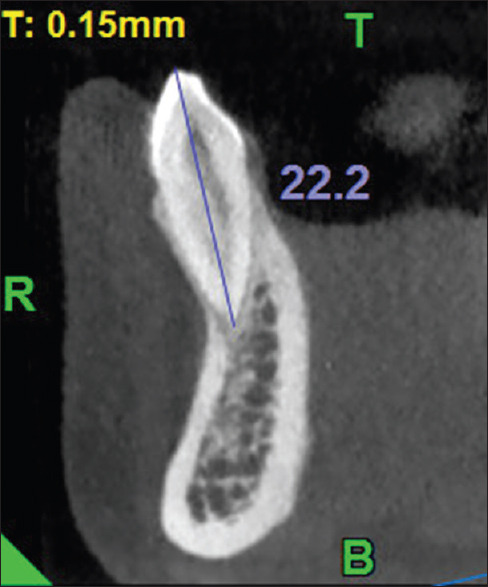
Measurement the root length on the sagittal section of CBCT before treatment
Figure 6.
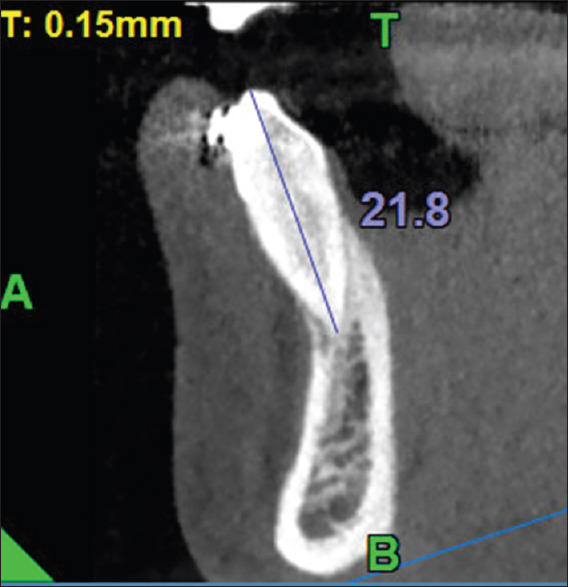
Measurement the root length on the sagittal section of CBCT after alignment
The maximum linear length between the cusps and root apex was estimated at 0.25-mm isometric voxel using multiplanar axial reconstruction. For sagittal or coronal multiplanar reconstruction, the distances between the reference points (incisal edge/cusp tip and root apex) were marked, providing measurements in millimeters. The measurements were rendered in pre- and postalignment CBCT of all the lower anterior teeth.
The maximum linear length between cusps and root apex was measured using axial multiplanar reconstruction at 0.25 mm isometric voxel. The distances between the reference points (incisal edge/cusp tip and root apex) were marked in the sagittal or coronal multiplanar reconstruction, providing measurements in millimeters. The measurements were made for all lower anterior teeth in pre and postalignment CBCT.
Results
A total of 20 patients were included in the study. In total, the sample included six males and 14 females. The mean age of patients was 18.7 ± 3.30 years in the heat-activated NiTi group and 19 ± 4.03 in the superelastic NiTi group. The results were tabulated and subjected to statistical analysis (SPSS 20.0, SPSS Inc, Chicago, Illinois). The intraexaminer reliability for recording LI was evaluated using the intraclass correlation coefficient [Table 1] and found to be high (ICC = 1). Table 2 shows the rate of alignment of both the groups over the study period. The reduction in LI was highest in the first month in both the groups, 2.88 ± 0.31 mm in heat-activated NiTi and 2.33 ± 0.66 mm in superelastic NiTi. Thereafter, the rate of alignment decreased till the completion of alignment in about four months. To compare the rate of alignment, measured as a reduction in LI, at different time intervals between superelastic NiTi and heat-activated NiTi, repeated-measures ANOVA was used. It was revealed in RM ANOVA that the time interval was the only statistically significant different factor while groups and interaction of time with groups were not significant. [Table 3] Root resorption in the lower anterior teeth was compared using the student's t-test and it was found to be generally higher for superelastic Ni-Ti in all the teeth except in the lower right incisor [Table 4]. The lower right canine showed the highest amount of root resorption in the superelastic group (0.75 ± 0.46 mm) and the lower right central incisor in the heat-activated group (0.64 ± 0.18 mm). However, root resorption did not differ significantly between the two groups for any tooth.
Table 1.
Intraclass correlation coefficient to determine interexaminer reliability
| Intraclass Correlation | 95% Confidence Interval | F Test with True Value 0 | |||||
|---|---|---|---|---|---|---|---|
|
|
|
||||||
| Lower Bound | Upper Bound | Value | df1 | df2 | Sig | ||
| Single measures | 1.00 | 0.99 | 1.00 | 1557.00 | 4 | 5 | 0.00 |
| Average measures | 1.00 | 1.00 | 1.00 | 1557.00 | 4 | 5 | 0.00 |
One-way random effects model where people effects are random. ICC value 1 shows a high degree of interexaminer reliability
Table 2.
Descriptive statistics of the rate of alignment using superelastic Ni-Ti and heat-activated Ni-Ti over the study time period
| Time interval | Group | n | Mean±SD reduction in L.I (mm) | 95% CI | |
|---|---|---|---|---|---|
|
| |||||
| Upper limit | Lower limit | ||||
| T0-T1 | Heat-activated Ni-Ti | 10 | 2.88±0.31 | 3.07 | 2.69 |
| Superelastic NiTi | 10 | 2.33±0.66 | 2.74 | 1.92 | |
| T1-T2 | Heat-activated Ni-Ti | 10 | 2.04±0.85 | 2.57 | 1.51 |
| Superelastic NiTi | 10 | 2.05±0.99 | 2.66 | 1.44 | |
| T2-T3 | Heat-activated Ni-Ti | 10 | 0.79±0.93 | 1.37 | 0.21 |
| Superelastic NiTi | 10 | 0.74±0.79 | 1.23 | 0.25 | |
| T3-T4 | Heat-activated Ni-Ti | 10 | 0.48±0.79 | 0.97 | -0.01 |
| Superelastic NiTi | 10 | 0.78±1.09 | 1.46 | 0.10 | |
Table 3.
Comparison of the rate of alignment in both groups using RM ANOVA
| Dependent Variable: Alignment Rate | |||||
|---|---|---|---|---|---|
|
| |||||
| Source | Type III sum of squares | df | Mean Square | F | Sig. |
| Time interval | 56.293 | 3 | 18.764 | 27.091 | 0.00** |
| Grouping | 0.105 | 1 | 0.105 | 0.152 | 0.69 |
| Time interval* Grouping | 1.87 | 3 | 0.623 | 0.9 | 0.45 |
Table 4.
Comparison of root resorption in both groups
| Tooth | Wire | n | Mean±SD (mm) | t | P |
|---|---|---|---|---|---|
| Lower left incisor | Heat-activated NiTi | 10 | 0.44±0.16 | -1.78 | 0.09 |
| Superelastic NiTi | 10 | 0.66±0.35 | |||
| Lower left lateral incisor | Heat-activated NiTi | 10 | 0.54±0.31 | -0.70 | 0.49 |
| Superelastic NiTi | 10 | 0.64±0.32 | |||
| Lower left canine | Heat-activated NiTi | 10 | 0.41±0.16 | -0.95 | 0.35 |
| Superelastic NiTi | 10 | 0.48±0.17 | |||
| Lower right incisor | Heat-activated NiTi | 10 | 0.64±0.18 | 2.04 | 0.06 |
| Superelastic NiTi | 10 | 0.50±0.12 | |||
| Lower right lateral incisor | Heat-activated NiTi | 10 | 0.55±0.17 | -0.11 | 0.92 |
| Superelastic NiTi | 10 | 0.56±0.25 | |||
| Lower right canine | Heat-activated NiTi | 10 | 0.46±0.40 | -1.51 | 0.15 |
| Superelastic NiTi | 10 | 0.75±0.46 |
Table 5 shows the comparison of the VAS scores 24 hours and 1 week after treatment using heat-activated and superelastic NiTi wires using the Mann–Whitney U test. The difference in pain perception was found to be statistically significant between the wires. Patients in the superelastic group reported more pain with a mean score of 42.9 ± 5.84 at 24 hours compared to those in the heat-activated group with a mean score of 35.5 ± 7.29. Although pain reduced after one week in both the groups, it was higher in the superelastic group than in the heat-activated group.
Table 5.
Comparison of VAS scores between the two groups at 24 hours and 1 week
| Time | Group | n | Mean rank | Mean score (SD) | Sum of ranks | Sig. |
|---|---|---|---|---|---|---|
| 1 day | Heat-activated NiTi | 10 | 7.65 | 35.5 (7.29) | 76.50 | 0.03* |
| Superelastic NiTi | 10 | 13.35 | 42.9 (5.84) | 133.50 | ||
| 1 week | Heat-activated NiTi | 10 | 7.65 | 4.1 (1.66) | 76.50 | 0.02* |
| Superelastic NiTi | 10 | 13.35 | 5.8 (1.32) | 133.50 |
Discussion
An initial archwire should be effective in aligning the arches while resulting in minimal pain and root resorption. An ideal aligning archwire should have good formability, spring-back, stiffness biocompatibility, low friction, and joinability and of low cost.[13]
Jian et al.[12] performed a systematic review to determine the impact of initial archwires on the alignment of the teeth with fixed orthodontic braces in relation to alignment duration, root resorption and pain severity. He concluded that the trials used in this analysis did not include any credible proof that any particular initial archwire was better or worse than any other in terms of speed of alignment or pain. He stated that there was no evidence regarding the initial effect of archwires on root resorption.
O'Brien[14] used edgewise brackets in his clinical trial but did not specify the dimensions and bracket type. Two trial reports by Evans et al.[15] and West et al.[2] also did not state the types of brackets used. Different clinical trials used different ligation methods. Cobb et al.[16] and Cioffi et al.[17] used elastomeric modules, Sebastian[18] used elastic modules or steel ties while Pandis[3] used self-ligating brackets. Studies (Cobb,[16] Evans,[15] Fernandes,[8] O'Brien[14] and West[2]) that did not specify whether or not tooth extraction was performed were included in the case-selection criteria.
The current research sought to address the limitations of the previous studies by evaluating the efficacy of the original aligning archwires by standardizing the bracket scheme, ligation scheme, extraction method, and concealment distribution.
A Cochrane systematic review by Jian et al.[12] suggested that trials should report both benefits (speed of alignment) and possible harms (such as pain and root resorption) and be of sufficient duration to enable these outcomes to be measured.
The present study found no significant difference in the rate of alignment between the two aligning archwires, superelastic NiTi and heat-activated NiTi when measured with Little's Irregularity Index. It was observed that greater irregularity required greater time to achieve alignment. The findings are in agreement with those of Abdelrehmann[13] who found that 0.014-inch conventional NiTi, superelastic NiTi, and thermoelastic NiTi were similar in terms of aligning efficiency. He reasoned that large deflections in the wire required to reach the superelastic plateau were rarely encountered clinically and therefore the properties of the wire may not have been fully expressed. Moreover, individual variations in the metabolic response of the periodontal ligament could mask the possible difference.
Archwire manufacturers claim the presence of specific properties by laboratory testing.
Low force distribution values resulting from in vitro experiments remain theoretical for most NiTi alloys, according to a study by Santoro et al.[19]. They concluded that certain archwires for therapeutic use do not display superelastic or plateau activity or need excessive deflection to do so.
Low force delivery values from in vitro testing remain theoretical for most NiTi alloys, according to an investigation by Santoro et al.[19] They concluded that many archwires do not exhibit superelastic or plateau behavior in clinical use or require excessive deflection in order to do so.
Pandis[3] reached a similar conclusion by comparing the efficiency of copper–nickel–titanium (CuNiTi) and nickel–titanium (NiTi) archwires. It was also a double-blind randomized clinical trial. He hypothesized that intraoral aging of the wires could cause significant morphological and structural alterations, including the destruction of the structural integrity of NiTi wires, delamination, the formation of craters, and increased porosity.
Phermsang-ngarm[20] conducted a clinical trial to compare the aligning efficiency of heat-activated NiTi and customized superelastic NiTi wires. Using a vertical and horizontal bias, unique bends were developed to achieve 1 mm activation of the archwire to be placed in the appropriate bracket slots of all the anterior teeth. He found that heat-activated NiTi wires took less time for alignment than customized superelastic NiTi wires. However, the study did not take into account the possible changes in the properties of the customized archwire due to bending.
Obrien et al.[14] investigated the rate of tooth movement with Nitinol and Titanol over a period of 35 days and found no significant clinical differences in this trial.
Evans et al.[15] evaluated 016 × 022 inch active martensitic medium force NiTi, 016 × 022 inch graded force active martensitic NiTi, and 0.0155-inch multistrand stainless steel aligning archwires for clinical efficiency. No statistically significant difference was found in tooth movements with these wires. He reasoned that individual metabolic responses within the periodontal ligament, variations in the ligation technique, and the absence of sufficient deformation of the wire in clinical factors could contribute to this result.
West et al.[2] investigated the alignment efficiency of 0.0155-inch diameter multiple-stranded stainless steel wire and 0.014-inch diameter nickel-titanium alloy wire over a six-week period.
It was observed that the nickel–titanium wire resulted in improved alignment in the lower labial section. They reasoned that the small interbracket span in the lower anterior segment contributed to the potency of superelastic effects of NiTi wire.
Cobb et al.[16] studied the effect of slot size (0.018 inch and 0.022 inch) and compared the aligning efficiency of 0.016-inch superelastic NiTi, 0.0175-inch multistranded stainless steel and ion-implanted NiTi wire. He concluded that both superelastic and multistranded wires provided similar aligning efficiency, if relegated monthly. Moreover, ion implantation on small round wires did not provide any advantage in initial alignment. The author stated that frictional resistance to sliding was not important in a clinical setting as observed in in vivo studies.
The extent of root resorption after orthodontic treatment influences the prognosis. Harmful consequences for the tooth may occur when severe or even a small percentage of resorption is present even in well-planned and conducted orthodontic treatment.[21] In the present study, CBCT was used to evaluate root resorption because of the ability of CBCT to obtain distortion-free and reproducible three-dimensional images. It was observed that root resorption was higher with superelastic Ni-Ti wire (0.59 mm) than heat-activated Ni-Ti (0.50 mm). However, the difference was not found to be statistically significant. Weltman[22] reported in a systematic review that strong orthodontic forces resulted in greater root resorption because the rate of development of the lacuna was faster and the mechanism of tissue repair was compromised.
It can thus be assumed that a wire exerting higher forces carries a risk of causing greater root resorption.
Similar results were observed by Alzahawi[23] who compared root resorption after the leveling phase of treatment, performed by either superelastic NiTi or conventional multi-stranded stainless steel archwires using conventional radiography. He hypothesized that the inactive intervals at force application, which may prolong treatment time, allow for the repair of resorption lacunae. Moreover, the use of conventional radiography could have influenced the results as it underestimates root resorption. The result of the present study is also supported by those of Phermsang-ngarm[20] who investigated root resorption during initial dental alignment with 0.012-inch preformed heat-activated (0.36 mm) or customized nickel-titanium (NiTi) archwires (0.23 mm) using CBCT images similar to the present study. However, the amount of resorption seen in their study was slightly less than the present study. This could have been due to the smaller size of the wire used in their study.
Pain and discomfort after the insertion of an initial archwire are common experiences among orthodontic patients. A relationship exists between the discomfort experienced after archwire placement and the forces being applied to the teeth.[24] In the present study, the pain and discomfort after the placement of the initial archwire were measured 24 hrs and 1 week after placing the wire on a visual analog scale of 100 mm. The visual analog scale is easy to administer and is a reliable method for measuring discrete pain. It can discriminate between small changes in pain intensity.[24] In the present study, it was observed that VAS scores were higher for superelastic NiTi, compared to heat-activated NiTi, both at 24 hours and 1 week after the insertion of the initial archwire. The difference was statistically significant. Gatto et al.[25] performed an in vitro evaluation of the load-deflection characteristics in heat-activated and superelastic NiTi. They observed that higher working forces were exhibited by superelastic NiTi than heat-activated NiTi. Therefore, the difference in pain intensity could be due to the difference in forces exerted by the two archwires, although these forces were not measured in the study. Cioffi et al.[17] compared pain intensity using the VAS scale after placing 0.016-inch superelastic NiTi and 0.016-inch thermoelastic NiTi in 30 individuals. Fernandes et al.[8] compared 0.014-inch Nitinol and 0.014-inch superelastic NiTi while Sebastian et al.[18] compared 0.016-inch superelastic wire and coaxial wire. They all found no difference in the overall discomfort level between different NiTi wires. Pain experience has great individual variation which may also have influenced the results.
The limitations of this study are the small sample size which did not allow the evaluation of archwire performance in patients of different age groups, gender, or levels of severity of crowding. The study also did not measure the force levels exerted by the two archwires on individual teeth or the tooth movement in three dimensions which could have helped to evaluate the difference in root resorption and pain.
Conclusions
There was no significant difference in the aligning efficiency and root resorption of superelastic and heat-activated NiTi wires. Superelastic NiTi wires resulted in more discomfort as compared to heat-activated NiTi.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient-consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Proffit WR. St Louis: CV Mosby Cooperation; 2000. Contemporary Orthodontics. [Google Scholar]
- 2.West AE, Jones ML, Newcombe RG. Multiflex versus superelastic: A randomized clinical trial of tooth alignment ability of initial arch wires. Am J Orthod Dentofacial Orthop. 1995;108:464–71. doi: 10.1016/s0889-5406(95)70046-3. [DOI] [PubMed] [Google Scholar]
- 3.Pandis N, Polychronopoulou A, Eliades T. Alleviation of mandibular anterior crowding with copper-nickel-titanium vs nickel-titanium wires: A double-blind randomized control trial. Am J Orthod Dentofacial Orthop. 2009;136:152–3. doi: 10.1016/j.ajodo.2009.03.030. [DOI] [PubMed] [Google Scholar]
- 4.Gravina MA, Brunharo IH, Fraga MR, Artese F, Campos MJ, Vitral RW, et al. Clinical evaluation of dental alignment and leveling with three different types of orthodontic wires. Dent Press J Orthod. 2013;18:31–7. doi: 10.1590/s2176-94512013000600006. [DOI] [PubMed] [Google Scholar]
- 5.Papageorgiou SN, Konstantinidis I, Papadopoulou K, Jäger A, Bourauel C. A systematic review and metaanalysis of experimental clinical evidence on initial aligning archwires and archwire sequences. Orthod Craniofac Res. 2014;17:197–215. doi: 10.1111/ocr.12048. [DOI] [PubMed] [Google Scholar]
- 6.Santoro M, Nicolay OF, Cangialosi TJ. Pseudoelasticity and thermoelasticity of nickel-titanium alloys: A clinically oriented review. Part I: Temperature transitional ranges. Am J Orthod Dentofacial Orthop. 2001;119:587–93. doi: 10.1067/mod.2001.112446. [DOI] [PubMed] [Google Scholar]
- 7.Jones M, Chan C. The pain and discomfort experienced during orthodontic treatment: A randomized controlled clinical trial of two initial aligning arch wires. Am J Orthod Dentofacial Orthop. 1992;102:373–81. doi: 10.1016/0889-5406(92)70054-e. [DOI] [PubMed] [Google Scholar]
- 8.Fernandes LM, Ogaard B, Skoglund L. Pain and discomfort with NiTi aligning archwires. J Orofac Orthop. 1998;59:331–9. doi: 10.1007/BF01299769. [DOI] [PubMed] [Google Scholar]
- 9.John F, Sherrard P, Rossouw E, Benson BW, Carrillo R, Buschang PH. Accuracy and reliability of tooth and root lengths measured on cone-beam computed tomographs. Am J Orthod Dentofacial Orthop. 2010;137:S100–8. doi: 10.1016/j.ajodo.2009.03.040. [DOI] [PubMed] [Google Scholar]
- 10.de Freitas JC, Lyra OCP, de Alencar AHG, Estrela C. Long-term evaluation of apical root resorption after orthodontic treatment using periapical radiography and cone beam computed tomography. Dent Press J Orthod. 2013;18:104–12. doi: 10.1590/s2176-94512013000400015. [DOI] [PubMed] [Google Scholar]
- 11.Riley M, Bearn DR. A systematic review of clinical trials of aligning archwires. J Orthod. 2009;36:42–51. doi: 10.1179/14653120722914. [DOI] [PubMed] [Google Scholar]
- 12.Jian F, Lai W, Furness S, McIntyre GT, Millett DT, Hickman J, et al. Initial arch wires for tooth alignment during orthodontic treatment with fixed appliances (Review) Cochrane Database Syst Rev. 2013;30:CD007859. doi: 10.1002/14651858.CD007859.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Abdelrahman RS, Al-Nimri KS, Al Maaitah EF. A clinical comparison of three aligning archwires in terms of alignment efficiency: A prospective clinical trial. Angle Orthod. 2015;85:434–9. doi: 10.2319/041414-274.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.O’Brien K, Lewis D, Shaw W, Combe E. A clinical trial of aligning archwires. Eur J Orthod. 1990;12:380–4. doi: 10.1093/ejo/12.4.380. [DOI] [PubMed] [Google Scholar]
- 15.Evans TJ, Jones ML, Newcombe RG. Clinical comparison and performance perspective of three aligning arch wires. Am J Orthod Dentofacial Orthop. 1998;114:32–9. doi: 10.1016/s0889-5406(98)70234-3. [DOI] [PubMed] [Google Scholar]
- 16.Cobb NW, III, Kula KS, Phillips C, Proffit WR. Efficiency of multi-strand steel, superelastic Ni-Ti and ion-implanted Ni-Ti archwires for initial alignment. Clin Orthod Res. 1998;1:12–9. doi: 10.1111/ocr.1998.1.1.12. [DOI] [PubMed] [Google Scholar]
- 17.Cioffi I, Piccolo A, Tagliaferri R, Paduano S, Galeotti A, Martina R. Pain perception following first orthodontic archwire placement—Thermoelastic vs superelastic alloys: A randomized controlled trial. Quintessence Int. 2012;43:61–9. [PubMed] [Google Scholar]
- 18.Sebastian B. Alignment efficiency of superelastic coaxial nickel-titanium vs superelastic single-stranded nickel-titanium in relieving mandibular anterior crowding, A randomized controlled prospective study. Angle Orthod. 2012;82:703–8. doi: 10.2319/072111-460.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Santoro M, Nicolay OF, Cangialosi TJ. Pseudoelasticity and thermoelasticity of nickel-titanium alloys: A clinically oriented review. Part II: Deactivation forces. Am J Orthod Dentofacial Orthop. 2001;119:594–603. doi: 10.1067/mod.2001.112447. [DOI] [PubMed] [Google Scholar]
- 20.Phermsang-ngarm P, Charoemratrote C. Tooth and bone changes after initial anterior dental alignment using preformed vs customized nickel titanium archwires in adults: A randomized clinical trial. Angle Orthod. 2018;88:425–34. doi: 10.2319/090317-589.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Castro OI, Alencar HG, Valladares J, Estrela C. Apical root resorption due to orthodontic treatment detected by cone beam computed tomography. Angle Orthod. 2013;83:196–203. doi: 10.2319/032112-240.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Weltman B, Vig KW, Fields HW, Shanker S, Kaizar EE. Root resorption associated with orthodontic tooth movement: A systematic review. Am J Orthod Dentofacial Orthop. 2010;137:462–76. doi: 10.1016/j.ajodo.2009.06.021. [DOI] [PubMed] [Google Scholar]
- 23.Alzahawi K, Færøvig E, Brudvik P, Bøe OE, Mavragani M. Root resorption after leveling with superelastic and conventional steel arch wires: A prospective study. Prog Orthod. 2014;15:35. doi: 10.1186/s40510-014-0035-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Buehler WJ, Gilfrich JV, Wiley RC. Effect of low-temperature phase changes on the mechanical properties of alloys near composition NiTi. J Appl Phys. 1963;34:1475–7. [Google Scholar]
- 25.Gatto E, Matarese G, Bella G, Nucera R, Borsellino C, Cordasco G. Load–deflection characteristics of superelastic and thermal nickel–titanium wires. Eur J Orthod. 2013;35:115–23. doi: 10.1093/ejo/cjr103. [DOI] [PubMed] [Google Scholar]