

Key Points
Question
Does use of a school-wide integrated pest management (IPM) program or high-efficiency particulate air (HEPA) filter purifiers in the classrooms reduce asthma symptoms in students with active asthma?
Findings
This factorial randomized clinical trial included 236 students (attending 41 elementary schools with 209 classrooms) randomized to an IPM program at the school level, use of HEPA filter purifiers at the classroom level, or both. Use of the school-wide IPM program resulted in a mean of 1.5 symptom-days with asthma during a 2-week period vs 1.9 symptom-days for no IPM; use of HEPA filter purifiers resulted in a mean of 1.6 symptom-days with asthma vs 1.8 symptom-days for sham HEPA filter purifiers; neither comparison was statistically significant.
Meaning
Among children with active asthma, use of a school-wide IPM program or HEPA filter purifiers in the classrooms did not significantly reduce symptom-days with asthma.
Abstract
Importance
School and classroom allergens and particles are associated with asthma morbidity, but the benefit of environmental remediation is not known.
Objective
To determine whether use of a school-wide integrated pest management (IPM) program or high-efficiency particulate air (HEPA) filter purifiers in the classrooms improve asthma symptoms in students with active asthma.
Design, Setting, and Participants
Factorial randomized clinical trial of a school-wide IPM program and HEPA filter purifiers in the classrooms was conducted from 2015 to 2020 (School Inner-City Asthma Intervention Study). There were 236 students with active asthma attending 41 participating urban elementary schools located in the Northeastern US who were randomized to IPM by school and HEPA filter purifiers by classroom. The date of final follow-up was June 20, 2020.
Interventions
The school-wide IPM program consisted of application of rodenticide, sealing entry points, trap placement, targeted cleaning, and brief educational handouts for school staff. Infestation was assessed every 3 months, with additional treatments as needed. Control schools received no IPM, cleaning, or education. Classroom portable HEPA filter purifiers were deployed and the filters were changed every 3 months. Control classrooms received sham HEPA filters that looked and sounded like active HEPA filter purifiers. Randomization was done independently (split-plot design), with matching by the number of enrolled students to ensure a nearly exact 1:1 student ratio for each intervention with 118 students randomized to each group. Participants, investigators, and those assessing outcomes were blinded to the interventions.
Main Outcomes and Measures
The primary outcome was the number of symptom-days with asthma during a 2-week period. Symptom-days were assessed every 2 months during the 10 months after randomization.
Results
Among the 236 students who were randomized (mean age, 8.1 [SD, 2.0] years; 113 [48%] female), all completed the trial. At baseline, the 2-week mean was 2.2 (SD, 3.9) symptom-days with asthma and 98% of the classrooms had detectable levels of mouse allergen. The results were pooled because there was no statistically significant difference between the 2 interventions (P = .18 for interaction). During a 2-week period, the mean was 1.5 symptom-days with asthma after use of the school-wide IPM program vs 1.9 symptom-days after no IPM across the school year (incidence rate ratio, 0.71 [95% CI, 0.38-1.33]), which was not statistically significantly different. During a 2-week period, the mean was 1.6 symptom-days with asthma after use of HEPA filter purifiers in the classrooms vs 1.8 symptom-days after use of sham HEPA filter purifiers across the school year (incidence rate ratio, 1.47 [95% CI, 0.79-2.75]), which was not statistically significantly different. There were no intervention-related adverse events.
Conclusions and Relevance
Among children with active asthma, use of a school-wide IPM program or classroom HEPA filter purifiers did not significantly reduce symptom-days with asthma. However, interpretation of the study findings may need to consider allergen levels, particle exposures, and asthma symptoms at baseline.
Trial Registration
ClinicalTrials.gov Identifier: NCT02291302
This randomized clinical trial compares use of a school-wide integrated pest management (IPM) program vs use of high-efficiency particulate air (HEPA) filter purifiers in the classrooms for students with active asthma attending urban elementary schools who were randomized to IPM by school and HEPA filter purifiers by classroom.
Introduction
Urban minority populations experience greater asthma-related morbidity and mortality than their nonurban, nonminority counterparts.1 Research since 1997 to the present has elucidated the important contribution of the home environment as a significant cause of these differences, with multiple efforts studying mitigation of home environmental exposures and health effects.2,3,4,5,6 Elementary school students spend all day in school (primarily in 1 classroom), making school akin to a source of occupational environmental asthma triggers for children. Previously confirmed in the School Inner-City Asthma Study, mouse allergens were detected in 99% of school dust samples and were associated with asthma morbidity, independent of home exposure and sensitization.7 In a pilot randomized clinical trial including 25 students from 3 schools, classroom high-efficiency particulate air (HEPA) filter purifiers reduced particles as measured by fine particulate matter (PM2.5) by approximately 45% compared with sham HEPA filter purifiers, but the study lacked power to study health effects.8 The School Inner-City Asthma Intervention Study aimed to test the efficacy of a school-wide integrated pest management (IPM) program and use of HEPA filter purifiers in the classrooms for reducing asthma morbidity.
Methods
This study was a factorial, randomized clinical trial conducted at 41 urban elementary schools in the Northeastern US. The study protocol was approved by the Boston Children’s Hospital institutional review board and by the principals at the participating schools. Per confidentiality agreements, the locations of the schools may not be disclosed. Written parental informed consent and student assent were obtained in English or Spanish. The trial protocol and statistical analysis plan appear in Supplement 1. Detailed methods have been published.9
Participants
Each spring, validated surveys10 were distributed at between 6 and 10 participating elementary schools (the number changed yearly), were given to all students, and were completed by the students’ caregivers (Figure 1 and eFigure 1 in Supplement 2). Children with active physician-diagnosed asthma (ie, unscheduled asthma visit, hospitalization, corticosteroid bursts, symptoms, or controller medication use within the past year) were eligible for a screening visit, which was similar to the requirements for other National Institutes of Health–funded asthma trials.11,12
Figure 1. Flow of Students in the School Inner-City Asthma Intervention Study.
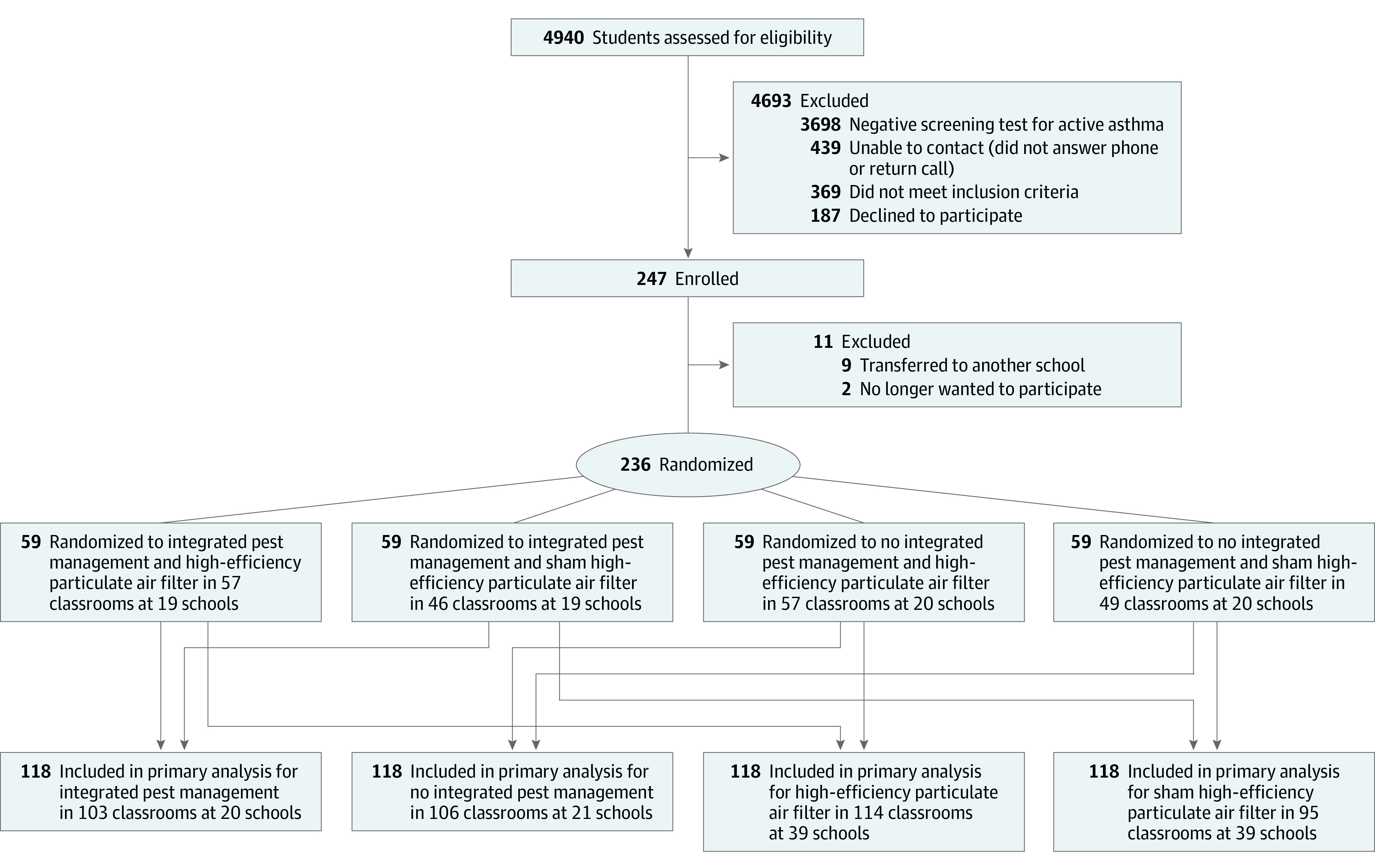
All students who were randomized received an intervention throughout the school year.
The screening visit included questionnaires, allergy skin testing to 14 common aeroallergens (ALK-Abelló) using the MultiTest II device (Lincoln Diagnostics), standard procedures,13 and spirometry (Koko, Respitech) per guidelines from the American Thoracic Society.14 These data were used to characterize the students prior to randomization. Students who fulfilled inclusion criteria were eligible for the trial and to have their classroom and school randomized to receive the intervention during the subsequent school year (eTable 1 in Supplement 2). Self-reported race and ethnicity were collected to characterize the sample because minority children are disproportionately affected by asthma. Race and ethnicity were classified and defined by self-report.
Randomization and Masking
Randomization to the school-wide IPM program and HEPA filter purifiers in the classrooms was performed using Stata version 14 (StataCorp) to generate random numbers at the beginning of the school year when the enrolled student’s classroom was confirmed.
The classrooms and schools were randomized independently (split-plot design) and were matched by the number of enrolled students to ensure a nearly exact 1:1 student ratio for each intervention. At the classroom level this typically involved 1:1 or 2:1 matching, but at the school level this sometimes required 3:1 or 2:2 matching given the small number of schools randomized per year and the varying number of enrolled students at each school. An example of 2:2 matching for year 2 of the study involved clustering schools A (n = 1 participant) and B (n = 12 participants) and matching this A/B cluster with a second cluster of schools C (n = 3) and D (n = 9). This 2:2 matching ensured greater balance in the number of participants randomized to IPM (schools A and B; n = 13) vs no IPM (schools C and D; n = 12) than would have occurred via simple random assignment of schools to IPM. Allocation was secured and generated centrally and independently; the designee who assigned the groups was not involved in other parts of the trial.
The allocation to classroom HEPA filter purifiers or sham HEPA filter purifiers was blinded to the participants, the people deploying the intervention, and those assessing the outcomes, including those obtaining parental informed consent and student assent. The engineers making and allocating the active and the sham HEPA filter purifiers were not involved in any other aspects of the trial and masking was maintained with quarterly assessments. The trained pest management specialists providing the school-wide IPM program were unblinded due to feasibility, but the student participants and trial investigators remained blinded throughout the trial. Students were randomized by school and classroom to 1 of the following groups: IPM and HEPA filter purifier; IPM and sham HEPA filter purifier; no IPM and HEPA filter purifier; or no IPM and sham HEPA filter purifier (no intervention).
Baseline Environmental Assessments
Baseline environmental assessments for a panel of allergens and particles were conducted at the schools by collecting a 1-week air sample immediately followed by vacuum-settled dust samples from each student’s primary (spend approximately 6 hours/day) classroom. One-week air samples were collected using pumps at a flow rate of 5 L/min for concentrations of particle matter (PM2.5) mass and coarse size (PM2.5-PM10) and black carbon and at a flow rate of 3 L/min for allergens. Asthma symptoms were assessed concurrently prior to deployment of both interventions.
Allergens (mouse, rat, dust mite, cockroach, cat, dog, Alternaria alternate, and Aspergillus fumigatus mold) were analyzed in both airborne and settled dust samples using a multiplex assay (MARIA, Indoor Biotechnologies)9 (eTable 2 in Supplement 2). A home environmental dust sample also was collected from the participant’s bedroom as a valid12 home exposure measure and to check for balance in each group.
Interventions
The IPM intervention included extermination with traps with nontoxic bait and sealing of holes by IPM professionals who were trained according to the study protocol.4 The focus was on surrounding areas that fed into the student’s primary classroom and could harbor infestation by food and water sources (ie, cafeteria). At the first IPM visit, a focused cleaning was aimed at the removal of trash or clutter and animal droppings and the wet mopping or vacuuming of the floors. Educational handouts were provided to the school staff explaining the IPM approaches for reducing pest allergen levels by source removal, prevention of reentry, and the cleaning of allergen reservoirs. A booster IPM visit was conducted 4 weeks later, which included an assessment of pest infestation evidence (ie, droppings) and repeated setting of traps and sealing of holes and cracks. Subsequent IPM intervention modules were done 2 months after the last IPM visit (2 additional visits spaced 2-4 weeks apart) and were delivered again if there was evidence of persistent infestation (details appear in the eAppendix in Supplement 2). The control schools did not receive the IPM intervention, cleaning, or education.
Active or sham HEPA filter purifiers (model AP101; Coway Co Ltd) were placed in the students’ primary classroom as free-standing units. To achieve maximum effectiveness with an acceptable noise level (52 dB), modification was made to get a dust-free air delivery rate of 3000 L/min, which was effective in reducing particles during a school pilot study (4 filters/classroom).8 Noise makers were engineered for the sham HEPA filter purifiers to make them indistinguishable from the active HEPA filter units. The HEPA filters were replaced every 3 months by staff who did not interact with participants or with trial investigators. Additional details appear in the eAppendix in Supplement 2.
Outcomes
The asthma-related health outcomes of the students were assessed by parent survey at baseline and every 2 months until the end of the school year. The primary outcome was assessed over 10 months. The primary outcome was the number of symptom-days with asthma during a 2-week period, which has been validated and used in other asthma trials.4,11,15,16 The outcome was defined as the largest value among 3 symptom variables: days of slowed activity due to asthma; number of nights of waking with asthma symptoms; and days of coughing, wheezing, or with chest tightness. The number of symptom-days with asthma during a 2-week period ranges from a minimum of 0 symptom-days to a maximum of 14 symptom-days. No minimal clinically important difference has been established for this outcome.
The prespecified secondary outcomes were school absences, Composite Asthma Severity Index (a comprehensive severity scale of symptoms and albuterol use during the day, symptoms and albuterol use during the night, controller treatment, lung function measures, and exacerbations),17 health care use, and pulmonary function testing (including forced expiratory volume in first second of expiration [FEV1], ratio of FEV1 to percent of forced vital capacity [FEV1:FVC], and forced expiratory flow between the 25% and 75% of FVC [FEF25%-75%]). The Composite Asthma Severity Index ranges from 0 points (lowest) to 20 points (highest) with a minimal clinically important difference of 0.49 points.18 Spirometry was conducted per American Thoracic Society standards during the 2 follow-up visits at the schools concurrent with the postintervention environmental sampling during the academic year.9
Follow-up school environmental assessments (a prespecified secondary outcome) after randomization took place once during the late winter semester and once during the spring semester. Environmental outcomes were based on the schools and the classrooms linked to the randomized students. Samples were collected in the same manner as at baseline.
Adverse Events
Adverse events, severity, and relatedness to study procedures were determined and recorded. Adverse events were considered at each clinical encounter and either observed by the study team or spontaneously reported by the parent or caregiver. Timing in proximity to the study procedure (ie, within 30 minutes) allowed the investigators to determine if the adverse events were related to the interventions.
Sample Size Calculation
For the primary outcome, assumptions for the sample size calculations used data on classroom exposure and symptom data from the prospective, observational school study7 that linked school-specific exposures with health outcomes, adjusting for exposures at home. Power was determined using a simulation-based approach that repeatedly generated data under the primary multilevel negative binomial model, calculating the proportion of time the null hypothesis of no school-wide IPM effect and no classroom HEPA filter purifying effect was rejected for a given effect size. The intercept value of log3 was chosen to correspond to a rate of 3 symptom-days at baseline prior to the intervention. The amount of overdispersion in the negative binomial distribution (θ = 3 in the megbin function using the MASS package in the R software package [R Foundation for Statistical Computing]) was set equal to that estimated in the observational school cohort.
The random-effects SD was set equal to 0.5 for the student random effects and equal to 0.2 for the school random effects. All power calculations were run assuming a 2-sided α level of .05 and all power estimates were based on 1000 simulated data sets. With a sample size of 240 students, there was greater than 80% power to detect a difference of at least 0.60 symptom-days and greater than 95% power to detect a difference of 0.75 symptom-days between the 2 groups. These effect sizes were based on other studies conducted in the same geographic region with the same outcome shown to be clinically meaningful along with the summary values of differences actually observed in other childhood asthma trials.4,11,16,19
To check the power to detect associations among quintiles of the exposure distribution (as a continuous variable), the same simulation strategy (based on a multilevel negative binomial regression model but with an exposure quintile) was used as a covariate. Using this approach, 90% power was estimated to detect the slope of 0.173 (estimated in the observational school study), which represents the log relative rate per 1-unit increase in the exposure quintile in as few as 40 students. This result demonstrated the increase in power that results from using the continuous exposure concentration when such an effect existed.
Statistical Analysis
Multilevel models20 were used to quantify the effects of the interventions (both school-wide IPM and classroom-specific HEPA filter purifiers) on the clinical outcomes in a factorial design. Count data (eg, primary outcome of symptom-days with asthma) were analyzed using negative binomial mixed models and continuous outcomes were analyzed using linear mixed models. The primary outcome was analyzed by randomization group, which included all randomized participants because all participants randomized received the intervention throughout the school year. These analyses contained all observations for a given student, the main effects of both interventions to account for any differences prior to the interventions, a categorical variable representing visit number, and the postrandomization × intervention (both the IPM and the HEPA filter purifier interventions) interactions that represent the effects of interest.
The negative binomial assumption for count outcomes accounts for overdispersion relative to the Poisson assumptions. The models also contained school-level and participant-level random effects to account for any clustering of the outcomes due to the hierarchical structure of the data. In the post hoc exploratory time analyses, the models were fit to estimate how the effects of the interventions varied over the remainder of the school year for the primary outcome. Specifically, these time-varying effect models contained the main effect of the interventions, a smooth term of day of the school year to account for seasonal patterns in an outcome, an effect of the interventions at the time of implementation, and a term that allows the effect of each intervention to change linearly with time since implementation.
For the secondary outcomes, we only analyzed and report the prespecified outcomes. The effect of the interventions on particles was estimated using linear mixed models with clustering at the classroom and school levels. Mixed-effects tobit regression was used for log-transformed allergens to left-censor samples that did not detect any allergens. Because of the potential for type I error due to multiple comparisons, the findings from the analyses of the secondary outcomes should be interpreted as exploratory. To account for data not missing completely at random, sensitivity analyses (including inverse proportional weighting of observations) were performed. This approach effectively increases the weight of the observations that are more likely to be missing.21
All tests were 2-sided with an α level of .05 and were performed using Stata version 16.1 (StataCorp).
Results
Enrollment and Study Completion
Recruitment began on April 1, 2015. A total of 4940 students were assessed for eligibility and, of these, 3698 had a negative screening result for active asthma, making them ineligible. A total of 247 children with asthma were enrolled and 236 were randomized into equal-sized treatment groups from 209 classrooms at 41 elementary schools (Figure 1). None of the randomized students receiving the interventions changed primary classroom or mean time spent in the classrooms per day throughout the academic school year. Adherence to the intervention protocol was monitored quarterly and there was greater than 95% adherence throughout the trial.
Randomization and follow-up were conducted during the academic school years of 2015-2020. The COVID-19 pandemic caused school shutdowns on March 17, 2020, limiting spring school data collection and analysis was truncated for 30 students randomized in year 5 to that date. The date of final follow-up was June 20, 2020.
Baseline Characteristics
The mean age of the population was 8.1 years (SD, 2.0 years) and 113 (48%) were female. The population consisted predominantly of children with minority race and ethnicity (57% Hispanic and 24% Black) and 32% were from households with an annual income of less than $45 000. At baseline, the 2-week mean was 2.2 symptom-days with asthma (SD, 3.9 symptom-days). Student sensitization to mouse allergens was 26% and to cockroach allergens was 14%, which is similar to home-based studies7,22 (Table 1). Of the total classrooms, 98% had detectable mouse allergens and the levels ranged from below detectable to 116 μg/g. Consistent with the observational cohort, more than 90% of baseline classroom allergen levels for cockroach, rat, Alternaria mold, Aspergillus mold, and dust mite were undetectable7; therefore, the analysis focused on classroom mouse, cat, and dog allergens. Classroom and home allergen and particle levels at randomization were balanced between the groups (Table 2).
Table 1. Student Characteristics at Baseline.
| No. (%) of studentsa | ||||
|---|---|---|---|---|
| IPM and HEPA filter (n = 59) |
IPM and sham HEPA filter (n = 59) |
No IPM and HEPA filter (n = 59) |
No IPM and sham HEPA filter (n = 59) |
|
| Demographic characteristics | ||||
| Age, mean (SD), y | 8.2 (1.9) | 8.2 (2.0) | 8.3 (2.2) | 7.9 (1.9) |
| Sex | ||||
| Male | 33 (56) | 26 (44) | 27 (46) | 37 (63) |
| Female | 26 (44) | 33 (56) | 32 (54) | 22 (37) |
| Race | ||||
| Black | 17 (31) | 13 (24) | 15 (29) | 12 (21) |
| White | 21 (38) | 26 (47) | 20 (38) | 33 (57) |
| Otherb | 17 (31) | 16 (29) | 17 (33) | 13 (22) |
| Hispanic ethnicity | 38 (64) | 26 (44) | 32 (56) | 35 (62) |
| Income | ||||
| <$25 000 | 13 (22) | 5 (8) | 11 (19) | 12 (20) |
| $25 000-$45 000 | 8 (14) | 8 (14) | 11 (19) | 8 (14) |
| >$45 000 | 18 (31) | 26 (44) | 18 (31) | 21 (36) |
| Refused or do not know | 20 (34) | 20 (34) | 19 (32) | 18 (31) |
| Asthma symptoms and medication use prior to the intervention | ||||
| No. of symptom-days with asthma, 2-wk mean (SD) | 2.0 (3.2) | 2.4 (4.2) | 1.5 (3.4) | 3.0 (4.7) |
| Range for No. of symptom-days with asthma | ||||
| 0-1 | 36 (61) | 40 (68) | 45 (76) | 36 (61) |
| 2-3 | 12 (20) | 8 (14) | 6 (10) | 7 (12) |
| 4-9 | 7 (12) | 5 (8) | 5 (8) | 8 (14) |
| 10-14 | 4 (7) | 6 (10) | 3 (5) | 8 (14) |
| No. of missed school days due to asthma, 2-wk mean (SD) | 0.16 (0.45) | 0.10 (0.40) | 0.12 (0.92) | 0.04 (0.19) |
| Range for No. of missed school days due to asthma | ||||
| 0 | 51 (88) | 55 (93) | 57 (98) | 55 (96) |
| 1-2 | 7 (12) | 4 (7) | 0 | 2 (4) |
| 3-7 | 0 | 0 | 1 (2) | 0 |
| Composite Asthma Severity Index | ||||
| Mean (SD) | 3.4 (2.5) | 3.0 (1.8) | 2.8 (2.3) | 3.0 (1.9) |
| Median (interquartile range) | 2 (2-5) | 2 (2-4) | 2 (1-5) | 3 (1-5) |
| No. of days with short-acting β-agonist use, 2-wk mean (SD) | 1.4 (3.1) | 1.4 (3.3) | 1.0 (2.7) | 1.4 (3.2) |
| Range for No. of days with short-acting β-agonist use | ||||
| 0-1 | 44 (75) | 46 (78) | 46 (78) | 36 (61) |
| 2-3 | 6 (10) | 7 (12) | 10 (17) | 7 (12) |
| 4-9 | 6 (10) | 2 (3) | 1 (2) | 8 (14) |
| 10-14 | 3 (5) | 4 (7) | 2 (3) | 8 (14) |
| Type of treatment received | ||||
| Short-acting β-agonist only | 23 (40) | 25 (43) | 23 (41) | 29 (50) |
| Low-dose inhaled corticosteroids or leukotriene modifier | 21 (36) | 22 (38) | 22 (39) | 16 (28) |
| Low-dose inhaled corticosteroids and long-acting β-agonist or medium-dose inhaled corticosteroids | 2 (3) | 1 (2) | 3 (5) | 4 (7) |
| Medium-dose inhaled corticosteroids and long-acting β-agonist | 4 (7) | 4 (7) | 2 (4) | 3 (5) |
| High-dose inhaled corticosteroids with or without long-acting β-agonist | 8 (14) | 6 (10) | 6 (11) | 6 (10) |
| Asthma-related health care use during prior year | ||||
| Acute visit | 11 (19) | 7 (12) | 12 (20) | 9 (15) |
| Emergency department visit | 3 (5) | 1 (2) | 3 (5) | 4 (7) |
| Hospitalization | 5 (8) | 3 (5) | 6 (10) | 4 (7) |
| Short course of oral corticosteroids | 15 (25) | 13 (22) | 14 (24) | 15 (25) |
| Lung function prior to treatment with bronchodilator | ||||
| No. of patients | 56 | 52 | 47 | 55 |
| FEV1, mean (SD), % predicted | 99.7 (21.9) | 99.3 (16.3) | 97.0 (14.2) | 98.7 (15.5) |
| FVC, mean (SD), % predicted | 97.4 (17.5) | 99.2 (15.5) | 100.0 (15.2) | 99.0 (12.8) |
| FEV1:FVC, mean (SD), % | 85.6 (8.8) | 85.7 (7.8) | 84.2 (6.3) | 84.2 (7.2) |
| Characteristics of skin test sensitivity | ||||
| Any sensitization, No./total (%) | 34/58 (59) | 38/58 (66) | 30/58 (52) | 34/57 (60) |
| Dust mite allergen | 15 (26) | 26 (45) | 15 (15) | 13 (23) |
| Cockroach allergen | 8 (14) | 17 (28) | 16 (28) | 14 (25) |
| Mouse allergen | 15 (26) | 16 (28) | 12 (21) | 11 (19) |
| Cat allergen | 13 (22) | 16 (28) | 8 (14) | 8 (14) |
| Mold allergen | 11 (19) | 7 (12) | 3 (5) | 6 (11) |
| Dog allergen | 3 (5) | 7 (12) | 5 (9) | 3 (5) |
Abbreviations: FEV1, forced expiratory volume in first second of expiration; FEV1:FVC, ratio of FEV1 to percent of FVC; FVC, forced vital capacity; HEPA, high-efficiency particulate air; IPM, integrated pest management.
Unless otherwise indicated.
Asian, American Indian/Alaska Native, multiracial, or specified as other.
Table 2. Classroom Exposure and Home Allergen Levels at Baseline.
| Median (10th-90th percentile)a | ||||
|---|---|---|---|---|
| IPM and HEPA filter | IPM and sham HEPA filter | No IPM and HEPA filter | No IPM and sham HEPA filter | |
| Classroom exposure levels | ||||
| Floor dust, μg/g | ||||
| No. of classrooms assessed | 55 | 43 | 52 | 47 |
| Mouse allergen | 0.24 (0.01-4.80) | 0.28 (0.02-2.38) | 0.10 (0.01-1.94) | 0.13 (ND-3.81) |
| Cat allergen | 0.08 (0.01-0.85) | 0.17 (0.02-1.85) | 0.15 (0.01-1.49) | 0.11 (ND-1.07) |
| Dog allergen | 0.05 (ND-0.38) | 0.08 (0.02-0.42) | 0.06 (ND-0.27) | 0.04 (ND-0.35) |
| Air dust, ng/m3 | ||||
| No. of classrooms assessed | 55 | 44 | 53 | 46 |
| Mouse allergen | 0.008 (ND-0.036) | 0.009 (ND-0.037) | 0.003 (ND-0.013) | 0.005 (ND-0.015) |
| Cat allergen | 0.007 (ND-0.022) | 0.006 (ND-0.027) | 0.006 (ND-0.030) | 0.006 (ND-0.027) |
| Dog allergen | ND (ND-0.015) | ND (ND-0.011) | ND (ND-0.009) | ND (ND-0.011) |
| Particulate, mean (SD), μg/m3 | ||||
| No. of classrooms assessed | 50 | 44 | 44 | 38 |
| Coarse PM | 8.1 (3.4) | 7.7 (3.2) | 7.3 (2.8) | 6.7 (3.2) |
| PM2.5 | 5.4 (1.9) | 5.7 (2.2) | 5.5 (2.0) | 6.1 (2.8) |
| Black carbon | 0.34 (0.13) | 0.33 (0.14) | 0.34 (0.12) | 0.38 (0.09) |
| Home allergen levels | ||||
| Floor dust, μg/g | ||||
| No. of homes assessed | 37 | 45 | 44 | 46 |
| Mouse allergen | 0.044 (ND-12.753) | 0.143 (ND-4.373) | 0.025 (ND-3.774) | 0.018 (ND-1.106) |
| Cat allergen | 0.014 (ND-0.328) | 0.028 (ND-1.095) | 0.031 (ND-2.078) | 0.017 (ND-0.390) |
| Dog allergen | 0.021 (ND-4.858) | 0.022 (ND-1.302) | 0.016 (ND-2.808) | ND (ND-2.808) |
Abbreviations: HEPA, high-efficiency particulate air; IPM, integrated pest management; ND, not detected; PM, particulate matter.
Unless otherwise indicated.
Primary Outcome
There was no statistically significant interaction between the 2 interventions (incidence rate ratio [IRR], 0.43 [95% CI, 0.12-1.49], P = .18 for interaction); therefore, the data are presented as pooled by each intervention (Table 3). The outcomes by mutually exclusive treatment groups appear in eTable 3 and eTable 4 in Supplement 2.
Table 3. Primary and Secondary Asthma Outcomes and Lung Function Assessmenta.
| Observed outcomes after the intervention | Adjusted effect (95% CI)b | Observed outcomes after the intervention | Adjusted effect (95% CI)b | |||
|---|---|---|---|---|---|---|
| IPM | No IPM | HEPA filter | Sham HEPA filter | |||
| Primary outcome | ||||||
| No. of students | 97 | 105 | 105 | 97 | ||
| No. of symptom-days with asthma, 2-wk mean (SD) | 1.5 (2.9) | 1.9 (3.3) | IRR, 0.71 (0.38 to 1.33) | 1.6 (3.0) | 1.8 (3.3) | IRR, 1.47 (0.79 to 2.75) |
| Prespecified secondary outcomes | ||||||
| No. of students | 97 | 105 | 105 | 97 | ||
| No. of missed school days due to asthma, 2-wk mean (SD) | 0.11 (0.50) | 0.17 (0.75) | IRR, 0.20 (0.04 to 0.96) | 0.15 (0.68) | 0.13 (0.59) | IRR, 0.74 (0.17 to 3.28) |
| Asthma-related health care use, 2-mo mean (SD)c | 0.04 (0.21) | 0.08 (0.29) | IRR, 0.94 (0.38 to 2.31) | 0.07 (0.27) | 0.06 (0.24) | IRR, 1.01 (0.43 to 2.38) |
| Composite Asthma Severity Index, mean (SD)d | 2.9 (2.2) | 3.0 (2.4) | MD, –0.2 (–0.7 to 0.3) | 3.0 (2.3) | 2.8 (2.3) | MD, 0.1 (–0.5 to 0.6) |
| Lung function | ||||||
| No. of students | 111 | 107 | 109 | 109 | ||
| FEV1, mean (SD), % predicted | 95.2 (17.5) | 98.0 (15.5) | MD, –3.8 (–6.8 to 0.8) | 96.2 (16.7) | 96.9 (16.5) | MD, –0.2 (–3.2 to 2.8) |
| FEV1:FVC, mean (SD), % | 82.8 (8.8) | 83.2 (7.1) | MD, –1.5 (–3.2 to 0.2) | 83.8 (7.9) | 82.2 (8.1) | MD, 1.6 (–0.1 to 3.4) |
| FEF25%-75%, mean (SD), % predicted | 88.4 (28.5) | 93.3 (32.0) | MD, –5.8 (–12.0 to 0.5) | 90.8 (31.1) | 90.6 (29.6) | MD, 4.7 (–1.6 to 10.9) |
Abbreviations: FEF25%-75%, forced expiratory flow between the 25% and 75% of FVC; FEV1, forced expiratory volume in first second of expiration; FEV1:FVC, ratio of FEV1 to percent of FVC; FVC, forced vital capacity; HEPA, high-efficiency particulate air; IPM, integrated pest management; IRR, incidence rate ratio; MD, mean difference.
The test for interaction between the 2 interventions yielded null results; therefore, pooled results are presented. Details of the 4 mutually exclusive treatment groups appear in eTable 3 in Supplement 2.
Adjusted for between-group differences prior to the intervention, visit, effect of the other intervention, and student and school random effects.
Defined as sum of unscheduled clinic visits, emergency department visits, and overnight hospitalizations.
No. of symptoms during the day and albuterol use and No. of symptoms during the night and albuterol use, controller treatment, lung function, and exacerbations (defined as need for systemic corticosteroids for asthma).
Adjusting for the preintervention differences between groups and the effect of the other intervention, the 2-week mean was 1.5 symptom-days with asthma after use of the school-wide IPM program vs 1.9 symptom-days after no IPM across the school year (IRR, 0.71 [95% CI, 0.38-1.33]), which was not statistically significantly different. Adjusting for the preintervention differences between groups and the effect of the other intervention, the 2-week mean was 1.6 symptom-days with asthma after use of HEPA filter purifiers in the classrooms vs 1.8 symptom-days after use of sham HEPA filter purifiers in the classrooms across the school year (IRR, 1.47 [95% CI, 0.79-2.75]), which was not statistically significantly different (Table 3). The intraclass correlation of symptom-days with asthma was estimated to be 0 at the school level and 0.22 at the student level.23
We identified that the missingness of the data was related to ethnicity (21% [28/131] of Hispanic or Latino participants had missing data for asthma symptoms vs 6% [6/100] of non-Hispanic or non-Latino participants, P = .001); therefore, the data were not missing completely at random. Inverse-probability weights based on demographics, symptom-days with asthma, and FEV1 were used to estimate the intervention effect. The 2-week mean was 1.6 symptom-days with asthma after use of the school-wide IPM program vs 1.9 symptom-days after no IPM across the school year (IRR, 0.66 [95% CI, 0.38-1.15]). The 2-week mean was 1.7 symptom-days with asthma after use of HEPA filter purifiers in the classrooms vs 1.8 symptom-days after use of sham HEPA filter purifiers in the classrooms across the school year (IRR, 1.58 [95% CI, 0.84-2.99]).
Secondary Outcomes
No statistically significant differences were found for most of the secondary outcomes. However, the difference was significant for the reduction in the number of missed school days due to asthma in the school-wide IPM program group. The 2-week mean was 0.11 missed school days due to asthma after use of the school-wide IPM program vs 0.17 days after no IPM across the school year (IRR, 0.20 [95% CI, 0.04-0.96]; Table 3).
Post Hoc Exploratory Analysis
In the post hoc exploratory analysis, there was a statistically significant improvement in the number of symptom-days with asthma for the IPM group during the first 2 postintervention visits but not during later visits. At 2 weeks’ postintervention, the 2-week mean was 1.1 symptom-days with asthma after use of the school-wide IPM program vs 2.5 symptom-days after no IPM across the school year (IRR, 0.37 [95% CI, 0.15-0.91]). At 8 weeks’ postintervention, the 2-week mean was 0.8 symptom-days with asthma after use of the school-wide IPM program vs 1.5 symptom-days after no IPM across the school year (IRR, 0.48 [95% CI, 0.23-0.99]). However, there was no statistically significant effect later in the school year. At 20 weeks’ postintervention, the 2-week mean was 1.3 symptom-days with asthma after use of the school-wide IPM program vs 1.4 symptom-days after no IPM across the school year (IRR, 0.80 [95% CI, 0.43-1.49]; Figure 2).
Figure 2. Integrated Pest Management vs No Integrated Pest Management During the School Year for the Primary Outcome of Symptom-Days With Asthma.

Data were collected from 2015 through 2020. IRR indicates incidence rate ratio.
At 2 weeks’ postintervention, the 2-week mean was 2.7 symptom-days with asthma after use of HEPA filter purifiers in the classrooms vs 2.5 symptom-days after use of sham HEPA filter purifiers in the classrooms across the school year (IRR, 1.61 [95% CI, 0.67-3.90]), which was not statistically significantly different. This effect remained null throughout the school year (eFigure 2 in Supplement 2).
Effects on Exposures After the Interventions
Use of the school-wide IPM program did not significantly reduce any of the measured allergens or particles, adjusting for differences prior to the intervention and for the use of HEPA filter purifiers in the classrooms. Use of the HEPA filter purifiers in the classrooms significantly reduced airborne mouse and dog allergen particles and other particles measured compared with the sham HEPA filter, adjusting for differences prior to the intervention and for the use of the school-wide IPM program (Table 4).
Table 4. Airborne Allergen, Particulate, and Settled Dust Allergen Exposure Outcomesa.
| Observed exposure levels after the intervention | Adjusted effect, β coefficient (95% CI)b |
Observed exposure levels after the intervention | Adjusted effect, β coefficient (95% CI)b |
|||
|---|---|---|---|---|---|---|
| IPM | No IPM | HEPA filter | Sham HEPA filter | |||
| Airborne allergen, median (10th-90th percentile), ng/m3 | ||||||
| No. of classrooms | 101 | 103 | 112 | 92 | ||
| Mouse | 0.006 (0.001 to 0.031) | 0.003 (ND to 0.020) | –0.17 (–0.51 to 0.17) | 0.003 (ND to 0.020) | 0.007 (ND to 0.038) | –0.54 (–0.88 to –0.19) |
| Cat | 0.005 (ND to 0.028) | 0.003 (ND to 0.015) | 0.41 (–0.12 to 0.94) | 0.003 (ND to 0.019) | 0.005 (ND to 0.019) | –0.34 (–0.87 to 0.19) |
| Dog | ND (ND to 0.011) | ND | 0.42 (–0.03 to 0.88) | ND | ND (ND to 0.011) | –0.62 (–1.08 to –0.17) |
| Particulate, mean (SD), μg/m3 | ||||||
| No. of classrooms | 95 | 99 | 107 | 87 | ||
| Coarse PM | 6.9 (3.3) | 6.2 (2.9) | –0.5 (–1.3 to 0.3) | 5.6 (2.7) | 7.6 (3.3) | –2.2 (–3.0 to –1.4)c |
| PM2.5 | 4.1 (3.4) | 4.1 (2.2) | 0.1 (–0.7 to 0.9) | 3.1 (3.0) | 5.3 (2.2) | –1.7 (–2.5 to –0.9)c |
| Black carbon | 0.15 (0.09) | 0.19 (0.11) | –0.02 (–0.05 to 0.01) | 0.11 (0.06) | 0.24 (0.08) | –0.12 (–0.14 to –0.09)c |
| Settled dust allergen, median (10th-90th percentile), μg/g | ||||||
| No. of classrooms | 101 | 105 | 112 | 94 | ||
| Mouse | 0.38 (0.03 to 8.83) | 0.12 (0.02 to 6.65) | –0.14 (–0.74 to 0.47) | 0.17 (0.02 to 6.40) | 0.26 (0.03 to 7.37) | –0.30 (–0.91 to 0.30)c |
| Cat | 0.14 (0.01 to 1.14) | 0.15 (0.02 to 1.42) | –0.14 (–0.68 to 0.40) | 0.12 (0.01 to 1.06) | 0.19 (0.02 to 1.44) | 0.01 (–0.53 to 0.55) |
| Dog | 0.10 (ND to 0.60) | 0.09 (0.02 to 0.48) | –0.18 (–0.63 to 0.28) | 0.09 (0.01 to 0.50) | 0.09 (0.02 to 0.51) | –0.02 (–0.48 to 0.43)c |
Abbreviations: HEPA, high-efficiency particulate air; IPM, integrated pest management; ND, not detected; PM, particulate matter.
The test for interaction between the 2 interventions yielded null results; therefore, pooled results are presented. Details of the 4 mutually exclusive treatment groups appear in eTable 4 in Supplement 2.
Adjusted for between-group differences prior to the intervention, visit, effect of the other intervention, and classroom and school random effects.
The reductions in exposure levels after use of HEPA filter vs sham HEPA filter were 31% for coarse PM, 37% for PM2.5, 54% for black carbon, 49% for mouse airborne allergens, and 36% for dog airborne allergens.
Adverse Events
There were 4 related adverse events (light-headedness, paleness, shakiness, vomiting), all of which were associated with data collection procedures and were unrelated to the interventions (eTable 5 in Supplement 2).
Discussion
In this school-based trial of children with active asthma, use of a school-wide IPM program or HEPA filter purifiers in the classrooms did not significantly reduce the number of symptom-days with asthma during a 2-week period. To our knowledge, there are no other published large-scale, school-based trials comparing use of a school-wide IPM program with use of HEPA filter purifiers in the classrooms for health outcomes. In the Mouse Allergen Asthma Intervention Trial,4 children in homes that received IPM and education vs education alone had significant reductions in exposure in both groups, therefore negating any ability to ascertain a between-group difference in the effects.
The results of the current trial suggest that the approach used to reduce mouse allergen exposure may not provide sustained health benefits in the school setting studied. The feasibility of sustained allergen reduction sufficient to improve the health of children with asthma remains to be demonstrated. Although HEPA filter purifiers reduced particle exposures (and hence allergens associated with these particles) at a similar magnitude as demonstrated in pilot work done in the same school setting,8 this reduction was not sufficient to improve health. The level of particle reduction needed to reduce symptoms in a school setting is not known. School districts have limited resources for environmental interventions and these data could inform use of IPM and HEPA filter purifiers. Classroom HEPA filter purifiers have been suggested as important to use during the COVID-19 pandemic with the perception that these will make schools safe without any objective data.
Although found in an exploratory analysis, there was an initial reduction in asthma symptoms with the school-wide IPM program, but only for a limited time (mid-November to February). Despite the typical seasonal peaks in asthma symptoms during this time as demonstrated in the control group, the school-wide IPM program alleviated these symptoms. It is possible that the reduction in mouse allergens, while reducing irritants and exposures, also reduced the susceptibility to symptomatic viral wheezing illnesses that naturally peak during this period.
Limitations
This study has several limitations. First, the amount of IPM may have been insufficient. Although the strategies used were similar to successful home-based IPM in reducing exposures,4 it may be difficult to achieve the same result in a larger school setting, and more aggressive and frequent booster visits may be required to sustain benefit. Second, the benefits of the IPM intervention may have waned as viral illness–related asthma symptoms decreased during the warmer seasons. Third, school scheduling limitations allowed dust sampling just prior to any subsequent IPM booster visits. Allergen levels measured after the intervention, but just prior to subsequent booster visits could be viewed as “peak exposure” levels and likely do not precisely reflect peak exposure reduction levels immediately after the intervention. Fourth, the schools that agreed to participate also may have been more primed for behavioral changes related to reducing mouse infestation even without the IPM intervention.
Fifth, the median classroom mouse dust allergen levels in this trial were lower than in the observational school study (median level, 0.17 μg/g vs 0.90 μg/g, respectively). However, the allergens were present in nearly all samples, and earlier observational studies have shown associations of respiratory symptoms with the presence of any detectable levels of home mouse allergen compared with no detectable mouse allergen.24 Sixth, the study focused on a general group of students with active asthma regardless of sensitization or baseline symptoms (determined based on previous observational data7).
Conclusions
Among children with active asthma, use of a school-wide IPM program or classroom HEPA filter purifiers did not significantly reduce symptom-days with asthma. However, interpretation of the study findings may need to consider allergen levels, particle exposures, and asthma symptoms at baseline.
Trial protocol and statistical analysis plan
eFigure 1. Annual protocol schema: seasonal recruitment and factorial design
eFigure 2. HEPA versus Sham HEPA over the school year for the study population for primary outcome of asthma symptom days in the past 2 weeks
eTable 1. Detailed inclusion/exclusion criteria
eTable 2. Assay performance
eTable 3. Asthma outcomes in mutually exclusive treatment groups
eTable 4. Exposure outcomes in mutually exclusive treatment groups
eTable 5. Adverse events
eAppendix
eReferences
Nonauthor Collaborators. Members of the School Inner-City Asthma Intervention study team
Data sharing statement
References
- 1.Del-Rio-Navarro BE, Navarrete-Rodríguez EM, Berber A, Reyes-Noriega N, García-Marcos Álvarez L; Grupo GAN México, Grupo ISAAC México . The burden of asthma in an inner-city area: a historical review 10 years after Isaac. World Allergy Organ J. 2020;13(1):100092. doi: 10.1016/j.waojou.2019.100092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rabito FA, Carlson JC, He H, Werthmann D, Schal C. A single intervention for cockroach control reduces cockroach exposure and asthma morbidity in children. J Allergy Clin Immunol. 2017;140(2):565-570. doi: 10.1016/j.jaci.2016.10.019 [DOI] [PubMed] [Google Scholar]
- 3.DiMango E, Serebrisky D, Narula S, et al. Individualized household allergen intervention lowers allergen level but not asthma medication use: a randomized controlled trial. J Allergy Clin Immunol. 2016;4(4):671-679,e4. doi: 10.1016/j.jaip.2016.01.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Matsui EC, Perzanowski M, Peng RD, et al. Effect of an integrated pest management intervention on asthma symptoms among mouse-sensitized children and adolescents with asthma: a randomized clinical trial. JAMA. 2017;317(10):1027-1036. doi: 10.1001/jama.2016.21048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Olson C, Leu CS, Alper H, Millican M, Reznik M. A randomized trial of a one-time pest intervention: impact on childhood asthma outcomes. J Asthma. 2021;58(5):616-624. doi: 10.1080/02770903.2019.1709870 [DOI] [PubMed] [Google Scholar]
- 6.Riederer AM, Krenz JE, Tchong-French MI, et al. Effectiveness of portable HEPA air cleaners on reducing indoor PM2.5 and NH3 in an agricultural cohort of children with asthma: a randomized intervention trial. Indoor Air. 2021;31(2):454-466. doi: 10.1111/ina.12753 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sheehan WJ, Permaul P, Petty CR, et al. Association between allergen exposure in inner-city schools and asthma morbidity among students. JAMA Pediatr. 2017;171(1):31-38. doi: 10.1001/jamapediatrics.2016.2543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jhun I, Gaffin JM, Coull BA, et al. School environmental intervention to reduce particulate pollutant exposures for children with asthma. J Allergy Clin Immunol. 2017;5(1):154-159,e3. doi: 10.1016/j.jaip.2016.07.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Phipatanakul W, Koutrakis P, Coull BA, et al. The School Inner-City Asthma Intervention Study: design, rationale, methods, and lessons learned. Contemp Clin Trials. 2017;60:14-23. doi: 10.1016/j.cct.2017.06.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Redline S, Gruchalla RS, Wolf RL, et al. Development and validation of school-based asthma and allergy screening questionnaires in a 4-city study. Ann Allergy Asthma Immunol. 2004;93(1):36-48. doi: 10.1016/S1081-1206(10)61445-7 [DOI] [PubMed] [Google Scholar]
- 11.Morgan WJ, Crain EF, Gruchalla RS, et al. ; Inner-City Asthma Study Group . Results of a home-based environmental intervention among urban children with asthma. N Engl J Med. 2004;351(11):1068-1080. doi: 10.1056/NEJMoa032097 [DOI] [PubMed] [Google Scholar]
- 12.Rosenstreich DL, Eggleston P, Kattan M, et al. The role of cockroach allergy and exposure to cockroach allergen in causing morbidity among inner-city children with asthma. N Engl J Med. 1997;336(19):1356-1363. doi: 10.1056/NEJM199705083361904 [DOI] [PubMed] [Google Scholar]
- 13.American Academy of Allergy and Immunology Board of Directors . Allergen skin testing. J Allergy Clin Immunol. 1993;92(5):636-637. doi: 10.1016/0091-6749(93)90004-Y [DOI] [PubMed] [Google Scholar]
- 14.American Thoracic Society . Standardization of spirometry: 1994 update. Am J Respir Crit Care Med. 1995;152(3):1107-1136. [DOI] [PubMed] [Google Scholar]
- 15.Wu TD, Perzanowski M, Peng RD, et al. Validation of the maximum symptom day among children with asthma. J Allergy Clin Immunol. 2019;143(2):803-805,e10. doi: 10.1016/j.jaci.2018.10.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Busse WW, Morgan WJ, Gergen PJ, et al. Randomized trial of omalizumab (anti-IgE) for asthma in inner-city children. N Engl J Med. 2011;364(11):1005-1015. doi: 10.1056/NEJMoa1009705 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wildfire JJ, Gergen PJ, Sorkness CA, et al. Development and validation of the Composite Asthma Severity Index—an outcome measure for use in children and adolescents. J Allergy Clin Immunol. 2012;129(3):694-701. doi: 10.1016/j.jaci.2011.12.962 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Krouse RZ, Sorkness CA, Wildfire JJ, et al. Minimally important differences and risk levels for the Composite Asthma Severity Index. J Allergy Clin Immunol. 2017;139(3):1052-1055. doi: 10.1016/j.jaci.2016.08.041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Szefler S, Weiss S, Tonascia J, et al. ; Childhood Asthma Management Program Research Group . Long-term effects of budesonide or nedocromil in children with asthma. N Engl J Med. 2000;343(15):1054-1063. doi: 10.1056/NEJM200010123431501 [DOI] [PubMed] [Google Scholar]
- 20.Goldstein H. Multilevel Statistical Models. 3rd ed. Arnold; 2003. [Google Scholar]
- 21.Applied Longitudinal Analysis. Wiley & Sons; 2011. [Google Scholar]
- 22.Phipatanakul W, Eggleston PA, Wright EC, Wood RA. Mouse allergen, II: the relationship of mouse allergen exposure to mouse sensitization and asthma morbidity in inner-city children with asthma. J Allergy Clin Immunol. 2000;106(6):1075-1080. doi: 10.1067/mai.2000.110795 [DOI] [PubMed] [Google Scholar]
- 23.Tseloni A, Pease K. Repeat personal victimization: random effects, event dependence and unexplained heterogeneity. Br J Criminol. 2004;44(6):931-945. doi: 10.1093/bjc/azh047 [DOI] [Google Scholar]
- 24.Phipatanakul W, Celedon JC, Hoffman EB, Abdulkerim H, Ryan LM, Gold DR. Mouse allergen exposure, wheeze and atopy in the first seven years of life. Allergy. 2008;63(11):1512-1518. doi: 10.1111/j.1398-9995.2008.01679.x [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial protocol and statistical analysis plan
eFigure 1. Annual protocol schema: seasonal recruitment and factorial design
eFigure 2. HEPA versus Sham HEPA over the school year for the study population for primary outcome of asthma symptom days in the past 2 weeks
eTable 1. Detailed inclusion/exclusion criteria
eTable 2. Assay performance
eTable 3. Asthma outcomes in mutually exclusive treatment groups
eTable 4. Exposure outcomes in mutually exclusive treatment groups
eTable 5. Adverse events
eAppendix
eReferences
Nonauthor Collaborators. Members of the School Inner-City Asthma Intervention study team
Data sharing statement