

Abstract
Objective:
To examine psychological health as a mechanism linking economic pressure and marital instability in the early middle years to poor physical health in later life.
Background:
Although previous research suggests that sustained stressful marital experience may lead to mental and physical health problems, little is known about how contextual factors, such as economic pressure, impact marital outcomes, and how changes in marital attributes influence health outcomes in a longitudinal and dyadic context.
Method:
Utilizing an actor-partner interdependence model within a latent growth curve approach and prospective data from couples in enduring marriages, we examined the associations between family economic pressure, marital instability, and mental health over their early middle years (1989–1994) and subsequent physical health in later adulthood (2015). Analyses assessed a couple-level pathway and an individual pathway involving within-spouse and between-spouse effects.
Results:
During the middle years, family financial difficulties were linked to reduced marital stability, which was associated with increased mental health challenges. The findings also reinforced the salient role of psychological distress for subsequent physical health outcomes as husbands’ and wives’ anxiety symptoms over their early middle years contributed to declines in their physical health outcomes in later adulthood. A partner effect was noted between husbands’ anxiety and wives’ physical health.
Conclusion:
For couples, experiences of financial and marital stress in their early middle years can have long-lasting detrimental impacts on their physical health in later adulthood.
Keywords: couples, longitudinal research, marital relations, mental health, physical health, stress
Background
Research has documented the strong connection between marital stress and health (Kiecolt-Glaser & Wilson, 2017; Whisman & Baucom, 2012). In addition, marital scholars have noted the adverse effects of contextual stressors surrounding couples, such as financial hardship, and the role of relationships in explaining the stress-health connection (Conger & Conger, 2002; Wickrama et al., 2018). More specifically, financial hardship is thought to lead to marital instability because it requires couples to engage in undesired resource management (i.e., reducing living expenses, finding a second job) that couples may disagree on. Numerous studies have also shown that financial stress is associated with declines in positive marital interactions, which can result in increased marital instability (Barton & Bryant, 2016; Gudmunson et al., 2007). In turn, marital instability is a stressor itself and can create psychological distress (Umberson et al., 2006), which explains why, over time, chronic marital stress can put husbands and wives at a greater risk for developing mental and physical health problems (Kiecolt-Glaser & Wilson, 2017; Robles et al., 2014).
This body of research has shown how contextual factors (e.g., financial stress) impact marital outcomes and how changes in marital attributes influence mental health. However, past studies have been fragmented and have largely focused on how marital outcomes/processes and psychological distress are connected over short periods of time (Barton & Bryant, 2016; Falconier et al., 2015; Neff & Karney, 2017; Wickrama et al., 2018). Less research has examined these influences in a single, unified analytic approach considering complex associations longitudinally, which would provide a more comprehensive understanding of the linkages between contextual stressors, marital instability, psychological distress, and physical health. Thus, there is a need for comprehensive research that is longitudinal and dyadic to elucidate the pathways that link contextual factors and related stressful life events to marital attributes and subsequent mental and physical health outcomes (Robles et al., 2014).
The conceptual framework of the current study is shown in Figure 1. The framework draws from several theories of marriage and health, including the vulnerability-stress-adaptation (VSA) model (Karney & Bradbury, 1995), a neurobiological stress-health perspective (McEwen, 1998; McEwen & Gianaros, 2010), and family systems theory (O’Brien, 2005). The VSA model explains how stressful life circumstances influence adaptive marital processes and marital outcomes, which are thought to be consequential for psychological and physical health (Kiecolt-Glaser & Wilson, 2017). Neurobiological research provides evidence of how psychological distress impacts physical health.
Figure 1.
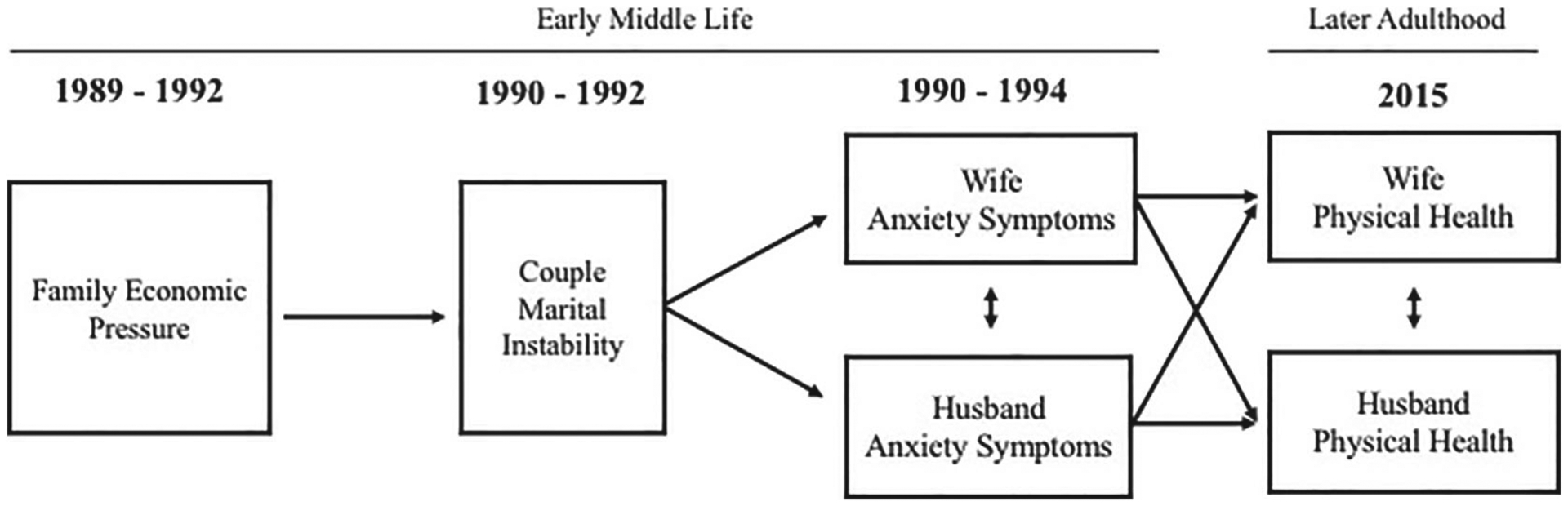
Conceptual Model.
Consistent with family systems theory (O’Brien, 2005), experiences of family financial stress are conceptualized as a family phenomenon with numerous consequences for families and their individual members. For instance, financial stress may impact couple functioning, including deteriorations in marital quality and, consequently, marital instability. Also, as spouses interact with each other daily, their experiences of emotional stress are communicated to one another, and, as such, their stressful experiences are interdependent (Beach et al., 2003; Randall & Bodenmann, 2009). That is, one partner’s thoughts and feelings of marital instability may transfer to his/her spouse, contributing to the spouse’s perceptions of marital instability. Because spouses’ perceptions of marital instability are closely interconnected, in the current study, we conceptualize marital instability as a couple-level construct. This conceptualization is consistent with recent family and social relationship research focused on couple-level constructs in dyadic analyses (Galovan et al., 2017; Ledermann & Kenny, 2012). Couple-level constructs reflect couple members’ shared experiences, measured by the shared variance between couple members. Recent research has shown that couple-level constructs (i.e., common fate model; Ledermann & Kenny, 2012) often have stronger predictive power when compared to spouses’ individual-level constructs for the same variable of interest (Lee et al., 2019; Wickrama et al., 2019).
Furthermore, marital attributes (e.g., marital instability) have consequences for both spouses’ psychological health (Nealey-Moore et al., 2007) as stressful experiences and psychological responses can be reciprocally transferred between spouses. Over time, these negative stress responses may escalate and become entrenched, with detrimental consequences for both partners’ physical health in later life. Utilizing a couple-level construct of marital instability and growth curves within an actor-partner interdependence model (APIM; Kenny et al., 2006) approach is well-suited to address these hypothesized dyadic processes linking financial stress, marital instability, psychological health, and physical health with the current sample of middle-aged couples.
Family Economic Pressure and Marital Instability
One specific component of family financial stress is family economic pressure as adverse financial events (e.g., low income, job loss) often force couples to make unexpected adjustments, such as borrowing money to help pay bills, selling property to raise money, or relocating to more affordable housing. This economic pressure and the stress associated with these changes may increase tension between spouses over time, leading to marital discord. In fact, research has shown that financial concerns are often the most common topic of marital disagreement (Papp et al., 2009). Marital conflicts related to finances have been shown to increase emotional distress and hostile behaviors between spouses (Conger et al., 1994), which, in turn, are implicated in reduced positive interactions (e.g., quality time, social support) and increased marital instability (Barton & Bryant, 2016; Gudmunson et al., 2007).
Compared to episodic financial problems, prolonged (or continuous) economic pressure may be particularly detrimental (Kahn & Pearlin, 2006). Couples with chronic economic pressure are likely to feel trapped and unable to escape from their economic difficulties. Recent research highlighted a cumulative negative impact of sustained financial hardship on individuals’ later health (Kahn & Pearlin, 2006). Thus, focusing on the cumulative effects of long-term family financial stress exposure on marriage, the present study investigates (a) trajectories of family economic pressure over time (measuring trajectories through growth curve modeling to refer to the initial level in 1989 and change over the early middle years from 1989–1992); (b) associations between trajectories of family economic pressure and couple-level trajectories of marital instability (1990–1992).
Marital Instability and the Development of Anxiety Symptoms
The psychological effects of negative marital attributes have been demonstrated, including elevated feelings of anger and anxiety (Nealey-Moore et al., 2007). Consistent with family systems theory (O’Brien, 2005), the psychological effects may be partly attributed to the cyclical nature of negative interactions; that is, one partner’s negativity often elicits negativity from their partner, enabling unhealthy interpersonal trajectories to become established and continue over time. These sustained negative patterns can be a source of chronic stress and result in marital instability; both of which are detrimental to psychological health (Wickrama et al., 2019). For instance, decreases in supportive marital interactions over time are closely related to husbands’ and wives’ marital instability (Barton & Bryant, 2016; Guilbert et al., 2000) and have long-term consequences for mental health (Wickrama et al., 2018). The cyclical nature of the dyadic context between spouses can promote further relational stress and also fosters shared perceptions of marital characteristics, including couple-level marital instability. Previous research also supports that emotional similarity exists between spouses due to the shared stressful life experiences, and this concordance of emotional attributes between partners generally increases with age as marital relationships became more salient (Kiecolt-Glaser & Wilson, 2017). Thus, spouses’ experiences of unstable marital relationships may be intertwined and become firmly established over time, creating similar patterns of trajectories of marital instability between husbands and wives.
These trajectories of marital instability may exacerbate negative emotions, such as anxiety, anger, sadness, and fear. Such feelings of anger and irritability can contribute to poor psychological health, particularly anxiety symptoms (Deschênes et al., 2012; Hawkins & Cougle, 2011), which is consistent with research demonstrating a strong association between marital distress and a wide range of mood and anxiety disorder symptoms (Whisman, 2007). Consequently, over their early middle years, we expect that couples’ marital instability trajectories are positively associated with husbands’ and wives’ subsequent trajectories of anxiety symptoms (measuring trajectories through growth curve modeling to refer to the initial level in 1990 and change over time from 1990–1994).
Anxiety Symptoms and Physical Health
Anxiety stemming from psychosocial stressors provokes arousal in the autonomic nervous system (Ulrich-Lai & Herman, 2009). Although arousal is adaptive because it promotes the circulation of hormones in the bloodstream, repeated and continuous arousal is associated with hypertension and a proinflammatory state, which can be risk factors for coronary heart disease and other negative health outcomes (Player & Peterson, 2011). Moreover, through neuroendocrine pathways, the body works to maintain homeostasis in various cardiovascular, metabolic, and immune systems, but these systems are taxed when psychosocial stressors activate these regulatory processes. When chronically overworked, these regulating processes can accelerate functional impairments and increase susceptibility to illness (Kiecolt-Glaser et al., 2002; McEwen, 1998). For instance, prolonged and frequent heightened anxiety is associated with increased cardiovascular reactivity in response to stressors, which results in a greater risk of future heart disease and faster disease progression (Treiber et al., 2003). The current study extends on this work by examining how husbands’ and wives’ trajectories of anxiety in their early middle years, as a consequence of marital instability, contribute to physical health problems in later adulthood.
Additionally, family systems theory (O’Brien, 2005) and the APIM approach (Kenny et al., 2006), highlight the interdependent nature of couples, which can include “physiological linkages” between couple members’ physiological responses to stress (Timmons et al., 2015). That is, emotional distress often increases an individual’s physiological arousal, and his/her partner may respond in a similar physiologic manner, which can prompt even greater increases in physiological activation in the first spouse. This physiological linkage between spouses can occur across an extensive range of physiological indices (blood pressure, cortisol, pulse, heart rate) (Timmons et al., 2015). For instance, the connection between spouses’ physiological reactivity has been observed for cortisol levels (Saxbe & Repetti, 2010) and respiratory and heart rate (Helm et al., 2012). Previous research has also shown that relationship satisfaction is associated with the cortisol linkage between spouses (Saxbe & Repetti, 2010) with greater physiological activation (and consequently increased risk for poor health) for less satisfied couples. We suspect that husbands’ and wives’ sustained psychological distress, including anxiety symptoms resulting from marital instability, will be closely associated with both partners’ physical health in their later years.
The Present Study
The conceptual model in Figure 1 illustrates how trajectories of family economic pressure are thought to shape couple-level trajectories of marital instability over time, and marital instability is thought to create long-term distress that results in more anxiety symptoms for husbands and wives. Ultimately, these trajectories of anxiety symptoms over time are expected to impact their own physical health (a latent construct capturing self-rated global health and physical illness) in later life as well as the physical health of their partner.
Hypothesis 1: Trajectories of family economic pressure will be positively associated with couple-level trajectories of marital instability over the early middle years.
Hypothesis 2: Couples’ marital instability trajectories will be positively associated with husbands’ and wives’ trajectories of anxiety symptoms over the early middle years.
Hypothesis 3: Husbands’ and wives’ trajectories of anxiety symptoms over the early middle years will be positively associated with their own physical health and that of their partner in later adulthood.
Method
Sample
The data used to examine these hypotheses come from couples who originally participated in the Iowa Youth and Family Project (IYFP) between 1989 and 1994 and continued to participate in the Iowa Midlife Transitions Project (MTP) in 2001 and the Later Adulthood Study (LAS) in 2015. The purpose of the IYFP was to understand the impact of financial hardship (particularly the farm crisis) on changes in family life, including parent–child relationships, marital relationships, children’s developmental outcomes, and the physical/psychological well-being of family members (Conger & Elder, 1994). The families meeting the selection criteria (i.e., couples living together with at least one target child in the seven grade and a sibling within 4 years of age of the target child, if the target child had) were identified and randomly selected through area schools located in rural communities in north-central Iowa. Eligible families were recruited, with about 78% of the couples agreeing to participate in the study (Conger & Elder, 1994). Consent of the families was obtained, and trained field interviewers visited families at their homes; during the visits, each family member was independently asked about family economic circumstances, relationships between family members, and their individual well-being.
At the first measurement occasion (1989), the median ages for husbands and wives were 39 and 37 years, respectively. The median years of education for both husbands and wives were 13 years, and couples had been married for at least 17 years. As there were very few minorities in rural areas, all participating couples were White, heterosexual married couples. From the larger sample of couples, the present study utilized data from 370 couples (82% of the original sample) who remained married to the same partner (from 1989 to 2001; over 20 years) and participated in multiple waves of data collection (from 1989 to 1994, and 2015).
Measures
Family Economic Pressure.
In 1989, 1990, 1991, and 1992, husbands and wives were asked to respond “yes” or “no” to each of the 22 items on experienced economic problems based on the question (Dohrenwend et al., 1978), “During the past 12 months, has your family made any of the following adjustments because of financial need?” The list of the economic problems included items such as “used savings to meet daily living expenses,” “changed food shopping or eating habits to save money,” “received government assistance,” and “borrowed money to help pay bills.” The measure was constructed by summing husbands’ and wives’ “yes” responses (1 = yes, 0 = no) to reflect family economic pressure in their early middle years; higher scores indicate more family economic pressure.
Marital Instability.
In 1990, 1991, and 1992, husbands and wives responded to the 5-item Marital Instability Index (Booth et al., 1983) to indicate their thoughts of divorce or separation during the past months on a 4-point scale ranging from 1 (not in the last year) to 4 (within the last 3 months). Sample items include “have you or your wife even seriously suggested the idea of divorce?” and “has the thoughts of separating or getting a divorce crossed your mind?” Separately for husbands and wives, at each time point, responses were averaged with higher scores representing a higher level of marital instability (Cronbach’s α’s ranged from .81 to .96, respectively, across years).
Anxiety Symptoms.
In 1990, 1991, 1992, and 1994, 10 items from the Symptoms Check-List-90-Revised (SCL-90-R) anxiety scale (Derogatis, 1996) assessed husbands’ and wives’ distress during the previous week. Respondents were asked to indicate their distress on a 5-point scale ranging from 1 (not at all) to 5 (extremely). Sample items include “feeling fearful” and “feeling tense or keyed up.” At each timepoint, separately for husbands and wives, an average was computed with higher scores reflecting more anxiety (Cronbach’s α’s ranged from .83 to .93 for husbands and wives across years).
Physical Health.
A latent variable was constructed to assess respondents’ physical health in later adulthood using data collected in 2015, capturing global physical health and physical illness. For global physical health, husbands and wives indicated their global physical health using one item on a 5-point scale included; “How would you rate your overall physical health” (1 = excellent; 5 = poor), with higher scores representing poorer global physical health. Physical illness was measured by a count of self-reported and physician-diagnosed symptoms or diseases from a list of 56 illnesses (e.g., asthma, irregular heartbeats, high blood pressure, chest pain, blood clot in lungs, blood clot in vessels, heart attack, breast cancer, high cholesterol). Husbands and wives were asked to indicate whether they had experienced any of the symptoms or illnesses during the past 2 years (1 = yes; 0 = no). Separately for husbands and wives, a sum score was computed with higher scores representing more illness or chronic health problems. A similar latent construct from 1990 was included in our analysis as a control variable to account for early physical health when explaining physical health in later adulthood.
Analysis
Structural equation modeling (SEM) was used to address the research hypotheses in three phases. First, five univariate growth curves were estimated separately (i.e., family economic pressure from 1989 to 1992, husbands’ and wives’ marital instability from 1990 to 1992, and anxiety symptoms of husbands and wives from 1990 to 1994). These growth curve analyses provided information on the initial level and rate of change over time. At the same time, these analyses were useful for identifying if there was sufficient variability within the sample to test the hypothesized model. Second, a second-order growth curve was estimated to reflect the longitudinal change in couple-level marital instability using a factor-of-curves approach (FCM; Wickrama et al., 2016). For the model specification, the second-order initial level factor was estimated using husbands’ and wives’ initial level growth factors. Likewise, the second-order rate of change factor was estimated using husbands’ and wives’ rate of change in marital instability as indicators. Third, the hypothesized model was tested within an SEM framework to explain how marital instability and anxiety symptoms operate as mechanisms linking family economic pressure to physical health in later adulthood (see the conceptual model in Figure 1 as a reference to the tested model). The statistical significance of indirect effects between family economic pressure and physical health were examined.
All analyses were performed using Mplus (version 8.0; Muthén & Muthén, 2017). Approximately 10% of participants had some missing data. In order to manage these missing cases, we used full information maximum likelihood (FIML). This approach improves the power and the accuracy of the analysis in comparison to other methods handling missing data (e.g., list-wise deletion) (Enders, 2010). When the root mean square error of approximation (RMSEA) value is close to or less than .06 and the comparative fit index (CFI) value is close to or greater than .95 (favorable = .90), the model is thought to fit the data well (Hu & Bentler, 1999).
Results
Descriptive Statistics
Table 1 displays the descriptive statistics and the correlations for measures of family economic pressure, marital instability, anxiety symptoms, and indicators of physical health. The mean values of family economic pressure ranged over time from 12.09 to 13.35 (capturing 1989 to 1992). Mean score comparisons were conducted for husbands and wives at each time point. For marital instability, these comparisons revealed no statistical differences, indicating that husbands and wives experienced similar levels of marital instability. However, gender differences were noted for anxiety symptoms. Wives reported slightly higher levels of anxiety symptoms at each measurement occasion (1990, 1991, 1992, and 1994). For both husbands and wives, global physical health was significantly correlated with physical illness in 2015.
Table 1.
Correlation Matrix and Descriptive Statistics for Study Variables (N = 370 Married Couples)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FEP | ||||||||||||||
| 1. 1989 | – | .94** | .87** | .90** | .10 | .16** | .13* | .94** | .05 | .21** | .96** | .94** | .00 | .01 |
| 2. 1990 | .94** | – | .89** | .86** | .12* | .06 | .06 | 1.0** | .17** | .22** | .90** | 1.0** | −.05 | .00 |
| 3. 1991 | .87 | .89** | – | .83** | .02 | .16** | −.10 | .89** | .48** | .24** | .85** | .89** | −.01 | −.01 |
| 4. 1992 | .90** | .87** | .83** | – | .02 | .02 | .13* | .86** | .13** | .47** | .86** | .86** | .01 | .06 |
| Marital instability | ||||||||||||||
| 5. 1990 | .05 | .06 | .02 | .05 | – | .52** | .40** | .15** | .02 | −.05 | −.18** | .06 | .03 | −.02 |
| 6. 1991 | .08 | .01 | .19** | .05 | .54** | – | .55** | .04 | .36** | −.15** | −.08 | .04 | .17* | .07 |
| 7. 1992 | .12* | −.20** | −.05 | .11* | .37** | .44** | – | .06 | −.10 | .23** | .29** | .06 | .10 | .03 |
| Anxiety symptoms | ||||||||||||||
| 8. 1990 | .93** | .99** | .88** | .86** | .26** | −.01 | −.21** | – | .17** | .22** | .91** | 1.0** | −.05 | .00 |
| 9. 1991 | .04 | .16** | .47** | .12* | .01 | .33** | −.06 | .16** | – | .08 | .08 | .17** | −.03 | .03 |
| 10. 1992 | .14** | .21** | .26** | .34** | −.10 | −.12* | .12* | .23** | .29** | – | 26** | .22** | .04 | .11 |
| 11. 1994 | .77** | .77** | .75** | .75** | −.13* | −.24** | −.17** | .78** | .19** | .41** | – | .91** | −.01 | .00 |
| Physical health | ||||||||||||||
| 12. Global health 90 | .94** | 1.0** | .89** | .86** | .05 | −.01 | −.21** | .99** | .16** | .21** | .77** | – | −.05 | .00 |
| 13. Global health 15 | −.10 | −.12 | −.15* | −.10 | .10 | .07 | .02 | −.12 | −.16* | −.06 | −.12 | −.12 | – | .48** |
| 14. Illness 2015 | .05 | .06 | .10 | .02 | .12 | −.01 | −.00 | .06 | .16* | .07 | .08 | .06 | .42** | – |
| FEP M (SD) | 13.35 (9.81) |
12.40 (9.55) |
12.74 (10.07) |
12.09 (9.24) |
– | – | – | – | – | – | – | – | – | – |
| Wives M (SD) | – | – | – | – | 1.27 (0.61) |
1.29 (0.58) |
1.24 (0.52) | 1.26a (0.36) |
1.29a (0.42) |
1.25a (0.40) |
1.26a (0.41) |
2.07a (0.81) |
2.55a (0.95) |
3.04a (2.69) |
| Husbands M (SD) | – | – | – | – | 1.22 (0.49) |
1.24 (0.49) |
1.22 (0.47) | 1.18a (0.26) |
1.19a (0.34) |
1.17a (0.35) |
1.17a (0.31) |
2.22a (0.87) |
2.82a (0.98) |
3.72a (2.93) |
Note: FEP = family economic pressure. Correlations for wives are above the diagonal. Correlations for husbands are below the diagonal. Means (M) and standard deviations (SD)are presented at the bottom of the table. Letter superscripts on mean values denote significant gender differences.
p < .05.
p < .01.
Univariate Growth Curves and a Factor-of-Curves Model (FCM)
The growth curve parameter estimates for family economic pressure, marital instability, and anxiety symptoms of husbands and wives are presented in Table 2. For each of these growth curves, the variances for the initial level and rate of change growth factors were statistically significant, indicating the existence of interindividual variability in both their initial level and rate of change over time. Although the mean rates of change in marital instability (1990–1992) and anxiety symptoms (1990–1994) were not significant (i.e., on average, across the sample marital instability did not change over time), the significant variance coefficient indicates that some individuals experienced increasing marital instability (and anxiety symptoms) while others experienced decreases in marital instability (and anxiety symptoms) over time.
Table 2.
Results From Univariate Growth Curves of Family Economic Pressure and Husbands’ and Wives’ Marital Instability and Anxiety Symptoms (N = 370 Married Couples)
| Initial level | Rate of change | RMSEA/CFI | |||
|---|---|---|---|---|---|
| Mean | Variance | Mean | Variance | ||
| Family economic pressure (1989, 1990, 1991, 1992) | 13.25 *** | 75.61 *** | −0.38 * | 5.23 ** | .05/.99 |
| Husbands | |||||
| Marital instability (1990, 1991, 1992) | 1.22 *** | 0.18 *** | −0.01 | 0.04 ** | .02/1.00 |
| Anxiety symptoms (1990, 1991, 1992, 1994) | 1.18 *** | 0.11 *** | 0.00 | 0.01 *** | .00/1.00 |
| Wives | |||||
| Marital instability (1990, 1991, 1992) | 1.28 *** | 0.24 *** | −0.01 | 0.05 ** | .05/1.00 |
| Anxiety symptoms (1990, 1991, 1992, 1994) | 1.26 *** | 0.09 *** | −0.00 | 0.01 *** | .04/1.00 |
Note: RMSEA = root mean square error of approximation. CFI = comparative fit index.
p < .05.
p < .01.
p < .001.
Next, an FCM was estimated to assess the initial level and rate of change in marital instability at the couple level from husbands’ and wives’ marital instability growth curves. This second-order model was a good fit to the data (CFI = .95, RMSEA = .06), χ2 (df) = 34.47(13). There was significant variability (p < .01) in the rate of change in couple marital instability from 1990 to 1992, indicating variation in couple-level marital instability over time across the sample.
Testing the Hypothesized Model
As shown in Figure 2, when the hypothesized model was estimated, the initial level of family economic pressure (1989) was related to the initial level of couple marital instability (1990) (β = .22, p < .01). Similarly, the rate of change in family economic pressure (1989–1992) was associated with the rate of change in couple marital instability (1990–1992) (β = .15, p < .05, respectively). Thus, couples with a higher level of family economic pressure generally experienced higher levels of marital instability concurrently, and couples with more rapid changes (i.e., a steeper slope) in family economic pressure from 1989 to 1992 tended to experience similar changes (i.e., more rapid changes) in their marital instability from 1990 to 1992.
Figure 2.
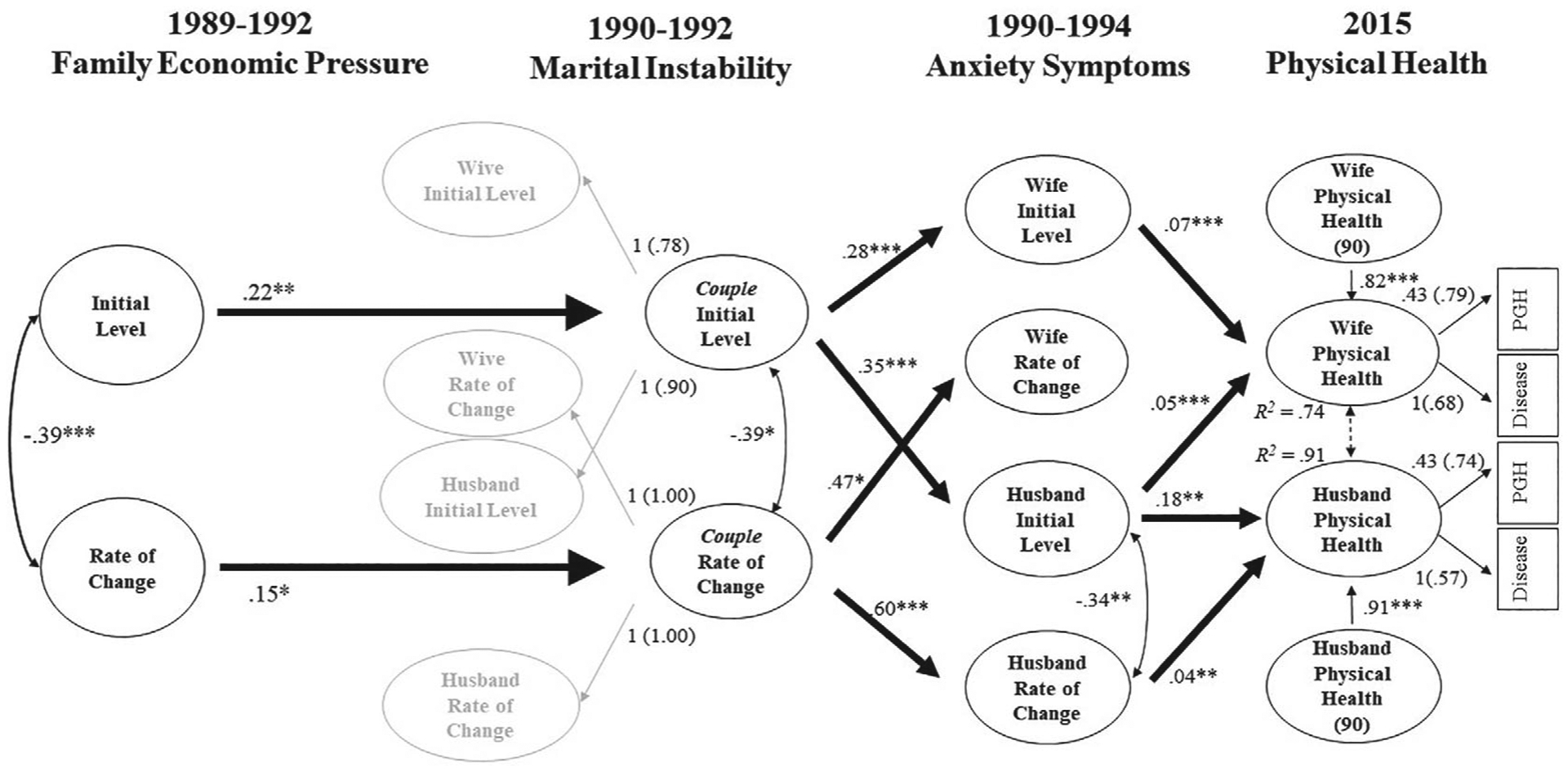
The Influence of Longitudinal Changes of Family Economic Pressure, Couple Marital Instability, and Husbands’ and Wives’ Anxiety Symptoms Over Midlife on Physical Health in Later Adulthood.
Note: Standardized Coefficients Are Shown With Standardized Loadings in Parentheses. All Loadings Were Significant at p < .001. PGH = Physical Global Health. Nonsignificant Paths and Correlations Are Not Shown. CFI = .93; RMSEA = .05.
*p < .05. **p < .01. ***p < .001.
In turn, the level of and the rate of change in couple marital instability was related to the subsequent anxiety symptoms of both spouses. More specifically, the initial level of marital instability (1990) was contemporaneously associated with both wives’ and husbands’ initial levels of anxiety symptoms (1990) (β = .28, p < .001 and β = .35, p < .001, for wives and husbands, respectively). That is, in couples with more marital instability, husbands’ and wives’ generally reported more anxiety symptoms compared to spouses with less marital stability. For both spouses, the rate of change in marital instability (1990–1992) was also related to the rate of change in their own anxiety symptoms (1990–1994) (β = .47, p < .05 and β = .60, p < .001, for wives and husbands, respectively). These findings provide strong evidence for parallel trajectories of couple marital instability and spouses’ anxiety symptoms over time.
Furthermore, linkages between husbands’ and wives’ anxiety symptoms and their physical health in later adulthood (2015) were also evident. Both the initial level of husbands’ anxiety symptoms (1990) and the rate of change in their anxiety symptoms (1990–1994) were consequential for their poor physical health in later adulthood (2015) (β = .18, p < .01 for the level; β = .04, p < .01, for the rate of change, respectively). For wives’ physical health, the initial level of both spouses’ anxiety symptoms was related to poor physical health in later adulthood (2015) (β = .07, p < .001 for wives’ anxiety; β = .05, p < .001 for husbands’ anxiety). In addition, we tested the equivalence of the partner effects (i.e., the influence of the initial level of husbands’ anxiety on wives’ physical health compared to the influence of the initial level of wives’ anxiety on husbands’ physical health) utilizing a chi-square difference test. The results indicated a statistically significant difference in the two partner effects (Δχ2 (2, N = 370) = 9.36, p < .05), reflecting a significant gender difference in the partner effects. That is, the initial level of husbands’ anxiety was implicated in their wives’ physical health in 2015, but wives’ anxiety was not related to husbands’ physical health in later adulthood.
It is notable that these associations between anxiety symptoms and physical health in later adulthood emerged after controlling for husbands’ and wives’ poor physical health earlier in their early middle years (1990). Consequently, the results identify the extent to which anxiety symptoms were related to changes in physical health from early middle years to later adulthood. Furthermore, the longitudinal associations between earlier and later physical health were large (β = .91, p < .001 and β = .82, p < .001 for husbands and wives, respectively), which indicates significant stability in the rank-ordering of physical health over the life course (i.e., those in the sample with the poorest health compared to others in 1990 generally had the poorest health in 2015). Thus, these findings indicate that health trajectories are largely established by the middle years, yet even when accounting for this stability, trajectories of anxiety symptoms emerged as significant determinants of later life physical health. The hypothesized model predicting husbands’ and wives’ poor physical health in later adulthood was an acceptable fit to the data (χ2 (df) = 553.02(287), CFI = .93 RMSEA = .05). The model explained 91% and 74% of the variance in husbands’ and wives’ self-rated physical health, respectively in 2015.
In examining the statistical significance of indirect effects within the model, the initial level of family economic pressure (1989) was indirectly related to wives’ physical health in later adulthood (2015) through the initial level of couple marital instability (1990) and husbands’ initial level of anxiety symptoms (1990) (indirect effect [I.E.] = .02; p = .05). A similar pattern was noted for the indirect effects linking the initial level of family economic pressure (1989) to wives’ physical health (2015) through the initial level of couple marital instability (1990) and wives’ initial level of anxiety symptoms (1990) (I.E. = .02; p = .05). Indirect effects for husbands’ physical health in later adulthood were not statistically significant.
Discussion
The connection between marital attributes and health outcomes has become a central theme in marital research (Kiecolt-Glaser & Wilson, 2017; Robles et al., 2014). Although various mechanisms underlying these associations have been identified, studies have predominantly focused on marital quality or status with fewer studies taking a long view to identify influences of contextual factors, such as economic pressure, on marital attributes and how specific aspects of marital relationships lead to psychological distress and poor physical health decades later. Furthermore, there is a need for comprehensive research integrating previous piece-meal studies to provide a more complete understanding of stress-marriage-health processes, particularly considering intraindividual and interindividual associations simultaneously. Thus, with prospective data from couples in marriages, an APIM (Kenny et al., 2006) with growth curves in an SEM framework was utilized to examine how chronic family economic pressure shaped couple-level marital instability trajectories and, eventually, their physical health through their psychological health.
Consistent with the VSA model (Karney & Bradbury, 1995), our findings demonstrated family economic pressure is a contextual factor that contributes to increased marital instability (Hypothesis 1). In turn, marital stability was implicated in subsequent psychological distress, particularly anxiety symptoms (Hypothesis 2). There were long-term physical health effects of these symptoms, given that anxiety symptoms were associated with physical health over two decades later (Hypothesis 3). By estimating trajectories of family economic pressure, marital instability, and anxiety symptoms, the current study sheds light on the unique roles of both the levels and rates of change in the hypothesized processes over a quarter of a century.
More specifically, these findings support previous research (Barton & Bryant, 2016; Wickrama et al., 2018) noting the adverse effects of stress proliferation on mental health. Family financial stress was related to increased levels of couples’ marital instability over time, which provides compelling evidence for systemic and dynamic associations between financial stress and marital attributes. These findings also reinforce the role of chronic contextual stressors in altering and shaping marital adaptations and are consistent with previous research indicating the particularly detrimental consequences of chronic economic stress for marital relationships (Kahn & Pearlin, 2006). Estimating a couple-level construct of marital instability from husbands’ and wives’ growth curves of perceived marital instability fit the data well, which supports previous research emphasizing the emotional concordance between couple members (Kiecolt-Glaser & Wilson, 2017).
For both husbands and wives, there were mental health consequences of marital instability. Identifying how, and to what extent, changes in marital instability over time impact changes in husbands’ and wives’ anxiety over time extends previous work linking marital instability to partners’ feelings of anxiety and stress (Nealey-Moore et al., 2007). The parallel trajectories between marital instability and anxiety symptoms provide evidence for the continual psychological effects of relational attributes over time. Thus, both the severity of couples’ marital instability as well as changes in their marital instability over time are influential for husbands’ and wives’ development of psychological distress. Consequently, in this fashion, adverse contextual stress can proliferate through declining marital stability and, in turn, result in increasing mental health challenges.
Furthermore, previous research has noted the physiological responses to psychological distress, including anxiety symptoms, and how these physiological responses, while adaptive in the moment, can have maladaptive and long-term health consequences (e.g., Player & Peterson, 2011). The current study findings indicated that the severity (i.e., initial level) of husbands’ and wives’ anxiety symptoms in their early middle years contributed to their physical health outcomes over 20 years later. The enduring consequences of the initial level of anxiety symptoms for both spouses highlight that elevated psychological distress is a long-term risk factor for poor physical health. Moreover, for husbands, the rate of change in anxiety symptoms also contributed to their physical health in later life. From a public health perspective, these findings highlight chronic anxiety as a risk factor for poor physical health, given that increases in anxiety symptoms over time were related to husbands’ subsequent increases in physical health risk.
Interestingly, it seems that husbands and wives have different sensitivities to anxiety symptoms. More specifically, for husbands, linkages between anxiety symptoms and physical health were limited to intraindividual associations in the initial level and rate of change in anxiety symptoms. For wives, their physical health in later adulthood (2015) was influenced by both their own and their partner’s level of anxiety symptoms in the early middle years (1990). This partner effect between husbands’ anxiety symptoms and wives’ physical health outcomes partially supports the hypothesized partner effects, drawn from APIM approach (Kenny et al., 2006), between spouses’ psychological distress and their partners’ physical health in later adulthood.
Simultaneously, these results revealed the influence of gender differences. On average, women were more influenced by their spouse’s psychological distress than men, which could amplify the negative influence of marital distress, increasing their risk for later physical health problems. These findings are congruent with the findings of previous research that showed women were often more sensitivity to marital distress than men (Kiecolt-Glaser & Newton, 2001) and more vulnerable to their spouse’s psychological distress (Behler et al., 2019; Kouros & Cummings, 2010). Similarly, other research (i.e., Revenson et al., 2016) also found that wives’ anxiety was more strongly impacted by husbands’ anxiety than the other way around, and higher levels of husbands’ anxiety predicted wives’ shorter sleep duration. Together, these findings suggest a pattern of greater relationally interdependence for women than men (Kiecolt-Glaser & Newton, 2001). The different responses to both physiological and emotional stressors between women and men may create variations in husbands’ and wives’ health in their later years. Further research is needed to enhance our understanding of gender differences within marital/romantic relationships and how these gender differences may contribute to stress-marriage-health processes.
Contemporaneous dependencies were also found between spouses’ physical health in later adulthood, suggesting concordant health patterns in couples. The health concordance between spouses may be a product of psychological stress-related responses that can be reciprocally transferred from one partner to the other. Furthermore, the sample represents an important subgroup of married couples (i.e., couples with marriages lasting over 20 years), which provides important insight into long-lasting intimate partner relationships. For instance, even in long-term marriages, experiences of marital instability relatively early in their relationship can have a detrimental impact on couple members’ physical health in later adulthood.
Limitations and Implications
There are several limitations that should be considered when interpreting the findings of this study. First, there are numerous marital attributes that may be indicators of how couples respond to stressful contexts (e.g., economic pressure), but the current study focused on one specific attribute—marital instability. This singular focus on one marital attribute may not fully delineate the dyadic processes in married couples. Future research incorporating additional characteristics of couples’ relational responses would extend these findings. For instance, assessing marital processes as a multidimensional construct, capturing observed behavioral exchange, communication skills, and conflict resolution styles, would provide a more nuanced understanding of marriage in the context of stressful experiences (Custer, 2009). Additionally, beyond the negative aspects of marital relationships, research is increasingly recognizing the impact of healthy marriages. There is a need to be more attentive to positive contexts and transformative processes, such as forgiveness, commitment, and sacrifice points (Fincham et al., 2007; Fincham & Beach, 2010). Taking these developments into account, future research can further explore how, and to what extent, such transformative processes override negative marital processes and related negative physical and mental health outcomes. Such research is well-positioned to inform the work of helping professionals engaging with couples to improve marital outcomes. Also, as previously mentioned, it is important to note that the sample was comprised of White families in long-term marriages who lived in the rural mid-West during a specific economic crisis. Because these families are similar to other families in many ways (i.e., experiences of significant financial hardship caused by various life challenges are not unique or uncommon), this study provides valuable insight into how families are affected by stressful times and how they adapt to the situations. Nonetheless, it is possible that the model tested may operate differently for families depending on their context, such as extreme economic hardship. This possibility is an important reason for replicating the current study findings with longitudinal data from diverse samples. Finally, beyond the long-term adverse effects of marital disruption on later physical health, there is growing interest in understanding the relationships between cumulative marital history and health as well as the differential effects of marital transitions, duration, and timing on physical health (Hughes & Waite, 2009; Zhang et al., 2016). As both the divorce rate and cohabitation increase among older people (Kennedy & Ruggles, 2014; Stepler, 2017), future research incorporating more detailed information of marital history would capture dynamic changes in marriages over the life course and provide additional insight into the effects of cumulative marital history.
In articulating useful implications that stem from these findings, the significance of earlier stressful life circumstances (such as financial difficulties) for marital relationships is apparent, which suggests the need for an integrated approach to improving marital processes and outcomes considering the contexts surrounding couples. For instance, it may be necessary for intervention and prevention efforts to focus greater attention on contextual stressors, such as chronic health problems or financial pressure. Interventions may need to focus on not only improving couples’ personal skills and resources but also on collaborating with family and community resources to ensure couples have access to resources that can foster resilience.
Furthermore, these findings inform policies and practices by identifying the extent of longitudinal influences and the ways in which stress proliferates from one experience (i.e., financial pressure in the current study) to influence key relationships and the detrimental mental health consequences of this stress proliferation which together culminate in increased physical health risk a quarter of a century later. Thus, policies at various levels must recognize the long-term impacts of stress, noting that efforts to reduce financial pressure or promote family financial stability can result in healthier families and communities in the future.
Acknowledgments
Support for this publication was provided by grant number T32HP30037 from the Health Resources and Services Administration (HRSA) through the Quality, Safety, and Comparative Effectiveness Research Training—Primary Care (QSCERT—PC) Program. This research is also currently supported by a grant from the National Institute on Aging [AG043599, Kandauda A. S. Wickrama, PI]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies. Support for earlier years of the study also came from multiple sources, including the National Institute of Mental Health [MH00567, MH19734, MH43270, MH59355, MH62989, MH48165, MH051361], the National Institute on Drug Abuse [DA05347], the National Institute of Child Health and Human Development [HD027724, HD051746, HD047573, HD064687], the Bureau of Maternal and Child Health [MCJ-109572], and the MacArthur Foundation Research Network on Successful Adolescent Development Among Youth in High-Risk Settings.
Contributor Information
Seonhwa Lee, University of California, Davis.
Kandauda K. A. S. Wickrama, University of Georgia.
Tae Kyoung Lee, University of Miami Miller School of Medicine.
Catherine Walker O’Neal, University of Georgia.
References
- Barton AW, & Bryant CM (2016). Financial strain, trajectories of marital processes, and African American newlyweds’ marital instability. Journal of Family Psychology, 30(6), 657–664. 10.1037/fam0000190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beach SR, Katz J, Kim S, & Brody GH (2003). Prospective effects of marital satisfaction on depressive symptoms in established marriages: A dyadic model. Journal of Social and Personal Relationships, 20(3), 355–371. 10.1177/0265407503020003005. [DOI] [Google Scholar]
- Behler R, Donnelly R, & Umberson D (2019). Psychological distress transmission in same-sex and different-sex marriages. Journal of Health and Social Behavior, 60(1), 18–35. 10.1177/0022146518813097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Booth A, Johnson D, & Edwards JN (1983). Measuring marital instability. Journal of Marriage and the Family, 45(2), 387–394. 10.2307/351516. [DOI] [Google Scholar]
- Conger RD, & Conger KJ (2002). Resilience in Midwestern families: Selected findings from the first decade of a prospective, longitudinal study. Journal of Marriage and Family, 64(2), 361–373. 10.1111/j.1741-3737.2002.00361.x. [DOI] [Google Scholar]
- Conger RD, Elder GH, Lorenz FO, Simons RL, & Whitebeck LB (1994). Social institutions and social change.Families in troubled times: Adapting to change in rural America. Aldine de Gruyter. [Google Scholar]
- Conger RD, Ge X, Elder GH, Lorenz FO, & Simons RL (1994). Economic stress, coercive family process, and developmental problems of adolescents. Child Development, 65(2), 541–561. 10.2307/1131401. [DOI] [PubMed] [Google Scholar]
- Custer L (2009). Marital satisfaction and quality. In Reis HT & Sprecher S (Eds.), Encyclopedia of human relationships (pp. 1030–1034). SAGE. [Google Scholar]
- Derogatis LR (1996). SCL-90-R: Symptom Checklist-90-R: Administration, scoring, and procedures manual. NCS Pearson. [Google Scholar]
- Deschênes SS, Dugas MJ, Fracalanza K, & Koerner N (2012). The role of anger in generalized anxiety disorder. Cognitive Behavior Therapy, 41(3), 261–271. 10.1080/16506073.2012.666564. [DOI] [PubMed] [Google Scholar]
- Dohrenwend BS, Krasnoff L, Askenasy AR, & Dohrenwend BP (1978). Exemplification of a method for scaling life events: The PERI life events scale. Journal of Health and Social Behavior, 19(2), 205–229. 10.2307/2136536. [DOI] [PubMed] [Google Scholar]
- Enders CK (2010). Applied missing data analysis. Guilford Press. [Google Scholar]
- Falconier MK, Nussbeck F, Bodenmann G, Schneider H, & Bradbury T (2015). Stress from daily hassles in couples: Its effects on intradyadic stress, relationship satisfaction, and physical and psychological well-being. Journal of Marital and Family Therapy, 41(2), 221–235. 10.1111/jmft.12073. [DOI] [PubMed] [Google Scholar]
- Fincham FD, & Beach SR (2010). Of memes and marriage: Toward a positive relationship science. Journal of Family Theory & Review, 2(1), 4–24. 10.1111/j.1756-2589.2010.00033.x. [DOI] [Google Scholar]
- Fincham FD, Stanley SM, & Beach SR (2007). Transformative processes in marriage: An analysis of emerging trends. Journal of Marriage and Family, 69(2), 275–292. 10.1111/j.1741-3737.2007.00362.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galovan AM, Holmes EK, & Proulx CM (2017). Theoretical and methodological issues in relationship research: Considering the common fate model. Journal of Social and Personal Relationships, 34(1), 44–68. 10.1177/0265407515621179. [DOI] [Google Scholar]
- Gudmunson CG, Beutler IF, Israelsen CL, McCoy JK, & Hill EJ (2007). Linking financial strain to marital instability: Examining the roles of emotional distress and marital interaction. Journal of Family and Economic Issues, 28(3), 357–376. 10.1007/s10834-007-9074-7. [DOI] [Google Scholar]
- Guilbert DE, Vacc NA, & Pasley K (2000). The relationship of gender role beliefs, negativity, distancing, and marital instability. The Family Journal, 8(2), 124–132. 10.1177/1066480700082003. [DOI] [Google Scholar]
- Hawkins KA, & Cougle JR (2011). Anger problems across the anxiety disorders: Findings from a population-based study. Depression and Anxiety, 28(2), 145–152. 10.1002/da.20764. [DOI] [PubMed] [Google Scholar]
- Helm JL, Sbarra D, & Ferrer E (2012). Assessing cross-partner associations in physiological responses via coupled oscillator models. Emotion, 12(4), 748–762. 10.1037/a0025036. [DOI] [PubMed] [Google Scholar]
- Hu LT, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55. 10.1080/10705519909540118. [DOI] [Google Scholar]
- Hughes ME, & Waite LJ (2009). Marital biography and health at mid-life. Journal of Health and Social Behavior, 50(3), 344–358. 10.1177/002214650905000307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kahn JR, & Pearlin LI (2006). Financial strain over the life course and health among older adults. Journal of Health and Social Behavior, 47(1), 17–31. 10.1177/002214650604700102. [DOI] [PubMed] [Google Scholar]
- Karney BR, & Bradbury TN (1995). The longitudinal course of marital quality and stability: A review of theory, methods, and research. Psychological Bulletin, 118(1), 3–34. 10.1037/0033-2909.118.1.3. [DOI] [PubMed] [Google Scholar]
- Kennedy S, & Ruggles S (2014). Breaking up is hard to count: The rise of divorce in the United States, 1980–2010. Demography, 51(2), 587–598. 10.1007/s13524-013-0270-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kenny DA, Kashy DA, & Cook WL (2006). Dyadic Data Analysis. Guilford Press. [Google Scholar]
- Kiecolt-Glaser JK, McGuire L, Robles TF, & Glaser R (2002). Psychoneuroimmunology: Psychological influences on immune function and health. Journal of Consulting and Clinical Psychology, 70(3), 537–547. 10.1037/0022-006X.70.3.537. [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, & Newton TL (2001). Marriage and health: His and hers. Psychological Bulletin, 127(4), 472–503. 10.1037/0033-2909.127.4.472. [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, & Wilson SJ (2017). Lovesick: How couples’ relationships influence health. Annual Review of Clinical Psychology, 13, 421–443. 10.1146/annurevclinpsy-032816-045111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kouros CD, & Cummings EM (2010). Longitudinal associations between husbands’ and wives’ depressive symptoms. Journal of Marriage and Family, 72(1), 135–147. 10.1111/j.1741-3737.2009.00688.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ledermann T, & Kenny DA (2012). The common fate model for dyadic data: Variations of a theoretically important but underutilized model. Journal of Family Psychology, 26(1), 140–148. 10.1037/a0026624. [DOI] [PubMed] [Google Scholar]
- Lee TK, Wickrama KAS, & O’Neal CW (2019). Midlife general psychopathology trajectories and later-life physical health in husbands and wives. Health Psychology, 38(6), 553–562. 10.1037/hea0000745. [DOI] [PubMed] [Google Scholar]
- McEwen BS (1998). Protective and damaging effects of stress mediators. New England Journal of Medicine, 338(3), 171–179. 10.1056/NEJM199801153380307. [DOI] [PubMed] [Google Scholar]
- McEwen BS, & Gianaros PJ (2010). Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Annals of the New York Academy of Sciences, 1186, 190–222. 10.1111/j.1749-6632.2009.05331.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2017). Mplus user’s guide (8th ed.). Muthén & Muthén. [Google Scholar]
- Nealey-Moore JB, Smith TW, Uchino BN, Hawkins MW, & Olson-Cerny C (2007). Cardiovascular reactivity during positive and negative marital interactions. Journal of Behavioral Medicine, 30(6), 505–519. 10.1007/s10865-007-9124-5. [DOI] [PubMed] [Google Scholar]
- Neff LA, & Karney BR (2017). Acknowledging the elephant in the room: How stressful environmental contexts shape relationship dynamics. Current Opinion in Psychology, 13, 107–110. 10.1016/j.copsyc.2016.05.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Brien M (2005). Studying individual and family development: Linking theory and research. Journal of Marriage and Family, 67(4), 880–890. 10.1111/j.1741-3737.2005.00181.x. [DOI] [Google Scholar]
- Papp LM, Cummings EM, & Goeke-Morey MC (2009). For richer, for poorer: Money as a topic of marital conflict in the home. Family Relations, 58(1), 91–103. 10.1111/j.1741-3729.2008.00537.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Player MS, & Peterson LE (2011). Anxiety disorders, hypertension, and cardiovascular risk: A review. The International Journal of Psychiatry in Medicine, 41(4), 365–377. 10.2190/PM.41.4.f. [DOI] [PubMed] [Google Scholar]
- Randall AK, & Bodenmann G (2009). The role of stress on close relationships and marital satisfaction. Clinical Psychology Review, 29(2), 105–115. 10.1016/j.cpr.2008.10.004. [DOI] [PubMed] [Google Scholar]
- Revenson TA, Marín-Chollom AM, Rundle AG, Wisnivesky J, & Neugut AI (2016). Hey Mr. Sandman: Dyadic effects of anxiety, depressive symptoms and sleep among married couples. Journal of Behavioral Medicine, 39(2), 225–232. 10.1007/s10865-015-9693-7. [DOI] [PubMed] [Google Scholar]
- Robles TF, Slatcher RB, Trombello JM, & McGinn MM (2014). Marital quality and health: A meta-analytic review. Psychological Bulletin, 140(1), 140–187. 10.1037/a0031859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saxbe D, & Repetti RL (2010). For better or worse? Coregulation of couples’ cortisol levels and mood states. Journal of Personality and Social Psychology, 98(1), 92–103. 10.1037/a0016959. [DOI] [PubMed] [Google Scholar]
- Stepler R (2017). Number of U.S. adults cohabiting with a partner continues to rise, especially among those 50 and older. Fact Tank: Pew Research Center. http://pewrsr.ch/2oMk0aR [Google Scholar]
- Timmons AC, Margolin G, & Saxbe DE (2015). Physiological linkage in couples and its implications for individual and interpersonal functioning: A literature review. Journal of Family Psychology, 29(5), 720–731. 10.1037/fam0000115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Treiber FA, Kamarck T, Schneiderman N, Sheffield D, Kapuku G, & Taylor T (2003). Cardiovascular reactivity and development of pre-clinical and clinical disease states. Psychosomatic Medicine, 65(1), 46–62. 10.1097/00006842-200301000-00007. [DOI] [PubMed] [Google Scholar]
- Ulrich-Lai YM, & Herman JP (2009). Neural regulation of endocrine and autonomic stress responses. Nature Reviews Neuroscience, 10(6), 397–409. 10.1038/nrn2647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Umberson D, Williams K, Powers DA, Liu H, & Needham B (2006). You make me sick: Marital quality and health over the life course. Journal of Health and Social Behavior, 47(1), 1–16. 10.1177/002214650604700101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whisman MA (2007). Marital distress and DSM-IV psychiatric disorders in a population-based national survey. Journal of Abnormal Psychology, 116(3), 638–643. 10.1037/0021-843X.116.3.638. [DOI] [PubMed] [Google Scholar]
- Whisman MA, & Baucom DH (2012). Intimate relationships and psychopathology. Clinical Child and Family Psychology Review, 15(1), 4–13. 10.1007/s10567-011-0107-2. [DOI] [PubMed] [Google Scholar]
- Wickrama KAS, Lee TK, & O’Neal CW (2019). Marital strain trajectories over a quarter century and spouses’ loneliness: Couple-level and individual pathways. Journal of Social and Personal Relationships, 37(3), 821–842. 10.1177/0265407519879512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wickrama KAS, Lee TK, O’Neal CW, & Lorenz FO (2016). Multivariate applications series.Higher-order growth curves and mixture modeling with Mplus: A practical guide. New York, NY: Routledge/Taylor & Francis Group. 10.4324/9781315642741. [DOI] [Google Scholar]
- Wickrama KAS, O’Neal CW, & Lorenz FO (2018). Marital processes linking economic hardship to mental health: The role of neurotic vulnerability. Journal of Family Psychology, 32(7), 936–945. 10.1037/fam0000435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang Z, Liu H, & Yu Y-L (2016). Marital biography and health in middle and late life. In Book-wala J (Ed.), Couple relationships in the middle and later years: Their nature, complexity, and role in health and illness (pp. 199–218). American Psychological Association. [Google Scholar]